
Abstract
Background:
Ultrasound (US) is useful in monitoring RA patients, with the US7 score allowing grey-scale and power-Doppler (PD) semi-quantitative evaluation of synovitis and teno-synovitis. We evaluated real-life efficacy and safety of Baricitinib, an oral selective JAK1-2 inhibitor, in RA patients using clinical, clinimetric, and US assessments.
Methods:
Disease activity score in 28 joints calculated with C-reactive protein (DAS28-CRP), disease activity score in 28 joints calculated with erythrocyte sedimentation rate (DAS28-ESR), clinical disease activity index (CDAI), simplified disease activity index (SDAI), visual analogue scale (VAS)-pain, health assessment questionnaire (HAQ), COCHIN scale, adverse events (AE), concomitant medications, laboratory parameters, and US7 were performed/recorded at baseline, 1, 3, and 6 months in RA patients starting Baricitinib. Responder/non-responder status was determined according to the EULAR Response Criteria at 3 months. SDAI clinical remission or low disease activity (LDA) were calculated at 3 and 6 months.
Results:
In 43 enrolled patients, a significant improvement in disease activity and US7 components (except tendon PD) and a reduction of steroid dosage were observed. Responders at 3 months showed a significantly higher reduction of CDAI, SDAI, COCHIN scale, VAS-pain, and US7 synovialPD, compared with non-responders. At 3 and 6 months, remission/LDA was achieved by 12.8/53.8% and 21.6/51.3% patients, respectively. The csDMARD co-treatment was independently associated with remission/LDA at 3 months. Safety-related drop-outs were in line with literature data. The steroid dosage was associated with AE development at 6 months.
Conclusion:
The real-life data, also obtained with US evaluation, confirmed the Baricitinib efficacy in RA disease control, as well as the utility of assessment during the follow up of disease activity.
Introduction
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by chronic inflammation of the synovial joints, with resulting joint damage, impairment of quality of life, and reduced life expectancy. 1
Remission in RA is the ultimate goal of an anti-rheumatic therapy. 2 Biologic disease-modifying anti-rheumatic drugs (bDMARDs) have changed the landscape of therapy of RA substantially and the management of these patients has changed over the past 30 years. Recently, the new class of target synthetic DMARDs (tsDMARDs) has been developed, including Janus kinase inhibitors (JAK-i). These small molecules interfere with intracellular signal transduction by inhibiting JAK enzymes. In fact, pro-inflammatory cytokines implicated in the pathogenesis of RA, including interleukin (IL)-6, IL-15, IL-17, IL-23, interferon-α/β, interferon-γ, and granulocyte-macrophage colony-stimulating factor, act primarily through intracellular JAK signalling pathways. 3 Baricitinib is an oral selective inhibitor of JAK-1 and JAK-2 enzymes, approved in different countries for the treatment of moderate-to-severe active RA in adults. 1 Several phase II and phase III randomized clinical trials (RCTs) showed efficacy of Baricitinib in the treatment of RA both in conventional synthetic (csDMARDs) and anti-tumour necrosis factor (TNF)α failure patients, both in combination with a csDMARD or in monotherapy.3,4–9
Among imaging modalities, muscle-skeletal ultrasound (US) is a valuable imaging tool in the detection of synovial inflammation and early erosive bone changes. 10 In order to measure RA progression, the semiquantitative US 7 joints score (US7) was developed, and was demonstrated to have face validity, feasibility, and responsiveness to treatment as an outcome measure to assess disease activity.11–13
Considering the differences between RCTs and real-life patients, in particular in terms of comorbidities and concomitant medications, the aim of our study was to describe the efficacy and safety profile of Baricitinib in a real-life cohort of RA patients, with a focus on the use of clinical, clinimetric, and US evaluation during the treatment monitoring. Moreover, we investigated the predictive factors for the development of AEs, for treatment response, and for the achievement of remission/low disease activity (LDA) status during the study.
Materials and methods
A monocentric, retro-prospective observational longitudinal study was conducted from June to November 2019 at the Rheumatology Department, Azienda Ospedaliera Universitaria Careggi, Florence, Italy. The study was approved by the local Institutional Review Board (IRB; protocol number CEAVC 14658) and all patients signed informed consent for data collection and analysis.
Patients aged over 18, classified a RA according to the 2010 ACR/EULAR criteria, 14 receiving Baricitinib on-label for at least three consecutive months were eligible for the study.
The following data were collected at baseline (BL, at the prescription of Baricitinib) and after 1, 3, and 6 months of follow up (1M, 3M, 6M, respectively), if available:
– demographic and anamnestic data: age, gender, disease onset and duration;
– treatments: current or previous csDMARDs exposure, previous bDMARDs exposure, current steroid therapy and prednisone equivalent daily steroid dose;
– laboratory parameters: rheumatoid factor (RF), and anti-cyclic citrullinated peptide (ACPA) positivity, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP);
– clinical evaluation: tender and swollen joint count on 28 joints;
– clinimetric data: physician’s global assessment of disease activity (PGA), patient’s assessment of disease activity (VAS), patient’s assessment of global health (GH) and patient’s assessment of pain (VAS pain) in a 0–100 mm scales, health assessment questionnaire (HAQ), Cochin hand function scale, disease activity score in 28 joints (DAS28), clinical disease activity index (CDAI), simplified disease activity index (SDAI);
– systemic adverse events collection: severe and non-severe adverse events (SAEs and AEs) from BL to 6M;
– US parameters: US study of hands and feet was performed with Esaote myLab70X Vision (Genova, Italy), using a linear probe 6–18 MHz. The calculation of the US7-score, included the determination of grey-scale synovitis (GSS 0–27) and tenosynovitis (GST 0–7) scores, power Doppler synovitis (PDS 0–39) and tenosynovitis (PDT 0–21) scores, and presence of erosions (erosions 0–14); the sonographer was blinded to the abovementioned clinical and clinimetric assessments, as well as to the ongoing concomitant medication profile.
Patients were clustered into responders and non-responders using DAS28-ESR improvement after 3M and 6M of treatment, according to EULAR response criteria. 15 Patients requiring an increase of steroid dose or the addition/change of csDMARD were arbitrarily considered as non-responders.
In addition, the rate of remission/low disease activity (LDA) achievement at 3M and 6M was calculated using the SDAI score (remission SDAI ⩽ 3.3; LDA 3.3 < SDAI ⩽ 11), according to EULAR/ACR criteria. 16 “Disease flares” were defined according to the OMERACT definition.17,18
Statistical analysis
The continuous variables are presented as mean ± standard deviation (SD), while categorical variables are presented as absolute frequency and percentage of each category. The associations between categorical variables were tested by Chi-square test or by Fisher test where appropriate. The associations between continuous and categorical variables, after normality test of Shapiro-Wilk, were evaluated by Student’s t test or Mann–Whitney test where appropriate. In order to evaluate the difference in efficacy parameters changes between responders and non-responders, we used a generalized estimating equation (GEE) linear regression model adjusting for baseline values.
In order to evaluate the association between AE development and possible risk factors, simple logistic regression was used. The statistically significant level was set to 5%. In all analyses, missing data were excluded.
Results
Study population
A total of 43 RA patients were included: 37 females (86.05%) and 6 males (13.95%), mean age 56.09 ± 11.15 years, mean disease duration 12.57 ± 10.01 years. RF and ACPA were positive in 22 (53.66%) and 28 (70.00%) patients, respectively. All patients had previously received treatment with at least one csDMARD; 12 (27.91%) were bDMARDs naïve, and 31 patients (72.09%) were bDMARDs failure. All patients received Baricitinib 4 mg; this was administered in combination with at least one csDMARD in 30 patients (69.77%) and in association with corticosteroids in 32 (74.42%) cases. Table 1 reports the baseline characteristics of the study population.
Characteristics of study populations at the baseline visit.

ACPA, anti-cyclic citrullinated peptide; csDMARD, conventional synthetic disease modifying anti-rheumatic drugs; RF, rheumatoid factor; SD, standard deviation.
The BL mean disease activity was severe according to DAS28-ESR (5.27 ± 1.33) and CDAI (27.68 ± 10.62) scores, while moderate according to DAS28-CRP (4.68 ± 1.03) and SDAI (25.01 ± 11.40). Using the US7 score, the sonographic assessment also confirmed the presence of a high disease activity, as presented in Table 2.
Change of the clinimetric, laboratory, and US parameters during the study period.

Significant at p < 0.05.
1M, 1 month visit; 3M, 3 months visit; 6M, 6 months visit; BL, baseline; CDAI, clinical disease activity index; CRP, C-reactive protein; DAS28-CRP, disease activity score in 28 joints calculated with CRP; DAS28-ESR, disease activity score in 28 joints calculated with ESR; ESR, erythrocyte sedimentation rate; GSS, grey-scale synovitis; GST, grey-scale tenosynovitis; HAQ, health assessment questionnaire; PDS, Power Doppler synovitis; PDT, Power Doppler tenosynovitis; SDAI, simplified disease activity index; US, ultrasound; VAS, visual analogue scale.
Efficacy evaluation
A statistically significant improvement of all the activity indexes and clinimetric scores was observed already after the first month of Baricitinib treatment and continued throughout the 3M and 6M follow-up visits (as described in Table 2).
Similarly, all the domains of the US7 score showed a statistically significant improvement already at 1 month of treatment with Baricitinib. In particular, GSS, GST, and PDS improved significantly at 1M, 3M, and 6M, whereas PDT improved at 1M and 3M and returned to values similar to baseline at 6M, despite being still numerically lower. When compared with the BL visit, the erosions score did not show any significant change at all time points. In addition, a significant reduction in the prednisone equivalents dose was noted as early as the first month of treatment and this trend persisted until the 6M visit (Table 2). Similarly, the number of patients treated with steroids progressively reduced, from 32/43 (74.42%) at BL to 29/38 at 1M (76.3%), 25/42 at 3M (59.52%), and 16/40 at 6M (40%).
At the 3M visit, four patients added a csDMARD, two patients changed the csDMARD, while three patients suspended or reduced the concomitant csDMARD. According to the abovementioned definition, 28/39 (71.79%) were classified as responders at 3M, while the non-responders were 11/39 (28.21%).
When comparing the two groups, they were similar in terms of age, gender, RF, and/or ACPA positivity rates. Despite this, responders at 3M showed numerically but not statistically significant higher BL activity indexes/scales and ultrasound scores (see Table 3). Conversely, GST was lower in the responders group and PDT was similar among them.
Changes of clinimetric and US parameters between responders or non-responders.

Significant at p < 0.05.
3M, 3 months visit; BL, baseline; CDAI, clinical disease activity index; GSS, grey-scale synovitis; GST, grey-scale tenosynovitis; HAQ, health assessment questionnaire; PDS, Power Doppler synovitis; PDT, Power Doppler tenosynovitis; SDAI, simplified disease activity index; US, ultrasound; US7, ultrasound 7 joints score; VAS, visual analogue scale.
At 3M, SDAI, CDAI scores, as well as COCHIN scale and VAS-pain, were significantly different between the two groups, with a higher improvement in the responders group. All US7 domains showed a numerical reduction in both groups, with PDS variation reaching a statistically significant difference between responders and non-responders. Interestingly, the mean steroid dosage decreased in both groups, without statistically significant difference.
Despite BL similarities, the presence of a combination therapy at BL was associated with a higher probability to be responders, as compared with monotherapy [24/29 (82.76%) versus 4/10 (40.00%), p = 0.0167].
At 6M, 25/36 patients (69.44%) were classified as responders, while 11/36 (30.56%) as non-responders. When comparing 3M and 6M assessments, we noted that 21 patients maintained the status of responders and 7 patients of non-responders at both timepoints. Conversely, three non-responders at 3M improved and became responders at 6M, while four responders at 3M lost this status at 6M. These seven cases are described in Table 4: it was interesting to observe that patients who lost their responder status showed a general increase in US scores between 3M and 6M, whereas those who newly gained responder status showed a general slow but progressive decrease of them from BL to 6M.
Evolution of US score domains in patients who changed their responder/non-responder status between 3M and 6M.
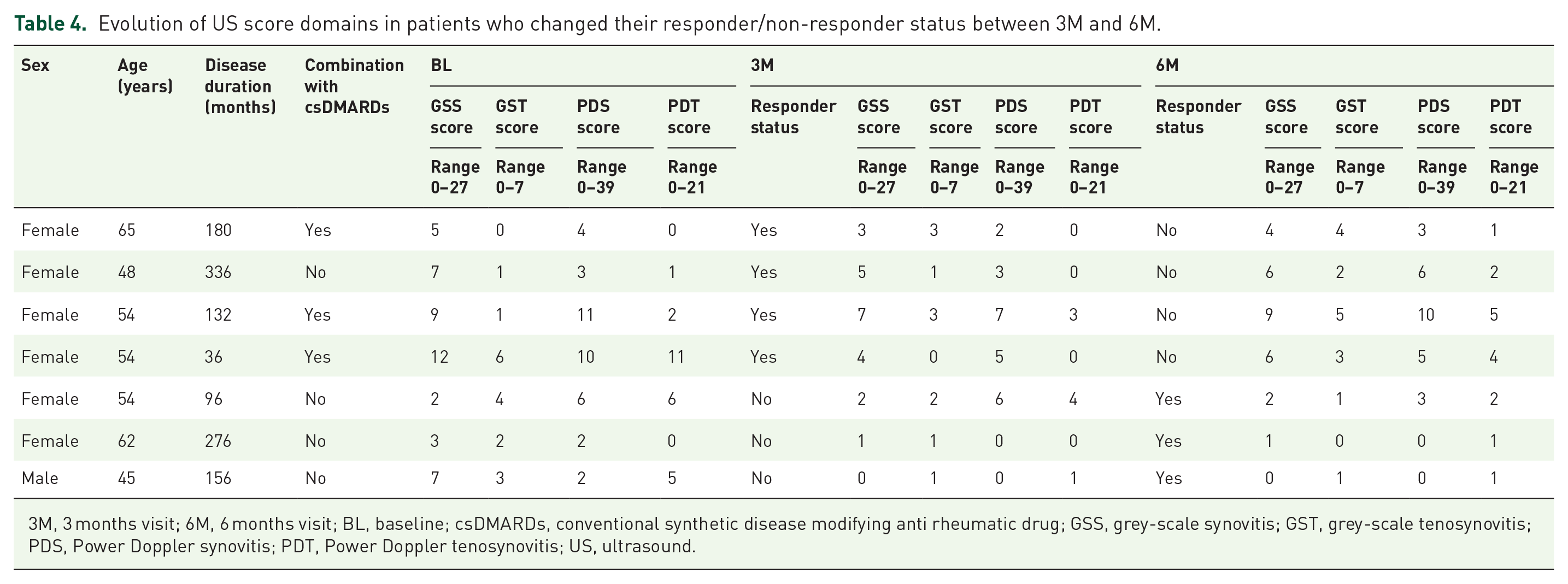
3M, 3 months visit; 6M, 6 months visit; BL, baseline; csDMARDs, conventional synthetic disease modifying anti rheumatic drug; GSS, grey-scale synovitis; GST, grey-scale tenosynovitis; PDS, Power Doppler synovitis; PDT, Power Doppler tenosynovitis; US, ultrasound.
Remission was achieved by 5/39 (12.8%) patients at 3M and 8/36 (21.6%) at 6M months, while LDA was registered in 53.8% and 51.3% patients at the respective timepoints. We identified no significant association between achievement of remission and demographic features, concomitant medication profile, serological status, and US domain scores.
Safety evaluation
Three patients dropped out from the study: two due to adverse events and one for a reason that was independent of treatment (moving to another country).
Table 5 reports the AEs that were observed during the whole study period (from BL to 6M): infections were the most frequent [7 patients from BL to 1M (18.42%), 12 patients from 1M to 3M (27.91%) and 9 patients from 3M to 6M (23.08%)], followed by nausea [3 patients (7.89%) from BL to 1M, 3 patients (6.98%) from 1M to 3M and 1 patient (2.56%) from 3M to 6M].
Distribution of AEs in the study population in the period BL–1M, 1M–3M and 3M–6M.

3M, 3 months visit; 6M, 6 months visit; AE, adverse events; BL, baseline; SAE, severe adverse event.
Liver enzyme increase and headache were rare, while six patients (15.00%) manifested anaemia between the third and the sixth month. Two patients presented with Herpes Zoster infections causing premature drug interruption. No episodes of deep venous thrombosis/pulmonary embolism or tubercular infection reactivation, were observed. During the study, two SAEs were registered, due to inguinal hernia surgery and cervical conization for a cervical intraepithelial neoplasia (CIN), both not related to Baricitinib. Disease flares were recorded for 2 patients (5.26%) from BL to 1M, 4 patients (9.30%) from 1M to 3M, and 13 patients (32.50%) from 3M to 6M visits.
Finally, we searched for factors that could predict the development of AEs. Among line of treatment after csDMARD failure, prednisone dose (at each visit), monotherapy/combination therapy, we identified the concomitant steroid dose was as the only factor associated with AEs development between the 3M and 6M [odds ratio (OR): 1.69 confidence interval (CI) (1.025–2.815) p = 0.039], with higher steroid dosages increasing the frequency of AEs. Despite this, we found no association between the average prednisone dose and any specific type of AEs.
Discussion
Our data confirm that Baricitinib is effective in patients with moderate-to-severe RA, determining a clinical, clinimetric and US improvement.
In RA, the efficacy of Baricitinib has been demonstrated previously in four registration studies, including patients with early active RA who received no or minimal treatment with csDMARDs and who were naïve to bDMARDs (RA-BEGIN), 8 RA patients bDMARD-naïve with inadequate response or intolerance to ⩾1 csDMARDs (RA-BUILD), 6 and RA-patients that have previously received ⩾1 bDMARD and discontinued because of an insufficient response or intolerance (RA-BEACON). 9 Finally, Baricitinib in combination with methotrexate showed a better clinical response than placebo and adalimumab in patients with insufficient response to methotrexate in the RA-BEAM study. 5
The results of our study, despite the small number of patients enrolled, are in line with the data reported in the literature, including other real-life cohorts, showing an improvement of all clinimetric scores and activity indexes in the entire study population, including both bDMARD-naïve and failure patients, showing a comparable percentage of patients who achieved remission.19,20
Similarly, no association was found between efficacy and BL patient characteristics when comparing responders and non-responders, in line with the data of Kremer et al. 1 The only exception is the presence of a combination therapy (Baricitinib + csDMARD), which seemed to be associated to a better response to treatment, with higher number of patients classified as responders at 3M in the combination group when compared with patients in monotherapy. We may hypothesize that the combination of Baricitinib and csDMARDs may promote the achievement of the remission/LDA earlier than Baricitinib alone. In fact, the three patients from our cohort who newly achieved the responder status between 3M and 6M were all in monotherapy with Baricitnib. These data are partially in agreement with Fleishmann et al., who presented long-term efficacy and safety data on Baricitinib monotherapy, from patients included in the RA-BEYOND extension study: among patients who showed poor disease control with Baricitinib in monotherapy at baseline, a significant improvement after methotrexate addition was achieved. 21 This is in partial agreement with what emerged from our study, where the addition of a csDMARD was not associated with a status variation at next visit (from non-responders at 3M to responders at 6M).
Interestingly, VAS-pain dropped significantly in the entire population at all follow ups. These data are in agreement with a post hoc analysis of the RA-BEAM study, in which Baricitinib demonstrated a greater and more rapid achievement of clinically significant pain relief when compared with Adalimumab or placebo. 22 In particular, the improvement of pain relief as early as week 1 was 25% for Baricitinib versus 4% for placebo (p < 0.0001), whereas the mean percentage reduction in pain from baseline at week 24 was 51% in the Baricitinib versus 39% for Adalimumab versus 17% for placebo. In addition, this analysis suggested that the ability of Baricitinib to improve pain could be explained only partially by the reduction of inflammatory markers (such as CRP levels), supporting the hypothesis of the anti-nociceptive action of JAK1 and JAK2 inhibition. 23
Considering safety, Baricitinib was suspended due to AEs in 5% of patients during the 6M of observation, and these results are consistent with other real-life national cohorts.20,21 However, we observed a few cases of Herpes Zoster infections/reactivation in 6 months of observation. We hypothesize that this might be related to the clinical practice use of steroids, not limited to a stable low-medium dose as commonly requested by clinical trials protocols. This might be supported by our findings of a positive association between the steroid dose and the risk of developing AEs. Similarly, we may hypothesize that the significant quick reduction of the steroid dose might have an impact on the numbers of disease flares we registered, in particular at 6-months evaluation (13 cases at 6M versus 4 cases at 3M versus 2 cases at 1M). Regarding laboratory parameters, our results were also consistent with literature data, showing an initial reduction in haemoglobin and increase of platelet count and lymphocytes after the first month of treatment, with subsequent stabilization and restoration of normal values, in addition to a slight transaminases increase, mainly in patients that were in combination therapy with methotrexate.24 Conversely, we observed an increase in neutrophil count rather than a decrease as reported in literature. 20 LDL and HDL were found to be significantly increased at 3M and subsequently LDL remained elevated while HDL reduced again.
In our study, US was able to reflect the trend of disease activity scores, in particular for the Power Doppler activity. In fact, PDS was the US parameter that better differentiated between responders and non-responders at 3M, confirming data from another Italian study that suggested PDS as a feasible and sensitive tool for assessing treatment response in the short term.21,25 In addition, US score domains reflected the change in responder/non-responder status, although the limited number of patients did not allow any statistical comparison.
Our study has strengths, such as the multi-dimensional evaluation of Baricitinib efficacy, including SDAI for the achievement of remission/LDA as suggested in ACR/EULAR guidelines, together with US evaluation with US7 score. In addition, we separately considered the responders and non-responders groups, in order to examine their features and better analyse the results that we found in the entire population. The main limitations of our analysis are the sample dimension, underpowered to perform smaller subgroup analysis and comparison with the results of other cohorts, as well as the retro-prospective nature of the study, which resulted in the presence of some extent of missing data. In addition, the duration of our observation may be considered short, in the light of the chronic nature of the disease, in particular for the detection of erosive changes. In this light, an extension of the duration of follow up could have been considered, in order to obtain more solid data about efficacy and safety of the drug. Despite this, we considered 3–6 months as a sufficient time to evaluate clinical treatment response, as presented by the Treat-to-Target recommendations. Finally, our analysis did not include a control group not receiving Baricitinib, which could have allowed us to compare changes in all the variables assessed, in particular the effect on pain and steroid dose reductions.
Conclusion
Our data shows real-life data of Baricitinib in RA, with a better response to therapy in patients with an elevated disease activity at baseline, as well as its ability to allow a significant reduction of pain and concomitant steroid dose. In addition, US was confirmed to be useful in monitoring disease activity and treatment response. The safety assessment showed a profile similar to the data available in literature, although identifying the concomitant steroid dosage as probable risk factor. Further studies on larger cohorts and longer follow-up observation are warranted to confirm our results.
Footnotes
Author contributions
All authors contributed to the study conception, design, and results interpretation. Material preparation, data collection, and analysis were performed by GT, CB, LC, MC, RT, and LT. The first draft of the manuscript was written by LC, GT, and CB and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Conflict of interest statement
Cosimo Bruni reports consultancy fee from Actelion, Eli Lilly; grants from Gruppo Italiano Lotta alla Sclerodermia (GILS), Fondazione Italiana Ricerca sull’Artrite (FIRA), European Scleroderma Trial and Research (EUSTAR), Foundation for Research in Rheumatology (FOREUM), Italian Society of Rheumatology (SIR), outside the submitted work.
Marco Matucci-Cerinic reports grant and personal fees from Actelion, personal fees from Biogen, personal fees from Bayer, personal fees from Boehringer Ingelheim, personal fees from CSL Behring, personal fees from Eli-Lilly, outside the submitted work.
GT, LC, FN, RT, LT, MC, FB, GF: no conflict of interest to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.