
Abstract
Interleukin 1 (IL-1), a central mediator of innate immunity, is considered a master cytokine of local and systemic inflammation. IL-1 has emerged as pivotal in the pathogenesis of autoinflammatory diseases (AIDs), and blockade of its pathway has become a crucial target for therapy. Anakinra (ANA), a recombinant IL-1β receptor antagonist, was the first anti-IL-1 agent employed in clinical practice. ANA is currently approved for the treatment of rheumatoid arthritis, systemic juvenile idiopathic arthritis, adult-onset Still’s disease, and cryopyrin-associated autoinflammatory syndrome. It has also been successfully used for off-label treatment of various monogenic, polygenic, or undefined etiology systemic AIDs.
This review describes currently available evidence for the off-label use of ANA in pediatric rheumatologic diseases. Specifically, the use of ANA in Kawasaki disease, idiopathic recurrent pericarditis, Behçet disease, monogenic AIDs, undifferentiated AIDs, chronic non-bacterial osteomyelitis, macrophage activation syndrome, and febrile infection-related epilepsy, in terms of its safety and efficacy. In selected pediatric rheumatic disorders, the off-label administration of ANA appears to be effective and safe. In order to control severe and/or relapsing disease, ANA should be considered as a valuable treatment option in children suffering from rare inflammatory diseases. However, currently available data consist of retrospective studies and short case series; thus, randomized controlled trials and larger series with long-term follow up are mandatory to better assess the efficacy and cost effectiveness of ANA in these challenging patients.
Introduction
The history of the interleukin-1 (IL-1) family of 11 cytokines began with the discovery of the first two members, IL-1α and IL-1β. IL-1 is a central mediator of innate immunity and is considered a master cytokine of local and systemic inflammation. IL-1α and IL-1β are encoded by distinct genes, bind to the same receptor (IL-1R1), and have similar biological properties. IL-1β is transcribed as an inactive precursor that requires the assembly of the NLRP3 inflammasome to activate caspase 1, the enzyme that releases the biologically active form of the cytokine. It mediates inflammation and enhances antigen-driven CD8+ T-cell differentiation, proliferation, memory, and migration into tissues. In contrast, IL-1α is functional and, following release from necrotic cells at the site of injury, can directly bind to the IL-1R1 of neighboring cells, activating a cascade of inflammatory cytokines and chemokines. 1
Since its first observation in 1999 by McDermott et al., IL-1β has assumed a pivotal role in the pathogenesis of autoinflammatory diseases (AIDs). 2 This observation catapulted the IL-1 family into clinical rheumatology research, and IL-1-pathway blocking became a crucial target for therapy. 3
Indeed, the positive effects of anti-IL-1 treatment have been demonstrated in several AIDs. Three anti-IL-1 therapies are currently available: canakinumab (an anti-IL-1β immunoglobulin), rilonacept (a dimeric fusion protein that binds the extracellular domains of IL-1α and IL-1β), and anakinra (ANA) [a recombinant IL-1-receptor antagonist (IL-1RA)]. Canakinumab is approved for the treatment of cryopyrin-associated autoinflammatory syndrome (CAPS), tumor-necrosis-factor-receptor-associated periodic syndrome (TRAPS), hyperimmunoglobulinemia D syndrome/mevalonate kinase deficiency (HIDS/MKD), colchicine-resistant familial mediterranean fever (FMF), systemic juvenile idiopathic arthritis (sJIA), and adult-onset Still’s disease (AOSD). Rilonacept is approved for the therapy of CAPS. ANA, the first licensed anti-IL-1 agent, is currently approved for the treatment of CAPS, rheumatoid arthritis, sJIA, and AOSD. However, it has also been successfully used off-label for the treatment of various monogenic, polygenic, or undefined etiology systemic AIDs. This review reports currently available evidence on the off-label use of ANA in pediatric rheumatology, including its off-label use in Kawasaki disease (KD), idiopathic recurrent pericarditis (IRP), Behçet disease (BD), monogenic AIDs, undifferentiated AIDs (uAIDS), chronic non-bacterial osteomyelitis (CNO), macrophage activation syndrome (MAS), and febrile infection-related epilepsy (FIRES), in terms of its safety and efficacy.
Kawasaki disease
KD is an acute inflammatory vasculitis of the medium and small-sized arteries, generally occurring in children under 5 years of age. It is associated with the development of coronary artery aneurysms (CAAs) or ecstasies (i.e. dilatation of an arterial vessel whose dimensions do not exceed 50% of the caliber of the vessel itself) in 15–25% of untreated children. Cardiac involvement is the main determinant of the long-term prognosis of KD patients, as coronary lesions may lead to ischemic heart disease and sudden death. 4 The etiopathology remains unknown, though it is widely accepted that KD results in an important inflammation cascade triggered by unknown infectious or other stress triggers in a genetically predisposed individual. A single infusion of 2 g/kg of intravenous immunoglobulin (IVIG) along with aspirin has reduced CAA frequency from 25% to 5%. 5 However, 10–20% of patients do not respond to standard treatment and have an increased risk of cardiac complications and death. 6
As in monogenic AIDs, IL-1 seems to play a key role in the physiopathology of KD and, more importantly, in cardiac involvement and the development of CAA leading to the potential use of IL-1 blockade in patients with refractory KD.7–9
Alphonse et al. showed a significantly increased level of IL-1β, IL-18, and of their antagonists (IL-1RA and IL-18BP) in acute KD patients compared with age-matched control patients with viral or bacterial infections. 10 In a microarray study of acute and convalescent whole-blood samples from 146 KD subjects, KD transcript profiles showed an abundance of transcripts related to the NLRP3 inflammasome, IL-1α and β, and caspase-1 compared with pediatric subjects with different acute infectious diseases, and with healthy controls. 11 Early studies determined that IVIG treatment was associated with a reduction in IL-1β secretion from KD patients without CAA versus persistently elevated levels in IVIG-treated patients with CAA. 12 It is well known that IVIG resistance is associated with coronary vasculitis, and IVIG-resistant KD patients have decreased expression of IL-1RA. 13 Genetic studies have also identified that polymorphisms of inositol 1,4,5-trisphosphate 3-kinase C (ITPKC) represent a susceptibility factor for KD and CAA. The ITPKC gene induces increased Ca2+ flux into the cell, NLRP3 inflammasome activation, and increased secretion of IL-1ß and IL-1a. 14
Moreover, in a Lactobacillus casei cell-wall-extract-induced mouse vasculitis model, ANA administration was able to prevent aortic aneurysms and to improve cardiac ejection fraction by controlling myocarditis, suggesting that early use of ANA might better prevent or treat early coronary lesions. 15
Similar successful results were confirmed in the clinical setting of refractory KD as well as in MAS caused by KD responsive to ANA treatment (Table 1).9,16–19
Main studies reporting anakinra administration in Kawasaki disease.

APPs, acute-phase proteins; CAA, coronary artery aneurysm; NA, not available.
Kone-Paut et al. recently published a case series of 11 children with refractory KD and cardiac complications who received ANA. All patients became afebrile and achieved significant decreases of inflammatory markers within a few days after administration of ANA, although the reported results on its effect on coronary dilations are heterogeneous. 20
Considering the upregulation of the IL-1 pathway in KD, ANA may represent a valuable therapeutic tool to control systemic inflammation in KD patients. The convergence of genetic data and results from animal models provide a strong rationale for the hypothesis that IL-1 signaling plays a key role in KD vasculitis and coronary arteritis; in this perspective, ANA may also have a role in preventing the onset of CAA, especially if used at diagnosis.21,22 In this regard, two clinical trials of ANA involving KD pediatric patients are currently underway in western Europe and the United States: the Kawakinra trial [Eudract no: 2014-002715-41]; and the ANAKID trial [ClinicalTrials.gov identifier: NCT02179853], respectively. The outcomes of these studies may better define the place of IL-1 blockade in KD treatment in association with or in replacement of IVIG and steroids.
Idiopathic recurrent pericarditis
Recurrent pericarditis is a relatively common complication (15–30%) of acute pericarditis. In the majority of patients with recurrent pericarditis (70–80%) no specific cause is identified and the disease is referred to as IRP. 23 Established therapeutic regimens, such as non-steroidal anti-inflammatory drugs (NSAIDs), colchicine, and steroids, induce remission in most cases. Nevertheless, a subset of patients either do not respond, relapse, or cannot tolerate the standard therapeutic interventions. 24 In this perspective, IRP shares many features consistent with AIDs. Indeed, recurrent episodes of apparently unprovoked inflammation and serosal involvement are characteristic of AIDs and it is well known that FMF and TRAPS can sometimes present with isolated serosal involvement, especially when the onset is in adulthood.25,26 In line with this hypothesis, Cantarini et al. found that 6% of IRP patients carry a mutation in the tumor necrosis factor (TNF) receptor superfamily member 1A (TNFRSF1A) gene. 27 Hence, biological agents are emerging as potential therapeutic options for the treatment of IRP, with the majority of experiences having been acquired with ANA. Considering the adverse impact of steroids in pediatric patients, treatment with ANA in this patient population was primarily taken into account (Table 2). 28
Main studies reporting anakinra administration in pediatric idiopathic recurrent pericarditis.
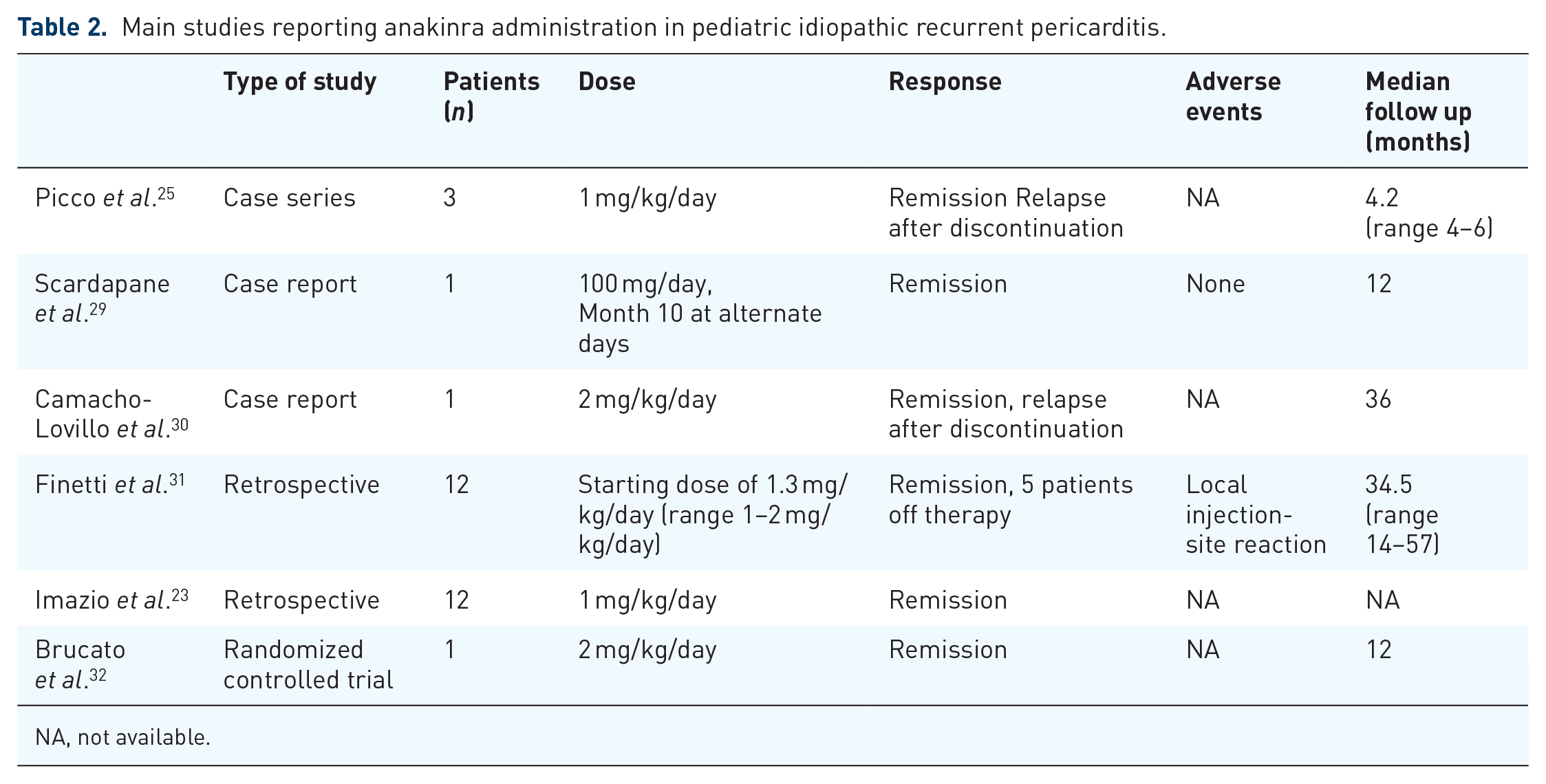
NA, not available.
In 2009, Picco et al. described the first small series of three pediatric subjects suffering from steroid-dependent IRP treated with ANA with an immediate clinical and laboratory response. 25 Pericarditis recurred when treatment was discontinued, and no relapses occurred after ANA was resumed. Subsequently, two further case reports have described the success of ANA therapy in IRP adolescents.29,30
A retrospective, multicentric evaluation of ANA efficacy both in children (n = 12) and adults (n = 3) with IRP showed a clinical and laboratory response in all patients with the concurrent withdrawal of steroid treatments. 31 During an attempt to taper treatment, approximately half of the patients experienced a flare, promptly controlled by ANA reintroduction. Moreover, during the follow-up period (median 39 months), a reduction of around 95% of relapses was observed compared with the pre-treatment period. In a large multicenter cohort study of 110 consecutive cases of IRP pediatric patients, ANA therapy was prescribed to 12 children. 33 In this subgroup, the number of recurrences dropped from 4.29 per year before ANA to 0.14 per year after (p < 0.05).
In the ANA Treatment of Recurrent Idiopathic Pericarditis (AIRTRIP) randomized controlled trial that enrolled 20 adult patients and 1 pediatric patient, ANA reduced the risk of recurrence over a median of 14 months compared with placebo. 32
The management of ANA discontinuation after remission remains controversial. Despite a lack of solid evidence, most experts recommend a gradual dose tapering. In a systematic review, Lazaros et al. recorded a 26% relapse rate during dose tapering or after drug discontinuation in 34 pediatric and adult patients with IRP successfully treated with ANA. 28
Behçet disease
BD is a multisystem inflammatory disorder characterized by variable involvement of the oral and genital mucosa, skin and eyes, and by a relapsing–remitting clinical course. The clinical spectrum includes mucocutaneous lesions (aphthous ulcers on the oral and/or genital mucosa, erythema nodosum, and other heterogeneous skin lesions), arthritis, eye involvement, vascular manifestations, gastrointestinal, and central nervous system involvement. The epidemiology of BD is strictly linked to the historical route of the Silk Road, with the highest incidence in Turkey and other Middle East countries, where an overall prevalence of 1 in 250 persons has been reported. 34 Most patients are diagnosed in young adulthood, although onset before the age of 16 is seen in 4–26% of cases. 35 The etiology remains unknown, but dysregulation of both innate and adaptive immunity is supposed. Recently, growing evidence supports the hypothesis of an autoinflammatory component in the pathogenesis of BD. Even if BD is typically considered a polygenic disorder with a predominant role for the sub-allele HLA-B51, a connection between the AIDs and BD is supported by the discovery of a hereditary ‘Behçet-like’ inflammatory syndrome. This rare condition, due to a mutation in the A20/TNFAIP3 gene, results in A20 protein haploinsufficiency causing a reduced suppression of nuclear-factor kappa B (NF-κB) activation and an abnormally increased inflammatory response. 36 Another similarity with AIDs is given by successful IL-1 inhibition in BD patients. Evidence from adult patients suggests that anti-IL-1 agents might be useful in the treatment of the most severe manifestation, unresponsive to conventional treatment with colchicine, steroids, or immunosuppressant drugs. 37 IL-1 antagonists, in particular ANA, are used off-label in both pediatric and adult patients; a survey among Italian physicians reported that ANA accounted for almost 10% of all off-label prescriptions during the period 2008–2016. 38
A recent systematic review suggested that IL-1 inhibitors may represent an effective therapeutic option, even if most of the data come from a limited number of observed patients. Bettiol et al. reported that ANA could be used effectively to control mucocutaneous symptoms and osteoarticular manifestations in BD patients and may represent an effective and safe therapeutic option for BD-related uveitis. 39
As for the use of anti-IL-1 treatments in the pediatric population, discrepant evidence was found, and the data are extremely limited (Table 3).38,40–42 In a case series of patients with BD resistant to standard therapy, Cantarini et al. described the case of a 7-year-old boy treated with ANA at a dosage of 2 mg/kg for BD non-responsive to prednisolone, colchicine, thalidomide, and mycophenolate mofetil. 40 The patient improved with the disappearance of systemic and mucocutaneous manifestations and steroid tapering. After 4 months, he experienced a disease relapse with abdominal pain, bipolar aphthosis, skin ulcers, and arthralgias. ANA dosage was subsequently increased to 2.5 mg/kg/day; clinical manifestations improved in frequency and intensity, although he still complained of severe oral aphthosis, abdominal distress, headache, and skin ulcers after 7 months.
Main studies reporting anakinra administration in pediatric Behçet disease.

FMF, familial Mediterranean fever; NA, not available.
The efficacy of ANA treatment has also been reported in a girl suffering from BD associated with FMF and will be described in detail in the next section. 41
Unsuccessful ANA treatment was reported in a letter by Ugurlu et al., who described persistent ocular inflammation despite treatment in a 16-year-old girl. 42 In another retrospective observational study, use of ANA in a child was associated with a partial response. 38
A higher dose of ANA may be efficacious in subjects initially unresponsive to the standard dosage, and may lead to complete remission. 38 However, an overall excellent safety profile has been reported in the literature and recently confirmed in two multicenter observational cohort studies including both pediatric and adult patients, which specifically evaluated side effects in BD patients treated with biologic agents.43,44
Familial Mediterranean fever
FMF is an autosomal-recessive AID characterized by recurrent attacks of fever and serositis.45,46 AA amyloidosis represents the main cause of mortality, which may complicate the disease due to persistent unremitting inflammation. Colchicine represents the milestone of FMF treatment, despite 10–15% of patients being either colchicine resistant or intolerant.47–50 Therefore, in such cases, additional or alternative treatment is required. The proof that FMF pathogenesis is driven by the overexpression of IL-1β justified the blockade of IL-1 as a potential target therapy.51–53 In this regard, canakinumab has recently been approved in resistant FMF, whereas ANA remains an off-label indication in pediatric patients. Most of the available literature refers to retrospective studies and short case series (Table 4). However, the efficacy of ANA is widely described in adult patients, in both systematic literature reviews and in randomized controlled trials.50,54 Hence, considering its efficacy and safety, ANA represents a valuable treatment option in resistant/intolerant FMF patients, including pediatric patients.55–59
Main studies reporting anakinra administration in pediatric FMF, TRAPS, HIDS and uAIDs.

CR, no attacks and APRs, i.e. C-reactive protein, erythrocyte sedimentation rate and serum amyloid A within normal range.
PR, decreasing the attack rate/duration ⩾50% and/or APPs reducing ⩾50%.
Data from Kostjukovits et al. 73
APPs, acute-phase proteins; APRs, acute-phase reactants; CR, complete response; FMF, familial Mediterranean fever; HIDS, hyperimmunoglobulinemia D syndrome; MKD, mevalonate kinase deficiency; NA, not available; OD, on demand; PR, partial response; TRAPS, tumor-necrosis-factor-receptor-associated periodic syndrome; uAIDs, undifferentiated autoinflammatory diseases.
Two case reports by Kuijk et al. and Calligaris et al. described a complete remission in adolescents with FMF, unresponsive to colchicine therapy.56,57 The first reported case described a 14-year-old patient that, after ANA administration, became free from disease attacks with normalization of C-reactive protein values. The patient also reported a marked improvement in quality of life and depressive symptoms. 56 Subsequently, in a larger pediatric series which demonstrated the efficacy and safety of ANA in achieving disease control, Ozen et al. reported a 60% rate of remission without adverse events in five pediatric patients with recurrent attacks despite optimal compliance to colchicine. 60 As observed in adult patients, ANA proved effective in restoring serum amyloid A levels to normal ranges as well as in reversing proteinuria and controlling disease progression in patients with secondary amyloidosis. Bilginer et al. reported the case of an 8-year-old girl with FMF and BD, complicated by secondary amyloidosis, who achieved clinical and biochemical remission after 6 months of therapy with ANA. 41 She remained asymptomatic, despite a gradual increase in proteinuria at the 18-month follow up.
In a cohort of seven pediatric FMF patients, four of whom had secondary amyloidosis, disease remission was achieved in all children with normalization of acute-phase reactants and regression of amyloidosis-related gastrointestinal findings. 61 One child with nephrotic syndrome achieved partial remission after 12 months. In two patients with chronic kidney disease and one with renal transplantation, the decline in renal function was interrupted.
Stronger evidence is derived from a larger series including 49 FMF patients, both pediatric and adult, 20 of whom received ANA. 75 Fourteen patients received ANA as a first biologic regimen, with a reported complete response rate of 50% (7/14), whereas biochemical control was achieved in 43% (6/14) of patients.
Tumor-necrosis-factor-receptor-associated periodic syndrome
TRAPS is the most common autosomal-dominant AID, characterized by recurrent attacks of prolonged fever, typically lasting several weeks, associated with different clinical manifestations including serositis, migratory rash, and ocular inflammation. 76 Many aspects of its pathogenesis remain unclear. However, there is evidence suggesting that an altered three-dimensional shape of TNFRSF1A leads to an increased production of pro-inflammatory cytokines and systemic inflammation through not completely clarified pathomechanisms. Among these, impaired TNFα binding, altered NF-κB pathway, abnormal neutrophilic TNFα-induced apoptosis, as well as defective TNFRSF1A trafficking have been described.77,78 NSAIDs could partially relieve symptoms and on-demand steroids usually block the attacks, but their efficacy decreases over time and a longstanding administration may cause the well-known side effects. 79 Moreover, these patients have an increased risk of AA amyloidosis. Based on a supposed TNFα-driven pathogenic mechanism, etanercept was administered in these patients without significant and longlasting efficacy. 80 Conversely, IL-1 blockade can control systemic inflammation in TRAPS. Canakinumab has been recently validated through two open-label studies demonstrating IL-β blockade superiority in achieving disease remission, compared with placebo.81,82 ANA remains off-label due to the lack of available randomized controlled trials, despite its widespread use in both adult and pediatric patients. Indeed, ANA has been demonstrated to induce rapid disease remission and prevent relapse. In the pediatric field (Table 4), the first study reporting data on ANA efficacy included four children affected by TRAPS with a recurrent or chronic course. 62 After 2 days of therapy, all patients showed resolution of symptoms with subsequent normalization of acute-phase reactants, including serum amyloid A, after 15 days. All patients relapsed a few days after treatment discontinuation at day 15, but they rapidly improved when ANA was resumed, maintaining a longlasting remission on therapy.
Since ANA induces a prompt response, administration of on-demand therapy appears a reasonable alternative approach, especially in cases of sporadic relapse and/or in patients intolerant to steroids. Grimwood et al. reported a favorable outcome of an on-demand treatment regimen with ANA in two pediatric patients with TRAPS. 63 ANA was administered within 24 h after the first clinical manifestations and treatment was continued for 5–7 days, depending on the usual duration of their attacks. After 24–48 h, both patients achieved a complete clinical response, and inflammatory markers normalized within a few days. No relapses were reported after treatment discontinuation.
ANA was administered in 33 subjects enrolled in the EUROFEVER registry: a complete response was reported in 79% (26/33) and a partial response in 15% (5/33) of cases. 79 In another cohort of 47 TRAPS patients (26 adults and 21 children), ANA was superior in inducing complete remission versus an anti-TNF regimen. 75
Mevalonate kinase deficiency
MKD is an extremely rare, autosomal-recessive AID, caused by mutations in the gene encoding mevalonate kinase (MVK) that lead to a partial enzyme deficiency. 83 MKD, also known as HIDS, shows a less severe phenotype compared with mevalonic aciduria (MVA), a disease with a critical MVK deficiency causing neurological involvement. 84 The enzyme defect interferes with the mevalonate pathway and cholesterol synthesis, and is responsible for IL-1β overproduction and systemic inflammation. 83 The typical clinic phenotype is characterized by recurrent attacks of fever lasting 3–7 days, associated with inflammatory symptoms such as lymphadenopathy, arthro-myalgia, mucocutaneous, and gastrointestinal manifestations. 83 NSAIDs and high-dose steroids are usually administered to relieve symptoms and reduce the duration of attacks. 79 Among biologic agents, those targeting IL-1 are the most effective.64,67,69,71,72 In a cohort of 38 MKD pediatric and adult patients treated with biologic therapies, ANA was administrated in 68% of cases as first-line therapy. 75 Further case reports have confirmed ANA efficacy in children.65,70 Moreover, a series of five pediatric patients was retrospectively described by Galeotti et al. (Table 4). In this study, ANA was administered daily in four patients and on demand in one patient, achieving complete and partial remission in 40% (2/5) and 60% (3/5) of patients, respectively. 68 In addition, a review of 21 pediatric patients treated with ANA observed a complete remission rate of 19% (4/21) and a partial remission rate of 71% (15/21). 73 Limited side effects were described, namely local injection-site reactions, bacterial pneumonia, and herpes zoster infection. Similar results were derived from a series including 27 adult and pediatric MKD patients treated with ANA: efficacy was reported in 89% of patients, with complete remission in 22%. 75
The co-existence with another disease, specifically early-onset ulcerative colitis and membranoproliferative glomerulonephritis, has been reported in two cases.65,70 Both patients were successfully treated with ANA and experienced a favorable control of MKD manifestations, as well as of the associated disease symptoms. Among pediatric studies, the case of a 10-year-old patient who experienced more prolonged and severe attacks under ANA, with rapid clinical improvement after discontinuation, is of note. 66
Undifferentiated autoinflammatory diseases
Patients who fulfill the clinical features of AIDs but have negative genetic screening for FMF, CAPS, TRAPS, or MKD, are defined as affected by uAIDs. Harrison et al. reported the efficacy of ANA administration in 9 of 11 uAID adult patients who were unresponsive to standard steroid/disease-modifying antirheumatic drug (DMARD) treatments. 85 Moreover, in a series of 22 pediatric patients retrospectively described by Garg et al., 72% of uAID children showed clinical improvement after ANA administration, with 36% achieving full remission within 3 months. 74 The efficacy of ANA has emphasized the implication of IL-1 dysregulation in the pathogenesis of uAID. Empirical trials of IL-1 blockade in uAID patients may be warranted, as long as advances in next-generation sequencing technologies can determine appropriate target therapies. In this study, ANA was well tolerated overall, and, unlike previous studies, the most common adverse event was infection, not local injection-site reaction (Table 4).
Chronic non-bacterial osteomyelitis
CNO is a group of autoinflammatory bone disorders typically affecting pediatric patients and characterized by accelerated bone remodeling and inflammatory bone loss. 86 The pathogenesis of CNO seems to be driven by IL-1 pathway over-activation and under-expression of the IL-10 family of cytokines. 87 The clinical spectrum ranges from asymptomatic localized bone inflammation to severe and disseminated forms. The most severe phenotype is represented by chronic, recurrent multifocal osteomyelitis (CRMO), characterized by bone pain and joint swelling potentially involving any skeletal site. 86 There are no validated treatments due to the rarity of the disorder. NSAIDs or high-dose steroids are prescribed as first-line therapies, depending on disease severity. When a response cannot be obtained, anti-TNFα agents and bisphosphonates are considered alternative regimens. 86 In patients refractory to such treatments, ANA appears to be a promising and safe option (Table 5).
Main studies reporting anakinra administration in pediatric CNO.

CR defined as no symptoms and radiological resolution of all bone lesions and no appearance of new bone lesions.
PR defined as symptoms improvement and/or decrease of radiological bone lesions.
CNO, chronic non-bacterial osteomyelitis; CR, complete response; NA, not available; PR, partial response.
The first report on the efficacy of ANA in CNO described the case of a 6-year-old girl with a recalcitrant disease unresponsive to NSAIDs, steroids, and bisphosphonates. 89 ANA was started, following the detection of high levels of circulating IL-1RA. After 6 weeks the symptoms resolved, and the inflammatory markers normalized. Unfortunately, remission was not sustained at the 1-year follow up, and, after a recalcitrant course, ANA was discontinued 3 years later.
In a retrospective analysis of 486 patients, including 455 pediatric CNO, ANA was administrated in four children, showing a complete remission in two patients, and a partial response or no response in one patient each. 86 The largest pediatric CNO series by Pardeo et al. described nine patients with refractory disease treated with ANA. 88 The response was evaluated through the Physician Global Assessment (PGA) scoring system, which included fever, functional impairment, inflammatory markers, and bone scintigraphy lesions. At baseline, all patients presented a mild-to-severe PGA and eight of nine patients had elevated inflammatory markers. After 6 months of therapy, five patients improved to a minimal or no PGA, and, in eight of nine patients, a reduction of acute-phase reactants was described, with normalization in five of them. Overall, 42 of 77 bone lesions resolved, and the remainder were stable. However, 20 new lesions appeared in 7 patients.
IL-1 targeting also demonstrated effectiveness in Majeed syndrome and deficiency of IL-1 receptor antagonist (DIRA) syndrome. Majeed syndrome is an autosomal-recessive disorder, caused by mutations in the LPIN2 gene and characterized by recurrent fever and the typical triad of CRMO, congenital dyserythropoietic anemia, and neutrophilic dermatosis.90,91 CRMO starts during infancy causing, if not recognized and treated, retarded growth, permanent joint contractures, and bone deformities. Steroids partially improve the bone and skin disease, whereas ANA can rapidly control systemic inflammation. Herlin et al. reported the case of a 2-year-old child with Majeed syndrome who was successfully treated with ANA for 6 weeks with prompt clinical and laboratory improvement, despite a rapid relapse after therapy discontinuation. 90
DIRA is an autosomal-recessive disease caused by the absence of the IL-1 receptor, characterized by neonatal onset and life-threatening manifestations. 92 The disease occurs within 3 weeks after birth with neutrophilic pustular rash, joint swelling, and oral mucosal lesions. The multifocal bone involvement leads to balloon-like widening of the ribs, periosteal elevation of long bones, and multiple osteolytic lesions. 92 Therapy with DMARDs and high-dose steroids can only partially control the clinical manifestations, whereas ANA has been demonstrated as highly effective in determining a complete resolution of symptoms and normalization of inflammatory markers. 92
Macrophage activation syndrome
MAS is a potentially fatal complication of several rheumatic disorders. The definition of MAS is applied to secondary hemophagocytic lymphohistiocytosis (sHLH) in the context of rheumatic diseases. In the pediatric age, sJIA is by far the disease most frequently complicated by MAS.93–95 However, in several reports the occurrence of MAS has been described during the course, or as revealing manifestation of AIDs (i.e. in CAPS, MKD, FMF and TRAPS), resulting in a severe complication with high morbidity and mortality rates.96–100
MAS is a unique clinical syndrome characterized by fever, organomegaly, cytopenia, and organ involvement up to multiple organ failure. Laboratory abnormalities include a decrease in white blood cells, platelet and hemoglobin, hypertransaminasemia, marked increase in ferritin, and evidence for intravascular coagulation activation. Uncontrolled activation and proliferation of T lymphocytes and macrophages are the typical immunological features.
Since 2008, several studies showed favorable results following ANA administration in patients affected by MAS unresponsive to conventional treatments (i.e. steroids, cyclosporin, IVIG) (Table 6).101–105 In this regard, Miettunen et al. described the achievement of clinical and biochemical remission with ANA in 12 patients with MAS (including five patients who required intensive care support) after the failure of treatment with steroids and other immunosuppressants. 106 Moreover, all patients experienced a good control of the underlying rheumatic diseases at follow up (Table 6).
Main studies reporting anakinra administration in pediatric MAS.
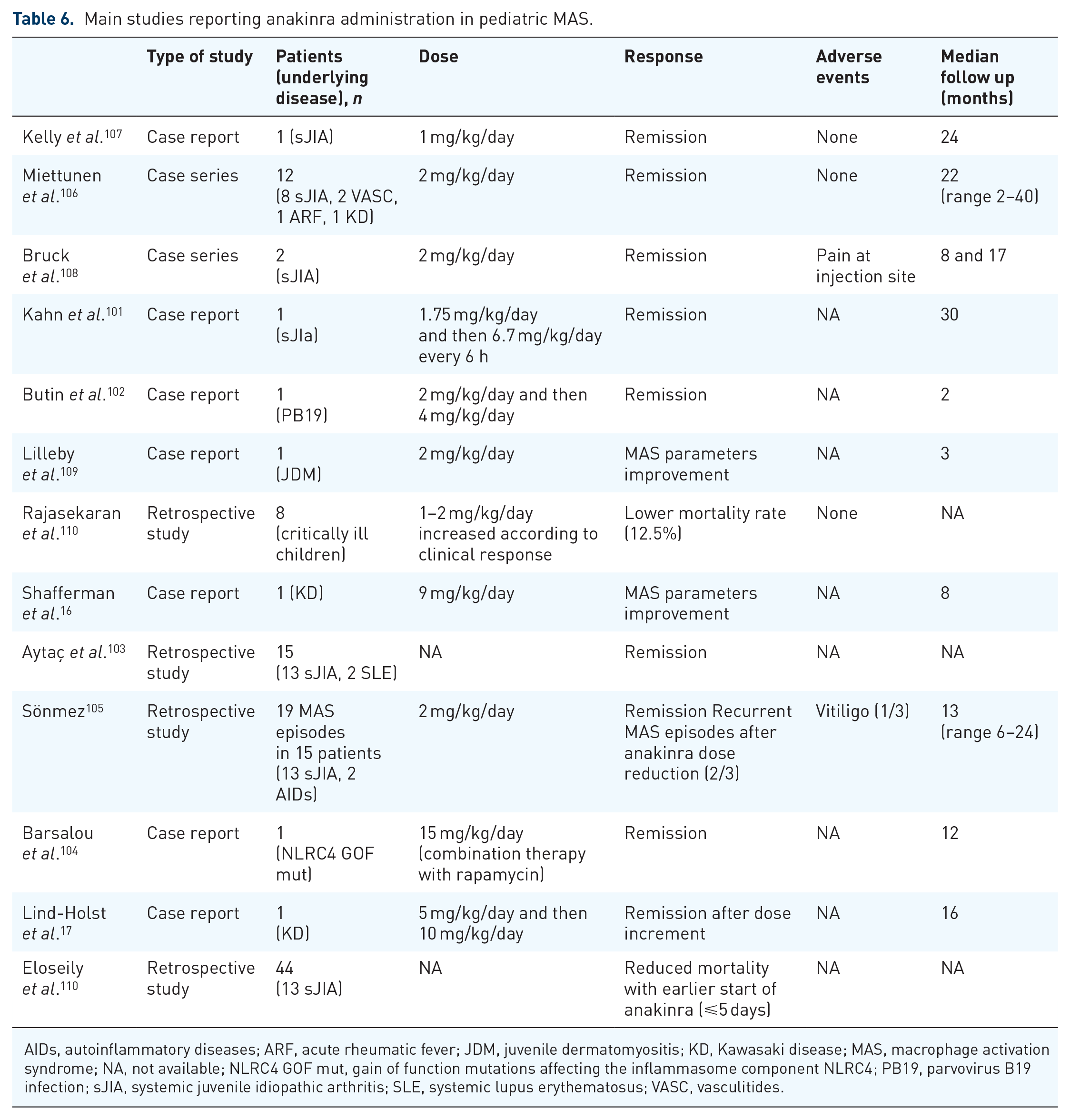
AIDs, autoinflammatory diseases; ARF, acute rheumatic fever; JDM, juvenile dermatomyositis; KD, Kawasaki disease; MAS, macrophage activation syndrome; NA, not available; NLRC4 GOF mut, gain of function mutations affecting the inflammasome component NLRC4; PB19, parvovirus B19 infection; sJIA, systemic juvenile idiopathic arthritis; SLE, systemic lupus erythematosus; VASC, vasculitides.
In most of the available studies, ANA was administered at the standard dosage (1–2 mg/kg/day).105,107–109 The response to treatment appears rapid and without significant side effects; only one case reported pain at the injection site. 108 However, a higher dose of ANA (ranging from 4 mg/kg/day to 15 mg/kg/day) was required to achieve remission in other studies, especially in the case of MAS associated with KD.16,17
While most of the patients received ANA in association with steroids, IVIG, or immunosuppressive drugs, monotherapy seems to be promising in patients affected by sJIA developing MAS. A recent retrospective study demonstrated that an earlier introduction of ANA treatment, within 5 days of MAS onset, was associated with reduced mortality, especially when sJIA represents the underlying diagnosis. 111
ANA treatment is not only limited to rheumatologic patients but is also adopted in children and adults affected by infection-associated sHLH and in critically ill patients with various underlying diseases. 110,112,113 The efficacy of IL-1 blockade in a cytokine storm was also confirmed by clinical experience in septic shock. 110,112,113
On the other hand, some studies reported that children with sJIA treated with ANA developed MAS.114,115 Nigrovic et al. described MAS in four patients receiving ANA, but none showed a clear causal association, and all patients could ultimately continue the therapy. 114 The underlying active disease rather than drug administration could be the real trigger of MAS. According to the authors, ANA at 1–2 mg/kg/day was not sufficient to prevent MAS in sJIA; but once it occurred, clinical features improved after dose increase. 114
A double-blind, randomized controlled trial [ClinicalTrials.gov identifier: NCT02780583] is currently underway to assess the efficacy, safety, and tolerability of ANA in combination with standard prescribed treatment for children and adults with MAS.
Febrile-infection-related epilepsy syndrome
FIRES is a subtype of new-onset refractory status epilepticus. According to the consensus definitions, it is a rare catastrophic epileptic encephalopathy characterized by a preceding febrile infection between 24 h and 2 weeks before the onset of seizures. 116 FIRES diagnosis is essentially clinical, and the syndrome should be suspected in patients of all ages. In pediatric patients, the estimated annual incidence is 1:1,000,000, while its prevalence is 1:100,000 in previously healthy children and adolescents. 117 FIRES is characterized by relentless cognitive and motor function decline and severe neurological sequelae with a high mortality rate. 118 The FIRES seizure pattern is usually resistant to multiple antiepileptic drugs. Alternative treatment options such as anesthetic drugs, immunotherapy, ketogenic diet, therapeutic hypothermia, and cannabidiol have shown only partial efficacy.119–121
Recent studies have evoked the role of IL-1β in seizure onset. 122 Experimental animal models support this hypothesis: IL-1β receptor-deficiency in mice seems to have a protective role against febrile seizures since high IL-1β doses induce epilepsy in IL-1β-receptor-expressing mice. 123 Another study proposed that FIRES is probably associated with reduced expression or functional deficiency of the intracellular IL-1 receptor. 124 This evidence justifies targeted therapy with IL-1 antagonists, especially ANA (Table 7). In the first reported case by Kenney-Jung et al. a 32-month-old girl with super-refractory status epilepticus despite multiple drugs and a 3-day course of high-dose methylprednisolone, was treated with ANA (5 mg/kg twice daily, subcutaneously) resulting in a progressive decrease in the frequency of recurrent seizures. 125 However, relapse was experienced after ANA withdrawal. A similar clinical response was described in four of five children suffering from FIRES treated with ANA at a dose ranging from 3 mg/kg/day to 7 mg/kg/day. 126 Further case reports confirmed ANA efficacy.127,128 Moreover, ANA was associated with deep brain stimulation of the centromedian thalamic nuclei in two boys, reporting a positive effect in one patient. 129
Main studies reporting anakinra administration in pediatric FIRES.

EEG, electroencephalogram; FIRES, febrile infection-related epilepsy; NA, not available.
Finally, Kenney-Jung et al. reported elevated levels of pro-inflammatory cytokines in cerebral spinal fluid before treatment that normalized after ANA administration, emphasizing a pathogenic role of autoinflammation in FIRES. 125
Conclusion
AIDs represent a heterogeneous group of disorders related to multiple genetic defects, including inflammasomes, proteasome, cytokine receptors or inhibitors, and different enzymes. 130 In pediatric AIDs, off-label use of ANA has been widely demonstrated as effective and safe. ANA should be considered in selected children suffering from systemic inflammatory diseases who do not tolerate other therapies or who require unacceptably high doses of steroids to control a severe and/or relapsing disease course.
Clinicians should direct the choice to switch to ANA based on the AID-related damage assessment, to capture potentially irreversible disorders of structure and function. Reproducible scores to evaluate the subsequent response to therapy in an objective way and to compare patients belonging to the same clinical setting or from different cohorts are needed. In the damage assessment, therapeutic toxicity must also be considered, for example, growth retardation, weight gain, and hypertension derived from chronic glucocorticoid consumption. In this regard, the autoinflammatory disease damage index has recently been developed for the evaluation of FMF, TRAPS, MKD, and CAPS patients. 131
ANA has a remarkable safety profile with over 150,000 patients treated daily for over 10 years. 132 Since blood levels drop significantly within a few hours after discontinuation of treatment, ANA represents a manageable drug. 3 In suspicion of AIDs, ANA could be considered as an empiric treatment in case of temporary contraindication to glucocorticoids for diagnostic workup, while waiting to exclude infection or malignancy. 133
However, some points need to be clarified in the near future: what kind of patients need treatment with ANA, which subgroup of patients could receive ANA as first-line therapy, how long should therapy be prolonged, and how and when it should be tapered or discontinued after the achievement of remission. In this regard, randomized controlled trials and large series with long-term follow up are still an unmet need.
Footnotes
Acknowledgements
Editorial assistance was provided by Melanie Gatt (PhD), an independent medical writer, on behalf of Springer Healthcare.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: SOBI, Swedish Orphan Biovitrum s.r.l., provided financial support for editorial assistance.