
Abstract
Background:
Immune checkpoint inhibitors (ICIs) improved cancer therapy by inducing a higher immune system activity. This effect can cause rheumatic immune-related adverse events (rh-irAEs), which have not yet been extensively studied.
Methods:
We analysed 437 patients between 2014 and 2019, treated with ipilimumab (anti-CTLA-4) and/or nivolumab (anti-PD-1) or pembrolizumab (anti-PD-1) at the Clinic for Internal Medicine III, Oncology, Haematology and Rheumatology at the University Hospital Bonn, Germany.
Results:
Of the 437 patients 60% were males. Patients were mainly treated for melanoma, lung cancer, head and neck tumour and urothelial carcinoma. At least one immune-related adverse event (irAE) was observed in 163 patients (37.3%), including rh-irAE. Most common side effects were rash, colitis and hepatitis. We identified 19 patients (4.3%) with a minimum of one rh-irAE due to ICI therapy; three of those had a pre-existing rheumatic disease. Arthralgia developed most frequently in eight patients (42.1%). Other rh-irAEs were: arthritis (n = 7; distinguished in rheumatoid arthritis, psoriatic arthritis, juvenile idiopathic arthritis and undifferentiated arthritis), myalgia (n = 2) and myositis (n = 3). Most rh-irAEs were classified as moderately severe (Common Terminology Criteria of Adverse Events grade 2: 68.4%). Median time between starting ICI therapy and the occurrence of rh-irAE was 109 days (interquartile range 40–420 days). Fifteen patients (78.9%) were treated with glucocorticosteroids. In four cases additional therapy with methotrexate or tocilizumab was required. Even though patients benefited from ICI treatment, therapy had to be discontinued in six of the participants due to rh-irAE. Interestingly, patients with rh-irAE had a significantly higher tumour response compared with patients without rh-irAE (94.4% versus 43.5%; p < 0.0001).
Conclusion:
Rh-irAEs occur under ICI therapy, especially in patients with higher tumour response. However, they are not the most frequent irAE after ICI exposure: 9.3% of all irAEs were rheumatic (20 rh-irAE cases in 19 patients of a total of 215 irAE cases in 163 patients).
Keywords
Introduction
Immune checkpoint inhibitors (ICIs) have accelerated the immunotherapy revolution in cancer therapy and improved clinical outcomes for oncological patients. 1 ICIs are newly developed monoclonal antibodies and play a crucial role in immune system activity.
The mechanism of ICI therapy is complex. The adaptive immune system plays an important role in the surveillance of the organism. Costimulatory and coinhibitory immune checkpoints (ICs) are provided for the regulation of the adaptive immune system. Stimulating ICs enables immune reactions and tumour cell elimination. The inhibitory function is important to prevent excessive immune response and autoimmunity. 2 However, many malignancies escape the immune response directed against them by expressing receptors and activating inhibitory ICs. This immune evasion of tumour cells is mainly the therapeutic starting point of ICI therapy. With the help of ICIs, T-cells can attack the tumour cells.
Cytotoxic T-lymphocyte antigen 4 (CTLA-4) and programmed cell death protein 1 (PD-1) have been most extensively evaluated in clinical practice. Ipilimumab (anti-CLTA-4) can be used in the treatment of patients with melanoma. 3 Pembrolizumab and nivolumab are antibodies against PD-1. Both are approved for several cancer entities, including melanoma, non-small-cell lung cancer, Hodgkin’s lymphoma, head and neck carcinoma, urothelial carcinoma and renal cell cancer. 4 Besides the option of ICI monotherapy, patients with melanoma or renal cell cancer have the opportunity to be treated with a combination therapy of ipilimumab and nivolumab. This dual blockade shows an increased antitumour effect. 5
Due to the suppression of inhibitory function and subsequent increasing immune response, ICI treatment is associated with various adverse effects, known as immune-related adverse events (irAEs), affecting nearly every organ system.6–8 Colitis and rash occur most frequently. 9 Rheumatic irAEs (rh-irAEs) are also described and have not been extensively studied and characterized yet. Arthralgias have been described in 1–43% 10 of patients receiving either single ICI or combination therapy. Despite this high frequency, the classification of rh-irAEs remains limited.10–14 Several institutions have reported the occurrence of rh-irAEs in a small number of patients. 15 Despite these reports, gaps in our understanding of this entity remain.
In this single centre study, we aimed to add important information regarding prevalence and type of rh-irAEs, as well as duration, therapy, laboratory findings, description of differences between patients with and without pre-existing rheumatic diseases and correlation between tumour response rate compared with patients with or without rh-irAEs.
Patients and methods
Patients
In this retrospective study, all patients were >18 years old and were treated for a malignancy with ICIs at the University Hospital Bonn, Germany. We analysed 437 patients treated with ipilimumab (anti-CTLA-4) and/or nivolumab (anti-PD-1) or pembrolizumab (anti-PD-1). We selected these three ICIs as they were already approved in Germany when our data collection started and were used in our clinic to treat various cancer entities. Our study focused on both PD-1 and CLTA-4 antibodies, despite their different mechanisms, in order to provide a realistic overview of ICIs used in clinical practice.
Patients were included between 1 January 2014 and 31 December 2018. Follow-up was conducted until 31 October 2019. Patients with pre-existing rheumatic diseases were included in this study.
Medical records of patients were reviewed and irAEs as well as rh-irAEs related to ICI therapy were identified. We examined the following rheumatic diseases or rheumatic symptoms: arthralgia, myalgia, arthritis, tenosynovitis, myositis, vasculitis, Sicca syndrome, Sjogren’s syndrome, polymyalgia rheumatica (PMR), systemic lupus erythematosus, sarcoidosis, dermatomyositis, polymyositis, eosinophilic fasciitis and giant cell arteritis. Below, we will only mention the rheumatic diseases that occurred in our patients. We did not investigate the occurrence of osteoarthritis. Severity of irAEs was graded according to Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. 19 Prednisolone doses were graded according to Buttgereit et al., 20 low dose ⩽7.5 mg, medium dose >7.5 mg to ⩽30 mg, high dose >30 mg to ⩽100 mg, very high dose >100 mg and pulse therapy ⩾250 mg prednisolone. The Karnofsky Performance Score (KPS) was defined by Karnofsky and Burchenal. 21 The tumour stage of melanoma skin cancer was classified according to the American Joint Committee on Cancer (AJCC). 22
We investigated 437 patients with first-line, 58 patients with second-line and 11 patients with third-line ICI therapy. Unless otherwise stated, all information refers to first-line therapy.
All patients with rh-irAEs were seen by a rheumatologist at the time of event occurrence. All cases were again reviewed by a rheumatologist (VSS) to confirm the presence of a rh-irAE.
Patient and disease related characteristics, type of cancer, previous treatment, occurrence of other irAEs and tumour response rate according to ICI therapy were also recorded for every patient. Tumour response, defined by RECIST version 1.1, 23 was classified as: complete response (CR), partial response (PR), stable disease (SD) and progressive disease (PD). In general CR, PR and SD were noted as tumour response. Non-responders suffered from PD.
Local ethics committee approval was obtained from the University Hospital Bonn, Germany (Lfd.Nr.010/19). Due to the retrospective study design, no consent form was needed, as advised by the local ethics committee.
The data underlying this article are available in the article and in its Supplemental Material online.
Statistical analysis
Statistical analyses were performed using SPSS version 26 (IBM). Descriptive data evaluation and explorative data analysis were used. Comparison among groups with different variables was assessed by Chi-square test. p values <0.05 were considered statistically significant, whereby p values are only reported in an explorative analysis and are therefore not corrected for multiple testing. Progression-free survival (PFS) in different cohorts [patients without irAEs, with non-rheumatic irAEs (non-rh-irAE) and with rh-irAEs] was compared with the Kaplan–Meier method. To evaluate a distinction of these cohorts, log rank test was applied. A Cox proportional hazards regression model with time-dependent covariates was used to examine associations between the occurrence of adverse events (rh-irAEs and non-rh-irAEs) and PFS. The time-dependent covariates had an initial value of 0 and were set to 1 after the first occurrence of rh-irAEs or rather non-rh-irAEs. This analysis was conducted in R (Version 4.0.3) 24 with the survival package by Therneau. 25
Results
Patient characteristics
We included 437 patients treated with ICIs. Demographic data, type of cancer, cancer therapy, previous treatment, tumour response and other non-rh-irAEs for all patients and for patients with rh-irAEs are listed in Table 1.
Demographic data and characteristics of all patients and of patients with rheumatic immune-related adverse events (rh-irAEs).
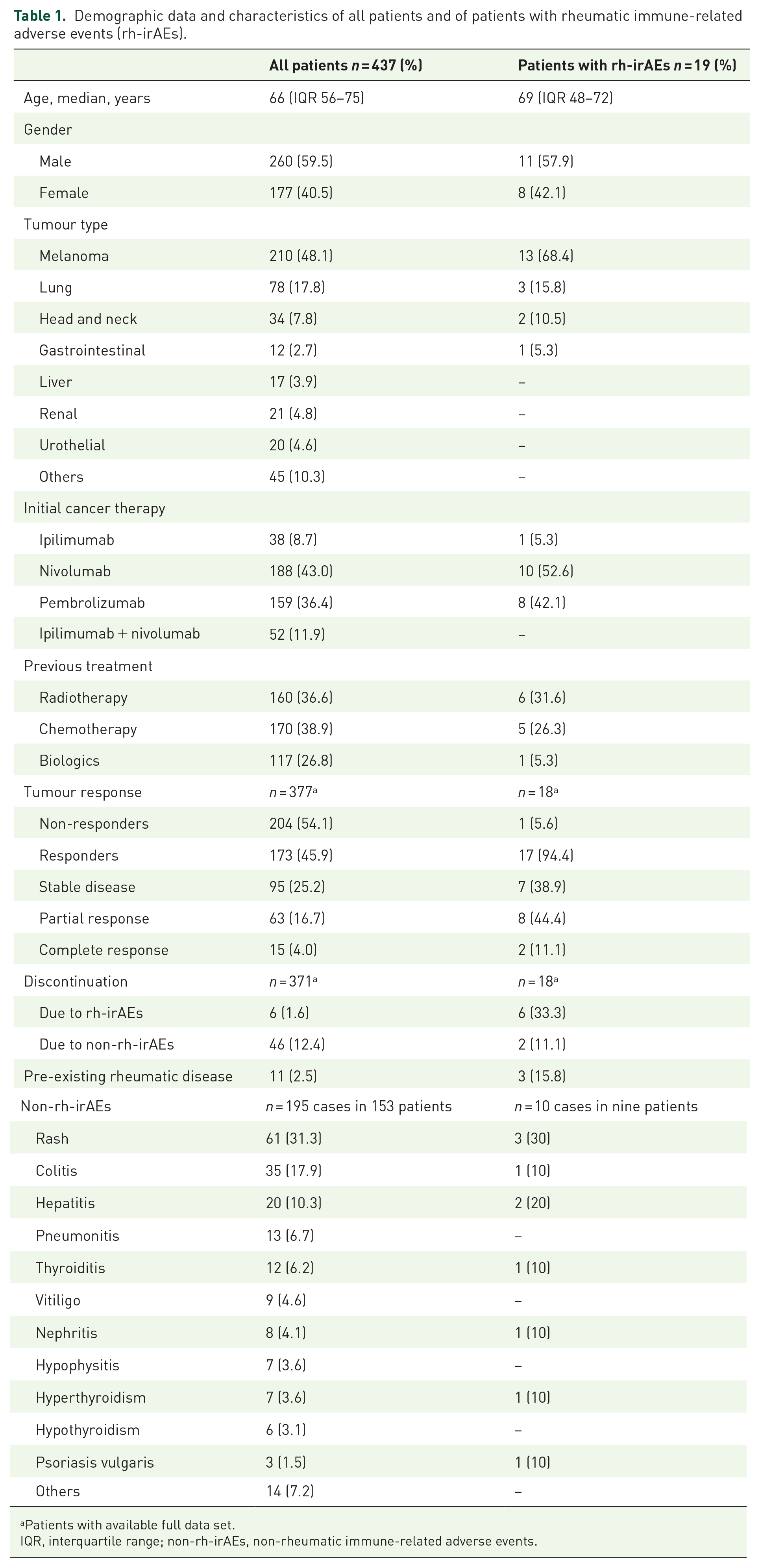
Patients with available full data set.
IQR, interquartile range; non-rh-irAEs, non-rheumatic immune-related adverse events.
Median ICI treatment time was 69 days [interquartile range (IQR) 28.5–187 days]. Most common reasons for discontinuation of ICI therapy were: progressive disease in 164 patients (37.5%), any irAE in 52 patients (11.9%) and stable disease or complete response in 19 patients (4.3%). Death occurred in 51 patients (11.7%) during ICI therapy; 20 patients (4.6%) continued the therapy beyond the follow-up time. Other reasons for discontinuing ICI therapy were: deterioration of general condition, change of location, end of therapy, change of therapy or patient’s request. In 66 patients (15.1%) the reason for discontinuing ICI therapy remained unknown as some patients were treated in different clinics.
Adjunctive radiotherapy was administered to 46 patients (10.5%) and 23 patients (5.3%) were treated with chemotherapy at the same time of ICI treatment. Five patients received additional radiotherapy and chemotherapy. Fifteen patients (3.4%) who were treated with additional chemotherapy received a fixed therapy scheme with pembrolizumab, pemetrexed and cisplatin.
In addition, we recorded pre-existing diseases and complaints of every patient. An overview is displayed in the Supplemental Material (Supplemental Table S1).
Characteristics of rh-irAEs
We identified 19 patients (4.3%) in first-line ICI therapy with a minimum of one rh-irAE due to ICI therapy, with a total of 20 rh-irAE cases (Table 1). The median time between first exposure to ICIs and the occurrence of rh-irAEs was 109 days (IQR 40–420 days).
In first-line ICI therapy one in 38 patients (2.6%) treated with ipilimumab, 10 in 188 patients (5.3%) treated with nivolumab and eight in 159 patients (5.0%) treated with pembrolizumab were affected by at least one rh-irAE. We observed rh-irAEs only in first-line ICI monotherapy. In second-line therapy four out of five patients with rh-irAEs received a combination therapy with ipilimumab and nivolumab. Rh-irAEs were observed in 19% of patients with second-line combination ICI therapy. In the other patient, rh-irAE occurred under pembrolizumab as second-line therapy. In third-line ICI therapy none of the 11 patients developed rh-irAEs.
Arthralgia developed most frequently in eight of the 19 patients (42.1%), arthritis in seven (36.8%), myalgia in two (10.5%) and myositis in three patients (15.8%). Further information and clinical characteristics of rh-irAEs are displayed in Table 2. All rh-irAEs were reviewed by a rheumatologist to confirm the occurrence of a rh-irAE. Myositis as a severe rh-irAE was diagnosed in the synopsis of the clinical presentation, a muscle biopsy was performed in one case, electromyography performed in two cases and myositis-associated and specific antibodies tested in two cases.
Clinical characteristics of rheumatic immune-related adverse events (rh-irAEs).

Excluding patients with arthritis.
Patients with available full data set.
ICI, immune checkpoint inhibitor; IQR: interquartile range; MTX: methotrexate; NSAID: non-steroidal anti-inflammatory drug.
Individual treatment and detailed information on every patient with rh-irAE in first- and second-line ICI therapy are listed in Table 3.
Characteristics of patients with rheumatic immune-related adverse events (rh-irAEs).

Patients 1 to 19: first-line ICI therapy, patients 20 to 24: second-line ICI therapy. (In only 13 patients were laboratory values examined).
ANA: anti-nuclear antibodies; anti-CCP: anti-citrullinated peptide; CTCAE: Common Terminology Criteria for Adverse Events; F, female; GC: glucocorticosteroid; MTX: methotrexate; M, male; NSAID: non-steroidal anti-inflammatory drug; RF: rheumatoid factor.
Most rh-irAEs were classified as moderately severe: in first-line ICI therapy two out of 19 patients (10.5%) reported CTCAE grade 1, 13 patients (68.4%) CTCAE grade 2 and four patients (21.1%) CTCAE grade 3.
In 13 of the 19 patients, rheumatological laboratory parameters were ordered. Nine patients were tested for anti-citrullinated peptide-antibodies (CCP) and 10 patients for rheumatoid factor (RF). One patient (number 6 in Table 3) was found to be positive for both parameters. He was diagnosed with RF- and CCP-antibody-positive rheumatoid arthritis (RA). In eight patients presence of anti-nuclear antibodies was examined and found to be elevated in one patient with myositis (1:1280) and one patient with arthralgia (1:320), both with granular fluorescence pattern. Out of four patients tested for anti-neutrophil cytoplasmic antibodies, no one was found to be positive.
Patients were most frequently treated with glucocorticosteroids (GCs). The majority of these patients received prednisolone therapy, with a median maximum dose of 25 mg (range 15–80 mg). No patient received a low GC dose, seven patients received a medium dose, five patients received a high dose and no patient received a very high dose. Two patients underwent intravenous steroid pulse therapy with either 250 mg or 500 mg, while in one patient the maximum GC dose remained unknown. The median duration of GC therapy (including tapering) was 92.5 days (range 41–189 days). In a few cases methotrexate (MTX) or tocilizumab was administered. Different treatment options and outcomes of rh-irAEs are displayed in Table 2.
Six of the 19 patients had to discontinue ICI therapy as a consequence of rh-irAE (Table 2). Other patients discontinued ICI therapy later because of tumour progression (n = 3), CR (n = 1), SD (n = 1), a non-rh-irAE (n = 2), end of therapy (n = 2) or change of therapy location (n = 1). Two patients continued ICI therapy beyond the follow-up time of this study. In one patient the reason for the end of ICI therapy remained unknown.
Pre-existing rheumatic diseases
Of all 437 patients, 11 patients (2.5%) had a minimum of one pre-existing rheumatic disease. Five patients out of 11 (45.5%) were diagnosed with RA, two patients (18.2%) with ankylosing spondylitis. Other rheumatic diseases, such as juvenile idiopathic arthritis (JIA), polymyositis, polymyalgia rheumatica, psoriatic arthritis and systemic lupus erythematosus occurred once each. Of these 11 patients, three patients (27.3%) developed a rh-irAE.
Three out of 19 rh-irAE patients (15.8%) had a pre-existing rheumatic disease. Two patients with RA experienced a disease flare. One patient with JIA suffered from an arthritis flare. In none of the three patients did ICI therapy have to be terminated due to disease flare. Four patients with rh-irAE suffered from psoriasis. Two of them developed a psoriatic arthritis under ICI therapy.
The median time between first exposure to ICIs and the occurrence of rh-irAEs in patients with pre-existing rheumatic disease was 30 days (range 15–365 days).
Relation to other irAEs
Overall, 153 of all 437 patients (35%) displayed at least one non-rh-irAEs, 35 of them suffered from a second irAE and seven of them displayed three irAEs. In total, there were 195 cases of non-rh-irAEs in 153 patients. Rh-irAEs occurred less frequently compared with other non-rh-irAEs: 9.3% of all irAEs were rheumatic (20 rh-irAE cases in 19 patients of a total of 215 irAE cases in 163 patients). Most common irAEs were rash, colitis and hepatitis (Table 1). More detailed information of all non-rh-irAEs can be found in the Supplemental Material (Supplemental Table S2). Median time to development of a non-rh-irAE was 60 days (IQR 30–145 days). Non-rh-irAEs were observed in nine patients with rh-irAE (47.4%). Patients without rh-irAE suffered from non-rh-irAE in 34.4% of patients. We did not observe a significant correlation between the occurrence of rh-irAEs and non-rh-irAEs in general (p = 0.248).
The severity of non-rh-irAEs was distributed as follows: CTCAE grade 1 in 32.5% of patients, CTCAE grade 2 in 40.8%, CTCAE grade 3 in 25.1%, while three patients (1.6%) were affected by CTCAE grade 4.
Tumour response according to rh-irAEs
Exact data on tumour response to ICI therapy were reported in 377 patients out of 437 patients. For 60 patients we lacked the exact data because the patients came from other clinics within the University Hospital Bonn. A summary of tumour response in all patients and in patients with rh-irAE is given in Table 1. In general, a treatment response was observed in 173 patients (45.9%), including CR (n = 15, 4.0%), PR (n = 63, 16.7%) and SD (n = 95, 25.2%). PD (non-responders) was observed in 204 patients (54.1%). Rh-irAEs were found in 17 patients (9.8%) of responders and in one patient (0.5%) of non-responders.
Patients with rh-irAEs had a significantly higher tumour response rate compared with patients without rh-irAEs (94.4% versus 43.5%; p < 0.0001). In addition, patients with rh-irAEs had a better tumour response than patients with non-rh-irAEs (94.4% versus 62.4%; p = 0.007). The comparison of tumour response in different cohorts (patients without irAEs, with non-rh-irAEs and with rh-irAEs) is listed in Table 4.
Comparison of best tumour response to immune checkpoint inhibitors in patients without immune-related adverse events (irAEs), patients with non-rheumatic irAEs (non-rh-irAEs) and in patients with rheumatic irAEs (rh-irAEs).
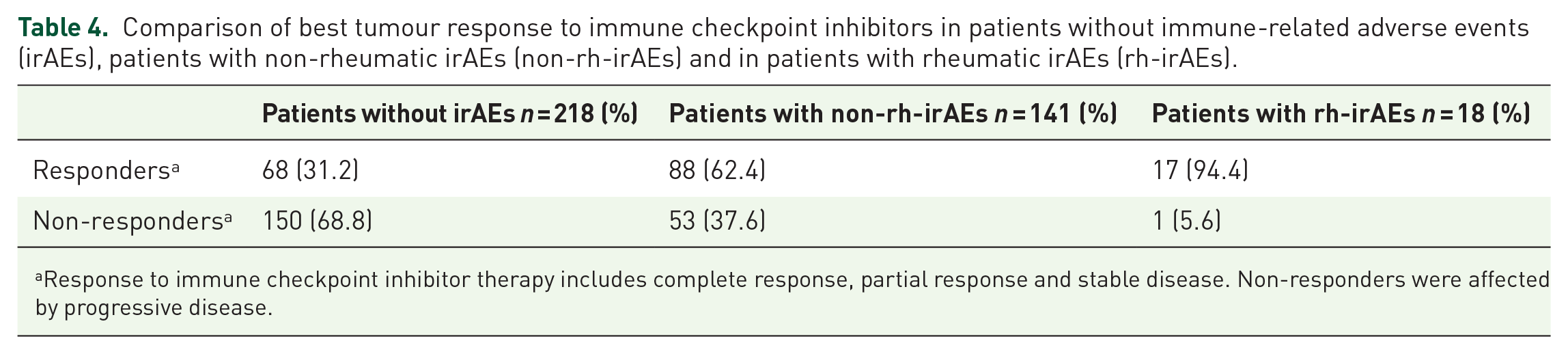
Response to immune checkpoint inhibitor therapy includes complete response, partial response and stable disease. Non-responders were affected by progressive disease.
In order to calculate PFS, we performed a Kaplan–Meier analysis (Figure 1) and compared PFS in three cohorts: patients without irAEs, patients with non-rh-irAEs and patients with rh-irAEs. Patients who suffered from rh-irAEs and non-rh-irAE were classified as rh-irAE cohort. This results in a median PFS of 3 months (range 0–43 months) for all patients with available data included in this calculation. For patients without any irAE the median PFS was 2 months [95% confidence interval (CI) 1.7–2.3]. The non-rh-irAE cohort showed a median PFS of 5 months (95% CI 2.4–7.6) and the rh-irAE cohort displayed a median PFS of 20 months (95% CI 9.1–30.9). The 95% CIs of these cohorts do not overlap and therefore differ considerably. To investigate the distribution of PFS of the three cohorts a Kaplan–Meier graph was constructed (Figure 1). Using the log-rank test, a significant difference in PFS was found in these three cohorts (p < 0.0001).
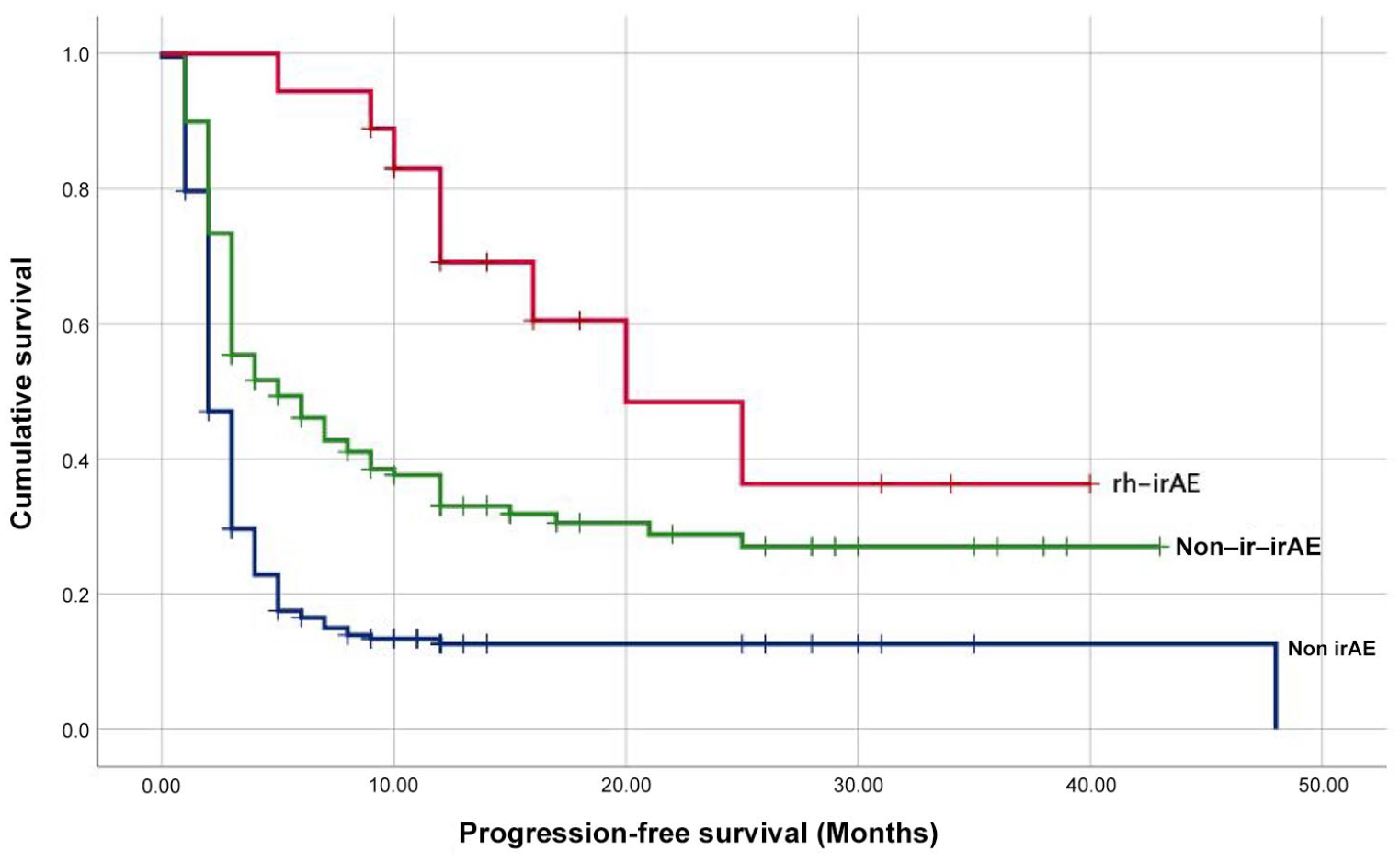
Kaplan–Meier analysis estimated progression-free survival after immune checkpoint inhibitor therapy.
To investigate the impact of rh-irAEs and non-rh-irAEs on PFS in a time-dependent manner and to account for immortal time bias, we conducted a Cox proportional hazards regression model. Please note that this modelling approach also considers the impact of non-rh-irAEs on the PFS in patients of the rh-irAEs cohort. When adjusting for age at baseline, sex and body mass index (BMI) at baseline, the occurrence of non-rh-irAEs showed a reduced hazard ratio (HR) (HR = 0.47, 95% CI 0.36–0.63, p < 0.0001), indicating a significant association with PFS. The occurrence of rh-irAEs also displayed a reduced HR concerning PFS; however, this was not found to be statistically significant (HR = 0.52, 95% CI 0.23–1.20, p = 0.128). PFS was not significantly affected by age (HR = 1.00, 95% CI 0.99–1.01, p = 0.816), sex (female: HR = 1.10, 95% CI 0.84–1.44, p = 0.465) or BMI at baseline (HR = 0.99, 95% CI 0.99–1.00, p = 0.574).
An additional model was adjusted for the different tumour types. Considering the different malignancies, the HR was not significantly affected in the groups clearly defined by tumour type.
We fitted additional models adjusting for the KPS and AJCC staging system for melanoma, as these variables were not available on the whole dataset. For the 178 patients with KPS data, the occurrence of non-rh-irAEs and the KPS at baseline showed a significant association with PFS (non-rh-irAEs: HR = 0.58, 95% CI 0.40–0.84, p = 0.004; KPS: HR = 0.84, 95% CI 0.75–0.95, p = 0.00425; rh-irAEs: HR = 0.47, 95% CI 0.14–1.53, p = 0.212). For the 178 patients with AJCC data in melanoma skin cancer, the occurrence of non-rh-irAEs and AJCC showed a significant association with PFS (non-rh-irAEs: HR = 0.56, 95% CI 0.39–0.81, p = 0.0021; stage III: HR = 0.30, 95% CI 0.17–0.53, p < 0.0001; rh-irAEs: HR = 0.62 95% CI 0.22–1.73, p = 0.3681). Of melanoma patients, 77.5% were identified as stage IV tumour patients. The remaining patients with melanoma were listed as stage III.
In 12 out of 15 patients (80%) who were treated with GC, PFS persisted after GC administration. Three patients who received GC were found to have disease progression at the next staging after starting GC therapy. One in six patients (16.7%) with a medium GC dose experienced progression after GC administration, as did two in five patients (40%) with high GC doses. In the two patients with steroid pulse therapy, PFS remained after GC therapy.
Discussion
The aim of this study was to determine the prevalence of rh-irAEs under ICI therapy. Due to widespread use of ICIs in many malignant diseases, the burden of irAEs as well as rh-irAEs has increased. A detailed description and investigation of rh-irAEs is therefore essential.
In our study, 4.3% of all patients with ICI therapy suffered from at least one rh-irAE. In the four publications available, the prevalence of rh-irAEs varied between 2.3% 26 and 6.6%. 17 This difference might be explained by different study designs: in the retrospective study by Le Burel et al., 26 21 of 908 patients (2.3%) were affected by rh-irAEs. Patients were selected via a French register (REISAMIC), which contains only rh-irAEs of CTCAE grade ⩾2. Applied to our study, this results in an adjusted prevalence of rh-irAEs of 3.9%. Kostine et al. 17 published a rather high prevalence of 35 rh-irAEs patients in 524 patients (6.6%) investigated in their prospective study, including all CTCAE grades. All patients were actively asked about symptoms such as arthralgia, which is a common complaint in general and might explain the higher prevalence published. In the other studies available, rh-irAEs occurred in 3% 27 and in 3.5%. 28 These results are comparable to ours.
Concerning the occurrence of new antibodies, in our cohort in only three out of 19 rh-irAE patients new antibodies were detected. Our results are in line with previous published studies.17,18,29
The most common previously reported rh-irAE is arthralgia, which occurs in 1%–43% of patients. 10 In our study, a total of 15 out of 437 (3.4%) patients complained of arthralgia. A much higher result was published in a study by Buder-Bakhaya et al., 30 where arthralgia was described in 13.3%. Authors in this study included also osteoarthritis as rh-irAE, which is a degenerative disease and, rather, not ICI related. In addition, 17 of the 26 patients complained of arthralgia of CTCAE grade 1 and only nine patients of CTCAE grade 2. Especially these mild and common symptoms are in our opinion difficult to classify in the context of rh-irAEs.
Rather rare previously described rh-irAEs such as PMR, 26 vasculitis,31,32 sarcoidosis,26,28,31 Sjögren’s syndrome 26 and systemic lupus erythematosus 31 did not occur in our cohort. This raises the question of whether these diseases are rh-irAEs or occurred by chance under ICI therapy. Le Burel et al. 26 investigated 908 patients: PMR and sarcoidosis occurred in two patients each. Three patients were affected by Sjögren’s syndrome. Considering that the number of patients examined was about twice as large as in our study, it is not surprising that these rare diseases did not occur in our study. Vasculitis was also observed very rarely (in 0.27% with anti-PD-1/anti-PD-L1 monotherapy and in 0.22% with anti-CTLA-4 monotherapy). 32 Systemic lupus erythematosus was reported in only one patient out of 524 patients (0.2%) receiving ipilimumab therapy. 31 In order to investigate the correlation between the described diseases and ICI therapy, a much larger patient population would be necessary.
Roberts et al. 33 examined 117 patients with rh-irAEs in a nationwide multi-centre cohort study. Although these data cannot be used to make conclusions about the prevalence of rh-irAEs, the large number of patients allows a good representation of the different rh-irAE types. In contrast to our data, the most common rh-irAEs in this study were symmetric polyarthritis (n = 45, 33.1%) and PMR-like syndrome (n = 17, 12.5%). In comparison, arthralgia and myalgia occurred in only 15 patients (11%). In our study, 10 patients (52.6%) complained of arthralgia and myalgia and no patient presented with PMR-like syndromes. This distinction could be interpreted by different reporting behaviour of the centres, or different evaluations of arthralgia as rh-irAE.
Some studies reported a general increase of irAEs 14 as well as rh-irAEs34,35 under ICI combination therapy with ipilimumab and nivolumab. We did not observe rh-irAEs under a combination first-line ICI therapy. However, in second-line ICI combination therapy the occurrence of rh-irAEs was 19%. This significant difference between first- and second-line ICI combination therapy raises the question of whether ICI combination therapy leads to an increase of rh-irAEs or whether this increase is related to second-line therapy. We also found rh-irAEs to occur more frequent under therapy with PD-1-inhibitors nivolumab (5.3%) or pembrolizumab (5.7%) compared with therapy with CTLA-4-inhibitor ipilimumab (2.6%). Kostine et al. 17 came to a similar observation in their prospective study, where all except one patient with rh-irAEs received anti-PD-1 or anti-PD-L1 treatment. This difference could result from the varying impact mechanism of PD-1 and CTLA-4 antibodies.36,37 In addition, a different spectrum of irAEs regarding anti-CTLA-4 versus anti-PD-1/anti-PD-L1 therapy has been reported. 9 Thereby, arthralgia and myalgia occur more frequently under anti-PD-1/anti PD-L1 therapy compared with anti-CTLA-4 therapy and consequently support our observation.
In therapy of rh-irAEs the cooperation between the treating oncologist and rheumatologist is of particular importance. The severity, classified by CTCAE grades, drives the therapy decision. 38 Patients with mild symptoms received non-steroidal anti-inflammatory drugs. If more severe symptoms occurred, GCs were administered. In our study, every patient with rh-irAE ⩾CTCAE grade 3 received GC and three patients required additional therapy with MTX. In some case reports, successful treatment of arthritis with tocilizumab was reported. 39 In our cohort only one patient with arthritis received tocilizumab and responded only partially to the treatment, indicating that Il-6 receptor inhibition might not work in every patient. In addition, EULAR recommendations on the diagnosis and therapy of rh-irAEs were published by Kostine et al. 40 in April 2020. Thereby, three treatment escalations were defined: (1) local/systemic glucocorticoids if symptoms are not controlled by symptomatic treatment, then tapered to the lowest efficient dose, (2) conventional synthetic disease-modifying antirheumatic drugs, in the case of inadequate response to glucocorticoids or for steroid sparing and (3) biological disease-modifying antirheumatic drugs, for severe or refractory irAEs. 40 In general, a similar procedure was followed for our patients. We achieved a good outcome with this therapy procedure in our patients with rh-irAEs, so that our study confirms the recommendations.
Another interesting aspect is whether GC therapy affects tumour response and PFS. In our study, PFS persisted in the majority of patients (80%) even after GC administration was initiated. Therefore, we hypothesize that the use of GC to control rh-irAEs is often associated with no negative PFS-related impact. This hypothesis is supported by Petrelli et al., 41 where the use of GC (to treat irAEs) does not appear to reduce overall survival in cancer patients treated with ICIs. Furthermore, our data suggest that there is no clear correlation between a high steroid dose and the occurrence of progression. This is because progression was indeed observed more frequently in patients with high GC doses than in patients with medium GC doses. Nevertheless, the two patients with steroid pulse therapy were among the majority of patients where PFS persisted. This observation demonstrates the importance of the adequate treatment of rh-irAEs.
Six of 18 patients (33.3%) with rh-irAE and available full data set discontinued ICI therapy as a consequence of rh-irAE. In the study by Richter et al. 27 ICI therapy was terminated in 13 of 61 patients with rh-irAE (21.3%). In general, the decision to discontinue ICI therapy prematurely depends on the severity. 38 In our study ICI therapy was discontinued in four rh-irAE patients with CTCAE grade 3 and two with CTCAE grade 2. In addition to the severity of rh-irAE, the response to therapy and other reasons, including personal reasons, always play a role in the decision to discontinue ICI therapy. Especially in myositis patients, the decision to discontinue ICI therapy should consider that continuation of ICI therapy could lead to potentially life-threatening myositis. 40 As a result, ICI therapy was also discontinued in two of our three patients with myositis as rh-irAE.
The remarkable aspect of this study was the investigation of rh-irAEs and irAEs in general. Rh-irAEs occurred less frequently compared with other irAEs (9.3% of all irAEs were rheumatic). In our study, no significant difference in the occurrence of non-rh-irAEs in patients with or without rh-irAEs was observed. Based on our results, we have established that various side effects occur independently of each other. In a publication by Cappelli et al. 35 the authors observed in 68.7% of patients with immune-related inflammatory arthritis the occurrence of another irAE. In that study, only patients with inflammatory arthritis due to ICI therapy were examined, so that no information about the overall occurrence of irAEs and no general data about all rh-irAEs are available. The study by Kostine et al. 17 is the only study available investigating the prevalence of rh-irAEs as well as non-rh-irAEs in all patients. Of the 35 patients with rh-irAEs, 16 patients (45.7%) were also affected by a non-rh-irAE. Our study yielded very similar results as we observed non-rh-irAEs in 47.4% of patients with rh-irAE. Despite a possible similar autoimmune pathogenesis, non-rh-irAEs were observed in only about half of patients with rh-irAEs.
Median onset of rh-irAEs in our cohort was 109 days, which is comparable to previous studies, where 70 days 17 to 100 days 30 were observed. However, in some patients, symptoms occurred months later, possibly partially due to diagnostic delay. Based on our results, it can be confirmed that rh-irAEs seem to have a later onset than non-rh-irAEs (median onset time of rh-irAEs: 109 days versus non-rh-irAEs 60 days). This result confirms the observation of Smith and Bass. 42
In most other studies on irAEs, patients with pre-existing rheumatic diseases were excluded.18,30 We decided deliberately to include all patients with pre-existing rheumatic diseases, as the aim of this study is to show a realistic prevalence also on the number of flares of a pre-existing rheumatic disease. In a study by Menzies et al., 43 52 patients with pre-existing autoimmune diseases were included, 27 of whom suffered from a rheumatological pre-existing condition. The authors concluded that, although irAEs occur frequently in these predisposed patients, they are usually mild and easy to manage and do not require discontinuation of therapy. Our results show that one-third (27.3%) of patients with pre-existing rheumatic disease experienced a disease flare, but in none of them did ICI therapy have to be terminated. It is important to notice that no new rheumatological diseases occurred in these patients. This result confirms the statement of Menzies et al., 43 that patients with pre-existing rheumatic diseases should not be deprived of ICI therapy. The observation that patients with pre-existing rheumatic diseases tend to have mild and reversible rh-irAEs is also supported by Sebastiani et al. 44 However, it is of great importance to pay attention to these patients in order to diagnose a disease flare in time. Differentiation of an ICI mediated flare of disease and a flare which would have occurred without ICI therapy remains a bias which can hardly be eliminated.
In our study, rh-irAEs occurred considerably earlier in patients with pre-existing rheumatic disease than in patients with de novo disease (median: 30 days versus 109 days). This observation confirms the thesis published in 2019 by Mooradian et al., 45 where the median time to the occurrence of de novo toxicity was 38 weeks and 4.6 weeks in patients with pre-existing rheumatic disease.
The role of rh-irAEs as predictor for response to ICIs is of particular interest. A correlation between irAEs (including rh-irAEs) and tumour response (CR, PR and SD) was observed in various studies.17,46,47 In our cohort, this association was also found; 17 of all 18 patients (94.4%) with rh-irAEs and available full data to therapy response responded strongly to ICI therapy. Moreover, patients with rh-irAEs had a higher rate of responders to ICIs compared with the non-rh-irAEs cohort. This result is different from the study published by Kostine et al., 17 where the authors did not find a difference between patients with rh-irAEs and with non-rh-irAEs concerning response to ICI therapy.
In the study by Buder-Bakhaya et al. 30 a significantly improved PFS in patients with arthralgia was reported. Our study comes to a similar conclusion, as a significant difference was observed between patients without irAEs, patients with non-rh-irAEs and patients with rh-irAEs. In the above-mentioned study 30 the number of patients was less than half of our study (195 patients versus 437 patients in our study). Furthermore, our study includes PFS of patients with all rh-irAE (not only patients with arthralgia) and patients with non-rh-irAE were also examined. Using the Kaplan–Meier analysis, our study showed significantly longer median PFS, especially in patients with rh-irAE than in patients without irAE or in patients with non-rh-irAE. In addition, we observed a strong association between the occurrence of non-rh-irAEs and a reduced risk of progression in the Cox proportional hazards regression model with time-dependent covariates. No significant reduction was observed concerning rh-irAEs. This might be due to the rather low number of rh-irAE patients compared with the non-rh-irAE cohort. Even though approximately 50% of patients with rh-irAEs were also affected by non-rh-irAEs, the effect on PFS reduction cannot be estimated precisely.
Conclusion
Rh-irAEs occur under ICIs and with the increasing use, related side effects will also become more frequent. We observed a prevalence of rh-irAEs of 4.3%. Most commonly observed was arthralgia, followed by arthritis, myositis and myalgia in line with current literature. Therapy of rh-irAEs requires close cooperation between the treating oncologist and rheumatologist. Best therapy for each patient has to be found in an interdisciplinary way according to CTCAE grade. ICI therapy termination has to be decided individually. The observed significantly improved tumour response in patients with rh-irAE (94.4% of patients with rh-irAE were responders to ICI therapy) should be kept in mind, considering termination of ICI therapy. Further prospective studies are necessary to define rh-irAEs more precisely and to derive treatment algorithms.
Supplemental Material
sj-docx-1-tab-10.1177_1759720X211006963 – Supplemental material for Prevalence, therapy and tumour response in patients with rheumatic immune-related adverse events following immune checkpoint inhibitor therapy: a single-centre analysis
Supplemental material, sj-docx-1-tab-10.1177_1759720X211006963 for Prevalence, therapy and tumour response in patients with rheumatic immune-related adverse events following immune checkpoint inhibitor therapy: a single-centre analysis by Sophia H. Verspohl, Tobias Holderried, Charlotte Behning, Peter Brossart and Valentin S. Schäfer in Therapeutic Advances in Musculoskeletal Disease
Supplemental Material
sj-docx-2-tab-10.1177_1759720X211006963 – Supplemental material for Prevalence, therapy and tumour response in patients with rheumatic immune-related adverse events following immune checkpoint inhibitor therapy: a single-centre analysis
Supplemental material, sj-docx-2-tab-10.1177_1759720X211006963 for Prevalence, therapy and tumour response in patients with rheumatic immune-related adverse events following immune checkpoint inhibitor therapy: a single-centre analysis by Sophia H. Verspohl, Tobias Holderried, Charlotte Behning, Peter Brossart and Valentin S. Schäfer in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.