
Abstract
Aims:
We aimed to evaluate the risk of valvular heart disease (VHD) among patients with ankylosing spondylitis (AS).
Methods:
This was a population-based cohort study utilizing the Longitudinal Health Insurance Research Database of the National Health Insurance in Taiwan. Patients with and without coding of newly diagnosed AS from 1999 to 2013 were assigned to the AS and non-AS groups, respectively. Primary outcome was the incidental risk of VHD. Multiple Cox regression was used to estimate the adjusted hazard ratio of VHD. Subgroup analysis and sensitivity tests were also conducted.
Results:
The AS group included 3780 patients, and 22,680 matched subjects without an AS diagnosis were identified as controls. The AS group had an increased risk of VHD compared with non-AS controls (adjusted hazard ratio: 1.63; 95% confidence interval: 1.43–1.86; p < 0.001). Subgroup analysis also revealed an increased risk of individual types of VHD, including aortic, mitral, and tricuspid valve disease. Patients in the AS group had a higher incidence of valve replacement surgery after the onset of VHD.
Conclusion:
Patients with AS had a significant risk of VHD compared to non-AS controls in this population-based cohort study. Screening for VHD may be needed in caring patients with AS. We suggest that echocardiography may be performed when patients are diagnosed with AS.
Keywords
Introduction
Ankylosing spondylitis (AS) is a complex disease that affects men more than women, with a worldwide prevalence of approximately 1.2%. 1 Most patients with AS have disease onset in their third decade. Radiographic evidence of sacroiliitis and symptoms of lower back pain that improve with exercise are diagnostic for AS. 2 AS-associated extra-articular manifestation has been described, including cardiovascular disease such as conduction disturbances, cardiac arrhythmias, cardiomyopathy, and ischemic heart disease.3,4 Moreover, cardiovascular involvement accounts for 40% of deaths in patients with AS. 5
Valvular heart disease (VHD) is reportedly associated with AS. Echocardiographic abnormalities, for example, fibrosis and dilatation of the aortic root or cardiac valve thickening, have been observed in patients with AS.6,7 Histopathological findings from necropsy patients with AS revealed fibrotic changes beneath the aortic valve and subaortic ridge, even extending to the anterior leaflet of the mitral valve. 8 In real-world research, the prevalence rate of VHD in patients with AS is inconsistent. Some descriptive studies found that 1–10% of patients with AS have aortic valve disease, whereas 5% of those have mitral valve disease.9,10 The prevalence rate is almost doubled in patients with AS in whom the peripheral joints are involved. 4 Grygiel-Górniak et al. 11 reported that approximately 80% of patients with AS have aortic valve and/or aortic root involvement. 12 Overall, aortic regurgitation is the most frequently reported VHD in patients with AS. Compared with rheumatoid arthritis, aortic involvement appears to be specific to patients with AS. 13
Studies have demonstrated a possible role for VHD as a predictive factor for the severity of AS.11,12 The presence of VHD is related to the duration of AS and predicate for peripheral joint involvement.14,15 The association between AS and VHD raises interesting and important issues since valve involvement is a potential risk for heart failure or even death. 16 However, current studies lack convincing evidence for the association between AS and VHD due to small numbers of participants, and study confounders such as age, hypertension, diabetes mellitus, or hyperlipidemia may contribute to the study bias. Thus, the aim of this study was to evaluate the risk of VHD among patients with AS by analyzing a nationwide population-based retrospective cohort from the National Health Insurance Research Database (NHIRD) in Taiwan. We hypothesized those patients with AS have a higher risk of developing VHD. We also examined the risk of individual types of VHD among patients with AS such as aortic valve disease, mitral valve disease, tricuspid valve disease, and pulmonary valve disease, and the risk of undergoing valve replacement surgery after the onset of VHD throughout the course of AS.
Methods
Ethics approval and study design
This study was approved by the Institutional Review Board of Chung Shan Medical University Hospital (CS2-19068). Written consent was not obtained from the study participants as only de-identified data were obtained from the Longitudinal Health Insurance Database (LHIRD), and a waiver of patient consent was provided by the Ethics Committee for this study.
This retrospective cohort study was based on the NHIRD, which provides comprehensive medical care coverage to more than 99% of Taiwan’s residents of 23 million beneficiaries. The database stores all insurance claims data and patient identification such as numbers, sex, age, diagnostic codes, hospital information, and drug prescriptions. The LHIRD consists of 1 million people randomly sampled from the 23 million beneficiaries of the NHIRD from 1999 to 2013.17–19
Participants
This study extracted data from the LHIRD in Taiwan using newly diagnosed AS [International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) code: 720.0] for at least three outpatient visits or one inpatient admission to ensure the accuracy of the diagnosis. The index date was defined as the date of the first available AS record according to modified New York’s criteria. 2 Individuals with a diagnosis of VHD (ICD-9-CM codes: 394–397, 424.0–424.3) prior to the index date were excluded. Study subjects were categorized into two groups: those with an AS diagnosis (the AS group, n = 3780) and those without an AS diagnosis (the non-AS group, n = 988,084). The study outcome was defined as the onset of VHD based on the ICD-9-CM codes. The participants were followed up until the occurrence of the study outcome, withdrawal from the NHIRD, or until 31 December 2013. A flowchart of the enrollment of the study cohort is presented in Figure 1.

Flowchart of study.
Covariates
The baseline characteristics included age, sex, hypertension (ICD-9-CM: 401–405), hyperlipidemia (ICD-9-CM: 272.0–272.4), chronic liver disease (ICD-9-CM: 571), chronic kidney disease (ICD-9-CM: 585), diabetes mellitus (ICD-9-CM: 250), chronic obstructive pulmonary disease (ICD-9-CM: 491, 492, 496), autoimmune disease (ICD-9-CM: 710.0, 720.0, 714.0), heart failure (ICD-9-CM: 428), ischemic heart disease (ICD-9-CM: 410–414), and arrhythmias (ICD-9-CM: 426–427). All of the comorbidities were included if they were recorded within 1 year before the index date for at least three outpatient visits or one hospitalization. A 1:6 matching by age and sex was used to assign the index date for the non-AS group to ensure the same initiation date for both groups.
Statistical analysis
Data are presented as valid percentages and mean values with a standard deviation. Absolute standardized difference was used to evaluate the heterogeneity of the baseline characteristics, and an absolute standardized difference ⩽0.1 indicated a negligible difference in potential confounders between the two study groups. The cumulative incidence of VHD development was calculated using Kaplan–Meier analysis, and the log-rank test was used to test the significance. The hazard ratios between the two study groups were estimated using the Cox proportional hazards model. Sensitivity analyses were performed using a propensity score method by matching age, sex, hypertension, hyperlipidemia, chronic liver disease, chronic kidney disease, diabetes, chronic obstructive pulmonary disease, other autoimmune diseases, heart failure, ischemic heart disease, and arrhythmias as controls. SPSS version 18.0 (SPSS Inc., Chicago, IL, USA) was applied for the statistical analyses.
Results
A total of 4007 subjects diagnosed with AS were enrolled from the NHIRD. After excluding subjects diagnosed with AS before the index date, 3780 subjects were assigned to the AS group. The incidence of AS is between 0.42 and 0.51 per 1000 person-years during 2004 and 2013. A total of 988,084 subjects without a diagnosis of AS were included in the non-AS group. The study group included 3780 participants with AS diagnosis, and the control group included 22,680 age-and-sex-matched randomly selected participants without an AS diagnosis (Figure 1). The baseline characteristics of all the patients are presented in Table 1.
Demographic characteristics of AS group and non-AS group.

AS, ankylosing spondylitis; ASD, absolute standardized differences; COPD, chronic obstructive pulmonary disease.
Risk of VHD
A total of 1043 subjects with VHD were observed over 176,680 person-years in the non-AS group, and a total of 287 subjects with VHD were observed over 28,845 person-years in the AS group. The cumulative probability of VHD was statistically higher among patients with AS over a 12-year period of follow-up (log-rank test, p < 0.001; Figure 2). The incidence density of VHD among patients with AS was higher compared with that in patients without AS (9.95 versus 5.90 per 1000 person-years). The Cox proportional hazards model revealed a statistically higher risk of VHD in the AS cohort [adjusted hazard ratio (aHR): 1.63, 95% confidence interval (CI): 1.43–1.86; Table 2].
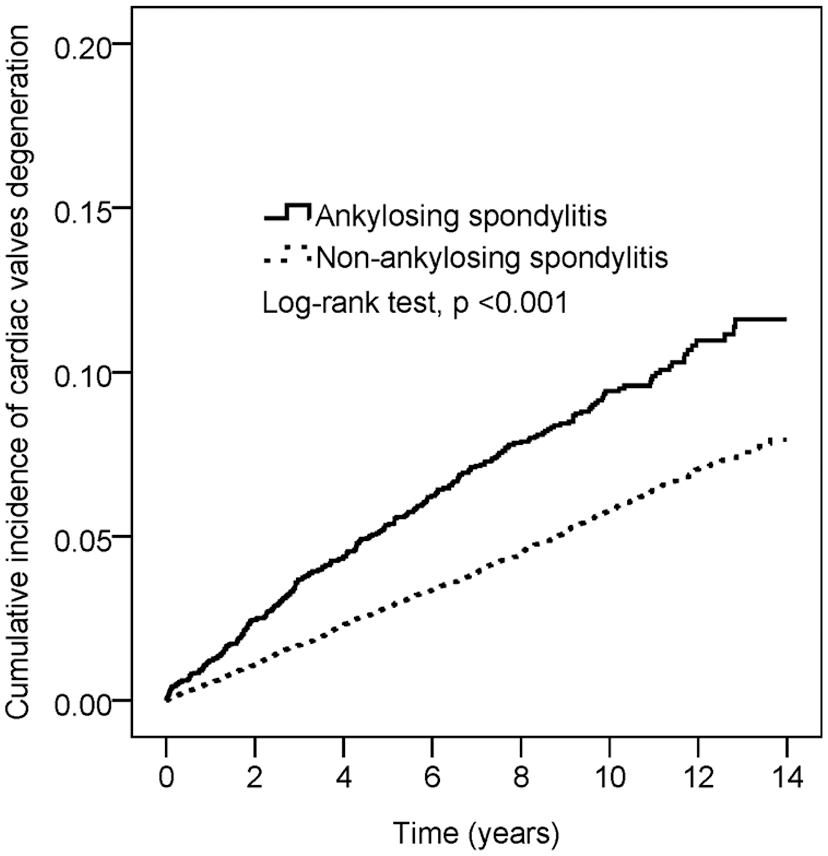
Kaplan–Meier curves of the cumulative probability of valvular heart disease for the study cohort with ankylosing spondylitis versus without ankylosing spondylitis.
Cox proportional hazard model analysis for risk of VHD.

Adjusted for age, sex, hypertension, hyperlipidemia, chronic liver disease, chronic kidney disease, diabetes, COPD, autoimmune disease, heart failure, ischemic heart disease, and arrhythmias.
AS, ankylosing spondylitis; COPD, chronic obstructive pulmonary disease; VHD, valvular heart disease.
Subgroup analysis of VHD
The secondary outcome analysis revealed that subjects with AS had a higher risk of developing aortic valve disease (aHR: 1.66, 95% CI: 1.42–1.95, p < 0.001), mitral valve disease (aHR: 1.54, 95% CI: 1.13–2.09, p = 0.006), and tricuspid valve disease (aHR: 1.71, 95% CI: 1.07–2.74, p = 0.025; Table 3). In addition, patients with AS tended to have a higher risk of developing VHD (aHR: 1.97, 95% CI: 1.70–2.29, p < 0.001) in aged less than 65 years, and this difference was not observed among those aged more than 65 years (aHR: 1.07, 95% CI: 0.81–1.41, p = 0.652; Table 4). As soon as VHD developed, the risk of VHD requiring valve replacement was higher among participants in the AS group than among those in the non-AS group (aHR: 5.09, 95% CI: 1.55–16.68, p = 0.007; Table 3).
Secondary outcome for risk of VHD subtype.

Adjusted for age, sex, hypertension, hyperlipidemia, chronic liver disease, chronic kidney disease, diabetes, COPD, autoimmune disease, heart failure, ischemic heart disease, and arrhythmias.
Adjusted for age, sex, hypertension, hyperlipidemia, chronic liver disease, diabetes, COPD, autoimmune disease, heart failure, ischemic heart disease, and arrhythmias.
ICD-9-CM for cardiac valve replacement included 68016A, 68016B, 68017A, 68017B, 68018A, and 68018B.
AS, ankylosing spondylitis; COPD, chronic obstructive pulmonary disease; VHD, valvular heart disease.
Subgroup analysis of the association between AS and VHD.

AS, ankylosing spondylitis; CI, confidence interval; HR, hazard ratio; VHD, valvular heart disease.
The sensitivity analysis revealed that the risk of VHD was higher in the AS group after propensity score matching using confounders than in the control group (aHR: 1.67, 95% CI: 1.38–2.02, p < 0.001; Table 5).
Sensitivity analysis for risk of VHD (propensity score matching).

Adjusted for age, sex, hypertension, hyperlipidemia, chronic liver disease, chronic kidney disease, diabetes, COPD, autoimmune disease, heart failure, ischemic heart disease, and arrhythmias.
AS, ankylosing spondylitis, CI, confidence interval; HR, hazard ratio; VHD, valvular heart disease.
Discussion
In our study, we observed that subjects with AS had a 1.63-fold higher risk of VHD compared with those without AS; moreover, the results were consistent regarding individual types of VHD such as mitral valve disease, aortic valve disease, and tricuspid valve disease. Our study also demonstrated that patients with AS are at higher risk of undergoing valve replacement surgery after the onset of VHD. To date and to the best of our knowledge, this is the first cohort study to demonstrate the increased risk of overall VHD among subjects with AS utilizing a nationwide longitudinal population-based database.
Like our report, studies noted that the prevalence of aortic regurgitation appears to be higher in patients with AS than in the general population.20,21 Similarly, one previous study also concluded that patients with AS are at higher risk of aortic regurgitation. 22 However, the small numbers of participants and a retrospective in the study design may have limited the strength of the evidence. Our cohort study revealed an increased risk of VHD among subjects with AS, and the risk of VHD in the AS group was consistent even after adjusting for multiple confounders. These results should alert physicians to the possibility of a higher risk of VHD in patients with AS as well as poor outcomes such as valve replacement surgery after the onset of VHD.
In our study, we found a significantly higher risk of aortic valve disease, mitral valve disease, and tricuspid valve disease among subjects with AS compared with the control group. The nonsignificant difference in the incidence of pulmonary valve disease between the AS and non-AS groups may be due to fewer events. In the subgroup analysis of participants aged younger than 65 years, the risk of VHD was higher in the AS group than in the non-AS group. However, this difference was not observed in the subgroup of participants aged 65 years or older. In the general asymptomatic population, the prevalence of clinically significant VHD was higher among older people, except for mitral stenosis. 23 Thus, a possible mechanism, such as chronic systemic inflammation, may account for the early onset of VHD in the AS group. By contrast, atherosclerotic changes related to the aging process may attenuate the impact of AS in VHD development. The inflammatory hypothesis underlying the causal relation between VHD and AS is unclear. However, VHD is characterized by a continuous inflammatory cellular response that results in a left ventricular hemodynamic stress change in response to valvulopathy.24,25 The present inflammatory hypothesis suggests that with the progression of AS, the inflammatory cytokine response is activated, leading to the continuation of deleterious effects on the valve. 26
In our study, both men and women with underlying AS were predisposed to the development of cardiac valve disease compared with the control group, whereas women with AS had a higher risk of VHD than men. Many reports demonstrated that female sex was associated with an increased risk of aortic regurgitation, mitral stenosis, and tricuspid regurgitation compared with male sex, although male sex is thought to be more prevalent in AS and have worse disease severity.27,28 It is possible that women had a slightly earlier age of disease onset and more frequently reported family histories of AS in first-degree relatives. 28 Our study demonstrated that patients with heart failure, ischemic heart disease, and arrhythmias are predisposed to a higher risk of developing VHD, which was consistent with current findings regarding the risk factors for VHD. 7
Inflammatory processes result in endarteritis and fibrous tissue deposition, involving valves and their apparatus including the annulus, cusp, and even the aortic root, thus contributing to inadequate valve alignment or root dilatation which may explain the development of VHD in patients with AS. 29 Histopathological findings from necropsy patients with AS also revealed fibrous tissue deposits in the adventitia and intima of the aortic valve and even subaortic ridge with platelet aggregation, even extending to the anterior mitral leaflet resulting in aortic valve and mitral valve thickening and, ultimately, valve incompetence. 8 On the other hand, aortic root dilatation related to endarteritis resulting in inappropriate aortic valve coaptation contributes to aortic valve regurgitation. The aneurysmatic changes in the aorta with microscopic characteristics of aortitis AS have been described from patients with AS and severe aortic regurgitation undergoing replacement of the aortic valve and ascending aorta. 30 Echocardiography findings included abnormal aortic ring reflectance and increased aortic root diameter in cardiopulmonary asymptomatic patients either with juvenile-onset AS or adult-onset AS. 31 Trans esophageal echocardiography in patients with AS revealed subaortic tissue hyper echogenicity that was consistent with microscopic fibrotic changes in the subaortic ridge. 32
The relationship between mitral valve disease and AS has been discussed, although the incidence of mitral valve disease in patients with AS is lower than that of aortic valve disease. A small cross-sectional study described a higher prevalence of mitral valve regurgitation and mitral valve prolapse in patients with AS compared with the general population. 32 Mitral valve disease plays an important role in the development of heart failure in patients with AS. 15 Our study demonstrated a statistically higher risk of mitral valve disease in patients with AS. The possible mechanism underlying the development of mitral valve disease includes stiffness and impaired mitral valve mobility due to fibrosis of the subaortic tissues that extend to the mitral valve leaflet. Otherwise, a hypertrophied left ventricle results from severe aortic regurgitation which may cause distorted mitral valve apparatus. 14
Limited studies have emphasized the risk of valve replacement in patients with AS and VHD. Kawasuji et al. 30 described three patients with AS who had severe aortic valve regurgitation and underwent aortic valve replacement. Our study demonstrated that, after age and sex adjustment, patients with AS are at a higher risk of undergoing valve replacement after the onset of VHD than those without AS. The risk in other studies was lower than those found in our study, possibly due to the fact that inherited and inflammatory connective tissue disorder in patients with AS contribute to aortic valve damage and aortic root dilation.12,33
Study limitation
We highlight the following limitations. First, our subgroup analysis found that subjects with AS have a statistically higher risk of mitral valve, aortic valve, and tricuspid valve disease development. Nevertheless, we could not distinguish the VHD from the type of regurgitation or stenosis. Second, the echocardiographic findings and hemodynamic parameters were not available from the NHIRD; thus, we also could not ascertain the severity of VHD. Third, the NHIRD does not include exposure information regarding patients’ body mass index, family history, or inflammatory biomarkers, which may be associated risk factors for VHD. Therefore, these unmeasured confounding factors might have biased our results. Fourth, the number of patients, both with or without AS, who underwent valve replacement surgery was limited, although the risk of valve replacement was statistically higher in patients with AS after adjusting for confounders.
Conclusions
In summary, patients with AS were at a higher risk of VHD compared with non-AS controls in this nationwide population-based cohort study. Clinicians should be aware of the possibility of VHD in patients with AS and appropriate screening for the same may be needed in caring for patients with AS. We suggest that echocardiography may be performed when patients are diagnosed with AS.
Footnotes
Acknowledgements
This study was supported by Dry Lab of the Chung Shan Medical University Hospital.
Authors’ note
The contents of this publication are solely the responsibility of authors and do not necessarily represent the official view of the funding sources.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the grant from Chung Shan Medical University Hospital (CSH-2020-C-001).