
Abstract
The crucial role of T cells in the pathogenesis of rheumatoid arthritis (RA) is well recognized. Tacrolimus is an immunomodulator that acts by the inhibition of T-cell activation. There have been numerous studies examining the use of tacrolimus in RA, including four randomized controlled trials. This article reviews these data with respect to the efficacy of the use of tacrolimus in RA as monotherapy and as part of combination therapy. The safety of tacrolimus use in RA is then evaluated. Tacrolimus is shown to be an effective and safe therapeutic option for RA patients intolerant of or resistant to previous disease-modifying antirheumatic drugs (DMARDs). In addition to monotherapy, tacrolimus has been successfully used as part of combination RA therapy, in particular in conjunction with methotrexate. Further assessment of combination approaches involving tacrolimus use alongside other DMARDs or biologics would be helpful. More studies are required to examine the effects of tacrolimus on the radiographic progression of RA.
Introduction
The management of rheumatoid arthritis (RA) has been transformed over the last few decades with advances in our understanding of the pathogenesis of RA, in particular the crucial role of T cells [Panayi et al. 1992]. Recent guidelines for the management of RA [Smolen et al. 2010] have reinforced the primary treatment aim which is disease remission in order to reduce the structural and functional impact of the disease. This goal is made more achievable by having the choice of a range of therapies with different modes of action, particularly as there are a substantial number of patients who will be resistant, intolerant or unsuitable candidates for the more widely used agents. Tacrolimus is an immunomodulator that acts by inhibiting T-cell activation. A number of clinical studies have been reported over the last decade supporting its use in RA. The aim of this review is to evaluate the efficacy and safety of tacrolimus in RA both as monotherapy and as part of combination therapy.
Tacrolimus: background and mode of action
Tacrolimus is a macrolide calcineurin inhibitor (Figure 1) isolated from Streptomyces tsukubaensis [Kino et al. 1987] and initially developed and used to prevent organ transplant rejection reactions. It acts by binding to specific intracellular proteins after entering T cells (Figure 2). The formed complex inhibits calcinuerin phosphatase, which prevents the activation of the nuclear factor of activated T cells (NF-AT), a transcription factor needed for the production of cytokines such as interleukin 2 (IL-2) and γ interferon [Miyata et al. 2005; Ho et al. 1996]. Its mechanism of action is similar to that of ciclosporin but its immunosuppressive effect has been shown to be 30–100 times greater in vitro and 10–20 times greater in vivo [Wiederrecht et al. 1993].

Molecular structure of tacrolimus, C44H69NO12•H2O.

Mechanism of action of tacrolimus. FKBP, FK506 binding protein; NFAT, Nuclear factor of activated T-cells. Illustration courtesy of Alessandro Baliani and Shouma Dutta © [2011].
Tacrolimus has also been shown to suppress inflammation by inhibiting prostaglandin E2 production from synovial cells [Sasakawa et al. 2005] and is capable of regulating matrix metalloproteinase 13 synthesis in rheumatoid synovium [Migita et al. 2005]. A further potential role for tacrolimus is overcoming drug resistance induced by P-glycoprotein (P-gp) on lymphocytes in patients with refractory RA. Tacrolimus is a competitive inhibitor of P-gp and can improve the therapeutic levels of corticosteroids, which are P-gp substrates [Suzuki et al. 2010; Tsujimura et al. 2008].
As tacrolimus is metabolized by the cytochrome P450 enzyme system (CYP3A) it is important to be aware that medications acting as CY3PA enzyme inhibitors or inducers may respectively increase or reduce blood concentrations of tacrolimus.
Clinical efficacy in randomized controlled trials
The efficacy of tacrolimus monotherapy use in RA has been studied in four double-blind randomized controlled trials (RCTs) (Table 1) and one meta-analysis [Lee et al. 2010]. Table 2 details the American College of Rheumatology 20% (ACR 20), ACR 50 and ACR 70 responses observed with tacrolimus 3 mg versus control. The highest ACR 20 response rates were seen in the Japanese studies, in which they approached 50%, whilst a lower rate of approximately 30% was found in the US studies. This may reflect differences in the populations, including body weight, and differences in prior use of disease-modifying antirheumatic drugs (DMARDs). Kawai and colleagues acknowledged that since the highest approved dose of methotrexate (MTX) in Japan at the time of this study was 8 mg/week, those patients previously resistant to MTX in Japan may well have responded to the higher doses of MTX used in the USA [Kawai et al. 2006]. Other potential confounding factors in these studies include the lack of a prior DMARD washout period in the study by Kondo and colleagues [Kondo et al. 2004] and the high withdrawal rate in the study by Yocum and colleagues [Yocum et al. 2003]. Only 46.9% of tacrolimus-treated patients completed 6 months of therapy, including 19.9% of tacrolimus-treated patients withdrawn for administrative reasons.
Overview of randomized, double-blind, controlled trials of tacrolimus in RA.

ACR 20 response, American College of Rheumatology 20% response; ACR 20 success, American College of Rheumatology 20% response on completion of the study; DMARD, disease-modifying anti-rheumatic drug; MTX, methotrexate; TAC, tacrolimus; tds, three times daily.
Efficacy results from randomized controlled trials with tacrolimus 3 mg per day versus control.
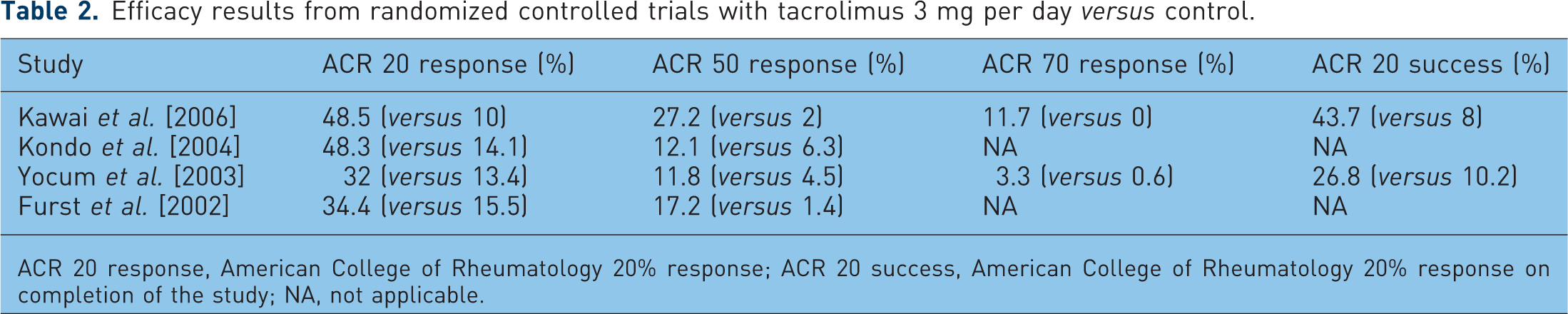
ACR 20 response, American College of Rheumatology 20% response; ACR 20 success, American College of Rheumatology 20% response on completion of the study; NA, not applicable.
All of the RCTs that incorporated different tacrolimus dose groups [Kondo et al. 2004; Yocum et al. 2003; Furst et al. 2002] demonstrated that ACR 20 response rates increased dose-dependently. Statistically significant differences in ACR 20 response rates were observed between the 3 mg and placebo groups in each study and also between the 5 mg and placebo groups in the study by Furst and colleagues [Furst et al. 2002]. However, no statically significant differences were found between the placebo and lowest dose groups (1 mg, 1.5 mg, 2 mg) in each study. The ACR 50 response rates for each of the tacrolimus dose groups (1–5mg) in the US studies [Yocum et al. 2003; Furst et al. 2002] were significantly higher than those in the groups receiving placebo. No significant differences in the ACR 50 response rates were found, however, between either of the tacrolimus dose groups and placebo in the study by Kondo and colleagues [Kondo et al. 2004].
The importance of functional and quality of life outcome measures is increasingly being recognized in guiding RA management. Modified Health Assessment Questionnaire (M-HAQ) information was included in the studies. Kawai and colleagues reported a significantly greater M-HAQ score improvement of −0.21 in the tacrolimus group versus +0.17 in the mizoribine group [Kawai et al. 2006]. Both the 2 mg and the 3 mg tacrolimus groups in the study by Yocum and colleagues also showed significantly greater improvements in M-HAQ scores compared with placebo [Yocum et al. 2003].
Additional subanalysis showed that DMARD-intolerant patients responded better to tacrolimus compared with DMARD-resistant patients in the study by Yocum and colleagues [Yocum et al. 2003]. Both the 2 mg and the 3 mg dose groups among the DMARD-intolerant patients achieved statistically higher ACR 20 and ACR 50 response rates and ACR 20 success rates compared with placebo-treated patients. In the study by Kondo and colleagues, however, MTX-resistant patients had a significantly higher ACR 20 response rate than placebo-treated patients for both the 3 mg and the 1.5 mg dose groups [Kondo et al. 2004]. This was in contrast with results from whole-group analysis and the patient group resistant to all DMARDs except MTX, both of which showed statistically higher ACR 20 response rates than placebo-treated patients for the 3 mg group only. The subgroup analysis in the study by Kawai and colleagues revealed better ACR 20 and ACR 50 response rates for patients with an insufficient response to DMARDs other than MTX compared with those with an insufficient response to MTX [Kawai et al. 2006]. When considering the data for the Japanese studies, however, it is again important to be mindful of differences that exist in international DMARD prescribing practices with respect to both dose (lower maximum MTX doses are approved in Japan than in the USA) and DMARD choice.
Efficacy evidence from other open-label studies
The largest multicentre open-label long-term study to date was reported by Yocum and colleagues, with the primary objective of evaluating the safety of tacrolimus 3 mg per day in RA patients [Yocum et al. 2004]. The primary efficacy endpoint was ACR 20 response at the end of treatment. A total of 896 patients were enrolled from two groups: those recruited directly into the study and those who were eligible to roll over from the placebo, 2 mg and 3 mg dose groups from a previous RCT [Yocum et al. 2003]. All patients received tacrolimus 3 mg monotherapy with a follow up of 12 months. The overall ACR 20 response rate at the end of treatment was 38.4%, with a higher rate (46.4%) found amongst patients who had previously been treated with tacrolimus compared with the new starters (35.9%). This result may have been influenced by some selection bias. Lack of efficacy was the reason for withdrawal for 12.5% of the patients from the study.
Elderly patients were the focus of another prospective open-label, noncontrolled study [Kawai and Yamamoto, 2006]. A total of 57 RA patients aged 65 years or more who had an insufficient response to at least one prior DMARD were treated with tacrolimus for 28 weeks. The starting dose was 1.5 mg/day, increasing to 3 mg/day after 6 weeks if no abnormal changes developed. The ACR 20 response rate was 50%, similar to the Japanese RCT findings involving RA patients younger than 65.
Efficacy evidence for combination therapy
Combination DMARD therapy including MTX is increasingly being used when MTX monotherapy is insufficient to fully control RA disease activity. Several studies have reported on the benefits of this combination DMARD therapy approach [Kremer et al. 2002; Weinblatt et al. 1999; Tugwell et al. 1995]. Kremer and colleagues conducted a prospective 6-month open-label study examining the use of tacrolimus in 80 active RA patients receiving concomitant oral MTX (5–20 mg/week) [Kremer et al. 2003]. Tacrolimus 3 mg daily was used and all other DMARDs were discontinued. ACR 20, ACR 50 and ACR 70 response rates at the end of treatment were 52.5%, 28.8% and 13.8% respectively, with a low rate of withdrawal due to lack of efficacy (5%). These results compared favourably with those reported in other, earlier studies when MTX was used in combination with other DMARDs. An RCT would be helpful, however, by providing more robust evidence with respect to the efficacy of combination tacrolimus and MTX therapy.
Combination therapy including anti-tumour necrosis factor (anti-TNF) agents and tacrolimus has not been studied to any great extent. A retrospective study was undertaken assessing the efficacy of low-dose tacrolimus (1.5–2 mg/day) as add-on therapy for five patients with resistant RA despite treatment with MTX and anti-TNF therapy [Naniwa et al. 2009]. The triple combination treatment period was between 1 and 2.5 years. At the point of starting tacrolimus, the anti-TNF agents being used were etanercept (three patients, duration of use ≥1.7 months prior to tacrolimus) and infliximab (two patients, duration of use >3 months prior to tacrolimus). Two of the etanercept-treated patients had not responded to infliximab previously. All were receiving low-dose prednisolone (≤10 mg/day). At 1 year, three patients were in remission and two had moderately active disease. Clearly, further controlled studies involving larger patient numbers would be required to make clear judgements on the efficacy of this therapeutic approach.
Safety of tacrolimus use in RA
Overview
Gastro-intestinal (GI) tract-related adverse events were amongst the most common reported across all the tacrolimus dose groups studies in the four RCTs (Table 3) and the 12-month open-label study by Yocum and colleagues [Yocum et al. 2004] (Table 4). In addition, significantly higher rates of nervous system-related adverse events (including tremor and anxiety) occurred amongst the 5 mg tacrolimus dose group compared with placebo [Furst et al. 2002]. Amongst tacrolimus users, a higher incidence of adverse events involving any system was reported in the RCTs in the USA (80–92.8%) compared with the RCTs from Japan (44.4–65%) and the open-label study by Yocum and colleagues [Yocum et al. 2004] (59%, possibly or probably related to tacrolimus). However, a higher incidence of adverse events was also seen in the placebo groups in the RCTs in the USA. The overall withdrawal rate due to adverse events within the RCT studies ranged between 4% and 16%. No statistically significant differences were found in the number of withdrawals due to adverse events between the tacrolimus dose groups (1.5–2 mg and 3 mg) and placebo in the meta-analysis [Lee et al. 2010].
Adverse events with tacrolimus from randomized controlled trials.

Significantly different compared with placebo.
No ranking information available.
No statistically significant differences found compared with control in any adverse event.
1–4, most frequent adverse event to fourth most frequent adverse event.
AE, adverse event; GI, gastrointestinal; NA, information not available; UTI, urinary tract infection.
Adverse events with tacrolimus in open-label studies.

Leading adverse events are ranked in order of decreasing frequency; for Kawai and Yamamoto [2006] only clinical adverse events are listed.
Results of adverse events possibly or probably related to tacrolimus in the opinion of an investigator.
Yocum et al. 3 mg dose group: some patients who were part of a previous randomized controlled trial could have had up to 18 months of tacrolimus exposure in total;
AE, adverse events; GI, gastrointestinal; MTX, methotrexate; NA, information not available.
Renal function-related adverse effect profile
Serum creatinine and glucose levels and blood pressure were monitored in some of the studies, given prior clinical experiences of tacrolimus use in the transplant setting. Approximately one third of patients on tacrolimus 3 mg experienced an increase in their baseline creatinine levels of ≥30% at any study time point (33.8% versus 16.1% for placebo [Yocum et al. 2003] and 34.4% versus 9.8% for placebo [Furst et al. 2002]). Higher proportions were reported in the longer open-label study by Yocum and colleagues [Yocum et al. 2004] (40.3%) and amongst the 5 mg tacrolimus dose group in the RCT reported by Furst and colleagues [Furst et al. 2002] (39%). In the lower dose groups, fewer patients experienced this rise. Creatinine levels requiring discontinuation were reported as 2.6% and 3.1% for the 3 mg group [Yocum et al. 2003; Furst et al. 2002] and 10.9% for the 5 mg group [Furst et al. 2002].
Blood pressure- and glucose-related adverse effect profile
No significant increases in mean systolic blood pressure levels were seen in the open-label study by Yocum and colleagues [Yocum et al. 2004] and between any dose group (1–5 mg) compared with placebo in the study by Furst and colleagues [Furst et al. 2002]. This finding was also noted when comparing the 3 mg dose group and placebo in the RCT by Yocum and colleagues [Yocum et al. 2003]. A statistically significant increase in mean diastolic pressure was found in the open-label study by Yocum and colleagues [Yocum et al. 2004] (78.3 mmHg at baseline versus 79.5 mmHg at the end of treatment), but this was not considered to be clinically significant. The frequency of upward shifts in diastolic pressure reported by Furst and colleagues [Furst et al. 2002] was also statistically significantly higher in the 3 and 5 mg dose groups versus placebo, but again the absolute changes were considered to be relatively small. Treatment-emergent hypertension was not more common in these dose groups either. Yocum and colleagues in their 12-month study noted that hypertension was reported as a treatment-emergent adverse event, possibly or probably related to tacrolimus, for 3% of patients [Yocum et al. 2004].
On assessing mean changes in serum glucose and HbA1c from baseline to the end of treatment, no significant differences between any of the tacrolimus dose groups versus placebo were found by Furst and colleagues in their study [Furst et al. 2002]. In the 12-month study by Yocum and colleagues, new-onset diabetes was reported as a treatment-emergent adverse event possibly related to tacrolimus for 0.3% of patients [Yocum et al. 2004]. In another prospective, open-label, uncontrolled study [Kawai et al. 2008] involving 115 Japanese patients receiving oral tacrolimus ≤3 mg daily for 76 weeks, increased blood glucose and HbA1C levels were reported as adverse events with a possible relationship to tacrolimus in 2.6% (n = 3) and 7% (n = 8) of patients respectively. Two patients from each of these adverse event groups had their treatment discontinued, following which the authors reported there was an improvement in levels.
Safety of tacrolimus use in elderly RA patients
Elderly RA patients aged ≥65 were the focus of a prospective open-label safety report [Kawai and Yamamoto, 2006] (Table 4). A starting tacrolimus dose of 1.5 mg daily could be increased to 3 mg daily if the treatment was well tolerated and the serum creatinine, fasting glucose, HbA1C and tacrolimus levels were within the parameters set out in the study protocol. Skin and appendage disorders were the most frequent clinical adverse events, followed by GI disorders. Increased serum glucose, HbA1C and creatinine levels occurred in 3.7%, 3.7% and 14.8% of patients respectively. Details regarding the degree of increase in each level were not given and the likelihood of a relationship between the blood changes and tacrolimus was not commented on. In the open-label study by Yocum and colleagues, the overall incidence of adverse events was reported to be similar in patients less than 65 and those 65 years of age or older [Yocum et al. 2004].
Safety of tacrolimus use in combination with methotrexate
The safety of tacrolimus use in combination with MTX for RA patients was assessed in the open-label study by Kremer and colleagues [Kremer et al. 2003] (Table 4). The incidence of adverse events overall was similar between the low- and high-dose MTX groups. These figures were similar to the incidence reported in the monotherapy tacrolimus study by Yocum and colleagues whose total adverse advent rate was 88.3% [Yocum et al. 2004]. A higher proportion of patients in the low-dose MTX group discontinued the study because of adverse effects compared with the high-dose MTX group (22.9% versus 4.4%). The more common adverse events leading to discontinuation were tremor and nausea. Pancreatitis was the one serious adverse event reported that was considered to be possibly related to tacrolimus. During treatment, an increase in creatinine of ≥30% from baseline occurred in 28.8% of patients. This was a lower incidence rate than that in the monotherapy tacrolimus 3 mg dose groups [Yocum et al. 2003,Yocum et al. 2004 and Furst et al. 2002]. Of the patients whose creatinine did rise ≥30% above baseline in this study by Kremer and colleagues, levels returned to baseline in 44% of patients [Kremer et al. 2003]. This included patients whose treatment was interrupted and uninterrupted. Creatinine levels were not monitored for a return to baseline in some of the remaining patients.
Tacrolimus blood concentrations
Tacrolimus blood concentration observations were included in some of the RA studies. In the renal transplant setting, where tacrolimus doses higher than those in the RA setting are used, higher incidences of adverse effects have been found in patients with higher tacrolimus blood concentrations (≥10 ng/ml) [Böttiger et al. 1999]. In the RCT reported by Kawai and colleagues, in which RA patients took a 3 mg daily dose, a tacrolimus level >10 ng/ml was found in 10 patients [Kawai et al. 2006]. Seven of these patients experienced nonserious adverse events. However, mean tacrolimus levels amongst patients who experienced adverse events overall were not different from those without adverse events. In the RCT by Yocum and colleagues, median trough levels were 2–3 ng/ml and the tacrolimus did not accumulate over the course of the study [Yocum et al. 2003]. Similar mean trough levels were found at the end of treatment for patients receiving tacrolimus in combination with MTX (2.9 and 2.6 ng/ml in the low-dose and high-dose MTX groups, respectively [Kremer et al. 2003]).
Conclusion
Tacrolimus has been shown to be an effective and safe therapeutic option for RA patients intolerant of or resistant to previous DMARDs, including MTX. ACR 20 response rates increased with increasing doses in all of the RCTs that incorporated different tacrolimus dose groups. The nephrotoxicity problems associated with the 5 mg daily dose, however, preclude this from being the optimum suggested therapeutic dose. The incidence of adverse events associated with tacrolimus use for RA patients appears to be much less than incidences found in the transplant setting. This was probably due to the lower doses of tacrolimus used in RA. There is little evidence to support its use as first-line therapy, but when conventional DMARDs have failed or biological agents are not an option, tacrolimus 3 mg per day could be an alternative option as monotherapy or in combination with MTX. Further analysis of the role of tacrolimus when used alongside other DMARDs or biologics in patients with resistant RA would be helpful. Finally, the lack of evidence regarding the effect of tacrolimus on radiographic progression of RA needs to be addressed with further studies.
Footnotes
This work received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
The authors declare that there was no conflict of interest in preparing this article.