
Abstract
The anatomy of the sacroiliac joint (SIJ) is complex with wide variations inter-individually as well as intra-individually (right versus left) and a frequent occurrence of anatomical variants. Besides, the joints are subject to strain, which may elicit non-inflammatory subchondral changes such as bone marrow edema (BME), sclerosis, and fat deposition simulating inflammatory SIJ changes. Furthermore, normal physiological changes during skeletal maturation can make interpretation of SIJ magnetic resonance imaging in children challenging. Knowledge about the wide range of normal findings is therefore important to avoid misinterpretation of findings as pathological. This review describes the current knowledge about normal SIJ findings across all ages.
Keywords
Introduction
The anatomy of the sacroiliac joint (SIJ) is complex with a wide range of normal variation. The SIJs connect the spine to the pelvis and are subject to considerable strain as the load from the lumbar spine to the lower extremities is transferred through the joints. This can result in non-inflammatory subchondral changes such as bone marrow edema (BME), sclerosis, and fat deposition in addition to signs of degenerative joint changes with osteophyte formation, joint space alteration, and sclerosis. Interpretation of SIJ is particularly challenging in children where normal physiological changes are seen during skeletal maturation. In the diagnostics of suspected inflammatory SIJ changes, knowledge about the range of normal findings is important to avoid misinterpreting findings as the disease.
This paper outlines current knowledge of normal SIJ findings across all ages but with a separate description of the normal physiological and growth-related findings in childhood.
Development and anatomical considerations
The sacrum is formed by a complex process of fusing primary and secondary ossification centers (Figure 1). The primary centers undergo fusion around 7 years of age, while multiple small apophyses slowly ossify during further maturation continuing into late adolescence.1,2 The ossification of the segmental and lateral apophyses of the sacral wings is completed significantly earlier in girls than in boys. 3 During this ossification process, these cartilaginous segmental and lateral apophyses of the sacral wings and the underlying newly formed subchondral bone are visible on magnetic resonance imaging (MRI). 3
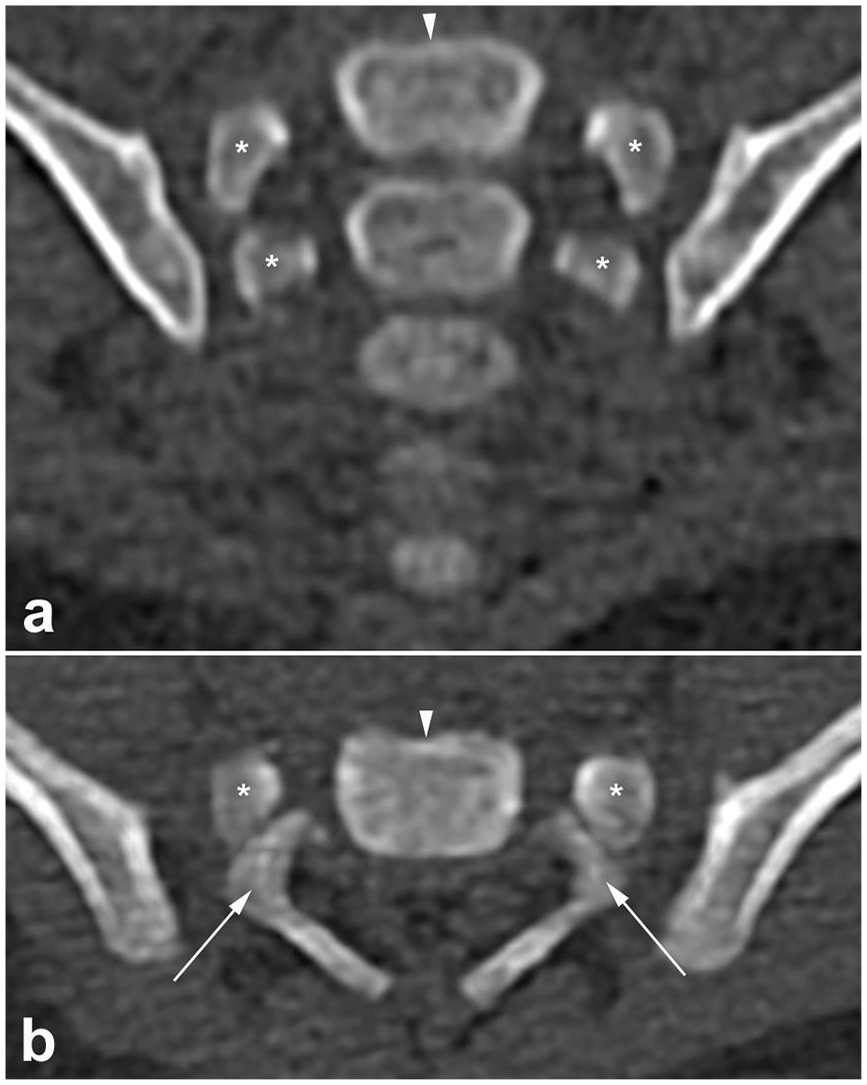
Normal sacral development. (a) Semi-coronal and (b) axial low-dose CT images in a 1-month-old girl illustrating the primary ossification centers of the sacrum. Each sacral vertebra has five primary ossification centers: the centrum (white arrowhead), two centers for the neural arch (asterisks), and two costal processes (white arrows). During further maturation, multiple small apophyses (secondary ossification centers) that fuse to the various surfaces of the primary centers slowly ossify a process that continues into late adolescence.
The SIJ is formed between the sacrum and the iliac bones and transfers all load between the spine and the lower extremities. Joint stability is secured by the sacrum being wedged cranially and dorsally between the iliac bones within the pelvic ring surrounded by strong ligaments and muscles. 4 The joint is composed of two anatomically different compartments, an anterior/inferior cartilaginous and a posterior/superior ligamentous compartment (Figure 2).4,5 The cartilaginous joint compartment is formed corresponding to the sacral segments S1–S3, but the inclusion of a complete S3 segment is uncommon in women. 4 The load-bearing cartilaginous joint surface of the SIJ is therefore smaller in women compared to men, whereas the interosseous ligament in the ligamentous compartment is larger in women than in men. 4 Moreover, the sacrum is usually located more horizontally in women compared to men. These anatomical differences may play a role in gender-related differences in the occurrence and location of strain-related changes. The iliac joint facet has a contour opposite to the sacral contour, both with small groves and ridges. There is considerable inter-individual variation in the shape and contour of the joint surfaces, especially in women, and also intra-individual variation (left versus right).4,6,7 The intervening slim joint space has a width of 2–3 mm in younger adults which gradually narrows with age.7,8
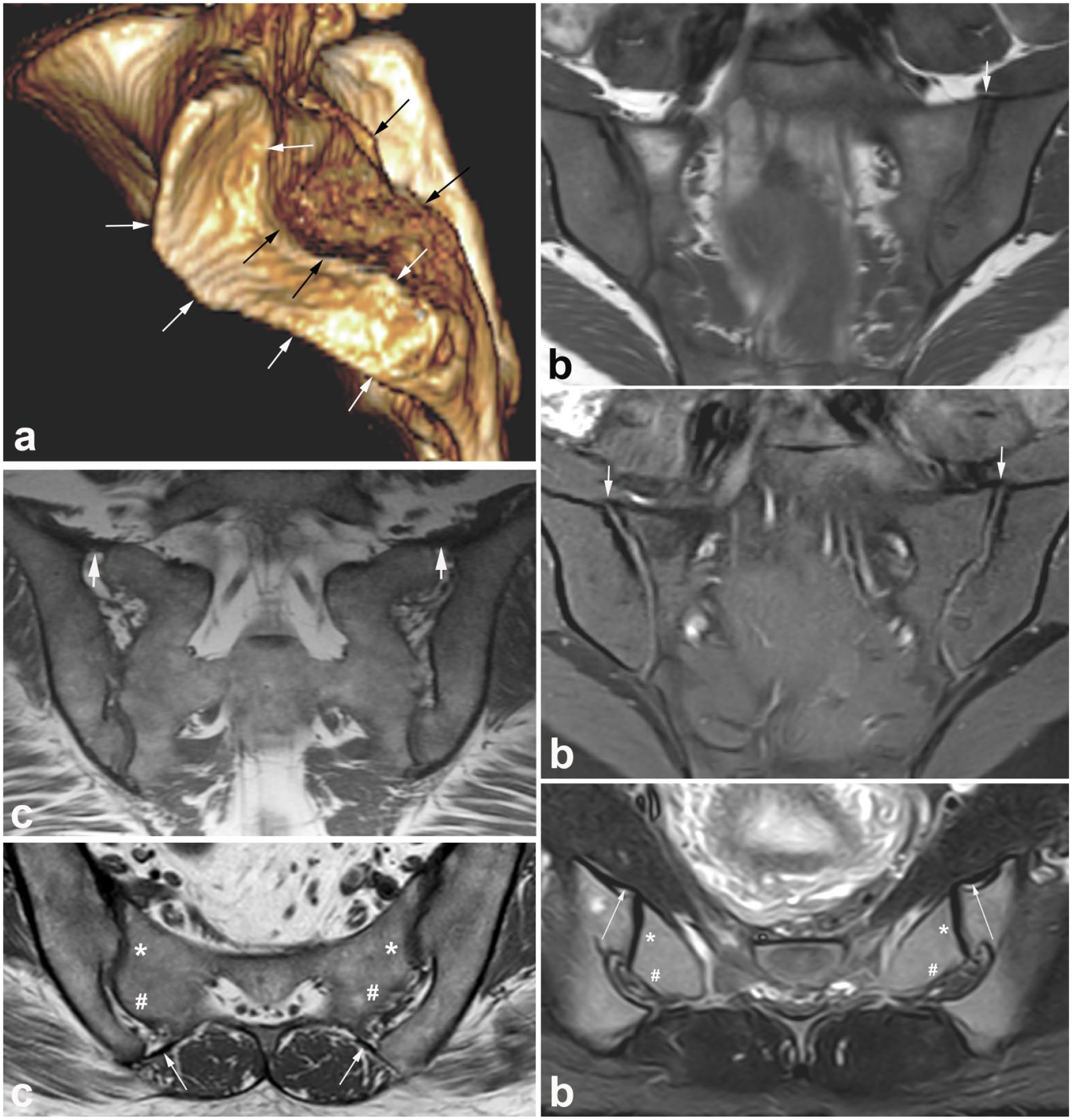
Normal anatomy in adults. (a) 3D CT reconstruction of the sacral joint facets showing the cartilaginous joint facets located anterior–inferiorly (marked with white arrows) and the ligamentous joint compartment located posterior–superiorly (black arrows). On MR images, the separation between the two compartments is clearly seen on axial slices, marked on images (b) and (c) with * and #, respectively. (b) Anterior sacroiliac ligament, MRI in a young healthy female volunteer. Semi-coronal T1-weighted (upper image) and T1FS images (middle image) and semi-axial STIR image (bottom image) at the lower part of the joints. On the semi-coronal slices, the ligaments are seen at the upper border of the joints, most clearly delineated on the T1FS image (arrows). On the semi-axial slice, a slightly thickened ligament is seen passing from the anterior surface of the ileum across the joint spaces to the sacrum passing anteriorly to a normal fluid-filled synovial pouch (long slim arrows). The cartilaginous compartment is on the sacral side marked with * and the ligamentous compartment with #. (c) Posterior sacroiliac ligament, MRI in a woman in the early 30s with intermittent low back pain and a disk herniation, but no clinical or biochemical signs indicating axial spondyloarthritis. Semi-coronal T1 at the posterior part of the SIJ (upper image) and semi-axial T1 in the middle portion of the joint. On the coronal image, the posterior sacroiliac ligament is seen at the upper part of the joint (thick arrows), but it is generally best visualized on the axial slice, extending from the posterior iliac spine to the posterior surface of the sacrum, located posteriorly to the interosseous ligament in the ligamentous joint compartment (long slim arrows). The axial slice also shows a crescent-like appearance of the right-sided ligamentous joint compartment and a brim of iliac sclerosis on both sides with adjacent fat deposition. The cartilaginous compartment is on the sacral side marked with * and the ligamentous compartment with #.
The surrounding stabilizing ligaments, the anterior and posterior sacroiliac ligaments, and also the iliolumbar ligament may be visualized by MRI of the SIJ (Figure 2). 4
Normal findings in children/adolescents
Interpretation of SIJ MRI in children and adolescents can be more challenging compared to adults due to normal physiological changes during skeletal maturation, which can give rise to diagnostic challenges as they can simulate disease. 9 If not recognized as normal findings, these growth-related changes can lead to false-positive diagnoses of sacroiliitis.10,11 Frequent pitfalls are growth-related signal changes in both subchondral bone and in the joint space itself, cortical blurring and irregularities, joint facet defects, and vascular structures.
Normal variability on T2/STIR
During the ossification process, the cartilaginous epiphyses and underlying newly formed subchondral bone are visible on MRI. They appear as areas of increased signal on water-sensitive sequences such as fat-saturated T2-weighted (T2FS) or short tau inversion recovery (STIR) sequences. 3 On SIJ MRI in children, a rim of subchondral high T2 signal (‘flaring’) is commonly observed along the borders of the SIJ, which is often confused with BME (Figure 3).12,13 This subchondral ‘flaring’ is most prominently seen in prepubertal and pubertal children, and is more frequently seen in boys, also with peak intensity of the signal changes later than in girls (ages 8–12 versus 7–10 years). The high signal intensity is typically symmetrical (in >90% of children), much more common at sacral than iliac SIJ margins (72% versus 16%), and gradually fades away with age, almost disappearing after the closure of the segmental apophyses. If not recognized as a normal finding in children, the Assessment of Spondyloarthritis International Society (ASAS) criteria for a positive MRI can even be erroneously considered to be fulfilled. Unusual patterns that are suspicious for true BME and sacroiliitis are when the high T2/STIR signal is observed only at the iliac side, when it is more intense at the iliac than on the sacral side, when there is a definite difference between left and right side, or when there is definite high T2/STIR signal of any pattern in adolescents after apophyseal closure.12,14 In those cases, the signal changes are less likely to be normal.

Normal variability of pediatric sacroiliac joints on STIR images. (a) Semi-coronal STIR image in a 13-year-old normal girl – sent to MRI for other reasons – showing normal sacroiliac joints with subchondral high signal (‘flaring’) along the lateral apophyses of the sacrum (arrows). Note also the increased ‘fluid-like’ signal in the joint space of pediatric sacroiliac joints, most prominently seen here in the left joint (arrowheads). This again is a normal variant and should not be confused with joint space inflammation. (b) Semi-coronal STIR image in a normal 14-year-old girl illustrating vascular channels abutting the superior edge of the joint, which can be misinterpreted as capsulitis. These vascular channels cross from the sacral to the iliac side and are mostly seen as a thin line at the cranial side of the joint, usually not continuous on one slice, and continuing beyond the margins of the joint capsule when scrolling through the images.
Also, a perceptible quantity of fluid can be present in the SIJ, as can be seen in other normal joints as well.13,15 In a study of 251 normal children, mildly increased T2/STIR signal – not as bright as fluid – was seen in the SIJ space in most children (>74% of children), probably mostly representing cartilage, whereas, in about 20% of children, this signal can be very bright, equivalent to fluid [Figure 3(a)]. There was no significant difference between girls and boys, although girls showed peak signals earlier than boys (10 versus 12 years old, respectively). 15 This high signal line does not necessarily imply joint space inflammation as a sign of sacroiliitis. If the high signal line is thin, regular, and mostly symmetrical, and when there are no other signs of inflammation, this should be considered a physiological phenomenon. When in doubt, contrast administration may help to confirm or exclude joint space inflammation.
Another possible pitfall is a misinterpretation of vascular channels abutting the superior edge of the joint as capsulitis.9,11 Vascular channels cross from the sacral to the iliac side and are mostly seen as a thin line at the cranial side of the joint, usually not continuous on one slice, and continuing beyond the margins of the joint capsule when scrolling through the images [Figure 3(b)].
Normal variability on T1
Detecting erosion in children can also be challenging due to normal variability.9,16 During the ossification process, the bony cortex is not fully ossified and may not appear as a black line on T1-weighted MRI, which is even further emphasized by the fact that the underlying bone marrow in children is still mainly red and thus has relatively low T1 signal, resulting in a lower contrast between cortex and bone marrow. Furthermore, the SIJ articular margins often appear blurred or irregular in children, findings that can make it very difficult to detect erosions, or can even mimic erosions [Figure 4(a)]. In a study of 251 normal children, the cortical black line was partially absent in >85% of children, blurred in 34.7%, and irregular in 41.4%. All these features were most common on the iliac side of SIJ and at the first sacral vertebral level. These findings are in contrast to adults, where the subchondral bone plate appears as a regular, sharply defined, thin black line [Figure 4(b)]. Clearly visualized, sharply delineated SIJ like in adults were seen in only 8.0% of children. 16 At least two-thirds (65%) of normal pediatric SIJ showed at least one feature that was a component of the adult definition of SIJ erosions, risking overdiagnosis of sacroiliitis. The ASAS adult definition of erosion 17 includes a defect in the subchondral bone with full thickness loss of the dark appearance of the subchondral cortex at its expected location and loss of signal intensity on T1 compared with the normal bright appearance of adjacent bone marrow, criteria that can be fulfilled if the (partially) absent cortical black line, blurring, and irregularity are not recognized as normal findings in children, risking overdiagnosis of erosions in children. 16

Normal variability of pediatric sacroiliac joints on T1-weighted images. Semi-coronal T1-weighted images of (a) a normal 15-year-old boy showing irregular articular surfaces on the sacral and iliac side of both sacroiliac joints (white arrows) and blurred iliac articular surface of the left sacroiliac joint (arrowheads), which is in contrast to adult sacroiliac joints, shown here in (b) a normal 21-year-old man, where the subchondral bone plate appears as a regular, sharply defined, thin black line (black arrows).
Other mimickers of erosion are articular defects, the so-called joint facet defects, which are also known as normal variants and frequently seen in pediatric SIJ [Figure 5(a)]. 18 In case of a joint facet defect, there are no other features of sacroiliitis, no surrounding BME, fat lesion, or sclerosis. Intra-articular ossified nuclei are also normal in children and should not be confused with pathology [Figure 5(b) and (c)]. They are frequently seen after the age of 13 years and can persist up to the age of 18 in both genders. 18

Other normal variants in pediatric sacroiliac joints. (a) Semi-coronal VIBE image in a 16-year-old girl illustrating a joint facet defect (arrow), a known normal variant in the pediatric sacroiliac joint that can mimic erosion. (b, c) Semi-coronal synthetic CT images in (b) a 13-year-old boy and (c) a 15-year-old girl showing intra-articular ossified nuclei (arrows), another normal variant that should not be confused with pathology. Intra-articular ossified nuclei are frequently seen in children after the age of 13 years and can persist up to the age of 18 in both genders.
Normal variability on contrast-enhanced sequences
Most normal pediatric SIJ will exhibit a thin rim of mild contrast enhancement at the bone/cartilage interface on post-contrast T1-weighted images, which is a normal, growth-related physiological phenomenon that should not be mistaken for joint inflammation [Figure 6(a) and (b)]. 15 Possible explanations for this thin enhancing line are enhancement of vascular structures or fibrovascular tissue, enhancement of the primary spongiosa of newly formed bone, or diffusion of contrast into the joint space. True inflammation can mostly be recognized as more focal, intense, and thick enhancement.10,15

Normal variability of pediatric sacroiliac joints on contrast-enhanced T1-weighted images. Semi-coronal contrast-enhanced fat-saturated T1-sequences in normal sacroiliac joints of (a) a 13-year-old girl and (b) a 14-year-old boy, showing a thin rim of mild contrast enhancement at the bone/cartilage interface along iliac and sacral borders of both sacroiliac joints (white arrows), which is a normal, growth-related physiological phenomenon that should not be mistaken for joint inflammation. Note also the vascular channels abutting the superior edge of the joint (black arrows), seen as a thin, enhancing line crossing from the sacral to the iliac side, which should not be confused with capsulitis.
Vascular channels, which can be clearly visualized on contrast-enhanced sequences, should not be confused with capsulitis [Figure 6(b)]. Vascular channels can be seen as a thin, enhancing line at the cranial side of the joint, crossing from the sacral to the iliac side, and not usually continuous on one slice.10,15
Normal findings in adults
Normal joint findings by MRI
The superior visualization of the bone marrow and soft tissue structures by MRI is an advantage in the diagnosis of sacroiliitis. However, features occurring as part of sacroiliitis such as BME, fat deposition, erosion, sclerosis, and joint space alterations may also occur in healthy individuals. MRI signal intensities in the bone marrow vary in healthy individuals both on STIR/T2FS and T1-weighted sequences,19,20 and there may be areas conforming to BME as well as fat deposition. In a study of 95 healthy individuals aged 20–49 years, BME was detected on coronal STIR sequences in all age groups, though with an increasing prevalence with age from 13.9% in the age group 20–29 years to 35.7% in individuals ⩾40 years. 19 However, the extent of BME was limited, and only one subject (2.8%) in the age group 20–29 years had a positive MRI for active sacroiliitis according to the ASAS definition, but 16.1% and 17.2% of the individuals ⩾30 and ⩾40 years old, respectively, met the ASAS definition. 21 However, deep (>1 cm) and intense BME (brighter than vascular structures or intervertebral disk) was relatively rare, detected in four and six persons, respectively, ⩾30 years except for one below 30 years. The BME was most frequent at the superior portion of the sacrum (both anterior and posterior) followed by the inferior ilium (Figure 7). A comparable prevalence was reported in a study by de Winter et al., 22 including 47 healthy individuals aged 18–45 years (mean 31 years). In this study, 23.4% had BME fulfilling the ASAS criteria for sacroiliitis, most frequently located to the inferior ileum, but deep and intense BME did not occur. Thus, BME as a normal finding is often limited in extent and intensity. The frequent location of BME to the upper sacrum and/or inferior ileum indicates that it may be induced by strain. 23
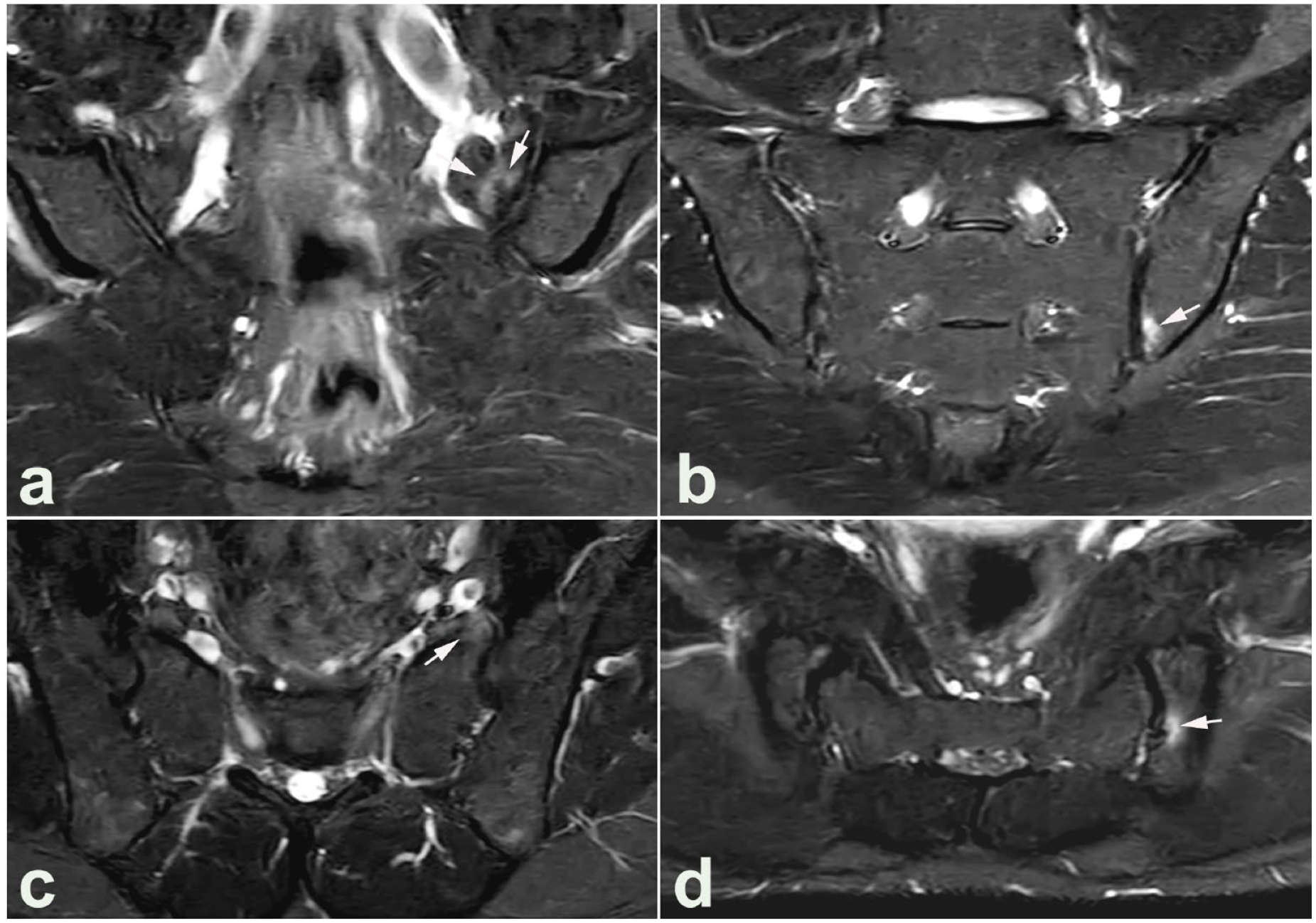
Non-inflammatory subchondral BME. MRI in a healthy man in his mid-30s with physically demanding work including heavy lifting; no clinical or biochemical signs indicating axial spondyloarthritis. The upper image row represents semi-coronal STIR images, at the anterior part of the joint (a) and posteriorly (b), showing subchondral BME anteriorly in the sacrum and posterior–inferiorly in the ileum (arrows), location indicating non-inflammatory BME due to strain. (c, d) Semi-axial slices correspond to the areas with BME on the coronal slices and confirm the presence of BME in both areas (arrows).
In the study of 95 healthy subjects, fat deposition in the bone marrow was detected on T1-weighted images in 13.7% across all age groups, increasing from 8.3% in the age group 20–29 years to 19.3% and 14.3% in the age groups 30–39 and 40–49 years, respectively. 19 However, none of the healthy subjects aged 20–29 years had fat deposition in three or more of the scoring areas (⩾3 quadrants 24 ); this occurred in 6.5% and 7.1% of the subjects aged 30–39 and 40–49 years, respectively. 19 The frequency of fat deposition was reported higher in a study of 485 non-rheumatological subjects without SIJ-related disorders. The fat deposition was observed in 50.6% in the age groups <45 years increasing to 94.4% in individuals ⩾75 years. 25 However, the fat deposition in non-rheumatological subjects had a patchy distribution without manifest subchondral areas with well-defined and well-demarcated fat deposition as in ankylosing spondylitis (Figures 8 and 9).19,25,26 The observed predominantly focal or patchy fat depositions can be considered non-inflammatory findings, especially seen in a degenerative setting and older healthy individuals.

Non-inflammatory fat deposition. (a) T1-weighted coronal MRI image in a man in his late 30s without sacroiliac joint disorder showing slight non-inflammatory subchondral fat deposition. (b) T1-weighted image for comparison shows the characteristic fat deposition in ankylosing spondylitis (slim long arrows).

Non-inflammatory subchondral sclerosis. MRI in a woman in her late 20s with hip dysplasia, but no symptoms or signs indicating sacroiliac joint disorder. (a) Semi-coronal T1-weighted and (b) T1FS image show subchondral iliac sclerosis at the upper part of the right SIJ (arrowheads) with concomitant slight fat deposition and also a small sacral osteophyte (arrows). Besides, there are irregular joint facets on the left side, but no erosions and there was no detectable BME (not shown). (c) CT reconstructions performed based on the pelvic CT obtained due to the hip dysplasia, semi-coronal and two semi-axial slices at the middle part of the joints more clearly show the sacral osteophyte superiorly. The axial slices in addition show small osteophytes located anteriorly at the sacrum and posteriorly at the ileum (arrows).
Erosions or erosion-like lesions can also be normal findings, probably because it may be difficult to distinguish irregular joint facets as part of strain-related or degenerative changes from erosions involved in sacroiliitis using MRI. The reported frequencies have varied. In the study of 95 healthy subjects, SIJ erosions were detected across all age groups in 20%, increasing from 9.7% to 13.9% in individuals aged <40 years to 39.3% in individuals aged ⩾40 years. 19 However, none of the healthy subjects aged 20–29 years met the proposed structural criteria for axial spondyloarthritis (axSpA) sacroiliitis using cutoff values for erosions and fat metaplasia with a specificity ⩾95% for axSpA (erosions in ⩾3 quadrants, fat metaplasia in ⩾3 quadrants, or erosions and/or fat metaplasia in ⩾5 quadrants 24 ); however, 17.9% of individuals aged ⩾40 years had erosions in ⩾3 quadrants. 19 In contrast to these findings, erosions were uncommon in the study group of 485 non-rheumatological patients, observed in 0.6% of patients <45 years of age and in 2.6% of the entire study group. 25 Thus, the definition and evaluation of erosions have varied. It is uncertain if the possibility of irregular joint surface due to degenerative and strain-related changes has been taken into account (Figure 9).
Subchondral sclerosis at the SIJ can be a normal finding. Sclerosis according to the ASAS definition24,27 (very low signal intensity on all sequences located in a typical subchondral area with a depth > 5mm in the ileum and >3 mm in the sacrum) was seen in 2.1% of the 95 healthy individuals without relation to age. 19
Prevalence was higher in the 485 non-rheumatological patients without SIJ-related symptoms where sclerosis was detected in 13.7% of the participants (females: 16.3%, males: 11.2%), being present in 9.8% aged <45 years and in 15.8% aged ⩾45 years. 25 The presence of osteophytes was also analyzed in this study and found to be present in 37% of the population, in 20.0% of individuals below the age of 45 years, and 46.2% of individuals aged above 45 years. 25 To our knowledge, the presence of osteophytes has only been described in one other MRI study with concomitant synthetic computed tomography (CT). 28 In this study involving 210 patients with clinically suspected sacroiliitis aged 18–74 years, signs of joint degeneration was the most frequent incidental finding, observed in 66.6%; 182 osteophyte formations were detected, but only 55% of them were visible by MRI. The use of cartilage sequences may improve the visibility of osteophytes (Figure 9).
MRI data regarding normal joint space width are scarce, probably because it is difficult to measure the space on T1-weighted sequences. The use of a cartilage sequence can facilitate it, but it may still be difficult to estimate the joint space width as it varies through the joint. Data regarding SIJ joint space have mainly been based on CT studies,6,7 and there are seemingly no valid data regarding normal joint space width visualized by MRI.
Morphological SIJ findings
The most frequent morphological SIJ findings causing diagnostic problems in the assessment of potential sacroiliitis are anatomical variants and strain-related or degenerative changes.
Normal joint variants
During the last 5 years, there has been a focus on normal SIJ variants by both CT and MRI because they can confuse when assessing the joints. Besides, variants seem to occur with increased frequency in patients with mechanical back pain 29 and may also influence the imaging findings in axSpA.30,31 Seven well-defined normal SIJ variations have been described: accessory SIJ, iliosacral complex, bipartite iliac bone plate, crescent-like articular surface, semicircular defects, ossification centers at the sacral wings, and dysmorphic cartilaginous joint facet (Table 1).29,31–39
Frequencies of normal variants in studies of individuals without symptoms or signs indicating sacroiliac joint disorders, percent of study subjects.

CT, computed tomography; f, females; m, males; f > m, frequency higher in females than in males; m > f, frequency higher in males than in females; MRI, magnetic resonance imaging.
Accessory SIJ is an additional joint located posteriorly within the ligamentous joint compartment with congruent joint facets covered by hyaline cartilage or fibrocartilage (Figure 10). It has been reported in 4.5–26% of study subjects without SIJ disorders29,31–39 (Table 1) and seems to occur equally frequently in both genders, though with a female predominance in one study. 37 The frequency has in some studies been reported to increase with age32,33,35,38 and be highest in obese persons and women with three or more childbirths.32,33 There may be concomitant BME and sclerosis, not only adjacent to the accessory joint but also in the SIJ,31,36,39 and the variant may be accompanied by pain.33,36,38 The presence of an accessory joint may therefore simulate sacroiliitis both by MRI and clinically.

The anatomical variants, are accessory sacroiliac joint, bipartite iliac bone plate, and semicircular defect. Semi-coronal STIR and T1-weighted MR images at the anterior (a, b), middle (c, d), and posterior (e, f) part of the joints with supplementary semi-axial STIR slices at the upper (g), middle (h), and lower (i) part of the joints in a woman in the early 40s without sacroiliac joint disorder. Accessory sacroiliac joints are seen in the ligamentous joint compartment located posteriorly at the inferior part of the joints (arrowheads). There are no concomitant subchondral BME corresponding to these joints, but subchondral edema anteriorly in the sacrum on the left side (arrows). The bipartite iliac bone plate is easily detected on the semi-axial slice (long slim arrows). On the semi-coronal slice, it gives rise to increased signal in the joint spaces inferiorly with localized round edematous areas (long slim arrows) not to be mistaken for intraosseous edema. The semicircular defects (asterisk) are filled with vascular structures giving rise to an increased signal, but there is no subcortical edema indicating enthesitis.
Iliosacral complex is a focal osseous protrusion of the iliac bone in the ligamentous joint compartment accompanied by a corresponding groove in the opposing sacral bone without the presence of a visible accessory joint. It usually occurs at the level between the first and second sacral segments. Detected frequencies have varied (Table 1). It seems most frequent in females29,31–37,39 although there was a male predominance in one group. 32 As there is no direct contact between the ileum and sacrum, this variant is not associated with adjacent significant subcortical BME or structural changes, but may be associated with low back pain and subchondral BME in the cartilaginous joint compartment 36 as well as degenerative SIJ changes, 34 and has been observed frequently in patients with mechanical back pain. 29
The bipartite iliac bony plate has a cleft-like appearance in the posterior part of the iliac bone due to a deep insertion of a distal portion of the posterior sacroiliac ligament (Figure 10). It is most frequent in women.29,31–37,39 The cleft-like appearance is easily detected on axial slices, but on coronal slices, the channel parallel to the joint space filled with vessels may potentially simulate inflammatory changes29,31–37,39 (Figure 10). The variant has been reported associated with an increased frequency of subchondral sclerosis anterior–superiorly in the ileum, 37 and has been observed to occur frequently in patients with mechanical back pain. 40
The crescent-like iliac bony plate is a concave configuration of the iliac bone with relatively congruent bulging of the opposite sacral bone located at the superior ligamentous joint compartment [Figure 2(c)]. It is a relatively rare finding and most common in women.29,31–37,39 The appearance and thereby the detected frequency partly depend on the slice orientation and technique used. 36 The variant has been observed to occur frequently in patients with mechanical back pain. 40
Semicircular defects are round well-defined defects in the sacral and/or iliac bone located in the upper part of the ligamentous joint compartment (Figure 10), which seem to be most frequent in females.32,35,39 As there is no direct contact between the ileum and sacrum, this variant is not associated with adjacent significant BME or structural changes, but vessels in the defect may be mistaken for enthesitis by MRI. 39
The persistence of ossification centers at the sacral wings appears as triangular osseous bodies in the superior posterior region of the joint. They are relatively rare, reported present in 0–5% of study subjects29,31–37,39 and mostly seen in young individuals aged <30 years.36,37 Persistence of non-fused nuclei in other areas of the joint, especially anteriorly between the first and second sacral segment can also occur and cause confusion and/or simulate scaroiliitis. 41
Dysmorphic SIJ changes are focal protrusion of the iliac or sacral joint facet in the cartilaginous joint compartment with a corresponding groove in the opposite joint facet (Figure 11). It has only been reported in MRI studies where the variant was detected in 14–21% of the study subjects.36,39 It seems to be more common in women than in men,36,39 and is often accompanied by subchondral BME simulating inflammatory changes (Figure 11). Besides, the changes may be accompanied by pain,36,41 and thus difficult to differentiate from sacroiliitis changes.36,41

Dysmorphic joint changes. MRI in a young healthy volunteer postpartum woman, semi-coronal STIR, and T1-weighted image (a, b) showing dysmorphic SIJ changes on the left side with the ileum protruding into the sacrum accompanied by BME in the sacrum adjacent to the dysmorphic changes (arrows), and also a subchondral cyst inferiorly in the ileum probably elicited by strain. The two semi-axial STIR slices (c, d) show that the BME (arrows) is located posteriorly at the border between the cartilaginous and ligamentous joint compartments.
The reported frequencies of the different variants have varied considerably (Table 1), which can be due to different compositions of study populations, but also to the definitions used and the possibility of recording the simultaneous occurrence of more than one variant, 36 a finding also noticed in a study of axSpA patients 30 and illustrated in Figure 10. There is a need for a uniform definition of the different variants and evaluation of their clinical significance.
Anatomical variation in the area of the SIJ also includes the lumbosacral transitional vertebra. This is a common variation with a wide variety of morphologies ranging from broadened transverse processes to complete fusion occurring bilaterally, symmetrically, or asymmetrically as well as unilaterally. 42 Transitional vertebrae have been observed in up to 25% of the population 43 and may be accompanied by low back pain, especially if there is a persistent cleavage between the transverse process and the upper border of the sacrum (Castellvi type I and type II 42 ). Concomitant BME, fat deposition, and/or sclerosis may occur but are usually confined to pseudo-articulations and rarely reach the SIJ, leading to confusion with axSpA sacroiliitis changes 43 (Figure 12).

Lumbosacral transitional vertebra. MRI in a male in his early 20s with low back pain for 6 months, but no clinical or biochemical signs indicating axial spondyloarthritis, semi-coronal STIR (a) and T1-weighted (b) image showing lumbalization of S1 with a pseudo-articulation between the right-sided transverse process and the upper surface of S2 with concomitant slight subchondral edema (arrow on STIR) and also fat deposition (arrow on T1). There are also disk degenerative changes at the L5/S1 intervertebral space with subchondral edema (long slim arrow on STIR).
Strain-related SIJ changes
BME changes at the SIJ have been reported in healthy individuals, especially sports-active persons and military recruits, and are therefore probably induced by strain.22,23,44,45 Frequencies as high as 41% have been observed, and it can be expected that a relatively large proportion of individuals without SIJ disorders have non-inflammatory subchondral BME at the SIJ (Figure 7). The BME observed in healthy individuals has usually been minimal compared to BME in axSpA. A study by de Winter et al. 22 reported changes to be highly suggestive of axSpA according to the ASAS criteria 21 in 12.5% (3/24) of runners and 23.4% (11/47) of healthy volunteers compared with 91.5% (43/47) of patients with axSpA. 22 However, deep BME lesions were not found in runners or healthy volunteers, but were observed in 89.4% (42/47) of patients with axial SpA. 22 Corresponding results based on semi-coronal images were obtained in a study of military recruits without back pain. Among these, BME fulfilling the ASAS MRI criteria before and 6 weeks after intensive physical training was seen in 22.7% (5/22) and 36.4% (8/22), respectively. 45 In another study also based on semi-coronal MR slices, BME at the SIJ fulfilling the ASAS 2009 criteria was detected in 35% (9/20) of healthy hobby runners and in 41% (9/22) of ice hockey players, most frequently located in the posterior lower ilium followed by the anterior upper sacrum. 23 However, concomitant use of semi-axial STIR images reduced the detection of subchondral BME in the lower posterior ileum because the axial slices visualized some of the BME changes to be due to partial volume effect of vascular signals, deep iliac ligament insertion containing vascular signals, or fluid-filled bone cysts giving the impression of SIJ BME on semi-coronal images. 46 The reduced frequency of BME in the lower ileum by two-plane assessment implied that the anterior sacrum was the most frequent site of strain-related BME, which was located in the middle portion of the joint on axial slices.
Data regarding strain-related structural changes have varied. In the study of hobby runners and ice hockey players, erosions were rare with only one erosion detected in three runners and one ice hockey player, respectively. 23 However, erosions were frequently detected in the study of military recruits; 27.2% (16/22) had structural lesions both at baseline and follow-up, 13.6% had erosion-like lesions, 13.6% fat metaplasia, and 4.5% sclerosis, respectively.
The findings in healthy individuals and persons with strain-related or degenerative SIJ changes underscore the importance of interpreting SIJ MRI findings in the appropriate clinical context, in young active individuals, as well as middle-aged and elderly persons. Thus, age, history, clinical features, topographic location/distribution of BME, and concomitant structural changes should be considered, keeping in mind that non-inflammatory BME is most common in the anterior middle portion of the joint.40,46–48
Degenerative SIJ changes
Degenerative SIJ changes without symptoms referable to the SIJ are frequent in middle-aged and elderly individuals, but signs of degenerative SIJ changes can occur already in the 20s, tend to progress with age, and are probably the result of strain.6,7,37,49,50 The detection of degenerative changes has mainly been based on CT studies of individuals without symptoms or signs of SIJ disorders.6,7,37,49,50 Diagnostics of degenerative changes may be difficult by MRI due to its poorer visualization of minor osseous changes such as osteophytes. Thus, in a recent MRI study with additional synthetic CT images, 45% of the osteophyte formation detected by CT was not visible by MRI, but sclerosis unrelated to axSpA was visible by both MRI and CT in 97.7% of the study subjects. 28 To our knowledge, the presence of osteophytes has only been systematically analyzed in one further MRI study. This study reported osteophytes in 37% of 485 non-rheumatological patients, and 20% and 46% of individuals aged below and above 45 years, respectively. 25 Degenerative changes can be accompanied by subchondral BME as well as sclerosis and fat deposition 25 causing a risk for misinterpretation as inflammatory changes by MRI. Supplementary CT may sometimes be necessary to diagnose and elucidate degenerative SIJ changes (Figure 9). Besides, the SIJs are visualized by pelvic CT performed on other indications. Thus, knowledge about the presence and appearance of degenerative SIJ changes by CT is important also considering that low-dose CT is increasingly used to detect early structural sacroiliitis changes.
The overall frequency of degenerative changes detected by CT has been reported in two studies involving 373 [aged 16–96 years (mean 57.7)] 50 and 95 [aged 19–72 years (mean 42)] 49 participants, respectively. The overall frequencies of slight and substantial/severe degenerative changes were rather similar in the two studies, 64.9%/66.3% and 31.1%/24.2%, respectively, but there were substantial differences in individuals below the age of 40 years with slight and substantial/severe degenerative changes detected in 20.4%/67.7% and 3.0%/8.1%, respectively.49,50 Some of these differences may be the result of different gradings or definitions of degenerative changes, but the CT techniques used probably play an important role. The lowest frequencies were based on axial single slice CT, 50 whereas the highest frequencies were based on helical CT with reconstructions making it possible to detect osteophytes and joint space narrowing in different planes. 49 Technical aspects have probably also influenced the results of studies analyzing the presence of the different features related to degenerative SIJ changes, sclerosis, osteophytes, joint space narrowing, subchondral cysts, and erosion-like lesions (Table 2). The frequencies were across all ages higher in the study based on helical CT 49 than in two previous studies based on the axial single-slice CT technique.6,7 The frequencies were also high in a recent study based on isotropic CT 37 (Tables 2 and 3).
Overall frequencies of features related to degenerative sacroiliac joint changes by CT in individuals without SIJ disorders, percent of study subjects, or joints.
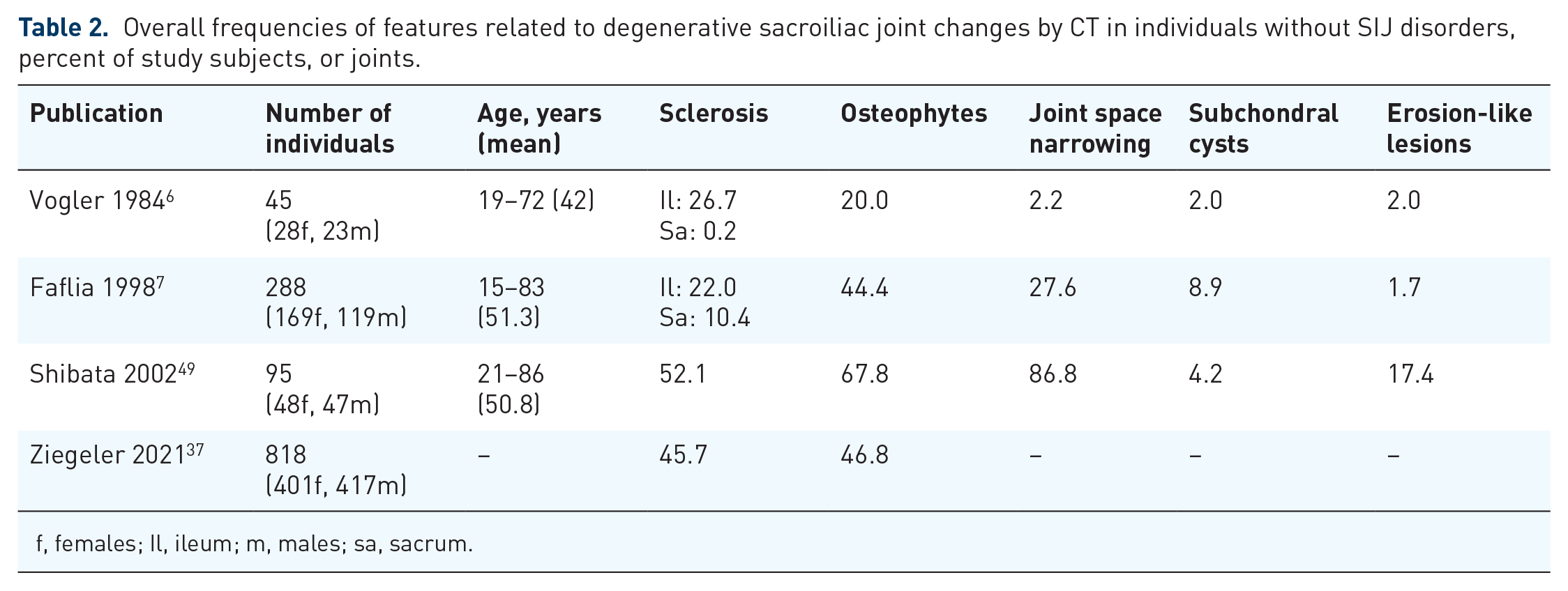
f, females; Il, ileum; m, males; sa, sacrum.
Frequencies of features related to degenerative sacroiliac joint changes by CT in individuals without SIJ disorders, divided into age groups, below and >40 years in two studies and below and >45 years in one study; percent of study subjects, or joints.

CT, computed tomography; f, females; Il, ileum; m, males; sa, sacrum; SIJ, sacroiliac joint; Yrs, years.
Normal values for subchondral sclerosis in individuals below the age of 40 years have in two CT studies been established to be ⩽5 mm in the ileum and ⩽3 mm in the sacrum,6,7 a definition also used by ASAS for sclerosis by MRI. 17 The overall frequency of iliac sclerosis and sacral sclerosis conforming to a depth >5 and >3 mm, respectively, was in two study groups 22.0–26.7% in the ileum and 0.2–10.4% in the sacrum6,7 (Figure 9). In another two studies, sclerosis was reported in 46–52% of the study subjects without division into iliac and sacral sclerosis37,49 (Table 2). The frequency of sclerosis increased substantially with age (Table 3), but sclerosis may be seen already in the 20s as observed in 17–23% of individuals without SIJ disorders.37,49
Normal values for the joint space width have been established in two CT studies to be ⩾2 mm in individuals below the age of 40 years.6,7 Joint space width was observed to decrease with increasing age, with mean values of 2.3 ± 0.4 and 1.9 ± 0.2 mm before and after 40 years of age, respectively. 7 The overall frequency of joint space narrowing has varied considerably and the frequency is generally substantially increased with age (Tables 2 and 3, Figure 13). Likewise, the overall reported frequency of osteophytes has varied considerably, but in all studies, the frequency increased with age6,7,37,49 (Tables 2 and 3, Figures 9 and 13).
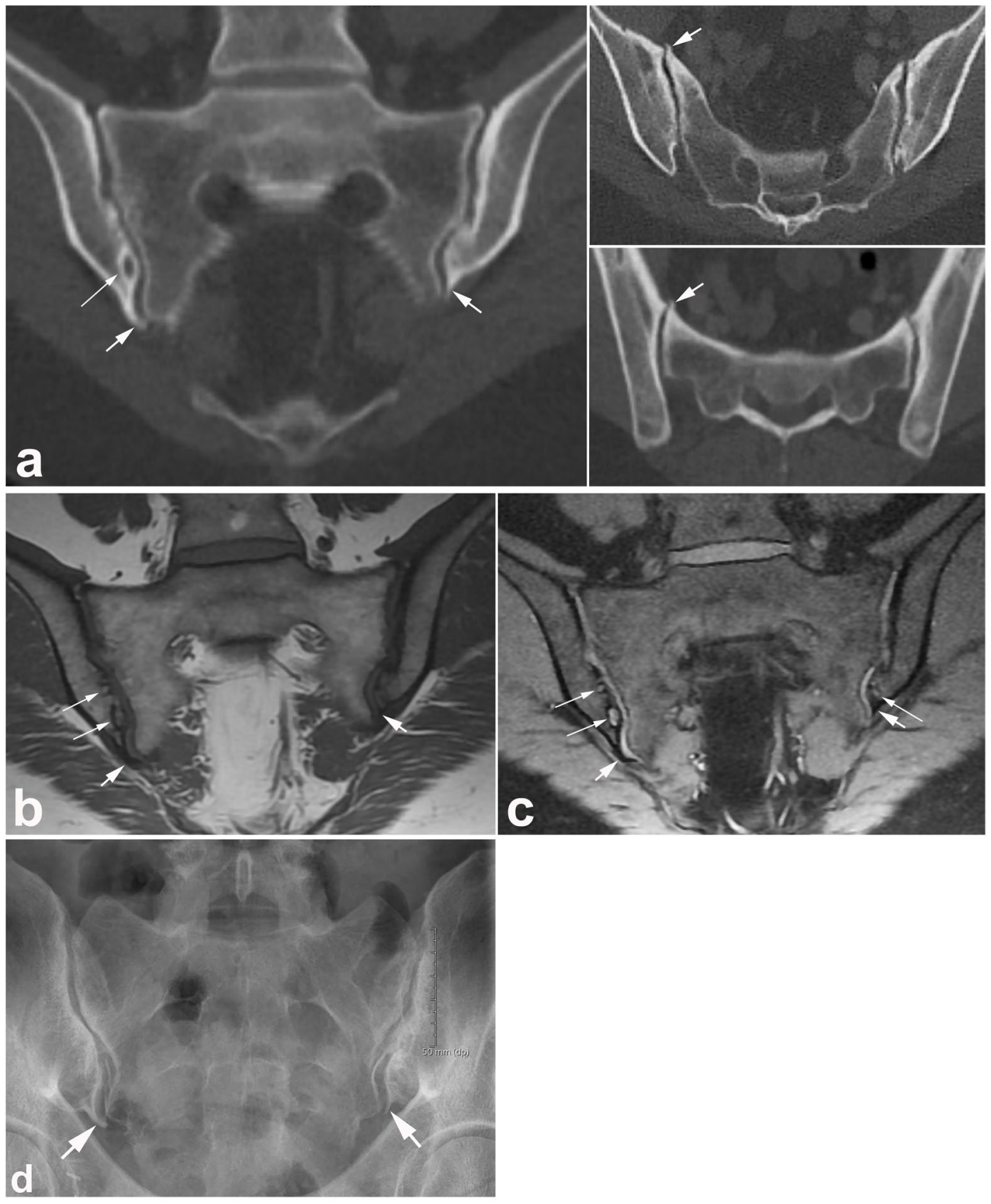
Manifest degenerative changes. (a) CT images in a woman in the early 50s with low back pain and disk degenerative changes, but no clinical or biochemical signs indicating axial spondyloarthritis; semi-coronal reconstruction on the left and a straight axial slice and a semi-axial CT reconstruction on the right, showing the presence of osteophytes at the inferior joint margins (thick arrows) in addition to subchondral cysts (long slim arrows). The axial slices also show osteophytes anteriorly (arrows) and concomitant joint space irregularities with subchondral sclerosis, especially anteriorly in the sacrum on the right side. (b) Semi-coronal T1-weighted and (c) T1FS MR images detect the osteophytes inferiorly at the ileum (thick arrows) and also subchondral cyst formation (long slim arrows). Although the osteophytes are difficult to see in the T1 images, they are clearly delineated in the T1FS image. (d) SIJ radiograph also visualizes the osteophytes inferiorly (arrows) and irregular joint spaces with subchondral sclerosis and narrowing, especially on the right side.
Subchondral cysts have generally been rare findings and the overall frequency of erosion-like lesions has varied considerably (Tables 2 and 3).6,7,49 However, erosions seem to be rare below the age of 40 years and two studies reported no erosions below the age of 30 years,7,49 compared with erosions reported in 2–22% of individuals above the age of 40 years.6,7,49 Intraarticular ankylosis was not reported, but para-articular synostosis due to bridging bone formation was reported in 6.9–9%.6,7
Degenerative SIJ changes have been reported more frequently in women than in men, 49 partly because pregnancy seemed to accelerate degenerative changes.7,49 The number of pregnancies has been reported to impact the degree of sclerosis, osteophytes, and para-articular ankylosis, 7 but the first pregnancy may have the greatest effect on the SIJ. 49 Obesity may also play a role7,37 although one study could not confirm this. 49
The anatomical location of degenerative changes has been analyzed in two studies both reporting sclerosis and osteophytes to be most frequent in the middle portion of the joint, especially anteriorly.37,49 The presence of sclerosis and osteophytes was in one study analyzed in relation to anatomical variants. Sclerosis was found to be rather frequent anteriorly in persons with bipartite iliac variant, and anterior as well as posteriorly in persons with accessory joints; posteriorly may correspond to the accessory joint. These two variants were found to be related to posterior osteophytes. This indicates that these variants may imply strain to the joint causing subchondral sclerosis and an atypical location of osteophytes.
Degenerative changes corresponding to those observed by CT may also be detected by MRI, especially if the semi-coronal T1-weighted sequence is supplemented with a cartilage sequence, improving the visibility of osteophytes (Figures 9 and 13). Joint space alterations and osteophytes at the inferior border of the joint can also be detected by conventional radiography, but CT is more sensitive than radiography in detecting subtle SIJ abnormalities such as subchondral cysts (Figure 13).51,52 and can detect para-articular bridging osteophytes, which may be misinterpreted as joint ankylosis on conventional radiography.
Importantly, degenerative SIJ changes are frequently incidental findings, especially in middle-aged and elderly persons. They can cause confusion when interpreting the joints, but their clinical significance is currently unknown and should be evaluated.
Conclusion
The SIJ has a complex anatomy with wide variations and a frequent occurrence of anatomical variants. The SIJ is also subject to considerable strain, which can result in non-inflammatory subchondral changes such as BME, sclerosis, and fat deposition in addition to signs of degenerative joint changes. In children, interpretation of SIJ MRI is particularly challenging due to normal physiological changes during skeletal maturation which can simulate disease. Knowledge about the wide range of normal findings is important to avoid misinterpretation of findings as pathological.