
Abstract
Background:
To investigate factors associated with flare in patients with ankylosing spondylitis (AS) who tapered tumour necrosis factor inhibitors (TNFis) after achievement of low disease activity (LDA) with the standard dose of TNFis.
Methods:
This retrospective cohort study included 101 patients with AS who tapered their first TNFis after achievement of LDA. The proportion of reduced versus standard doses of TNFi throughout the follow up in each patient was quantified using the time-averaged dose quotient (DQ). Clinical characteristics were compared between patients who did and did not experience flare after TNFi tapering. Multivariable Cox regression analysis was performed to identify factors associated with flare. Receiver operating characteristic curve analysis was performed to determine the cut-offs of these covariates that best predicted flare.
Results:
Of the total 101 patients, 45 (44.6%) patients experienced flare after TNFi tapering. Compared with patients who did not experience flare, those who experienced flare had a shorter disease duration (p = 0.006), shorter LDA duration before TNFi tapering (p < 0.001) and lower time-averaged DQ (p < 0.001). In multivariable Cox regression analysis, the LDA duration [adjusted hazard ratio (HR): 0.944, 95% confidence interval (CI): 0.906–0.983, p = 0.006] and time-averaged DQ (adjusted HR: 0.978, 95% CI: 0.959–0.998, p = 0.032) were inversely associated with flare. The cut-off values of the LDA duration and time-averaged DQ that best predicted flares were <5.3 months and <60.6%, respectively.
Conclusion:
Shorter LDA duration (cut-off value: 5.3 months) and lower time-averaged DQ (cut-off value: 60.6%) were associated with a higher risk of flare after tapering TNFi.
Introduction
Ankylosing spondylitis (AS) is a chronic inflammatory disorder characterised by inflammatory back pain, sacroiliitis, spinal inflammation and bony ankylosis, which leads to reduced spinal mobility and functional limitations.1,2 For the treatment of active AS, non-steroidal anti-inflammatory drugs (NSAIDs) are used as a first-line treatment, and for patients with active AS despite treatment with NSAIDs, tumour necrosis factor inhibitors (TNFis) are used as a second-line treatment.3,4
Although the introduction of TNFi has markedly improved the treatment of AS,5–9 their long-term use imposes a substantial economic burden on patients and possess a risk of infection.10,11 Given these concerns, several studies have compared the reduced dose (i.e. tapering) and standard dose of TNFi in patients with low disease activity (LDA) and have reported that both have similar effects on disease control.12–15 Based on these data, the Assessment of SpondyloArthritis international Society–European League Against Rheumatism (ASAS–EULAR) recommended that tapering of TNFi can be considered in patients with sustained remission. 3 However, other observational studies that focussed on complete discontinuation of TNFi, reported that 60–74% of patients relapse after TNFi discontinuation.16–18 Accordingly, the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network (ACR/SAA/SPARTAN) conditionally recommended against discontinuation of TNFi in patients with stable AS. 4 Moreover, the ACR/SAA/SPARTAN conditionally recommended against tapering TNFi as a standard approach because of the limited evidence in maintaining long-term remission after tapering TNFi. 4
Given that tapering TNFi in patients with inactive AS is controversial, tapering TNFi injudiciously in patients with inactive AS may not be desirable. Rather, careful selection of patients who could benefit from tapering TNFi without having a flare and implementation of TNFi tapering in these selected patients would be a better approach. Currently, limited data are available on predictors of flare after tapering TNFi; therefore, it is unclear which patients are appropriate to be selected for the implementation of TNFi tapering and what extent of dose reduction is appropriate. The aim of this study was to investigate factors associated with the risk of flare after TNFi tapering.
Methods
Study population
Patients with AS who received TNFi between January 2010 and December 2018 at a tertiary referral hospital in Seoul, South Korea were reviewed retrospectively for inclusion in this study. All patients included in the study fulfilled the following inclusion criteria: (a) the radiological criterion of the 1984 modified New York criteria (sacroiliitis grade ⩾2 bilaterally or grade ⩾3 unilaterally) 19 ; (b) tapering of the first TNFi after achievement of LDA; and (c) followed up for at least 6 months after initiation of TNFi tapering. Exclusion criteria were: (a) received a standard dose of TNFi throughout the observational period; (b) prior use of other TNFis (i.e. tapering of TNFi not implemented for the first TNFi); and (c) discontinued TNFi for other reasons.
After diagnosis of AS, all patients were started on NSAIDs with or without conventional synthetic disease-modifying anti-rheumatic drugs (csDMARDs). For patients with active AS despite treatment with NSAIDs (with or without csDMARDs) for at least 3 months, standard dose of TNFi was started. After achievement of LDA, the TNFi was tapered by gradual prolongation of dosing interval and/or by dose reduction. The decision of when and how to taper TNFi was at the discretion of the treating physicians.
At the time of TNFi tapering initiation (referred to as the baseline), the following data were reviewed: age, age at symptom onset, sex, disease duration, body mass index (BMI), smoking history (current smoker: yes or no), HLA-B27 positivity, presence of syndesmophyte, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), time from the start of TNFi to the achievement of LDA, duration of LDA at the initiation of TNFi tapering, concomitant use of NSAIDs and csDMARDs, and type of TNFi used. Concomitant uses of NSAIDs and csDMARDs at the time of flare or end of follow up were also reviewed.
This study was approved by the Institutional Review Board (IRB) of Gangnam Severance Hospital (IRB No: 3-2018-0283). Owing to the retrospective nature of this study, the requirement for informed consent was waived.
Definition of LDA and disease flare
LDA was defined as BASDAI < 4, 15 and disease flare was defined as BASDAI ⩾ 4 and a ΔBASDAI ⩾ 2 compared with baseline BASDAI. 15 Electronic medical records of each patient were reviewed from baseline to the last follow-up date to determine whether flare occurred during this time period.
Quantification of TNFi tapering
As used in previous studies, we used the term ‘dose quotient’ (DQ) to quantify the reduced dose of TNFi.14,20 The DQ was calculated as (actual dose/standard dose) × (standard dosing interval/actual dosing interval) × 100. As the dose and interval of TNFi administration were tailored according to the discretion of the treating physicians, the DQ was not constant and varied throughout the disease course. Therefore, instead of using DQ at a single time point, we used time-averaged DQ for analysis. Time-averaged DQ was calculated as [sum of (particular DQ × administration duration of that particular DQ)]/total duration of observation time. The total duration of observation time for calculating time-averaged DQ was from the baseline to either the last follow up or occurrence of flare, whichever came first. For example, if a patient observed for 5 months had received a DQ of 50% for 3 months followed by DQ of 25% for 2 months, the time-averaged DQ was [(50 × 3) + (25 × 2)]/(3 + 2) = 40%.
Statistical analysis
Continuous variables were expressed as the mean ± standard deviation and median [interquartile range (IQR)] for a normal and a non-normal distribution, respectively. The normality of continuous variables was evaluated using the Kolmogorov–Smirnov test. Categorical variables were expressed as number (%). For comparison between two groups, Student’s t test or Mann–Whitney U test was performed for continuous variables, and χ2 test (or Fisher’s exact test when the frequency of any cell was <5) was used to compare categorical variables. Factors associated with flare were evaluated by Cox proportional hazard regression analysis. The proportional hazards assumption for each independent variable was confirmed by testing Schoenfeld partial residuals. Factors with a p value of <0.15 in univariable analysis were included in multivariable analysis. The variation inflation factor (VIF) was assessed to exclude multicollinearity among covariates included in the multivariable analysis. VIFs of all covariates were <5, confirming the absence of multicollinearity. For the factors identified as statistically significant in the multivariable Cox regression analysis, receiver operating characteristic (ROC) curve analysis was used to determine the cut-offs that best predicted flare (i.e. points that yielded the maximum Youden index). Potential confounding by indication was adjusted by propensity score matching. A p value of <0.05 was considered statistically significant. All analyses were performed using SPSS software (version 25.0; IBM Corporation, Armonk. NY, USA), and figures were generated using GraphPad Prism (version 7.0; GraphPad Software, San Diego, CA, USA).
Results
Baseline characteristics of the patients
A total of 321 patients with AS who received TNFi between January 2010 and December 2018 were screened. Of these 321 patients, 71 who had prior exposure to another TNFi before 2010, 46 who failed to achieve LDA with the use of first TNFi, 15 who were followed up for less than 6 months after initiation of TNFi tapering, 81 who received standard dose of TNFi throughout the observational period, and 7 who discontinued TNFi for other reasons (cost issue, 1 patient; side effects, 4 patients; pregnancy, 1 patient; and occurrence of cancer, 1 patient) were excluded. The remaining 101 patients with AS who initiated TNFi tapering after achievement of LDA with the standard dose of TNFi were included. The median follow-up duration from baseline to the last follow-up date was 50.6 (28.3–89.7) months. Clinical characteristics of the patients at the initiation of TNFi tapering are summarised in Table 1. The median age of the patients was 35.0 (26.0–48.0) years and the majority of the patients were male (84.2%). The values of ESR, CRP and BASDAI were 5.0 (2.0–11.0) mm/h, 0.6 (0.3–1.2) mg/l and 2.2 ± 0.5, respectively. TNFi tapering was initiated after a LDA duration of median 8.9 (3.3–16.8) months.
Baseline characteristics of the patients at the time of initiation of TNFi tapering.

Patients (n = 3) with missing data excluded.
Patients (n = 8) with missing data excluded.
At baseline.
At flare or end of follow-up.
BASDAI, Bath ankylosing spondylitis disease activity index; BMI, body mass index; CRP, C-reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; IQR, interquartile range; LDA, low disease activity; NSAIDs, non-steroidal anti-inflammatory drugs; TNFi, tumour necrosis factor inhibitor.
Comparison between patients who did and did not experience flare
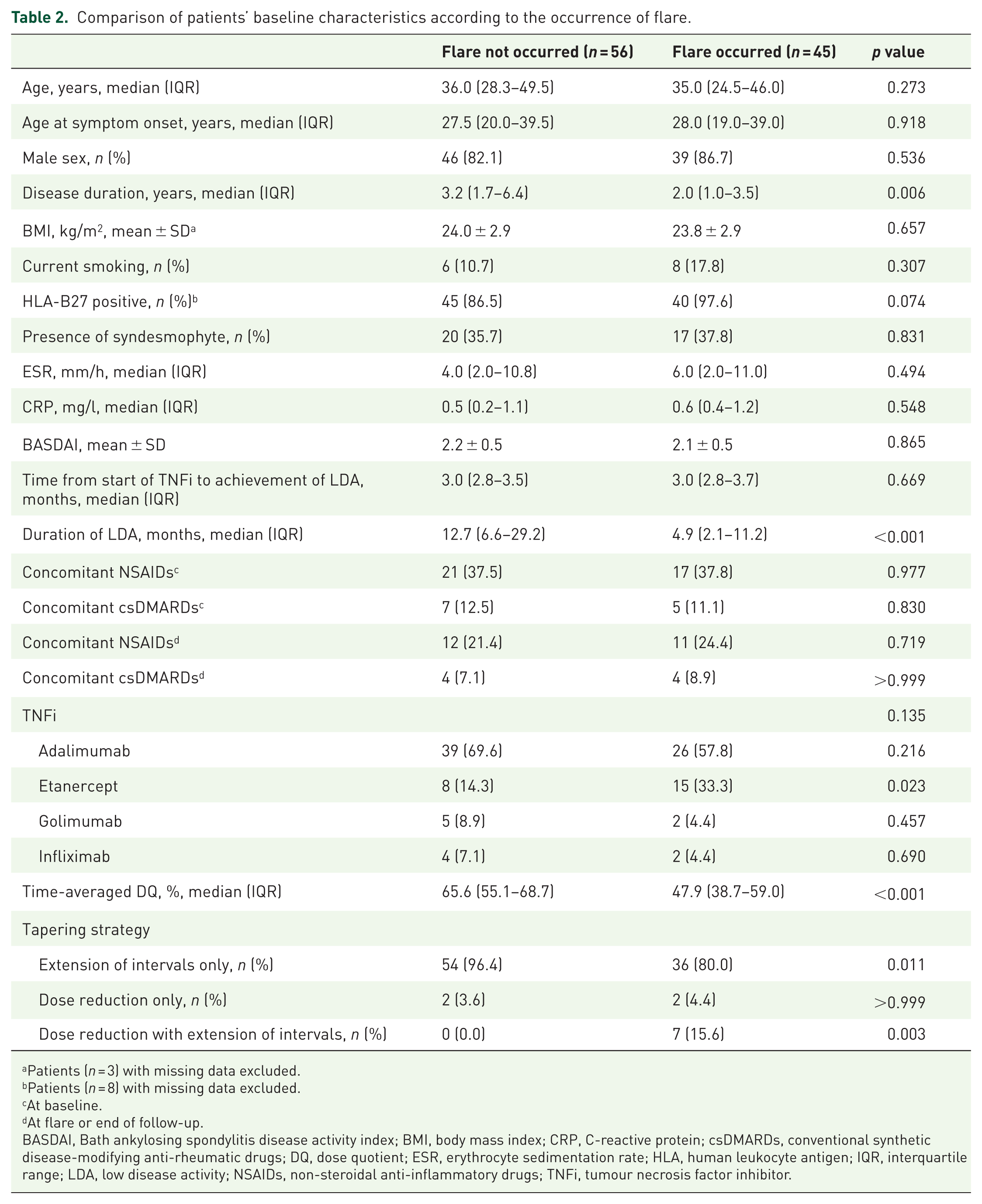
After the tapering of TNFi, flare occurred in 45 (44.6%) patients at a median of 29.4 (16.1–48.0) months. For the 45 patients who experienced flare, the mean value of BASDAI at occurrence of flare was 6.9 ± 1.2. A total of 41 (91.1%) patients improved after increasing the TNFi to standard dose, whereas the other 4 (8.9%) patients did not improve after increasing the TNFi to standard dose and were switched to another TNFi or secukinumab. Compared with patients who did not experience flare, patients who experienced flare had a shorter disease duration [3.2 (1.7–6.4) years versus 2.0 (1.0–3.5) years, p = 0.006] and shorter duration of LDA [12.7 (6.6–29.2) months versus 4.9 (2.1–11.2) months, p < 0.001] at baseline, and a lower time-averaged DQ [65.6 (55.1–68.7) % versus 47.9 (38.7–59.0) %, p < 0.001] throughout follow up. In terms of tapering strategy, extension of intervals only was the more common tapering strategy in patients who did not experience flare (96.4% versus 80.0%, p = 0.011), whereas dose reduction with extension of intervals was the more common tapering strategy in patients who experienced flare (0.0% versus 15.6%, p = 0.003) (Table 2).
Comparison of patients’ baseline characteristics according to the occurrence of flare.
Patients (n = 3) with missing data excluded.
Patients (n = 8) with missing data excluded.
At baseline.
At flare or end of follow-up.
BASDAI, Bath ankylosing spondylitis disease activity index; BMI, body mass index; CRP, C-reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; DQ, dose quotient; ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; IQR, interquartile range; LDA, low disease activity; NSAIDs, non-steroidal anti-inflammatory drugs; TNFi, tumour necrosis factor inhibitor.
Factors associated with flare
In the univariable Cox regression analysis, disease duration [unadjusted hazard ratio (HR): 0.922, 95% confidence interval (CI): 0.832–1.022, p = 0.123], CRP level (unadjusted HR: 1.244, 95% CI: 0.946–1.637, p = 0.118), BASDAI (unadjusted HR: 1.644, 95% CI: 0.901–2.998, p = 0.105), duration of LDA (unadjusted HR: 0.941, 95% CI: 0.908–0.975, p = 0.001), time-averaged DQ (unadjusted HR: 0.971, 95% CI: 0.953–0.988, p = 0.001) and tapering strategy using dose reduction with extension of intervals (versus tapering strategy using extension of intervals only, unadjusted HR: 2.344, 95% CI: 1.036–5.302, p = 0.041) had a p value of <0.15. These variables were incorporated in the multivariable analysis: longer duration of LDA (adjusted HR: 0.944, 95% CI: 0.906–0.983, p = 0.006) and higher time-averaged DQ (adjusted HR: 0.978, 95% CI: 0.959–0.998, p = 0.032) were significantly associated with a lower risk of flares (Table 3).
Factors associated with flare after TNFi tapering.

Covariates with a p value of <0.15 in the univariable analysis were incorporated in the multivariable analysis.
At baseline.
At flare or end of follow-up.
BASDAI, Bath ankylosing spondylitis disease activity index; BMI, body mass index; CRP, C-reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; DQ, dose quotient. ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; HR, hazard ratio; LDA, low disease activity; NSAIDs, non-steroidal anti-inflammatory drugs; TNFi, tumour necrosis factor inhibitor.
Cut-off values of duration of LDA and time-averaged DQ that best predict flare
To determine the cut-off values of duration of LDA and time-averaged DQ that best predicted the occurrence of flare, ROC analysis was performed (Figure 1). A duration of LDA < 5.3 months [area under the curve (AUC): 0.745, 95% CI: 0.651–0.840] and a time-averaged DQ < 60.6% (AUC: 0.761, 95% CI: 0.665–0.856) best predicted the occurrence of flare.

ROC curve analysis of (A) duration of LDA, and (B) time-averaged DQ in predicting disease flare.
Propensity score-matched analysis
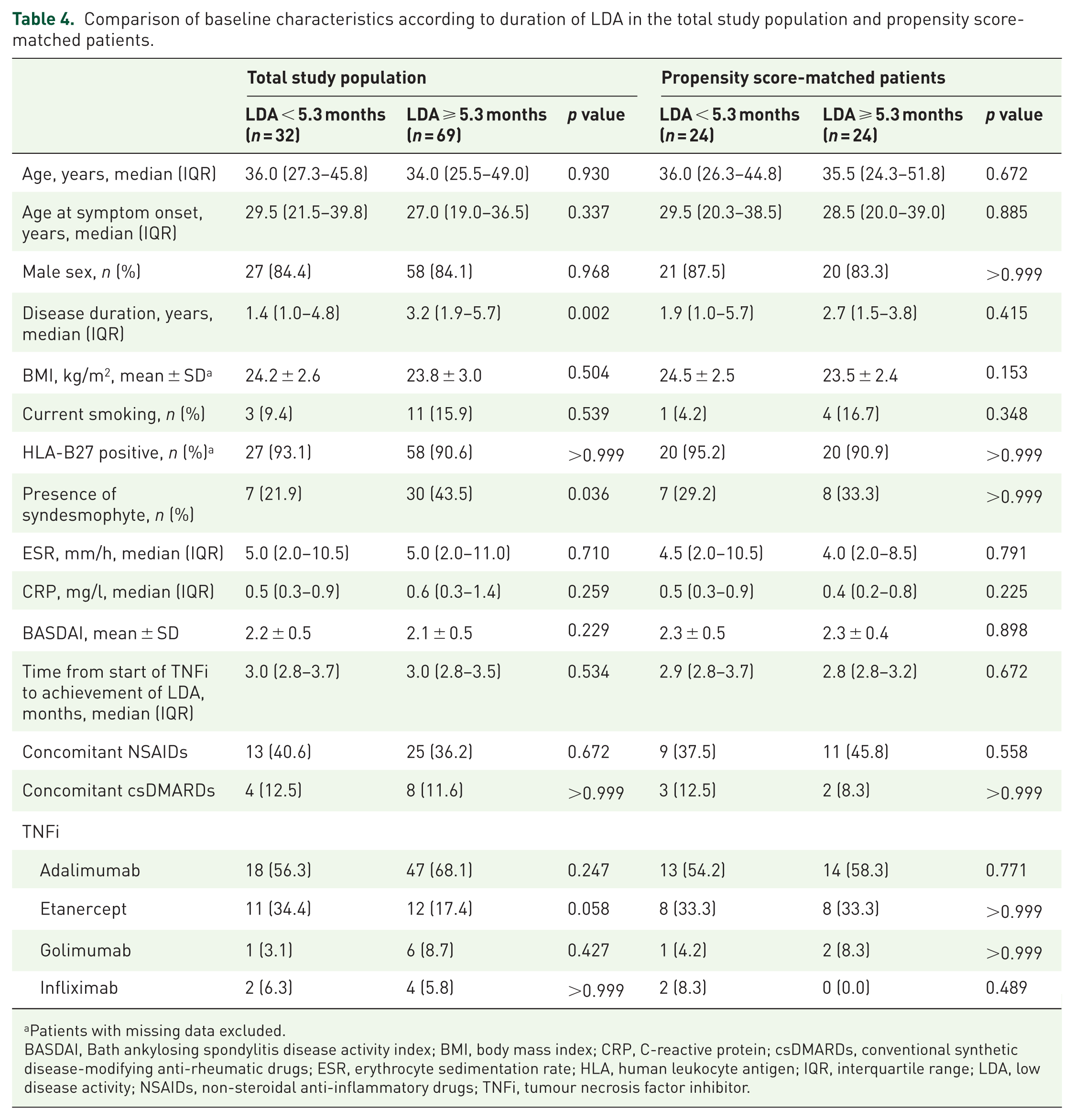
Because patients were not randomly assigned for when (duration of LDA) and how (time-averaged DQ) to taper TNFi, we performed propensity score-matched analysis to adjust for confounding by indication. The propensity score for initiating TNFi tapering at an LDA duration <5.3 months and the propensity score for tapering TNFi at a time-averaged DQ < 60.6% were matched, respectively. Comparisons of the baseline characteristics according to the duration of LDA (<5.3 months and ⩾5.3 months) and time-averaged DQ (<60.6% and ⩾60.6%) in the propensity score-matched patients are shown in Tables 4 and 5, respectively. As opposed to the total study population, these propensity score-matched patients were well matched; no significant difference in the baseline characteristics was observed. In these propensity score-matched patients, duration of LDA < 5.3 months (HR: 2.596, 95% CI: 1.027–6.567, p = 0.044) and time-averaged DQ < 60.6% (HR: 7.563, 95% CI: 2.177–26.274, p = 0.001) were significantly associated with a higher risk of flare.
Comparison of baseline characteristics according to duration of LDA in the total study population and propensity score-matched patients.
Patients with missing data excluded.
BASDAI, Bath ankylosing spondylitis disease activity index; BMI, body mass index; CRP, C-reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; IQR, interquartile range; LDA, low disease activity; NSAIDs, non-steroidal anti-inflammatory drugs; TNFi, tumour necrosis factor inhibitor.
Comparison of baseline characteristics according to time-averaged DQ in the total study population and propensity score-matched patients.

Patients with missing data excluded.
BASDAI, Bath ankylosing spondylitis disease activity index; BMI, body mass index; CRP, C-reactive protein; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; DQ, dose quotient; ESR, erythrocyte sedimentation rate; HLA, human leukocyte antigen; IQR, interquartile range; LDA, low disease activity; NSAIDs, non-steroidal anti-inflammatory drugs; TNFi, tumour necrosis factor inhibitor.
Discussion
In this study, we found that a shorter duration of LDA at the initiation of TNFi tapering and a lower time-averaged DQ throughout the disease course were associated with a higher risk of flare in patients with AS whose TNFi dose was tapered after achievement of LDA. In particular, a duration of LDA shorter than 5.3 months and a time-averaged DQ less than 60.6% best predicted a flare.
The optimal duration of sustained LDA in which initiation of TNFi tapering could be considered is currently uncertain. Despite the lack of evidence, the recommendations from ASAS–EULAR suggested that the duration of sustained inactive disease should be at least 6 months. 3 In our data, we showed that a duration of LDA < 5.3 months best predicted the occurrence of flares. In addition, the risk of flares decreased by 5.5% per 1-month increase in the duration of LDA (adjusted HR: 0.945). These data suggest that TNFi tapering could be considered if LDA is maintained for at least 5.3 months, with longer durations of sustained LDA being better.
The extent of reduction in TNFi dose was also associated with an increased risk of flares (time-averaged DQ, adjusted HR: 0.977). Similar to our present finding, a previous study reported that heavy-tapering of TNFi, but not mild-tapering of TNFi, decreased the likelihood of maintaining an inactive disease, compared with the standard dose of TNFi. 20 In that study, the cut-off value for classifying mild-tapering and heavy-tapering groups were arbitrarily chosen (mild tapering: DQ < 50 and heavy tapering: DQ = 50–99). 20 Our findings add to the previous report by analysing time-averaged DQ as a continuous variable, rather than as a categorical variable, and by providing the cut-off value that best predict a flare. The cut-off value of time-averaged DQ was 60.6%, suggesting that clinicians should be cautious when considering tapering the dose of TNFi below 60.6% of the standard dose.
One could argue that tapering of TNFi should be implemented only in patients with ‘deep’ sustained remission, to minimise the risk of flares. In our study population, ESR, CRP and BASDAI, which are the indicators of disease activity, were 5.0 (2.0–11.0) mm/h, 0.6 (0.3–1.2) mg/l and 2.2 ± 0.5, respectively, at the initiation of TNFi tapering. Within these ranges, ESR, CRP and BASDAI were not associated with flare after TNFi tapering. Considering the normal range of ESR (0–15 mm/h for male and 0–20 mm/h for female) and CRP (0.0–6.0 mg/l), and the cut-off value of BASDAI for LDA (BASDAI < 4), the levels of disease activity indices in our patients were relatively low. Although there are no universally accepted definitions for deep remission and less stringent remissions in patients with AS, the proportion of patients with less stringent remission might have been very low in our study. This may have led to an underestimation of the association between these disease activity indices and the risk of flares. Therefore, it is unclear by our data whether the risk of flares is lower in patients with deep remission than in those with less stringent remission.
Other important clinical questions include whether a particular TNFi is harder or easier to taper than other TNFis, and whether tapering strategy (dose reduction versus extension of intervals) affect the risk of flare. In our data, we found that no particular TNFi was associated with risk of flare (Table 3), and presume that no particular TNFi is harder or easier to taper than other TNFis. However, for a more accurate comparison of feasibility among tapering of different TNFis, head-to-head comparison trials are needed. In regard to tapering strategy, no particular strategy was associated with risk of flare (Table 3), which suggests that, regardless of tapering strategy (whether it is through dose reduction and/or extension of intervals), duration of LDA and time-averaged DQ are the factors associated with risk of flare.
Previous studies have reported predictors of flares after tapering TNFi, with conflicting results.15,18 Plasencia et al. reported that male sex was protective of having a flare, 15 while Zhao et al. suggested older age and younger onset age as factors associated with an increased risk of relapse, 18 both of which are different from our results. This discrepancy is likely due to the difference in inclusion criteria among the studies. We included only the patients with AS who were receiving their first TNFi, whereas Plasencia et al. included patients with non-radiographic spondyloarthritis (SpA), SpA associated with inflammatory bowel disease, psoriatic SpA and patients who had history of prior biologic use. 15 In the study by Zhao et al., patients instantly discontinued their TNFi shortly after achievement of remission, rather than gradually tapering it after sustained LDA or remission. 18 An important clinical implication of our data is that information regarding when and how to taper TNFi in patients with inactive AS has been provided, which had not been previously addressed.
This study has several limitations. First, owing to the retrospective design of the study, the possibility of confounding by unmeasured variables exists. In particular, patient preference, which can affect the treating physicians’ decision on tapering TNFi, is an important variable that cannot be measured retrospectively. However, as the BASDAI is an index determined entirely by patient-reported outcomes, this index might reflect patient preference in tapering TNFi. Considering that baseline BASDAI was well matched in the propensity score-matched patients, we presume that our results are not likely the consequence of confounding by patient preference. Second, we lacked data about patient global assessment of disease activity, which is one of the component of AS disease activity score (ASDAS) formula, in a number of patients, and were unable to use ASDAS as an indicator of disease activity. Third, for homogeneity of the study population, we included only the patients with AS fulfilling the radiological criterion of the 1984 modified New York criteria, 19 and those who were on their first TNFi. Therefore, our results may not be applied to patients with SpA in general, and to those who have previously failed the first TNFi. Fourth, although we found that a shorter duration of LDA and a lower time-averaged DQ were associated with a higher risk of flares, it was difficult to define the single best strategy for tapering TNFi because the TNFi tapering strategy varied widely among patients.
In conclusion, we demonstrated that a shorter duration of LDA, with a cut-off value of 5.3 months at the initiation of TNFi tapering, and a lower time-averaged DQ, with a cut-off value of 60.6%, were associated with a higher risk of flare occurrence. Our data provide clinicians an insight on predictors of flares after tapering TNFi in AS patients with LDA. When considering TNFi tapering after achievement of LDA with the use of standard dose TNFi, these predictors could be taken into account to tailor when and how to taper TNFi.
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from LG Chem, Ltd. (3-2018-0283).
Data availability statement
All data are incorporated into the article.