
Abstract
Background:
The value of normal C-reactive protein (CRP) in psoriatic arthritis (PsA) is debatable.
Objectives:
To test the hypothesis that CRP is frequently normal in contemporary real-world PsA patients, despite active disease.
Design:
In this cross-sectional study, patients were divided into two groups: CRP ⩽ 0.5 mg/dl (normal) and CRP > 0.5 mg/dl (increased). Having as dependent variable the CRP status, these groups were compared for disease-related features, including composite disease activity indices [clinical Disease Activity in PSoriatic Arthritis (cDAPSA) and minimal disease activity (MDA)] and patient-reported outcomes (PROs). Agreement between CRP status and cDAPSA/MDA scores was calculated (Cohen’s kappa).
Methods:
Data from consecutive PsA patients attending two outpatient rheumatology clinics (January 2019–June 2021) were analysed.
Results:
From 128 patients enrolled (51.6% females; mean ± standard deviation age: 53.4 ± 11.7 years; 23.4%, 48.4% and 64.1% treated with glucocorticoids, conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs) and biologic DMARDs, respectively), two-thirds (66.4%, n = 85) had normal CRP values. CRP status was not associated with any of the disease-related parameters and PROs, but only with ESR [odds ratio: 1.04 (95% confidence interval: 1.01–1.06), p = 0.005]. Among patients with normal CRP, 45.9% (39/85) were on non-MDA state, while 21.2% (18/85) had cDAPSA-moderate and 5.9% (5/85) had cDAPSA-high disease activities. Conversely, 54.2% (39/72) of patients on non-MDA state and 52.3% (23/44) of those with cDAPSA-moderate or cDAPSA-high disease activity had normal CRP values. Cohen’s kappa between normal CRP and MDA, cDAPSA-remission, and cDAPSA-remission/low disease activity was –0.26, –0.21 and –0.22, respectively, displaying total disagreement.
Conclusion:
Normal CRP in PsA should not be used as surrogate marker of remission or low/MDA, therefore needs to be interpreted with caution in clinical decision-making.
Keywords
Introduction
Psoriatic arthritis (PsA) is a chronic inflammatory disease associated with a wide spectrum of clinical manifestations; namely, musculoskeletal (peripheral arthritis, enthesitis, dactylitis, spondylitis and sacroiliitis) and extra-musculoskeletal (skin/nail psoriasis, uveitis and inflammatory bowel disease), in addition to associated comorbidities.1,2
Given the inherent heterogeneity of PsA, no consensus has been reached thus far regarding an optimal index to capture the overall disease activity. 3 Among the laboratory markers, C-reactive protein (CRP) is a classic, though non-specific, inflammatory marker readily measured in everyday clinical practice, also incorporated into composite indices of PsA activity [e.g. the Disease Activity index in PSoriatic Arthritis (DAPSA)]. 3
CRP is still frequently used by rheumatologists for diagnosis and/or monitoring of PsA patients. 4 However, while elevated CRP has been suggested to associate with worse disease prognosis, 5 the value of normal CRP for assessing disease activity and guiding decisions is debatable. Indeed, experts in PsA have recently challenged CRP value in these patients.6 –8
Herein, we tested the hypothesis that CRP is frequently normal in contemporary real-world patients with PsA, despite active disease. Therefore, we have cross-sectionally analysed data from a real-world PsA population and searched for associations of CRP status with disease-related parameters. We also evaluated the agreement between normal CRP and clinical disease activity indices that have been used in clinical trials of PsA and routine practice.
Methods
Patient population and data collection
All PsA patients [fulfilling ClASsification criteria for Psoriatic ARthritis (CASPAR) 9 ] who consecutively attended the outpatient rheumatology clinics from two tertiary hospitals between January 2019 and June 2021 were included. Patients with active infection or malignancy were excluded from the study.
A range of pre-specified parameters were recorded at the time of their visit in the clinics (‘time of clinical assessment’). These included demographic characteristics: age, age at diagnosis, sex, body mass index (BMI), smoking status, disease duration (time interval between disease diagnosis and time of clinical assessment) and features present at the time of clinical assessment: (a) clinical manifestations; peripheral arthritis [66 swollen joint count (SJC) and 68 tender joint count (TJC) and involvement of distal interphalangeal joints (DIP])], enthesitis, dactylitis, skin psoriasis [assessed by body surface area (BSA)], nail involvement, uveitis and inflammatory bowel disease, (b) inflammatory markers; erythrocyte sedimentation rate (ESR) and CRP, (c) patient-reported outcomes (PROs); Patient Global (PtG) and Patient Pain (PtP) Assessment [both on a on visual analogue scale (VAS) from 0 to 100 mm], Health Assessment Questionnaire Disability Index (HAQ-DI) as a measure of functional status, EuroQol-5 Dimension (EQ-5D) as an index of quality of life (QoL) and (d) medication for PsA; glucocorticoids, conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs) and biologic DMARDs (bDMARDs).
Disease activity state was defined using the following composite clinical indices:
Clinical Disease Activity in PSoriatic Arthritis (cDAPSA), which is calculated as the sum of TJC, SJC, PtG and PtP, and the score is interpreted as follows: ⩽ 4 = remission, 5–13 = low disease activity, 14–27 = moderate disease activity and ⩾ 28 = high disease activity. 10
Minimal disease activity (MDA) criteria, including seven cutpoints: TJC ⩽ 1, SJC ⩽ 1, BSA ⩽ 3, PtG (VAS) ⩽ 15 mm, PtP (VAS) ⩽ 20 mm, HAQ ⩽ 0.5 and enthesitis count ⩽ 1. Patients achieving at least five of them were considered to be on MDA state. 11
Study design and statistical analysis
Patients were divided into two groups depending on CRP status, those with CRP ⩽ 0.5 mg/dl (normal) and those with CRP > 0.5 mg/dl (increased).
Testing whether normal CRP truly reflects inactive disease as well as favourable PROs, we examined the association of CRP status with disease-related parameters, including clinical and laboratory features, demographic characteristics and PROs, respectively.
For univariate analyses, Mann–Whitney and two-sided Fisher’s tests were performed. Continuous variables were presented as mean ± standard deviation (SD) if distributed normally or median (interquartile range [IQR]) for those without normal distribution, and categorical as percentages (%). In binomial multivariable analysis (enter model), CRP status was the depended variable, while the features that displayed statistically significant differences (p-value < 0.05) in the univariate analysis, served as independent variables. Results were expressed as odds ratios (ORs), 95% confidence intervals (CIs).
Moreover, we estimated the agreement between normal CRP status and cDAPSA/MDA scores through Cohen’s kappa coefficient (higher kappa denotes greater agreement; negative kappa represents agreement worse than expected or disagreement). 12
Analyses were conducted through statistical packages GraphPad Prism 9.0.0 and SPSS 24.0.
This study was conducted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 13 The STROBE checklist is provided in Supplementary Table 1.
Results
Patient characteristics
A total of 128 PsA patients were included (Table 1). The mean ± SD age was 53.4 ± 11.7 years and 51.6% of patients were female. Patients had mean ± SD BMI of 28.3 ± 6.4 kg/m2. Regarding inflammatory markers, patients had a median (IQR) ESR of 16.0 (10.0–26.0) mm/h and a median (IQR) CRP of 0.29 (0.1–0.6) mg/dl. The frequency distribution of CRP values is depicted in Supplementary Figure 1. Overall, 43.8% of patients were on MDA state. Regarding treatments regimens, 23.4%, 48.4% and 64.1% received glucocorticoids, csDMARDs and bDMARDs, respectively. The mean ± SD cDAPSA score was 11.6 ± 9.5 with 28.9%, 36.7%, 27.4% and 7.0% having cDAPSA-remission, -low, -moderate and -high disease activity, respectively. Further characteristics are displayed in Table 1.
Demographic characteristics, disease-related features and outcomes at the time of clinical assessment.
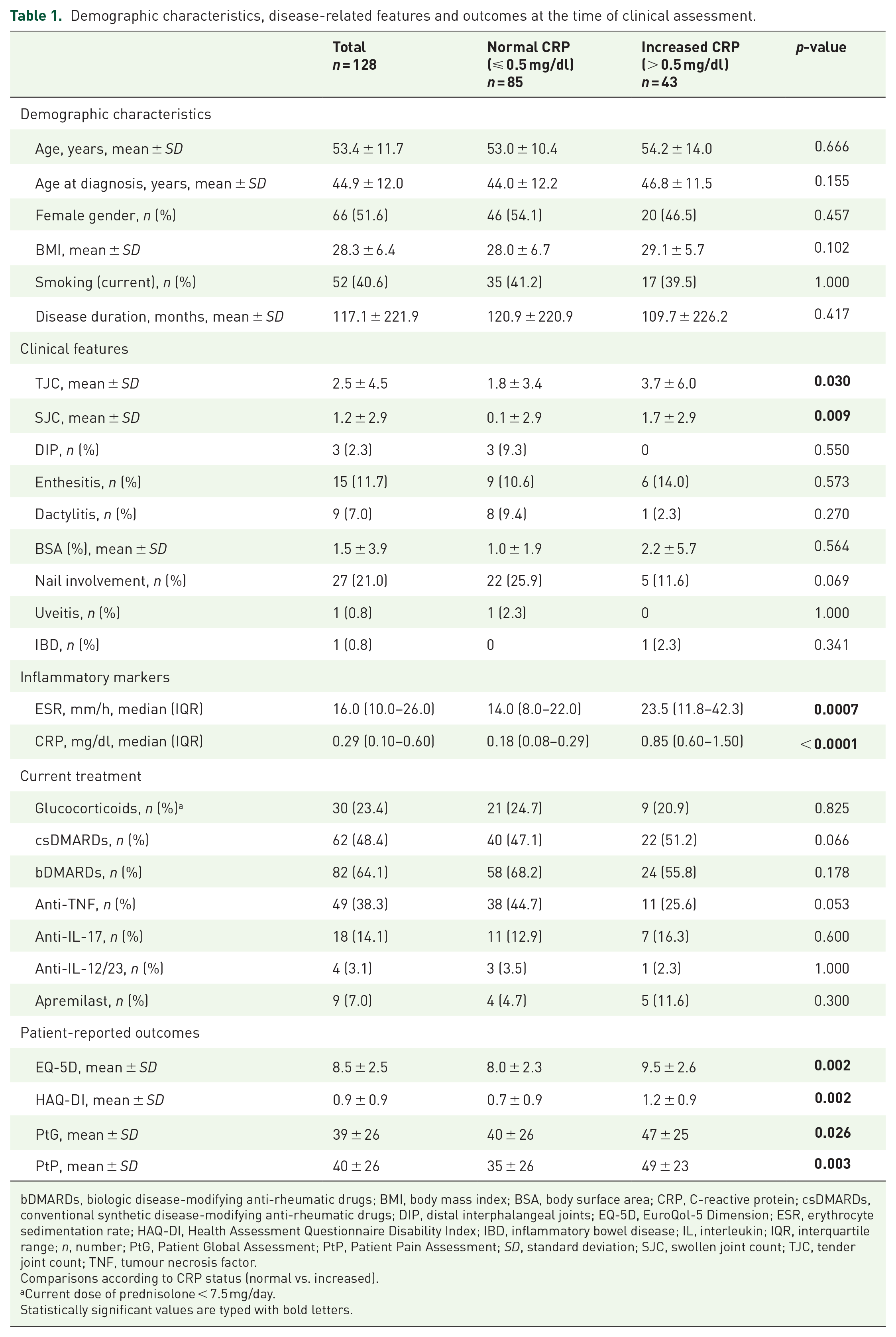
bDMARDs, biologic disease-modifying anti-rheumatic drugs; BMI, body mass index; BSA, body surface area; CRP, C-reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; DIP, distal interphalangeal joints; EQ-5D, EuroQol-5 Dimension; ESR, erythrocyte sedimentation rate; HAQ-DI, Health Assessment Questionnaire Disability Index; IBD, inflammatory bowel disease; IL, interleukin; IQR, interquartile range; n, number; PtG, Patient Global Assessment; PtP, Patient Pain Assessment; SD, standard deviation; SJC, swollen joint count; TJC, tender joint count; TNF, tumour necrosis factor.
Comparisons according to CRP status (normal vs. increased).
Current dose of prednisolone < 7.5 mg/day.
Statistically significant values are typed with bold letters.
Association of normal CRP with parameters reflecting disease activity
In this PsA population, 66.4% (n = 85) had normal CRP (⩽ 0.5 mg/dl), while the rest displayed increased CRP values at the time of clinical assessment. In the univariate analyses, patients with normal CRP had significantly lower TJC (p = 0.03), SJC (p = 0.009) and ESR levels (p = 0.0007), as well as better scores in terms of pain, patients’ perception about the disease, QoL and functional status (PtP, PtG, EQ-5D and HAQ-DI, respectively) (Table 1). No significant association was found between CRP status and any other parameters tested, including demographic features and concomitant treatment received for PsA (Table 1).
Three multivariable analysis models were performed having as dependent variable the CRP status. In the first, adjustments were conducted for all abovementioned variables that displayed statistically significant differences, while in the second, we corrected only for TJC, SJC and ESR levels. Across both models, CRP status was not associated with any of the tested parameters reflecting disease activity (TJC, SJC and PROs). Instead, its association with ESR remained significant [first model; OR: 1.04 (95% CI: 1.01–1.06), p = 0.005, standardized B: 0.136, Nagelkerke R2: 0.219]. Further details for the first model are shown in Supplementary Tables 2 and 3. In addition, we reran the first model adjusting also for the treatment with tumour necrosis factor (TNF) inhibitors and csDMARDs, given the borderline association with CRP status in univariate analyses (Table 1). ESR was still the only parameter associated with CRP status (Supplementary Table 4).
Despite these results, still a sizable number of patients had discordant results. In fact, 23/85 (27.1%) of patients with normal CRP had ESR above 20 mm/h, while 19/43 (44.2%) of patients with increased CRP had ESR ⩽ 20 mm/h.
Agreement between normal CRP and disease activity indices
The majority of patients being on MDA state (46/56, 82.1%) had normal CRP (Table 1). Conversely, in the group of patients with normal CRP (n = 85), 39 (45.9%) were on non-MDA state. Also, sensitivity of CRP for recognizing patients on non-MDA state (n = 72) was 45.8% (33/72), with false-negative tests (i.e. normal CRP value) being observed in 54.2% (39/72) (Figure 1). In line, kappa coefficient between normal CRP status and MDA state was –0.26, corroborating disagreement among them.

CRP status with respect to disease activity indices in PsA.
Regarding cDAPSA scores, most of the patients being on remission (30/37, 81.1%) had normal CRP (Table 1). On the other hand, among patients with normal CRP, 21.2% (18/85) had moderate and 5.9% (5/85) had high disease activity. Sensitivity of CRP for identifying moderate/high disease activity was 47.7%. In other words, 52.3% of patients with cDAPSA score ⩾ 14 had false-negative/normal CRP values (Figure 1). Cohen’s Kappa displayed total disagreement between normal CRP status and cDAPSA-remission/low disease activity, as well as cDAPSA-remission alone (–0.22 and –0.21, respectively).
Discussion
This study essentially challenged the usefulness of normal CRP for assessing disease activity in PsA patients. In our dataset, the majority of patients had normal CRP, which is consistent with previous studies.14,15 Importantly, we found major disagreements of normal CRP status with cDAPSA scores for remission/low disease activity, as well as with MDA state. In detail, 54.2% of patients on non-MDA state and 52.3% of those with cDAPSA moderate/high disease activity had normal CRP values. Supporting our findings, previous cross-sectional studies have shown a perfect agreement between DAPSA (cDAPSA + CRP) and cDAPSA scores, implying that CRP was redundant in estimating PsA activity.6,7 Interestingly, in our study, CRP status did not show any association with any of the PROs, in the multivariable analyses. Of note, although it was out of scope of this study, most of the patients with increased CRP were on non-MDA state and/or had non-remission DAPSA scores (Figure 1).
It is unknown in which PsA patients CRP status concurs with disease activity. Sokolova et al. 15 have reported that the elevation of CRP depends on the clinical pattern of PsA, demonstrating that patients with arthritis – and not these with skin and/or entheseal disease – had elevated CRP, but still this pertained to one-third of this subset. In another large cross-sectional study [Assessment in SpondyloArthritis Inter-national Society-CoMorbidities in SpondyloArthritis (ASAS-COMOSPA)], CRP values did not differ significantly between PsA patients with peripheral arthritis versus those with axial involvement, regardless of the presence of skin psoriasis, although these groups exhibited several differences in demographic, clinical and treatment features. 16 In our cohort, patients with increased CRP had significantly more tender and swollen joints, but this association attenuated after controlling for confounders. Three different multivariable models were ran, with ESR remaining in all of them the only parameter which significantly associated with CRP status. However, still there was a discordance between these two inflammatory markers. Besides, age, gender and other variables like BMI, hypergammaglobulinaemia or anaemia could affect ESR. 17
Considering the above, it seems that the association of CRP with certain PsA phenotypes merits further investigation. The value of CRP has been examined in other forms of spondyloarthritis as well. A pooled analysis of clinical trials for secukinumab in patients with ankylosing spondylitis (AS) showed response to treatment irrespective of baseline CRP status. 18 Notably, Claushuis et al. 19 have identified different CRP genotypes between AS patients with low and high CRP levels.
Inability of CRP to reflect disease activity, as well as lack of association with PROs could be owed to several factors. For example, comorbid mood disorders and/or fibromyalgia, which are common in PsA,20,21 could affect and/or distort disease activity measurements. Alternatively, mechanisms that suppress CRP production despite underlying inflammatory process could operate in PsA. Besides, systemic inflammation can be detectable in many PsA patients with normal CRP, through a range of other serum immune markers. 15 Towards this direction, one could hypothesize that different inflammatory pathways might be activated in diverse PsA subtypes.
One major strength of our cohort is that is based on real life data from consecutive examined patients under various standard treatment regimens, providing the opportunity to estimate the performance of CRP in PsA without selection biases. Furthermore, this is the first study examining simultaneously, associations between CRP status and various patient- and disease-related parameters in PsA patients. Also, we used widely implemented and validated indices and questionnaires to define the state of disease activity and assess subjective disease outcomes, respectively, both applied concurrently with clinical examination and CRP measurement.
We also acknowledge that our study has certain limitations. First, the cross-sectional design did not allow us to follow the course of CRP in parallel with changes of the tested variables and disease activity. Second, patients included in this cohort were consecutive and so groups were not matched for certain features, such as treatment with csDMARDs and TNF inhibitors (TNFi). Third, our population size was not appropriate to consider comorbidities, such as cardiovascular disease, which has been proposed to associate with CRP levels.22,23 Finally, CRP was analysed as a dichotomous variable, with cut-off being 0.5 mg/dl, in accordance with most of the studies examining CRP in the context of PsA.6,7
Conclusion
In conclusion, more than half of PsA patients have normal CRP values which do not consistently denote remission, neither low/MDA, therefore, CRP needs to be interpreted with caution in clinical decision-making. The need of an easy to obtain, reliable biomarker to reflect disease activity and steer the rationale in PsA remains unmet. This study underpins future research for elucidating pathogenetic mechanisms that operate in this heterogeneous disease.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X221122417 – Supplemental material for Normal C-reactive protein in active psoriatic arthritis: results from real-world clinical practice
Supplemental material, sj-docx-1-tab-10.1177_1759720X221122417 for Normal C-reactive protein in active psoriatic arthritis: results from real-world clinical practice by Chrysoula G. Gialouri, Gerasimos Evangelatos, Maria Pappa, Anastasios Karamanakos, Alexios Iliopoulos, Maria G. Tektonidou, Petros P. Sfikakis and George E. Fragoulis in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-jpg-3-tab-10.1177_1759720X221122417 – Supplemental material for Normal C-reactive protein in active psoriatic arthritis: results from real-world clinical practice
Supplemental material, sj-jpg-3-tab-10.1177_1759720X221122417 for Normal C-reactive protein in active psoriatic arthritis: results from real-world clinical practice by Chrysoula G. Gialouri, Gerasimos Evangelatos, Maria Pappa, Anastasios Karamanakos, Alexios Iliopoulos, Maria G. Tektonidou, Petros P. Sfikakis and George E. Fragoulis in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-rtf-2-tab-10.1177_1759720X221122417 – Supplemental material for Normal C-reactive protein in active psoriatic arthritis: results from real-world clinical practice
Supplemental material, sj-rtf-2-tab-10.1177_1759720X221122417 for Normal C-reactive protein in active psoriatic arthritis: results from real-world clinical practice by Chrysoula G. Gialouri, Gerasimos Evangelatos, Maria Pappa, Anastasios Karamanakos, Alexios Iliopoulos, Maria G. Tektonidou, Petros P. Sfikakis and George E. Fragoulis in Therapeutic Advances in Musculoskeletal Disease
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.