
Abstract
The treatment of chronic, non-cancer musculoskeletal pain has become a topic growing interest as it is believed to be one of the reasons for the current opioid epidemic. The medicinal use of cannabis has a long history as a number of active compounds in cannabis have been shown to interact with the body’s endocannabinoid system to reduce pain. This position paper provides a history on the evolution of cannabis, the science behind its therapeutic effects, and review of the evidence and current guideline recommendations on its use as a treatment for patients with chronic, non-cancer musculoskeletal pain. Results from systematic reviews have demonstrated a statistically significant reduction in chronic pain conditions with cannabinoids, compared with placebo, although the effects might be considered small and did not reach the minimally important difference. More adverse events were reported in the cannabinoid group than in the placebo group with longer than 2 weeks of treatment. There is a lack of evidence on dependence. With changes to policies, patients’ perception has changed to be more positive toward the use of medical cannabis. Current recommendations from North America, Latin America, Europe, Australia and Iran support the use of medical cannabis for chronic, non-cancer pain. Based on the current evidence, it is our position that cannabinoids may be considered as an adjunctive therapy after recommended first- and second-line therapies have failed to provide sufficient efficacy or tolerability. Patients should consider the balance between the desirable and undesirable effects of taking cannabis for chronic pain, and comprehensively consider their own values and preferences, as well as cost-effectiveness factors, based on the information provided by their physician.
The impact of musculoskeletal pain
Musculoskeletal pain is a clear driver of the opioid epidemic, as acute and chronic musculoskeletal pain continue to be among the leading reasons for patients to seek opioid prescriptions from providers. 1 While the initiation of this class of analgesics may often be considered when treating severe injuries or intractable pain, its addictive potential and narrow toxic range make it a high risk first-line medication. The opioid epidemic continues to dominate headlines as opioid-related hospitalizations and emergency department visits in Canada have ballooned by over 50% during the last decade, with the majority occurring over the last 3 years. 2 Even more staggering is the 500% increase in opioid-related deaths across North America over the last year, with over 50,000 reported fatalities; more than a third of which are related to prescription medications.2,3
Canadian and American guidelines have been putting forth for responsible prescribing of opioids, and discourage their use in the treatment of chronic, non-cancer pain (CNCP), which is defined as persistent or recurrent pain lasting beyond 3 months or having an established diagnosis of a chronic condition that is not associated with cancer.4–7 However, opioids remain the default choice for the majority of orthopaedic providers across North America, with deeply ingrained practice patterns leading to their routine prescription following an orthopaedic injury, surgery, or worsening degenerative bone and joint diseases.
The purpose of this position was to provide an overview of the history of medical cannabis, how cannabis functions based on laboratory findings, and the current evidence and healthcare guidelines on its applications for patients with CNCP. We intended to provide knowledge of medical cannabis and facilitate patient decision-making, in this evidence-based position paper.
The evolution of cannabis use
In parallel with the rising opioid crisis, there has been a societal shift in attitudes surrounding another of the world’s most commonly used recreational drugs. With an estimated 200 million current or past users worldwide, cannabis usage has spread to every continent, despite being illegal in almost all countries. Much of the controversy surrounding cannabis has focused on its associated euphoric ‘high’; however, the plant has been integrated throughout civilizations over thousands of years, primarily for non-euphorigenic purposes. Ancient texts describing cannabis use in traditional Chinese medicine date back as early as 2700 BC, and archeologic findings from East Asia indicate that cannabis may have been used by humans up to 10,000 years ago (Figure 1). 8 Over centuries, cannabis and its derivatives have been utilized as textile bases, food sources, analgesics, anti-inflammatories, antiemetics, and mood enhancers. By the 1800s, cannabis was a widely grown agricultural crop, mainly to produce sails and ropes using hemp plants that had little to no psychotropic potential. However, in many areas of Asia and the Middle East, marijuana was commonly infused into food and liquids, or smoked as hashish for both medicinal and recreational purposes.
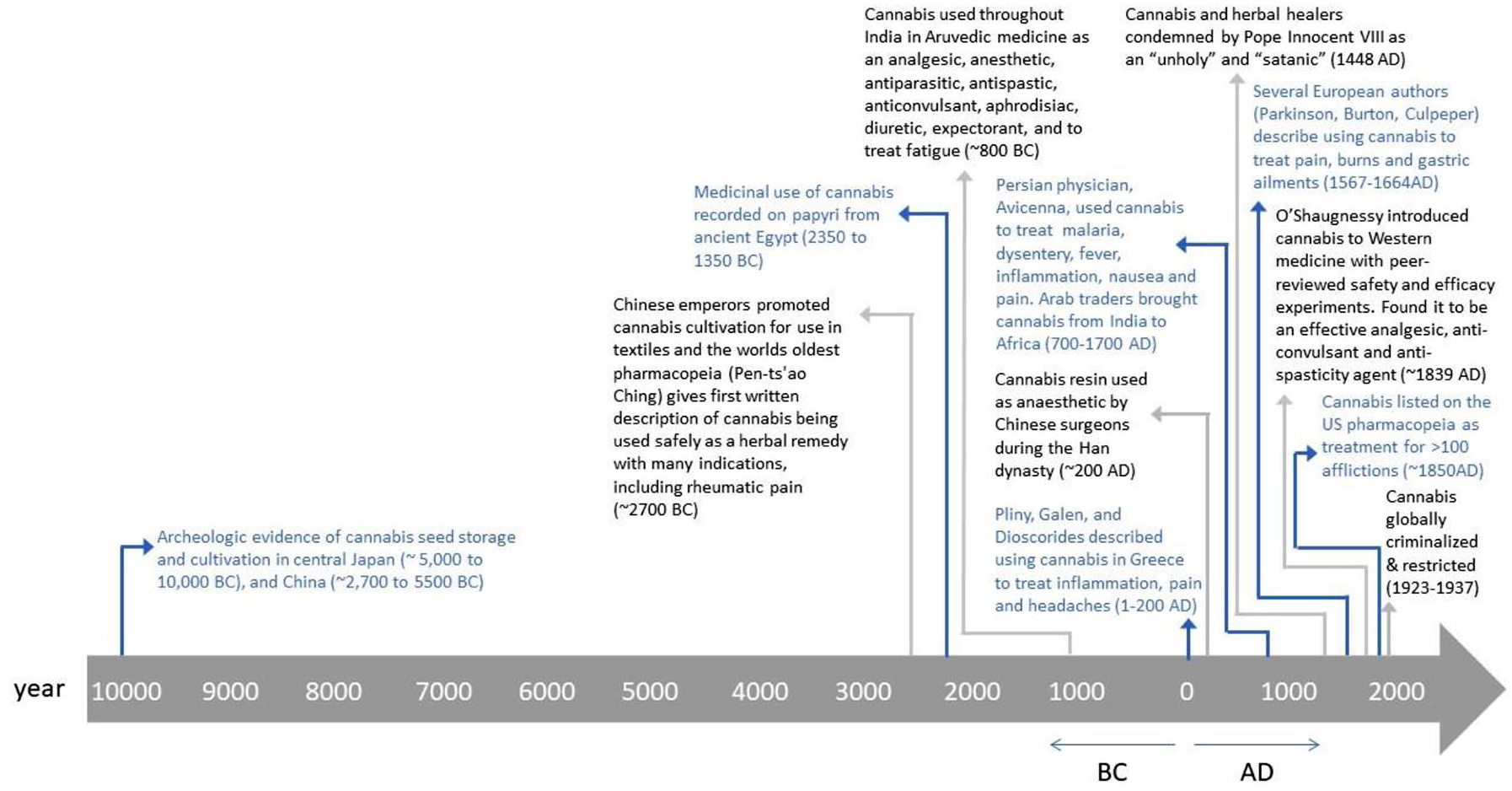
Timeline of cannabis use throughout human civilization.
Medicinal applications of cannabis remained largely unknown to the West until the mid-1800s, when William O’Shaughnessy, an Irish physician working in Calcutta, India, first reported a series of basic animal experiments and human cases on various Indian Ayruvedic medicinal claims.8–10 Based on his studies on cannabis extracts and tinctures, O’Shaughnessy recommended its use for spasticity, pain and epilepsy-related convulsions.8–10 Following this, the availability of cannabis extracts in over-the-counter medications, as well as its general use, proliferated rapidly throughout North America and Europe and, by 1850, cannabis was listed in the United States (US) Pharmacopeia as a treatment option for approximately 100 symptoms. On the other hand, many in the West were concerned about users’ report of cannabis-induced hallucinations and an overall dulling of senses. 10 This led to its moral and political opposition in the early 20th century. 8
By 1906, the Pure Food and Drug Act required any cannabis-containing product to clearly identify its components and, by 1912, a certification was required for the importing of any cannabis-containing product. 10 Both in the US and globally, cannabis has remained under the most restricted schedule category of controlled substances, with the 1970 Drug Abuse Prevention and Control Act and 1971 World Health Organization (WHO) treaty defining it as having a high potential for abuse with no currently accepted medicinal use and a lack of safety data to permit its use under medical supervision.11,12
Despite this, various countries have challenged this designation and have permitted limited medical and recreational use of cannabis based on a growing body of scientific evidence and sociopolitical shift in attitudes. 13 The 17 October 2018 marked the day that Canada became the second country to fully legalize the use of cannabis (Uruguay was the first in 2013). 14 Since then, several other countries have enacted similar legislation or are considering doing so in the near future, including South Africa, New Zealand, and the United Kingdom. In addition, the WHO now recommends reclassifying cannabis under international treaties to permit its medical use.12,14 Currently, in the US, recreational and medical use of cannabis is legal in 10 states, with an additional 23 states providing legal medical access for a limited list of conditions.8,13
Surrounding this shift in cannabis legislation, more emphasis has been put on generating new scientific evidence on the efficacy and safety of cannabinoids for an array of medical indications, including its use as an opiate alternative.
Basic science of cannabis
The cannabis plant’s flowers and leaves have been found to contain about 500 distinct compounds and 144 different cannabinoids, of which delta-9-tetrahydrocannabinol (∆9-THC, THC) and cannabidiol (CBD) are the most common (Box 1).15–18 The relative proportions and effective concentrations of these and other possibly active cannabinoids varies, and are not standardized outside of plants legally cultivated by licensed producers in North America.19,20
Key terms.
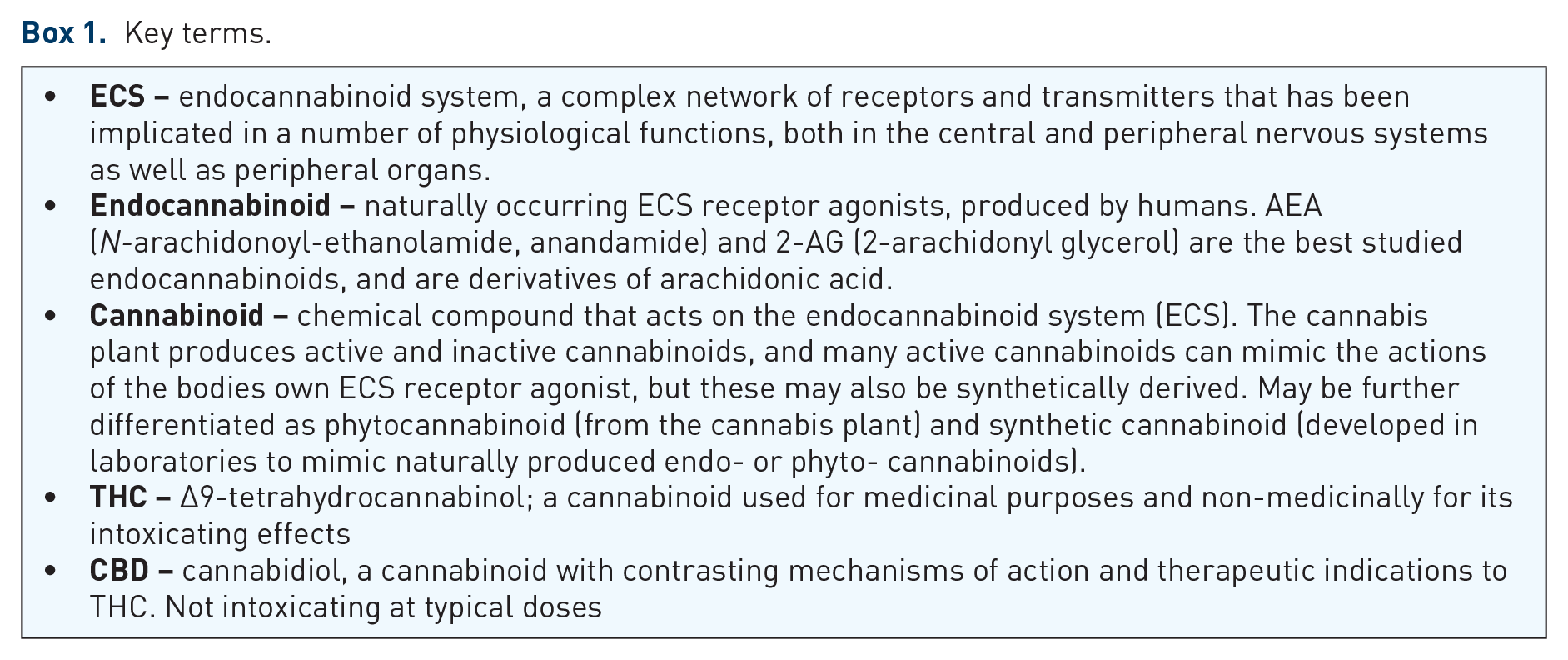
Among the chemical constituents of cannabis, THC is the most considerably studied and responsible for the majority of the physical and psychotropic effects. 21 The average amount of THC is typically 10–12.5% (range 1–30%) in cannabis plants found on markets in Canada. CBD, the second most prevalent cannabinoid in most strains of cannabis (with typical concentrations of < 1%), has effects counter to those of THC, with less psychoactive potential and more calming and anti-inflammatory effects. 22 The interaction between THC and CBD is complex, and there may be benefits to using them in combination as CBD may temper the undesired psychotropic side-effects associated with THC.22,23 Other cannabinoids are present in the plant with lesser amounts (0.5%) and pre-clinical research suggest that they may have their own independent effects. In vitro and in vivo mouse studies have indicated that cannabinol (CBN) may been associated with prolonged sleep, 24 and that non-psychoactive cannabigerol (CBG) and tetrahydrocannabinolic acid (THCA) may protect against neurodegeneration.25,26 THCA is a THC precursor that have many of the same molecular targets as THC that play a role in anti-inflammation, immunomodulation, neuroprotection and antineoplastic actions, and is not associated with potentially undesired psychoactive effects. 26 The remainder of the plant consists of non-cannabinoid compounds, such as terpenes and flavonoids, that have little, if any, psychotropic properties, but may have additional therapeutic actions (e.g. anti-oxidant, anti-anxiety, anti-inflammatory, anti-bacterial, anti-neoplastic).16,21 Laboratory studies have indicated that the interaction between the various cannabinoids and non-cannabinoid compounds from the plant may result in increased effectiveness while decreasing negative side-effects when administered together, indicating that trying to isolate individual compounds from cannabis may not be the best approach.23,27–30 Furthermore, in living plants, the phytocannabinoids exist as both inactive monocarboxylic acids (e.g. THCA) and active decarboxylated forms (e.g. THC), with biologic activation occurring when heated to a temperature above 120°C.31–33 This leads to a transformation into a number of active compounds, many of which contribute further to the varied physiological effects as they interact with the body’s endocannabinoid system (ECS).
The ECS is implicated in inflammation, bone development, and pain. Also, the ECS is involved in other physical functions or systems including memory, learning, reproduction, appetite, psychiatric symptoms, psychomotor behaviour, digestion, sleep and wake cycles, the regulation of emotion, and synaptic plasticity. 34 This has led to concerns regarding the non-specific effects of cannabis, including undesired side-effects. The ECS is comprised of two main receptors, cannabinoid receptor type-1 (CB1) and type-2 (CB2), as well as endogenous ligands that bind and activate these receptors [N-arachidonoylethanolamide (AEA) and 2-arachidonyl glycerol (2-AG)]. Although found throughout the body, including the brain, endothelium, gastrointestinal lining, lungs, bone and muscle, there is considerable variation in receptor expression. CB1 receptors are highly localized to the central and peripheral nervous systems, whereas CB2 receptor expression is greatest in the immune tissues and can also be found in bone and muscle.33–35 In addition, a number of cannabinoids and other constituent compounds are believed to bind to target receptors outside of the ECS, such as the serotonin 1A receptor (or 5-HT1A receptor), 36 voltage gated sodium channels 37 and G protein-coupled receptor 55 (or GPR55), 38 furthering the complexity of determining the impact of cannabis use.
Can cannabinoids treat chronic musculoskeletal pain?
A recent British Medical Journal (BMJ) evidence review indicated, with moderate certainty, that nabiximols had a higher odds of providing a 30% reduction in pain scores compared with placebo for patients with chronic pain [odds ratio 1.46, 95% confidence intervals (CI) 1.16–1.84; reduction in pain scores was statistically significant, but clinically non-significant], but was no more effective than placebo in treating symptoms associated with multiple sclerosis.39,40 The authors of the review also concluded that cannabinoids may provide a 50% reduction in seizure frequency and alleviate symptoms of chemotherapy-associated nausea and vomiting; however, there was only low certainty in the results for these indications. 39 The inclusion of low-quality trials, heterogeneous studies, and failure to perform a comprehensive assessment of methodological quality may result in misleading findings from meta-analyses.40–46 Given this, although there are clinical trials that have investigated other indications for the therapeutic use of cannabinoids, including post-traumatic stress disorder, anxiety, sleep and schizophrenia, among others, there is currently insufficient evidence to estimate efficacy in these areas.39,44,47,48 Among the indications examined, the treatment of pain is the most pertinent for orthopaedic patients, who suffer from a combination of acute pain associated with musculoskeletal injuries and the perioperative period, as well as chronic pain associated with degenerative conditions such as arthritis or long-standing back pain. This is reflected in the fact that, under previous Canadian medical cannabis access programs, 65% of Canadians authorized to possess medicinal cannabis claimed to need it for severe arthritis. Similarly, in one US pain clinic, up to 80% of cannabis users report myofascial pain as their primary diagnosis.16,49 Especially amid the opioid epidemic, the use of cannabinoids for specific analgesic indications may represent the most promise for their clinical integration; however, a thorough look at the safety and efficacy of the evidence surrounding these indications is required.
Although limited clinical evidence supports the use of cannabinoids for chronic, non-cancer related pain, studies continue to emerge rapidly; therefore, we performed a systematic review that included 36 randomized controlled trials (RCTs, 4006 participants) comparing cannabinoids to placebo on patients with CNCP (MEDLINE search strategy in Supplement).50–86 We found that, compared with placebo, cannabinoids showed a statistically significant reduction in pain scores. Within the first 2 weeks of treatment, cannabinoids had a greater reduction in pain, measured on a 0–10 visual analog scale, compared with placebo (–0.54, 95% CI –0.76 to –0.31). This difference remained statistically significant at 2 months (–0.68, 95% CI –0.96 to –0.40) and, though the effect estimate decreased, it still remained significant by 6 months (–0.43, 95% CI –0.75 to –0.10). 50 Based on the recommended minimally important difference (MID) of 10 mm on a 100 mm visual analogue scale (VAS) when reporting treatment effects regarding pain, which is equivalent to 1 cm on a 10 cm VAS 87 ; the differences in our findings did not reach the threshold of MID at any duration of treatment. There is little evidence that cannabinoids increase the risk of experiencing serious adverse events, although non-serious adverse events may be common when longer than 2 weeks’ treatment. Serious adverse events were rare and risks were similar across the cannabinoid (74/2176, 3.4%) and placebo groups (53/1640, 3.2%) at the longest follow-up. The most commonly reported adverse events included dizziness, drowsiness, dry mouth, nausea, fatigue, headache and euphoria. We did not find significant differences between subgroups of natural extracts of marijuana (THC, CBD, combination of THC and CBD) and synthetic cannabis (ajulemic acid, nabilone, dronabinol) on pain reduction or adverse events between. 50
Although there are concerns regarding potential dependence associated with long-term and high-dose cannabinoids for pain, there is a lack of evidence.88–91 An answer to such a question requires a minimum 6 months follow up from an RCT or large observational study. 92
Based on the current available research findings, low-to-moderate-quality evidence shows that cannabinoids are associated with a small, but statistically significant reduction in chronic pain. In addition, there is a need for further research to investigate the optimal route and composition of cannabinoids in the musculoskeletal pain setting, including large, high-quality RCTs to better understand the risks and benefits of cannabinoids in this patient population.
Making sense of current guideline recommendations
The overarching message emerging from both the Canadian and American Medical Associations remains one of extreme caution.93–95 They emphasize that, while there may be a limited role for cannabis in select patients with terminal illness or chronic disease refractory to conventional therapies, there is an overall lack of clinical evidence for most of the purported indications for cannabis. This includes musculoskeletal pain, which has been a driver of prescriptions since 2001, when Health Canada first granted access through the Marijuana Medical Access Regulations (MMAR). Current recommendations from North America, Latin America, Europe, Australia and Iran are consistent in supporting the use of medical cannabis for chronic, non-cancer pain, with comprehensive knowledge sharing and consideration of a patient’s own values and preferences. Physicians are suggested to take a shared decision-making approach to discuss the prescription of cannabinoids with their patients.89–92,96–103
Changes to policies regarding the use of medical cannabis have occurred worldwide. These changes might be related to a transition in the public perception of cannabis and attitudes towards cannabis.104,105 A survey enrolling approximately 1000 participants, among whom two-thirds were diagnosed with chronic pain, in the US found a level of 75% symptom relief with cannabis prescription. In the same study, over one-third of the near 2600 qualitative responses conveyed health benefits of the medical cannabis in treating their condition. 106
Conclusion
Cannabinoids are being approved globally for pain management, especially in the last decade. Controversies and uncertainties on the trade-off between the benefits and harms of medical cannabis still remain. Whether or not cannabinoids can be used as an opioid-deterrent requires further investigation. Our current evidence review serves as a position paper to inform orthopaedic surgeons on the appropriate use of medical cannabis for their patients presenting with chronic musculoskeletal pain. Based on the current evidence, cannabinoids may be considered as an adjunctive therapy after recommended first- and second-line therapies have failed to provide sufficient efficacy or tolerability. In general, the evidence on cannabinoids in musculoskeletal patients based on high-quality clinical trials are limited. Prescribers need to supervise all patients taking cannabinoids for any condition.
Supplemental Material
TAB937968_Supplemental_Material_CLN – Supplemental material for Medical cannabis for orthopaedic patients with chronic musculoskeletal pain: does evidence support its use?
Supplemental material, TAB937968_Supplemental_Material_CLN for Medical cannabis for orthopaedic patients with chronic musculoskeletal pain: does evidence support its use? by Herman Johal, Christopher Vannabouathong, Yaping Chang, Meng Zhu and Mohit Bhandari in Therapeutic Advances in Musculoskeletal Disease
Footnotes
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: A research grant was received from Spectrum Therapeutics, A Canopy Growth Company.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.