
Abstract
Background:
Cardiovascular autonomic neuropathy (CAN) is a significant risk predictor for sudden cardiac death in autoimmune rheumatic diseases. As yet, there is no therapeutic treatment of CAN in psoriatic arthritis (PsA). Even now, the impact of the most commonly employed disease-modifying antirheumatic drug (DMARD) therapy on CAN in PsA is not known. Hence, we investigated the impact of DMARDs on CAN in PsA.
Methods:
In this prospective, cross-sectional study, 20 patients of PsA and 20 age- and sex-matched healthy controls were recruited. CAN was diagnosed by applying the five cardiovascular reflex tests according to Ewing. Parasympathetic dysfunction was established by performing three tests: heart-rate response to deep breathing, standing, and Valsalva tests. Sympathetic dysfunction was examined by applying two tests: blood pressure response to standing, and handgrip tests. Disease severity was assessed by the 28-joint-count disease activity score (DAS-28) and the disease activity score in psoriatic arthritis (DAPSA).
Results:
Cardiovascular reflex tests were impaired significantly among the PsA patients compared with well-matched healthy subjects (p < 0.05). Parasympathetic dysfunction was more prominent than sympathetic dysfunction. After 12 weeks treatment, parasympathetic dysfunction (heart rate response to deep breath and standing) significantly (p < 0.05) improved in patients with PsA, while there was no significant improvement in sympathetic function.
Conclusion:
These study results suggests parasympathetic autonomic dysfunction is more prominent than sympathetic dysfunction in PsA. Synthetic DMARDs improved parasympathetic dysfunction in PsA.
Keywords
Introduction
Cardiovascular autonomic neuropathy (CAN) is a significant risk predictor for sudden cardiac death in rheumatic diseases [Milovanovic et al. 2010]. Interestingly, autonomic neuropathy is a third form of neurological involvement observed in these diseases [Toussirot et al. 1999]. Rheumatic diseases are characterized by excess cardiovascular (CV) morbidity and mortality [Amaya-Amaya et al. 2014; Wright et al. 2014]. Autonomic neuropathy has been known to occur in rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), systemic sclerosis, Sjögren’s syndrome and ankylosing spondylitis (AS) [Stojanovich, 2009], but was first reported in psoriatic arthritis (PsA) by Syngle and colleagues in 2013 [Syngle et al. 2013]. However, no therapeutic treatment strategy for CV autonomic dysfunction in PsA has been demonstrated. We do not even know the impact of disease-modifying antirheumatic drugs (DMARDs) in the treatment of PsA.
In this study we aimed to investigate the impact of DMARDs on CV autonomic dysfunction in PsA patients.
Material and methods
Study participants
The study population consisted of 20 PsA and 20 unrelated, age- and sex-matched healthy control subjects. The baseline demographic and clinical features of PsA patients and healthy control subjects are described in Table 1. The diagnoses of PsA patients were according to CASPAR criteria (classification criteria for psoriatic arthritis) [Taylor et al. 2006]. Inflammatory disease activity was assessed using the 28-joint-count Disease Activity Score (DAS-28) and Disease Activity in Psoriatic Arthritis (DAPSA). Erythrocyte sedimentation rate (ESR) was measured by the Westergreen method and the C-reactive protein (CRP) level was determined using standard commercial kits. Body mass index (BMI) was calculated as the ratio of weight (kg) to height (m) squared (kg/m2). Biochemical assessment, including a complete blood count, liver function tests, renal function test, vitamin B12 and glycated haemoglobin (HbA1c) levels were determined using standard commercial kits. All of the clinical and biochemical assessments were done on the same day of the recruitment and after 12 weeks’ treatment. Autonomic measures were double blinded to the physician and patients for the study duration. Therefore, the patients were treated without influence of the autonomic function data.
Demographic and clinical features of the study population.
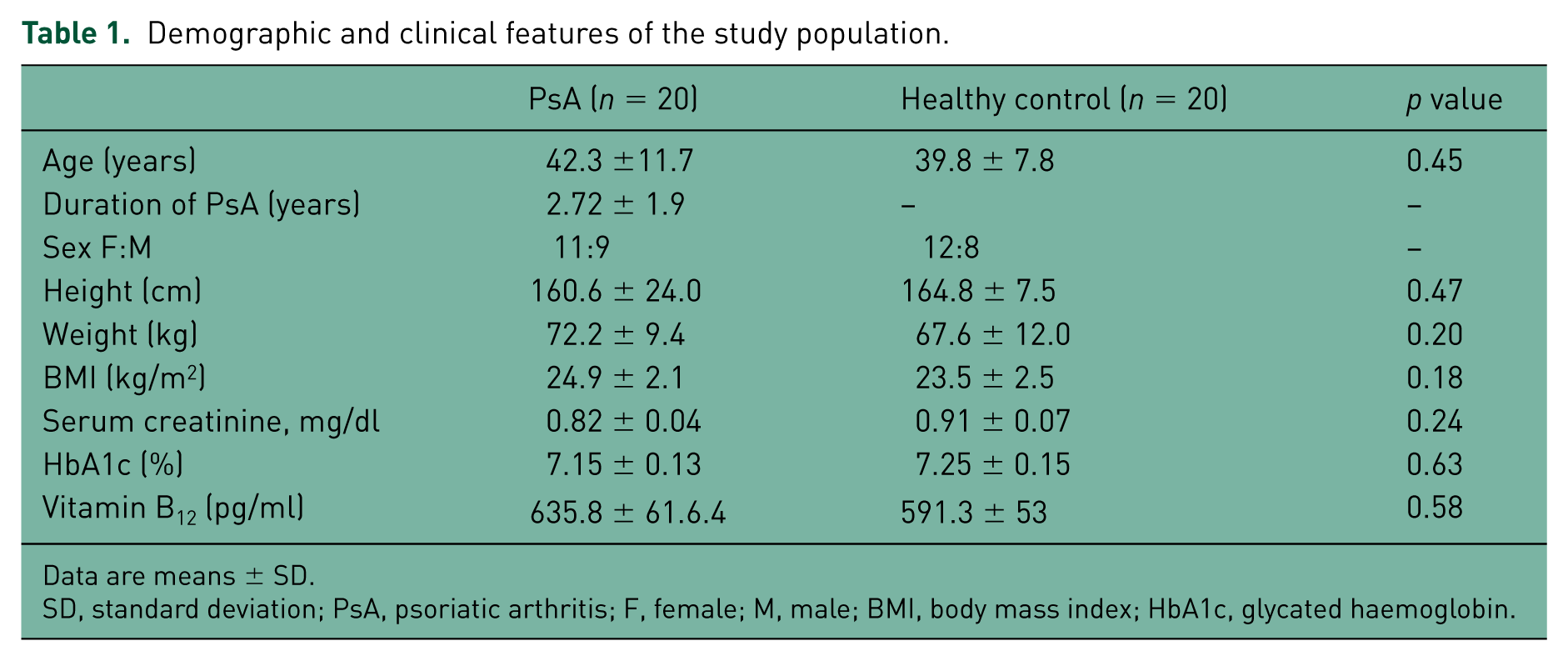
Data are means ± SD.
SD, standard deviation; PsA, psoriatic arthritis; F, female; M, male; BMI, body mass index; HbA1c, glycated haemoglobin.
Patients were excluded from the study if they had any of the following conditions: presence of skin lesions that could affect the ability to assess their neuropathic pain, renal or liver insufficiency, thyroid disorder, diabetes mellitus, pregnancy, patients on neuroprotective drugs, β blockers, antihypertensive drugs, vitamin B12 deficiency, anaemia, cardiac failure, cardiac arrhythmia, acute thrombosis, pericarditis or nephritis, paraneoplastic neuropathy, alcoholism, smokers and patients on steroid therapy. Patients with disorders responsible for neuropathy and neurological disorders other than rheumatic disorders were also excluded. Patients with PsA who were scheduled to start treatment with synthetic DMARDs were referred to the Cardio Rheuma Division for the assessment of autonomic function. The researcher involved in assessing the autonomic function was blinded to the treatment protocol. The project was approved by the regional institutional clinical ethics committee of the Punjabi University Patiala, India, and was performed in accordance with the declaration of Helsinki and the code of Good Clinical Practice. All DMARD-naïve PsA patients were initiated on methotrexate (10–15 mg/week) along with sulfasalazine (1–3 mg/day).
Assessment of cardiovascular autonomic neuropathy
CV autonomic function assessment was done using noninvasive CV reflex tests, the gold standard for the diagnosis of CANs [Balcioglu and Muderrisoglu, 2015]. All tests were performed under standardized conditions, in climate-controlled rooms (temperature 23°C), in the morning. CV autonomic functions tests were carried out at baseline and after 12 weeks of treatment.
Clinical measurements of CV autonomic neuropathy were carried out using the battery of five CV reflex tests, described by Ewing and Clarke [Ewing and Clarke, 1986].
Parasympathetic dysfunction was diagnosed by applying three tests, as follows.
Heart rate (HR) response to deep breathing (HRD): Participants lay flat. After the pulse had steadied, the pulse rate was recorded during six slow, maximal deep breaths. In normal subjects, the pulse rate should fall by at least 15 beats; borderline, 11–14 beats; and with autonomic disturbances, no more than 10 beats per minute [Ewing and Clarke, 1986].
HR response to standing (HRS): The R–R interval on the ECG was recorded and used to determine the instantaneous HR at rest and then on the 15th and 30th beats after standing. The HR should normally rise after about 30 seconds as part of the response to return the blood pressure (BP) to normal. The normal 30th:15th pulse–HR ratio is at least 1.04; borderline, 1.01–1.03; and abnormal, 1.0 or below [Ewing and Clarke, 1986].
HR response to Valsalva (HRV): The test was performed by asking the subject to sit quietly and then blow into a mouthpiece attached to an aneroid pressure gauge at a pressure of 40 mmHg for 15 seconds. The ratio of the longest R–R interval shortly after the manoeuver (within about 20 beats) and the shortest R–R interval during the manoeuver is then measured. The result was expressed as the Valsalva ratio that is taken as the mean ratio from three successive Valsalva manoeuvers. In normal subjects, the Valsalva ratio is at least 1.21, and in those with autonomic disturbances, 1.20 or below [Ewing and Clarke, 1986].
Sympathetic dysfunction was assessed with two tests, as follows.
BP response to standing (BPS): Participants were asked to stand up for 3 minutes after a 10-minute resting period in a supine position. The systolic and diastolic BP (SBP and DBP) just before standing, and 3 minutes after active standing were determined, in order to define postural change in BP and to evaluate orthostatic intolerance. A fall of SBP by: less than 10 mmHg is normal; 11–29 mmHg is borderline; and more than 30 mmHg is abnormal [Ewing and Clarke, 1986].
BP response to handgrip: Patients performed three consecutive (within 5-minute resting periods) handgrip tests for 2 minutes, while beat-to-beat BP was recorded simultaneously. The absolute difference between the highest DBP during handgrip and the basal DBP just before the handgrip was noted. A DBP that is raised by at least 16 mmHg is normal; borderline is 10–15 mmHg; and abnormal is 10 mmHg or below [Ewing and Clarke, 1986].
Results of each CV reflex test are expressed as normal (0), borderline (1), or abnormal (2), as in reference values according to Ewing and Clarke [Ewing and Clarke, 1986]. Maximal possible cumulative score is 10 (i.e. if all five tests were abnormal). Autonomic neuropathy was considered with a total score no less than 4 [Aydemir et al. 2010].
Statistical analysis
Test values are reported as mean ± standard deviation. Comparisons between two categories were made using Student’s t-test for continuous variables and unpaired Student’s t-test for comparison of PsA and healthy controls. Spearman correlation analysis was used to evaluate the correlation between disease variables and indices of CAN. A p value ⩽ 0.05 was considered statistically significant. Statistical analysis was performed using the Sigmastat 3.5 for Windows 7.0.
Results
DMARD-naïve PsA patients had significantly impaired HR response to deep breath, HR response to standing and HR response to handgrip as compared with healthy controls (Table 2). None of the healthy population had CAN.
Results of cardiovascular autonomic function in patients with psoriatic arthritis and healthy controls at baseline.
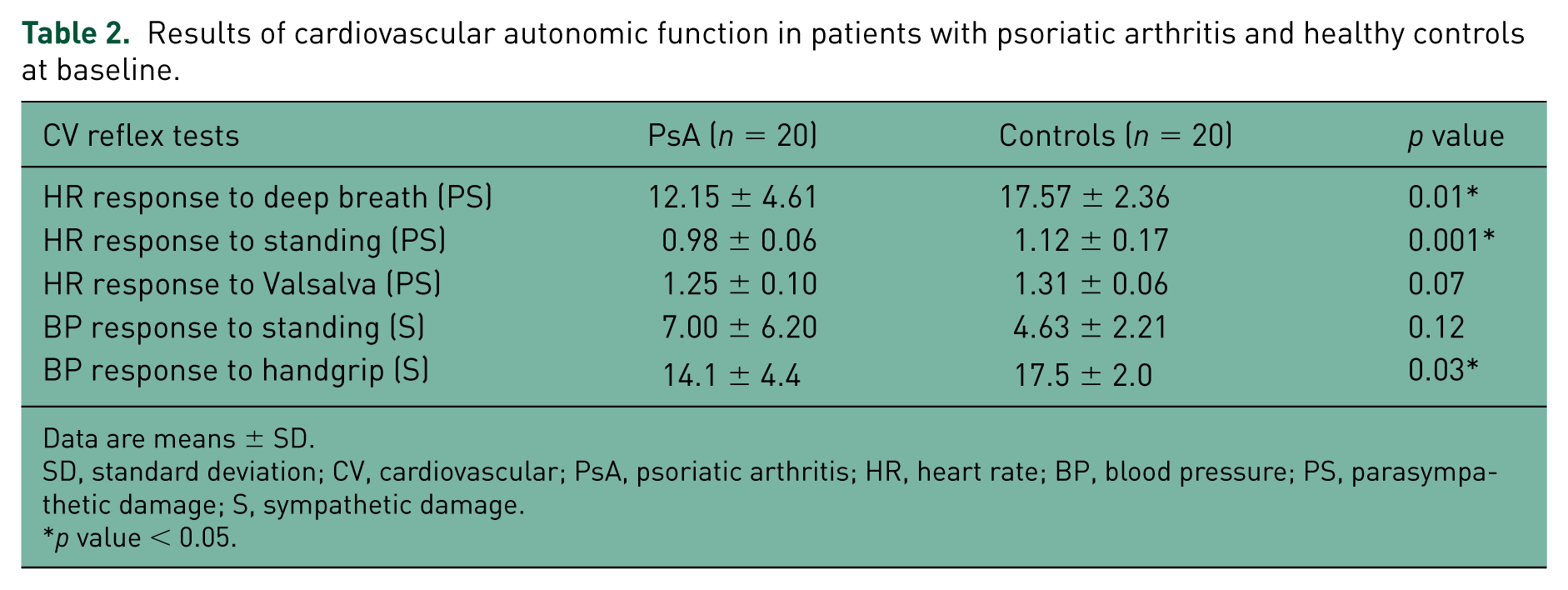
Data are means ± SD.
SD, standard deviation; CV, cardiovascular; PsA, psoriatic arthritis; HR, heart rate; BP, blood pressure; PS, parasympathetic damage; S, sympathetic damage.
p value < 0.05.
The results of cardiovascular autonomic function tests before and after treatment with synthetic DMARDs (sDMARDs) in PsA patients are shown in tables 3 and 4. After 12 weeks, treatment with sDMARDs, parasympathetic dysfunction, that is, HR response to deep breath and HR response to standing, significantly improved, while there was no improvement in sympathetic dysfunction, that is, BP response to standing and BP response to handgrip (Table 3). A total of 55% (11/20) DMARD-naïve patients had autonomic dysfunction. After treatment, 72.7% (8/11) improvement was seen in autonomic dysfunction in DMARD-naïve PsA patients. Patients with normal CV autonomic function had no change after 12 weeks’ treatment with synthetic DMARDs.
Effect of disease-modifying antirheumatic drugs on cardiovascular autonomic functions and disease variables in psoriatic-arthritis patients after 12 weeks’ treatment.

Data are means ± SD.
SD, standard deviation; CV, cardiovascular; HR, heart rate; BP, blood pressure; PS, parasympathetic damage; S, sympathetic damage; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; DAS-28, disease activity score in 28 joints; DAPSA, disease activity score in psoriatic arthritis.
p value < 0.05.
Cardiovascular autonomic status before and after treatment in patients with psoriatic arthritis.

The table shows the number of patients with psoriatic arthritis who displayed abnormal or borderline values of cardiovascular autonomic assessment according to Ewing and Clarke’s criteria [Ewing and Clarke, 1986].
BT, before treatment; AT, after treatment.
In the current study, biomarkers of inflammation, ESR (r = −0.59, p = 0.006 and r = −0.74, p = 0.001) and CRP (r = −0.64, p = 0.001 and r = −0.59, p = 0.007) significantly correlated with HR response to standing, before and after 12 weeks treatment, respectively. Disease activity, that is, DAS-28 score (r = −0.51, p = 0.03) and DAPSA (r = −0.49, p = 0.04) significantly negatively correlated with HRS and BP response to hand grip (r = −0.49, p = 0.02) significantly correlated with DAS-28 score before treatment. DAS-28 score (r = −0.52, p = 0.02) and DAPSA (r = −0.57, p = 0.009) significantly correlated with HRS after 12 weeks’ treatment with DMARDs. There was no statistically significant correlation between CV autonomic function tests with age, disease duration or BMI.
Discussion
This is the first study to investigate the clinical impact of synthetic DMARDs on CAN in PsA patients. The early diagnosis and appropriate treatment of autonomic neuropathy is important because of patients being at higher risk of morbidity and mortality, particularly if CAN is present [Boulton et al. 2005].
Our study results demonstrated significant differences in values of CV reflexes in patients with PsA compared with healthy control subjects. In the current study, parasympathetic dysfunction emerged as the predominant autonomic dysfunction in PsA. Earlier work on autonomic dysfunction in PsA and other autoimmune rheumatic diseases like RA and AS has also demonstrated predominance of parasympathetic dysfunction [Syngle et al. 2013, 2014; Stojanovich et al. 2007; Borman et al. 2008].
The efficacy of synthetic DMARDs and biologic DMARDs has been well demonstrated in RA and AS [Syngle et al. 2014]. It has been shown that biologic DMARDs improved both parasympathetic and sympathetic dysfunction to a greater extent than synthetic DMARDs in both RA and AS patients [Syngle et al. 2014]. Similarly, in the current study, treatment with synthetic DMARDs over 12 weeks has shown significant improvement in HR response to deep breath and standing suggesting improvement in parasympathetic dysfunction. However, there was no significant improvement in sympathetic dysfunction in the present study.
The exact mechanism of autonomic neuropathy still remains to be elucidated. It could result from vasculitis, amyloidosis or therapeutic side effect, circulating auto-antibodies directed against nervous structures, represented by the superior cervical ganglia and the vagus nerve [Maule et al. 1997]. A study by Altawil and colleagues demonstrated that elevated intrathecal proinflammatory cytokine interleukin-1β, reduces the vagus activity and interferes with the cholinergic neurotransmission in RA patients [Altawil et al. 2012]. The cholinergic anti-inflammatory pathway is based on the finding that vagal stimulation can reduce inflammation; however, the original theory that the vagal nerve has an inhibitory tone on the immune response has been largely disproved by Martelli and colleagues [Martelli et al. 2014] when they showed that vagotomy did not affect inflammatory responses but rather splenic sympathetic denervation did, that suggests that the sympathetic nerve has an inhibitory or modulatory effect on the immune responses. Also Bratton and colleagues found that there was no parasympathetic innervation of the spleen or synapse with sympathetic nerves [Bratton et al. 2012]. On the other hand, it has been shown that stimulation of the vagus nerve significantly inhibits tumor-necrosis-factor-α (TNF-α) release in animals [Borovikova et al. 2000]. Furthermore, experimental models studying sepsis, myocardial ischemia and pancreatitis have documented an inhibition of cytokine activity through vagus-nerve stimulation [Mioni et al. 2005; Saeed et al. 2005; van Westerloo et al. 2006]. Recently, a comprehensive review by Andersson and Tracey stated that the inflammatory reflex regulates innate and adaptive immunity via activation of the cholinergic anti-inflammatory pathway through the vagus nerves, which then drive the splenic nerves to inhibit excessive release of TNF-α [Andersson and Tracey, 2012]. A recent study by Koopman and colleagues demonstrated that stimulation of the cholinergic anti-inflammatory pathway (implantable neuromodulation device) could favourably impact clinical manifestations of systemic inflammation in RA patients [Koopman et al. 2012].
In the present study, the improvement in parasympathetic CV autonomic dysfunction in the PsA patients may have resulted from the inhibition of proinflammatory cytokines and immunological effects of synthetic DMARDs. Methotrexate has been shown to decrease secretion of interleukin-1 (IL-1) and interleukin-6 (IL-6) [Barrera et al. 1996]. Sulfasalazine has also demonstrated anti-inflammatory and immunomodulatory effects through inhibiting production of TNF-α, IL-1 and IL-6 [Smedegard and Bjork, 1995]. This hypothesis is supported by the observation that R–R-interval variability (HR variability), a marker of vagus nerve tone (that reflects parasympathetic activity), was inversely related to levels of inflammatory markers (IL-6 and CRP) in the CARDIA (the Coronary Artery Risk Development in Young Adults) study of the evolution of risk factors in young adults [Sloan et al. 2007]. A recent study by Lieb and colleagues also showed that cardiac autonomic imbalance correlates with IL-6 concentrations in newly diagnosed diabetic patients [Lieb et al. 2012]. The circulating level of TNF has been described as an independent predictor of depressed HR variability [Malave et al. 2003]. Furthermore, a recent study has demonstrated that HR variability predicts anti-TNF therapy response in RA patients [Holman and Ng, 2008]. A summarizing review by Haensel and colleagues that covered 13 studies on HR variability, inflammation, and CV function stated a strong relationship between HR variability and inflammatory markers in CV diseases [Haensel et al. 2008].
In PsA patients, disease severity (DAS-28 and DAPSA) and biomarkers of inflammation (ESR and CRP) correlated with variables of CAN before and after treatment with DMARDs. This suggests that these may predict the occurrence of neuropathy and response to treatment. Earlier study on autonomic neuropathy in PsA patients has shown a positive correlation between biomarkers of inflammation (ESR and CRP) and parasympathetic dysfunction [Syngle et al. 2013]. In another spondyloarthropathy disease, AS, there is a positive correlation between parasympathetic dysfunction and disease activity (BASDAI) and biomarkers of inflammation (ESR and CRP) [Toussirot et al. 1999].
Our study has some limitations. First, it has a small number of PsA patients. This was because of wide range of exclusion criteria present in this study that limits the number of patients. Second, this study was not designed to identify which elements of intensive DMARD therapy contributed most to the reduction in CAN. Another lacuna was our inability to determine the mechanisms of autonomic dysfunction in PsA patients. In addition, inflammation was assessed using only ESR and CRP as markers; further studies, including inflammatory cytokines are warranted.
In conclusion, parasympathetic autonomic dysfunction is more pronounced than sympathetic dysfunction in DMARD-naïve PsA patients. Synthetic DMARDs significantly improved parasympathetic dysfunction. Disease severity and biomarkers of inflammation are potential risk factors for autonomic neuropathy in PsA patients.
Footnotes
Acknowledgements
We are very grateful to University Grant Commission, New Delhi (Government of India) for providing the research fellowship [No. F.10–15/2007 (SA-I)].
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare that there is no conflict of interest.