
Abstract
Background:
The mechanism explaining low cholesterol concentrations in chronic inflammatory rheumatic disease (CIRD) is incompletely understood. We hypothesized that chronic inflammation impairs the functionality of high-density lipoprotein (HDL), for example, by oxidative processes.
Objectives:
Assessment of oxidized HDL (HDLox), a marker of dysfunctional HDL, in newly diagnosed patients with CIRD before and after initiation of immunosuppressive therapy and comparison of HDLox values of patients with CIRD to non-CIRD controls.
Design:
Prospective observational trial.
Methods:
The study was conducted on 44 newly diagnosed CIRD patients, who were initiated on immunosuppressive therapy (baseline). A total of 136 patients without CIRD served as control. Lipid profiles including HDLox levels and C-reactive protein (CRP) were measured in both groups at baseline. In CIRD patients, measurements were repeated 12 weeks after baseline. Validated outcome tools for disease activity and function were assessed at baseline and 12 weeks.
Results:
A total of 33 (75%) patients with rheumatoid arthritis, 7(16%) with axial spondyloarthritis, and 4 (9%) with systemic lupus erythematosus were included. Groups were comparable for age and BMI. CIRD patients had higher HDLox concentrations (1.57 versus 0.78, p = 0.02) and tended to have lower low-density lipoprotein cholesterol, HDL cholesterol, and cholesterol concentrations compared to controls. HDLox (1.57 versus 1.4, p = 0.26) and CRP levels (2.1 versus 0.7 mg/dl, p < 0.01) decreased in CIRD patients from baseline to follow-up.
Conclusion:
CIRD is associated with an impairment of the anti-inflammatory properties of HDL as reflected by an increase in HDLox concentrations. This effect may contribute to the increased cardiovascular risk in chronic inflammatory diseases.
Keywords
Introduction
Patients with chronic inflammatory rheumatic diseases (CIRD) like rheumatoid arthritis (RA), axial spondyloarthritis (axSpA), and systemic lupus erythematosus (SLE) are at increased risk of cardiovascular morbidity and mortality.1–4 The underlying mechanisms for this increased risk, as compared to the general population, are incompletely understood. It is well known, that alterations in the lipid profile are in general likely to contribute to atherosclerotic events, while chronic inflammation in CIRD decreases cholesterol and low-density lipoprotein (LDL)-cholesterol (LDL-C) concentrations. 5 This finding is known as the ‘lipid paradox’ in rheumatology and leads to inverse epidemiology: Patients with low cholesterol concentrations have the highest incidence of cardiovascular events. 6
In contrast to LDL-C, the effects of rheumatic diseases on high-density lipoprotein (HDL) concentration and function remain elusive. HDL particles have a broad spectrum of antiatherogenic properties including efflux of cellular cholesterol, vasodilation, reduction of apoptosis, anti-inflammatory effects, and diminishing platelet activation. 7 Following a ‘the higher, the better’ view, clinical and scientific concepts strongly focused on the quantity of HDL for decades and prompted the development of pharmacological interventions to increase HDL concentrations by inhibition of cholesteryl ester transfer protein (CETP). The disappointing results of the phase III trials of CETP inhibitors changed this view and moved the focus from HDL quantity to HDL quality. 8 Under particular circumstances, such as the oxidative environment of the acute-phase response, the HDL particles may lose their anti-inflammatory properties and become pro-inflammatory, 9 hence dysfunctional.
We hypothesized that chronic inflammation in rheumatic disease increases the level of dysfunctional HDL. Therefore, we compared oxidized HDL (HDLox) – as a measure of dysfunctional HDL – concentrations of therapy-naive patients with RA, axSpA, and SLE to non-CIRD controls. Moreover, we aimed to describe the course of HDLox concentrations after the initiation of anti-inflammatory therapy.
Methods
Study population and design
We conducted a prospective cohort study on patients with RA, SLE, and axSpA recruited from Rheumazentrum Ruhrgebiet, a tertiary care rheumatology center at Ruhr-University Bochum, Germany. The patients were continuously screened for inclusion and exclusion criteria as they presented to our outpatient clinic over a 6-month period. Study visits were conducted at baseline during hospitalization due to symptoms suspicious of CIRD and at week 12 during routine outpatient visits. In the case of patients newly diagnosed with CIRD, patients underwent a standardized physical examination by rheumatologists and laboratory tests according to a standard protocol. Inclusion criteria were established diagnosis of RA, axSpA, or SLE and an indication for treatment with conventional synthetic disease-modifying antirheumatic drugs. Exclusion criteria were age <18 years of age, advanced chronic kidney disease with an estimated glomerular filtration rate (eGFR) ⩽ 30 ml/min, and established immunosuppressive therapy.
The disease activity was assessed in patients with newly diagnosed RA and SLE by the 28-joint disease activity score, 10 and in patients with axSpA by the Bath ankylosing spondylitis disease activity index. 11 Physical function was assessed in both RA and SLE patients using the Funktionsfragebogen Hannover (FFbH), which was found to correlate well with the Health Assessment Questionnaire (HAQ). FFbH values are converted to HAQ values by the formula: HAQ score = 3.16 − (0.028 × FFbH score). 12 In patients with axSpA, physical function was assessed using the Bath Ankylosing Spondylitis Functional Index. 13
Patients diagnosed with RA (n = 33, 75%) received methotrexate and prednisolone, those diagnosed with SLE (n = 4, 9%) hydroxychloroquine and prednisolone and those diagnosed with axSpA (n = 7, 16%) nonsteroidal inflammatory drugs (NSAIDs) after baseline.
A total of 136 age- and sex-matched controls without any history of CIRD were recruited in the Department of Cardiology, University Hospital Brandenburg, Germany, and served as control. These patients were electively admitted to the hospital for cardiovascular diagnostics. An active or known inflammatory or rheumatic disease, history of cancer, coronary artery disease, diabetes, and current smoking were exclusion criteria for the control patients.
Demographic and clinical data, including comorbidities, laboratory parameters [lipid profile, C-reactive protein (CRP)], and medication of the patients were documented at their initial visit to the rheumatology center and, respectively, at the time of their visit to the cardiology clinic. Traditional cardiovascular disease (CVD) risk factors were assessed at the time of recruitment of patients in both groups. Hypertension was defined as blood pressure levels ⩾140/90 mmHg and/or the use of antihypertensive medication. Diabetes mellitus was defined as the presence of a physician-verified diagnosis and/or use of antidiabetic medication.
The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology statement. 14 Written informed consent was obtained from all participants before entry into the study. The study was performed by the Declaration of Helsinki and approved by the Ruhr-University Bochum ethics committee (ethics committee reference number: 19-6775) and the local ethics committees of the medical association of Brandenburg (Nr. AS69bB/2016).
Laboratory measurements
Lipid profile [LDL-C, HDL cholesterol (HDL-C), total cholesterol, and triglycerides] and CRP were measured in patients with CIRD before initiation of anti-inflammatory therapy (baseline) and also at 12 weeks thereafter (follow-up). Baseline concentrations of patients with CIRD were compared with non-CIRD controls.
Total cholesterol, LDL-C, HDL-C, triglycerides, and CRP were determined by validated standard clinical blood tests. LDL-C was measured using a photometric method analysis. HDLox was quantified using a fluorometric biochemical assay that measures HDL lipid peroxidation based on the oxidation of the fluorochrome Amplex Red.15,16 Shortly, serum was depleted from apolipoprotein B (ApoB) by polyethylene glycol precipitation. ApoB-depleted serum of 50 μl was then added to the wells of a 96-well plate in duplicate. The addition of 0.075 units per well of horseradish peroxidase and 50 µM Amplex Red reagent for a total volume of up to 100 µl catalyzes the reaction of Amplex Red to resorufin in combination with endogenous peroxides. After 1 h, the fluorescence of resorufin at wavelengths of 535/590 nm was determined using a Spark 10 M microplate reader (Tecan, Austria). Mean fluorescence from each sample was normalized by the mean fluorescent readout of the pooled control and HDL-C using the following calculation: ‘normalized’ oxidized HDL (nHDLox) = [HDLox_sample × 47 (mg/dl)]/[HDLox_control × HDL-C sample (mg/dl)], where 47 mg/dl represents HDL-C of the pooled serum control. Based on the last equation adjusting for the HDL-C level of each patient, the HDLox has no unit. nHDLox is simply referred to as HDLox throughout this article.
Statistical analysis
Data were tested for normal distribution and presented as mean and standard deviation. The numeric baseline data of the two groups were compared by the student’s t-test and dichotomic data by the chi-squared test. 17 Intraindividual changes in lipid concentrations before and after the initiation of anti-inflammatory therapy were analyzed by Wilcoxon paired tests. A two-sided p < 0.05 was regarded as significant. A multivariate regression analysis was performed using the level of HDLox as dependent variable and the concentrations of HDL-C, LDL-C, cholesterol, triglyceride, CRP, age, BMI, and smoking status as independent variables. Finally, subgroup analysis for RA patients was conducted.
Results
Serum was obtained from 44 patients with CIRD and 136 non-CIRD control patients. The demographic and clinical characteristics of the study population are presented in Table 1.
Epidemiological and clinical characteristics of the study population.
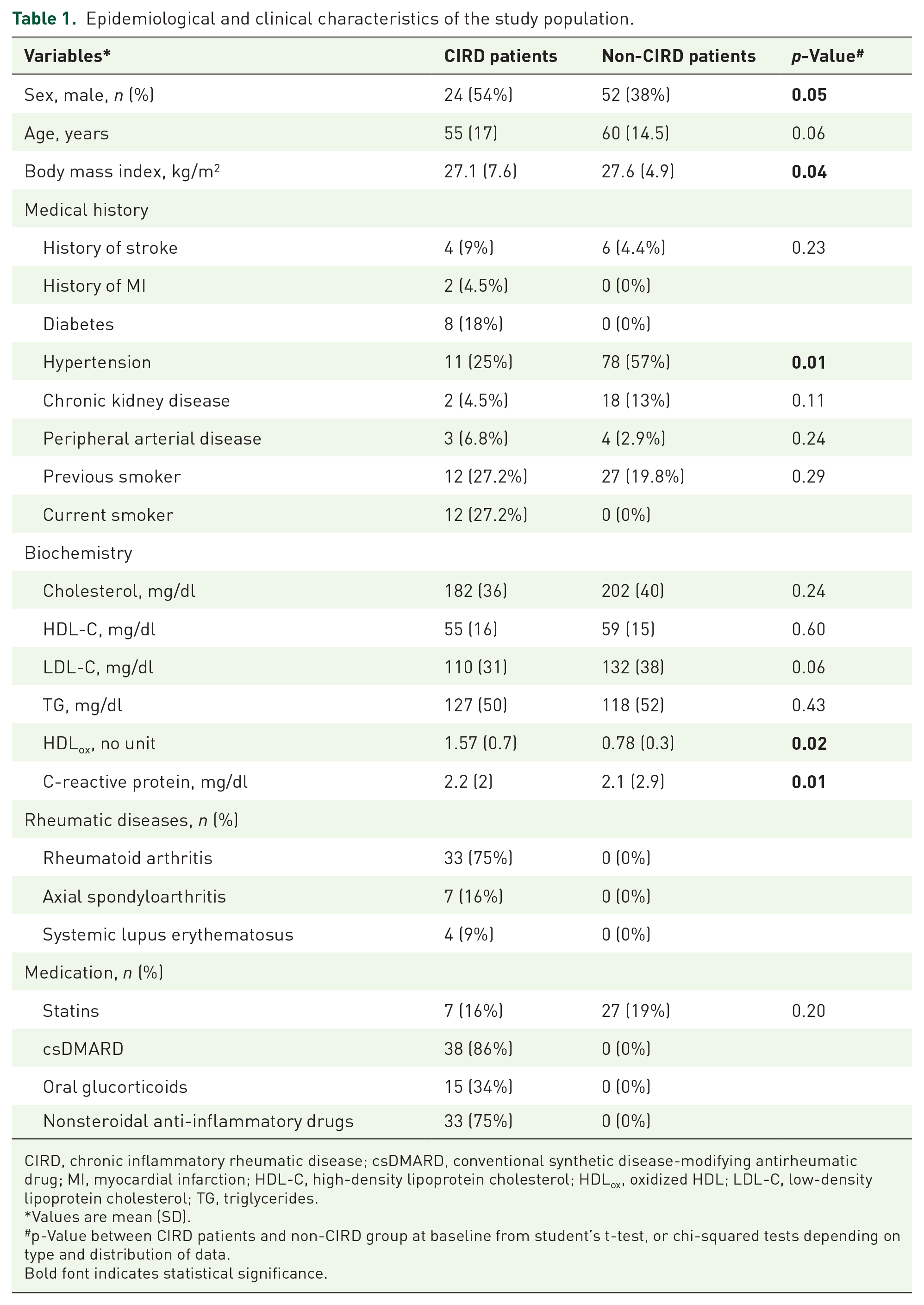
CIRD, chronic inflammatory rheumatic disease; csDMARD, conventional synthetic disease-modifying antirheumatic drug; MI, myocardial infarction; HDL-C, high-density lipoprotein cholesterol; HDLox, oxidized HDL; LDL-C, low-density lipoprotein cholesterol; TG, triglycerides.
Values are mean (SD).
p-Value between CIRD patients and non-CIRD group at baseline from student’s t-test, or chi-squared tests depending on type and distribution of data.
Bold font indicates statistical significance.
The CIRD patients group consisted of 33 (75%) patients with RA, 7 (16%) with axSpA, and 4 (9%) with SLE, with a mean age of 55 ± 17 years. All CIRD patients had moderate-to-low disease activity and limited impairment of physical function (Table 2).
Change of disease activity and physical function in CIRD-patients during follow-up.

BASFI, Bath Ankylosing Spondylitis Functional Index; BASDAI, Bath ankylosing spondylitis disease activity index; DAS-28, 28-joint disease activity score; HAQ, Health Assessment Questionnaire.
Values are mean (SD).
values are given as mean changes (SD).
p-value comparing differences between follow-up and baseline.
Bold font indicates statistical significance.
Among patients with CIRD, 34% were prescribed glucocorticoids and 75% were prescribed NSAIDs before they were diagnosed with CIRD. A total of 14 patients (RA: n = 13, SLE: n = 1) had been prescribed glucocorticoids prior to presentation at our clinic and had been taking them for a short period. No patient had been receiving therapy with glucocorticoids at the time of presentation at our clinic. A total of 34 patients (axSpA: n = 7, SLE: n = 4, RA: n = 23) have intermittent pain-adapted therapy with NSAIDs at the time of presentation. There were no differences in age between CIRD and non-CIRD patients. BMI was slightly but significantly higher in the non-CIRD group. Interestingly, there were slightly more male than female patients (54% versus 46%) in the CIRD group. Non-CIRD patients had a higher prevalence of hypertension and no history of myocardial infarction or diabetes (Table 1). Overall, 7 (16%) of CIRD and 27 (19%) of non-CIRD patients were on statin therapy (p = 0.20). None of the patients received other lipid-lowering drugs.
Cholesterol, LDL-C, and HDL-C were slightly higher and triglycerides were lower in the non-CIRD group compared to the CIRD group (Table 3). Patients with CIRD had higher HDLox values (1.55 versus 0.78, p = 0.02), and similar CRP values (2.2 versus 2.1 mg/dl, p = 0.01) compared to non-CIRD patients, respectively (Figure 1).
Serum lipid concentrations and C-reactive protein in patients with and without CIRD.

CIRD, chronic inflammatory rheumatic disease; HDL-C, high-density lipoprotein cholesterol; HDLox, oxidized HDL; LDL-C, low-density lipoprotein cholesterol.
Values are mean (SD).
p-Value between CIRD-baseline and CIRD-follow-up from Wilcoxon-test.
p-Value between CIRD- and non-CIRD group at baseline from student’s t-test.
Bold font indicates statistical significance.

Comparison of HDLox and CRP between CIRD and non-CIRD patients.
In patients with CIRD, a decrease in HDLox (1.57 versus 1.4, p = 0.26) and CRP (2.1 versus 0.7 mg/dl, p < 0.01) levels was observed at the follow-up visit compared to baseline values, although only the decrease in CRP values was statistically significant (Figure 2). Baseline HDL-C (55 versus 58 mg/dl, p = 0.04) and LDL-C (110 versus 111 mg/dl, p = 0.10) values in patients with CIRD did not differ from those at the follow-up visit, while cholesterol (182 versus 189 mg/dl, p = 0.01) and triglycerides (127 versus149 mg/dl, p = 0.14) values slightly increased at the follow-up (Figure 3). Subgroup analysis of RA patients revealed an HDLox level of 1.41 in 33 RA patients versus 0.78 in 136 non-CIRD controls. This difference was highly significant (p = 0.013).

Comparison of HDLox and CRP between baseline and follow-up in CIRD patients.

Serum lipid profile at baseline and follow-up in CIRD patients.
An adjusted regression model was performed using HDLox as dependent variable and the concentrations of HDL-C, LDL-C, cholesterol, triglyceride, CRP, age, BMI, and smoking status as independent variables. This model showed no significant association except for HDL-C and smoking status. HDLox was inversely correlated with HDL-C (p = 0.01) and positively with smoking status (p = 0.03) (Table 4).
Effect of HDLox on lipid profile, CRP, body mass index, age, and current smoking status of patients with CIRD and non-CIRD.

Dependent variable: HDLox, no unit.
Statistical significance was determined using multivariate-adjusted regression analysis and the significance level was set at 0.05.
HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol.
Bold font indicates statistical significance.
Discussion
The present study is the first to investigate the impact of rheumatic disease on HDLox as a marker of dysfunctional HDL. As initially hypothesized, the serum HDLox value was found to be higher in patients newly diagnosed with CIRD than in non-CIRD patients. We decided against healthy controls as a control group to have comparable traditional cardiovascular risk factors. Indeed, groups were well-matched regarding age, sex, and comorbidities except for hypertension, which was more prevalent in the non-CIRD group. Moreover, there was no significant difference in lipid-lowering medication intake. No drug has proven to have an effect on HDLox levels so far. Thus, the intergroup difference in HDLox has likely to be attributed to the state of chronic inflammation. Nevertheless, although initiation of treatment with a subsequent reduction of inflammation led to a numerical decrease in HDLox levels, we need to acknowledge that the study was not powered to provide a statistically robust treatment effect on HDLox. The regression model showed an increase in HDLox with nicotine use. This finding is plausible as smoking is considered to lead to the oxidation of lipoproteins, including HDL.18–20 Given the limited information available on the association between HDLox and smoking, it is relevant to add the present findings to those of previous studies.18–20 Another significant finding of the regression analysis was that HDL-C concentrations slightly increased with decreasing HDLox levels. Since we enrolled patients with different CIRD entities, we performed a subgroup analysis of RA patients showing an even more pronounced difference in HDLox compared to controls, thereby confirming the major result of the study.
But is HDLox indeed an appropriate marker to reflect the antiatherogenic properties of HDL? Due to the broad variety of properties of this complex lipoprotein, it is difficult to measure HDL quality. Measurement of cholesterol efflux capacity necessitates a cell culture-based assay. In an attempt to measure HDL functionality in an automated, observer-independent manner, novel cell-free assays have been established that, for example, quantify the redox activity of HDL. HDLox behaves in the bloodstream as dysfunctional HDL and has therefore been established as a marker to assess HDL functionality. 21 HDLox, as a marker of lipid peroxidation of HDL, has been studied in several populations, demonstrating a constant association with increased systemic inflammation and immune dysfunction.22–24 In the Mashhad stroke and heart atherosclerotic disorders (MASHAD) cohort of 330 individuals who had a median follow-up period of 7 years, plasma baseline HDLox levels independently predicted risk for clinical CVD (odds ratio, 1.62; 95% confidence interval, 1.41–1.86; p < 0.001). 25 In patients with HIV, it has been shown that HDLox serves as a driver of HIV-related inflammation, immune dysfunction, and CVD.16,24,26,27 Hence, HDLox is currently the best cell-free marker of dysfunctional HDL.
Atherosclerosis has been regarded as an exclusively metabolic disease for decades. In recent years, however, experimental and clinical data suggest that chronic inflammation promotes atherosclerosis. In order to prove this principle, it has been demonstrated that periodontitis, as an example of systemic microinflammation, is associated with endothelial dysfunction that can be remedied by treatment of periodontitis. 28 The inflammatory nature of atherosclerosis has finally been proven by data from the CANTOS trial which have, for the first time, demonstrated that anti-inflammatory treatment with canakinumab, a monoclonal antibody targeting interleukin-1ß, and reduces the number of major cardiovascular events. 29 The subsequent COLCOT and LODOCO2 trials confirmed these results using colchicine as an anti-inflammatory drug.30,31
To date, however, the mechanisms for inflammation to promote atherosclerosis remain largely unclear. The present study unmasks one of these mechanisms. Untreated RA, axSpA, and SLE are associated with an inflammatory milieu that is characterized, for example, by an increase of reactive oxygen species, which can induce the oxidization of proteins and lipoproteins. 32 Oxidization of HDL, however, diminishes its cholesterol efflux properties.32–34 The same phenomenon has been demonstrated for diabetes and chronic kidney disease, which are associated with an increase in HDLox as well.
Chronic inflammation is associated with a decrease of LDL cholesterol levels but an increase in cardiovascular risk. The present findings on HDLox contribute to our understanding of this lipid paradox in rheumatology. As described above, low levels of cholesterol and LDL-C are associated with an increased risk of mortality in rheumatic diseases, since chronic inflammation reduces the concentration of cholesterol and LDL-C. 5 Our study population confirms this phenomenon. Cholesterol concentrations were lower in patients with CIRD as compared to non-CIRD patients. It may be speculated that the effects of inflammation itself and the associated increase in HDLox outweigh the benefit of a slightly lower LDL-C. Hence, appropriate treatment of a rheumatic disease not only leads to a relief of symptoms but also contributes to a reduction of cardiovascular risk. Therefore, a reduction of systemic inflammation in RA by either methotrexate or TNFα-antagonists is able to reduce cardiovascular morbidity, and mortality and even nonsteroidal anti-inflammatory drugs may be of cardiovascular benefit in an anti-inflammatory indication.35–37 In contrast, methotrexate failed to reduce cardiovascular events in the CIRT trial. 29 In this trial, however, patients had no CIRD and no other inflammatory state as expressed by CRP levels.
A strength of the present study is that it enrolled treatment-naive patients with CIRD. Hence, it could examine the potential impact of inflammation on HDLox concentrations in two ways: First, by comparison with patients without CIRD, and second by the prospective view on the impact of a de novo treatment. However, this very strict inclusion criterion prevented a substantially larger study cohort even in the largest rheumatology clinic in Germany.
The study is limited by its study size and the inclusion of heterogeneous inflammatory entities (RA, axSpA, and SLE). Thus, the initiation of anti-inflammatory treatment tended to reduce HDLox concentrations without reaching statistical significance due to the limited sample size. Multicenter studies will be necessary to focus on isolated diseases like RA in larger populations. Moreover, there were slightly more males than females in the CIRD group, which does not reflect the real-world distribution. Finally, diabetes and smoking were exclusion criteria in the CIRD group and hypertension was more prevalent in the control group. The results of our study may be interpreted considering the above stated limitations.
Conclusion
In conclusion, the study shows that RA, axSpA, and SLE, as key representatives of CIRD, are associated with an impairment of the anti-atherosclerotic properties of HDL as reflected by an increase in HDLox concentrations. These findings may provide a new candidate mechanism to explain the increased cardiovascular risk in rheumatic diseases. Moreover, they contribute to our understanding of why patients with CIRD have an increased mortality risk despite low LDL-C concentrations.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X231187191 – Supplemental material for Dysfunctional high-density lipoprotein in chronic inflammatory rheumatic diseases
Supplemental material, sj-docx-1-tab-10.1177_1759720X231187191 for Dysfunctional high-density lipoprotein in chronic inflammatory rheumatic diseases by Sabina Waldecker-Gall, Felix Seibert, Sebastian Bertram, Adrian Doevelaar, Jürgen Braun, Xenofon Baraliakos, Nina Babel, Christoph Waldecker, Linda Scharow, Nikolaos Pagonas and Timm H. Westhoff in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-2-tab-10.1177_1759720X231187191 – Supplemental material for Dysfunctional high-density lipoprotein in chronic inflammatory rheumatic diseases
Supplemental material, sj-docx-2-tab-10.1177_1759720X231187191 for Dysfunctional high-density lipoprotein in chronic inflammatory rheumatic diseases by Sabina Waldecker-Gall, Felix Seibert, Sebastian Bertram, Adrian Doevelaar, Jürgen Braun, Xenofon Baraliakos, Nina Babel, Christoph Waldecker, Linda Scharow, Nikolaos Pagonas and Timm H. Westhoff in Therapeutic Advances in Musculoskeletal Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.