
Abstract
Psoriatic arthritis (PsA) is a chronic inflammatory condition with articular and extra-articular manifestations: peripheral arthritis, axial disease, enthesitis, dactylitis, and skin and nail disease. It is associated with cardiovascular comorbidities. It is now recognized as a new entity, different from rheumatoid arthritis and other spondyloarthritis in terms of clinical manifestations, pathogenesis, and response to therapies. Anti-tumor necrosis factors (anti-TNFs) have demonstrated clinical efficacies exceeding that of conventional disease modifying antirheumatic drugs (DMARDs). The current treatment paradigms recommend early diagnosis and treatment, and a strategic and target orientated approach, aiming at a low disease activity status. New understanding in the immunopathogenesis of PsA has led to new treatment targets. This review addresses the evidence of current treatment for each of the domains as an aid to the clinician managing these patients in the clinic. Some new therapeutic targets are presented. We highlight the importance of development and validation in outcome measures, including that of composite scores that capture various disease domains that will facilitate future clinical trials to inform the best treatment.
Keywords
Introduction
Psoriatic arthritis (PsA) is increasingly considered a unique disease entity that is different from rheumatoid arthritis (RA) and other spondyloarthritis (SpA) in terms of clinical manifestation, pathogenesis, response to treatment and prognosis. It is a serious condition that leads to joint destruction, disability [Gladman et al. 1990] and impaired quality of life [Husted et al. 2001; Leung et al. 2008] and even increased mortality [Gladman et al. 1998]. PsA has a wide spectrum of manifestation and a variable clinical course. Apart from the skin and nails, it affects the joints, synovial sheaths of tendons, entheses, soft tissue of the digits (dactylitis) and the axial skeleton. The increased prevalence of metabolic syndrome, type 2 diabetes mellitus, obesity, hyperlipidemia, hypertension and cardiovascular disease among PsA patients is well described [Mallbris et al. 2006; Zhu et al. 2012].
Over the past decade, the management of PsA has advanced with earlier diagnosis, validation of outcome measures for different manifestations, development of target of treatment and new modalities of therapeutic agents. In this article, we highlight the progress on PsA diagnosis, outcome measures, and treatment strategies and modalities.
Classification criteria and outcome measures
Central to the assessment of effectiveness, any modality of treatment are first, whether one could identify PsA as a homogenous entity that is distinct from other conditions, and second, whether there are valid outcome measures used to quantify disease activity in the different manifestations of the disease. The most commonly used classification criteria previously, the Moll and Wright criteria, have been criticized for their ambiguity that has resulted in a wide variation in the proportion of PsA subtypes from different PsA cohorts, inclusion of different proportion of seronegative RA and insensitive in classifying patients with early PsA [Helliwell and Taylor, 2005]. In 2006, the CLASsification of Psoriatic ARthritis (CASPAR) criteria were developed from prospective clinical and radiological data in multiple centers [Taylor et al. 2006]. The CASPAR criteria are more specific and sensitive, and universally accepted. Studies have established that the CASPAR criteria can identify patients with early disease [Chandran et al. 2007; Coates et al. 2012; van den Berg et al. 2012] and different ethnicities [Leung et al. 2010].
There was a general lack of accurate and well validated instruments to measure the clinical outcomes in PsA as most of the instruments were ‘borrowed’ from other kinds of arthritis [Mease et al. 2005a; Wong et al. 2012]. The Group for Research and Assessment of Psoriasis and Psoriatic Arthritis (GRAPPA) has proposed a core set of six domains of health to be included in randomized clinical trials (RCTs) and observational studies regarding PsA: joints, skin, pain, patient global assessment, physical function, and health-related quality of life. These were endorsed by the Outcome Measures in Rheumatology (OMERACT) [Gladman et al. 2007b]. In the last decade, there has been substantial effort in validating PsA-specific outcome measures [Healy and Helliwell, 2008; McKenna et al. 2004; Wajed et al. 2014; Gossec et al. 2014], although there are heterogeneity in reporting outcomes and there is no consensus regarding areas like the number of joints to assess and instruments for dactylitis and enthesitis [Palominos et al. 2012]. International collaborative efforts have been put up to develop composite measures that capture all aspects of this complex disease with different domains into a single score that represent ‘PsA activity’ and also to serve as a responder index [Coates et al. 2014]. The concept is similar to the development of Disease Activity Score in 28 joints (DAS28) for RA. While there is no single measure that is universally accepted [Her and Kavanaugh, 2014], the field has generally accepted minimal disease activity (MDA) as a treatment target [Coates et al. 2010]. Studies have shown that 96% of subjects who achieved MDA had no radiographic progression of disease in long term [Coates and Helliwell, 2010].
Current treatment guidelines
A new strategic approach in treatment for PsA has been gaining acceptance within the field. It includes: (1) early diagnosis and treatment; (2) low disease activity state as a treatment target; (3) assessment of all domains for the many clinical manifestations of the disease; and (4) frequent measurement of disease activity and adjusting therapies (treat-to-target). The Group for Research and Assessment of Psoriasis and Psoriatric (GRAPPA) and the European League against Rheumatic Diseases (EULAR) has published recommendations for treatment [Ritchlin et al. 2009; Gossec et al. 2012]. GRAPPA suggested treatment based on the distinct organ involvement (domain), as per peripheral arthritis, skin and nail involvement, enthesitis, dactylitis and axial arthritis. EULAR used an algorithmic approach that focused mainly on peripheral arthritis and suggested considering other manifestations separately. Both emphasize the use of a strategic and target orientated approach, aiming at a low disease activity status. This approach has been supported by a multicenter open-labelled RCT in early PsA, showing better joints, skin and radiographic outcomes in the protocol-driven tight control group using MDA as a treatment target compared with standard of care at the end of 48 weeks [Coates et al. 2013].
Treatment of PsA
To reiterate the target-orientated approach, we describe the treatment options for each of the following domains: peripheral joint disease, axial disease, dactylitis, enthesitis, skin psoriasis (PsO) and nail dystrophy.
Peripheral joint disease
Non-steroidal anti-inflammatory drugs (NSAIDs)
NSAIDs are often prescribed as part of the management of PsA. The short term (4 week) improvement in tender and swollen joints was demonstrated in a small RCT [Sarzi-Puttini et al. 2001], but was not substantiated in another larger trial at 12 week [Kivitz et al. 2007]. A Cochrane systematic review suggested that NSAIDs can be used safely with methotrexate (MTX) without an increased risk of side effects [Colebatch et al. 2011].
Corticosteroids
Systemic corticosteroids are not typically recommended in the treatment of PsO and PsA, unless in discrete circumstances and not for chronic use. There is a concern of pustular psoriasis after systemic corticosteroid withdrawal, though only a few cases had been reported in the literature [Brenner et al. 2009]. The use of intra-articular corticosteroids (IACS) is mainly based on clinical experience rather than clinical trials. From a prospective observational study in 133 PsA patients with polyarthritis who received at least one IACS, clinical response was achieved in 41% of the injected joints, which were associated with the use of MTX or anti-tumor necrosis factor (anti-TNF) agents at the time of injection. Within 12 months, 25.5% of the joints relapsed [Eder et al. 2010].
Disease-modifying antirheumatic drugs
Despite the fact that disease antirheumatic drugs (DMARDs) are widely used, the evidence base for their effectiveness is not well established. A Cochrane review in 2000 revealed that only parenteral high-dose MTX and sulfasalazine (SSZ) have demonstrated published efficacy, while the high magnitude of the improvement observed in the placebo group suggested that uncontrolled trials should not be used to guide management decisions [Jones et al. 2000]. Subsequently, there were several meta-analysis of use of DAMRDs in PsA [Ravindran et al. 2008; Ash et al. 2012; Acosta Felquer et al. 2014].
Although MTX is the most commonly used DMARD in PsA, results from clinical trials are contradictory. Data from small RCTs have shown the efficacy of MTX in treatment of peripheral arthritis and PsO [Black et al. 1964; Scarpa et al. 2008; Willkens et al. 1984]. Yet in the Methotrexate in Psoriatic Arthritis (MIPA) study, where 221 patients were randomized to MTX (15 mg per week) or placebo for 6 months, there were no differences in the Psoriatic Arthritis Response Criteria (PsARC), American College of Rheumatology (ACR) response criteria or DAS28, active joint counts or erythrocyte sedimentation rate (ESR). There were significant differences only in patient and physician global assessment and mean Psoriasis Area and Severity Index (PASI) score [Kingsley et al. 2012]. The study was limited by the high dropout rates and the relatively low dose of MTX used. The use of MTX, however, is supported in a recent meta-analysis that evaluated five RCTs and eight nonrandomized observational studies [Ceponis and Kavanaugh, 2010], showing a beneficial effect of MTX in peripheral arthritis, skin and acute phase reactants. In an open-labelled trial that included 115 treatment-naïve PsA patients, MTX monotherapy was compared with MTX plus infliximab (INF). At week 16, 66.7% and 86.3% of patients receiving MTX monotherapy and MTX plus INF, respectively, achieved an ACR 20% improvement criteria (ACR20) response [Baranauskaite et al. 2012], illustrating the efficacy of MTX at least in some PsA patients. Despite the controversies, MTX remains the mainstay of treatment for PsA.
SSZ has a larger evidence base of use in PsA compared with the other DMARDs [Clegg et al. 1996]. Studies have shown an improvement in PsARC, peripheral arthritis and functional outcome in those taking SSZ compared with controls but no evidence on improvement of axial symptoms or inhibition of radiographic joint damage [Clegg et al. 1999].
The efficacy of leflunomide (LEF), an oral pyrimidine synthesis inhibitor, was evaluated in a multicenter RCT (n = 190). A significantly higher proportion of LEF-treated patients achieved the PsARC response at week 24 compared with placebo (59% versus 29.7%) [Kaltwasser et al. 2004]. In a large prospective, multinational observational study in patients with active PsA (n = 514) who initiated LEF (n = 514), 86.4% of patients achieved a PsARC response at week 24. Significant improvements were observed in tender and swollen joint counts, dactylitis, skin and nail lesions, fatigue and pain [Behrens et al. 2013]. The use of LEF in combination with MTX may be associated with elevation of liver function test that requires cautious monitoring [Curtis et al. 2010].
Anti-TNFs
Anti-TNFs given either alone or with other DMARDs have revolutionized the treatment paradigm in PsA. The clinical efficacies of anti-TNFs exceed that of conventional DMARDs in improving peripheral arthritis, axial arthritis, enthesitis, dactylitis, skin and nails [Antoni et al. 2005; Kavanaugh et al. 2006, 2007, 2009, 2012, 2013a; Mease et al. 2004, 2005b, 2006, 2009; Gladman et al. 2007a], and most importantly in inhibiting joint damage and radiographic progression [Goulabchand et al. 2014] (Table 1).
Summary of efficacies of biological DMARDs and apremilast in psoriatic arthritis (PsA).
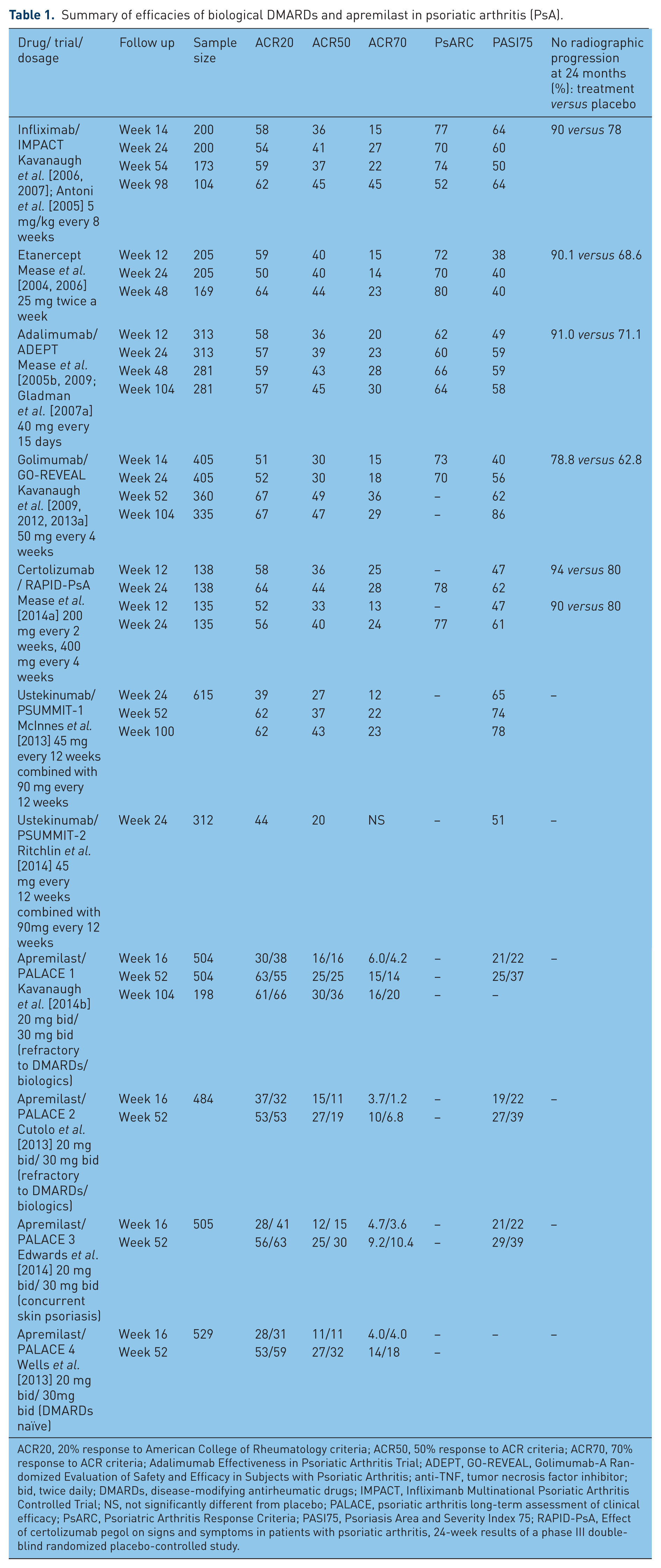
ACR20, 20% response to American College of Rheumatology criteria; ACR50, 50% response to ACR criteria; ACR70, 70% response to ACR criteria; Adalimumab Effectiveness in Psoriatic Arthritis Trial; ADEPT, GO-REVEAL, Golimumab-A Randomized Evaluation of Safety and Efficacy in Subjects with Psoriatic Arthritis; anti-TNF, tumor necrosis factor inhibitor; bid, twice daily; DMARDs, disease-modifying antirheumatic drugs; IMPACT, Infliximanb Multinational Psoriatic Arthritis Controlled Trial; NS, not significantly different from placebo; PALACE, psoriatic arthritis long-term assessment of clinical efficacy; PsARC, Psoriatric Arthritis Response Criteria; PASI75, Psoriasis Area and Severity Index 75; RAPID-PsA, Effect of certolizumab pegol on signs and symptoms in patients with psoriatic arthritis, 24-week results of a phase III double-blind randomized placebo-controlled study.
The availability of drugs that can slow down or even prevent joint damage further reinforces the importance of early diagnosis and treatment in PsA. There are five anti-TNFs that are approved by the US Food and Drug Administration (FDA) for PsA including infliximab, etanercept, adalimumab, golimumab and the new certolizumab pegol. Indirect evidence from retrospective review of data from RCTs did not suggest significant differences in efficacies and safety between anti-TNFs [Atteno et al. 2010; Thorlund et al. 2012; Fénix-Caballero et al. 2013], although there has been no head-to-head comparison. The efficacy of the newly approved certolizumab pegol has been evaluated in the RAPID-PsA study. A significant higher rate of ACR20 response at week 12 was shown in the treatment group than in placebo [Mease et al. 2014a] (Table 1). Similarly, there were better ACR50, ACR70, PsARC response rates, enthesitis, dactylitis, nail lesions and physical function in the treatment group.
Axial disease
Axial PsA is distinct from ankylosing spondylitis (AS) in many ways. These includes reduced male predominance, asymmetrical distribution of marginal and paramarginal syndesmophytes, scattered involvement along the axial skeleton (compared with predominant sacroiliitis in AS) and reduced association with the HLA-B27 allele [Scarpa et al. 1988; Helliwell et al. 1998]. Although axial PsA seem to be less symptomatic [Leung et al. 2008; Thumboo et al. 1997] and have better preservation of spinal mobility [Leung et al. 2011], recent observational data suggest that the limitation in functional capacity and quality of life is similar to AS [Pérez Alamino et al. 2011]. The health burden of axial PsA may be higher than peripheral PsA [Zhu et al. 2010; Zink et al. 2006]. Knowledge gaps exist in the current understanding of axial PsA. There is no formal effect to identify and validate the PsA axial subset, making treatments evaluation specifically for ‘axial PsA’ difficult to initiate. GRAPPA, by consensus, adopts the Assessment of SpondyloArthritis International Society (ASAS) recommendation guideline for the management of axial spondyloarthritis [van der Heijde et al. 2011]. DMARDs are in general not useful for axial PsA and evidence is in support of the use of anti-TNFs [Nash et al. 2014].
Enthesitis
Enthesitis is the inflammation at sites where tendons, ligaments and joint capsules attach to bone, and may be the origin of PsA pathogenesis [Benjamin and McGonagle, 2001]. Although local glucocorticoid injection in enthesitis is commonly used, the evidence that support its use is not well established. A systematic review and meta-analysis on controlled studies of local glucocorticoid injections in tendinopathy (not limited to PsA enthesitis) found broadly negative effects on tendon healing, weakened mechanical properties and possible long-term harm to tendon tissue, despite the short-term pain relief in a few studies [Dean et al. 2014]. Different clinical trials have used different instrument for enthesitis outcomes. Individual anti-TNF agents have shown effectiveness for enthesitis, with moderate effect sizes for golimumab [Kavanaugh et al. 2009] and certolizumab [Mease et al. 2014a] and significant improvement for infliximab [Antoni et al. 2005. Based on limited clinical trial data, ustekinumab and apremilast are also effective for enthesitis in PsA [Orbai et al. 2014].
Dactylitis
Dactylitis is the hallmark feature of PsA and is counted as an active joint. However, there is a dearth of evidence for treatment. The most commonly used therapies, NSAIDs and local corticosteroid injections, have not been formally assessed. A systematic review included 29 studies that assessed dactylitis as an outcome measure noted again the heterogeneity of outcome measures that ranges from simple count of dactylitis digits to imaging scores. There is also large variability in study design. In general, only biological agents such as ustekinumab, certolizumab and infliximab were likely to be efficacious with effect sizes ranges from 0.29 to 0.50 [Rose et al. 2014]. Looking forward, it is important to have quantifiable outcome measures (both clinical and/or imaging indexes) and assessing dactylitis as a primary outcome in trials to determine the most appropriate treatment.
PsO
Most PsA patients have PsO skin lesions. There are numerous guidelines and recommendations for skin management based on multiple clinical trials in patients with PsO [Hsu et al. 2012; Langley et al. 2012]. From observational study, the severity of PsO was associated with risk of PsA [Wilson et al. 2009; Soltani-Arabshahi et al. 2010; Haroon et al. 2013], PsA patients may have relatively mild skin disease. However, it has been observed that the mean PASI was low among reported PsA cohorts in different parts of the world [Gladman and Chandran, 2011; Leung et al. 2014a], as well as patients recruited to RCTs for biologics studies. This limits the direct extrapolation of PsO treatment results to PsA patients with skin PsO. For instance, the milder the skin PsO, the more difficult it is to use the common instruments (e.g. PASI) to detect difference or treatment response. It is also important to note PSAI and many other instruments are not developed on a metric scale, which introduce systematic bias to the studies that included patients with mild skin disease [Leung et al. 2014b]. A systematic review by GRAPPA, which included 25 studies, revealed both DMARDs (MTX, LEF, cyclosporine A) and biologics (mainly anti-TNFs) have some efficacy as therapy for skin PsO [Boehncke et al. 2014]. Looking forward, it will be important to develop appropriate outcome measures on metric scale to be used in clinical trials.
Cardiovascular comorbidities
Both PsO and PsA patients have increased cardiovascular (CV) comorbidities (type II diabetes mellitus, hyperlipidemia, hypertension, heart failure, ischemic heart disease and cerebrovascular disease), subclinical atherosclerosis, and incident CVS events [Ramonda et al. 2011; Jamnitski et al. 2013; Zhu et al. 2012]. From registry data, PsA has a higher prevalence of all the CVS comorbidities compared with PsO [Husted et al. 2011]. The systemic inflammation of PsO or PsA has been postulated to increase insulin resistance, oxidative stress and endothelial cell dysfunction, and thus the development of atherosclerosis.
Annual assessment of CVS risk using national guidelines is recommended for all patients with PsA. Any CVS risk factors identified including smoking habit, systolic blood pressure and lipid (cholesterol and high-density lipoprotein cholesterol levels) and type II diabetes should be managed appropriately. Statins, angiotensin converting enzyme inhibitors and/or angiotensin II blockers are the preferred treatment options due to their potential anti-inflammatory effects. Prescribing cyclooxygenase-2 (COX2) inhibitors and most NSAIDs in patients with a documented CV disease or in the presence of CV risk factors should be cautious. It remains controversial whether treatment of PsA with anti-TNFs may reduce atherosclerosis. In a prospective study in 32 PsA patients, there was significant progression of ultrasonographic carotid intimal thickness (IMT), which is a surrogate for CV disease, despite treatment with anti-TNF for 2 years, although beneficial effects in the arterial remodeling profiles were demonstrated (increase in serum TNF-α levels and reduction in osteoprotegerin) [Ramonda et al. 2014]. There are other studies that show treatment with anti-TNFs may reduce carotid IMT in PsA patients compared with those treated with conventional DMARDs [Tam et al. 2011; Di Minno et al. 2011]. Due to the small absolute number of CV events in studies, there is currently limited evidence to suggest systemic therapies with conventional or biological DMARDs are associated with a decrease in CV risk in PsA. It highlighted the need for larger, prospective, adequately controlled and powered studies to address the protective effect of treatment [Roubille et al. 2015; Ogdie et al. 2014]. Based on evidence established mainly in RA, EULAR has developed recommendations for CV risk management in patients with inflammatory arthritis that encompass PsA [Peters et al. 2010]. The association between inflammation and atherosclerosis in patients with inflammatory arthritis is recognized and aggressive suppression of disease activity or inflammation is recommended to lower the CV risk.
New therapeutic targets and therapies
Despite the advances in therapy for PsA with anti-TNFs, there remain many patients who fail to respond and lose efficacy over time. In recent years, there has been new understanding of the importance of the T helper 17 cells (TH17) lineage of T cells and the related cytokines, interleukin (IL) 17 and IL23 that modify the innate immunity and play major roles in immunopathogenesis of SpA. In a landmark study, Sherlock and colleagues identified a new lineage of T cells resident in the enthesis that, in response to IL23, lead to development of entheseal inflammation and local bone erosion and proliferation through a variety of effector mediators, including IL17 and IL22 (Figure 1) [Sherlock et al. 2012]. This has led to a new therapeutic target for PsA beyond anti-TNFs.

Pathogenesis of resident entheseal T cells in psoriatic arthritis.
Ustekinumab
Ustekinumab is a human monoclonal antibody (mAb) directed against the p-40 subunit of IL12 and IL23. It was approved by the FDA in 2013 for use in PsO and PsA based on two phase III multicenter, randomized, double-blind, placebo-controlled trials known as PSUMMIT I and PSUMMIT II (Table 1). In PSUMMIT I, PsA patients with no prior exposure to anti-TNFs received ustekinumab 45 and 90 mg, respectively, and 42% and 50% achieved an ACR20 response at week 24 [McInnes et al. 2013] and responses were sustained up to 108 weeks [Kavanaugh et al. 2014c]. In PSUMMIT II, which included PsA patients with prior exposure to anti-TNFs, more ustekinumab-treated (43.8% combined) than placebo-treated (20.2%) patients achieved ACR20 at week 24 and clinical responses were sustained at week 52 [Ritchlin et al. 2014]. Ustekinumab also improved dactylitis, enthesitis and skin PsO as measured by PASI75. Integrated analysis of combined radiographic data from PSUMMIT-1 and PSUMMIT-2 showed significantly inhibition of radiographic progression of joint damage ustekinumab treated patients [Kavanaugh et al. 2014d]. Ustekinumab was safe and well tolerated.
IL17 inhibitors
IL17 is produced by the unique TH17 cells and plays a key role in the pathogenesis of PsO and PsA. There are a number of IL17 inhibitors in phase III clinical trials for PsA. Secukinumab and ixekizumab are mAb against IL17A and brodalumab is a mAb against the IL17 receptor A (IL17RA). They have demonstrated significant improvement in skin PsO [Papp et al. 2013]; [Leonardi et al. 2012; Papp et al. 2012]. However, clinical response in joints is modest. A small RCT of secukinumab has shown significant improvement in physical function and C-reactive protein; however, the primary endpoint of ACR20 improvement was not achieved [McInnes et al. 2014].
Small molecules
Apremilast is an oral specific phosphodiesterase-4 (PDE-4) inhibitor that regulates inflammatory mediators. Inhibition of PDE-4 leads to increase in intracellular cyclic adenosine monophosphate (cAMP) which, in turn, reduces the expression of inflammatory cytokines such as IL12, IL23, TNF and interferon gamma (IFN-γ) and increases the expression of anti-inflammatory mediators such as IL10. Apremilast was approved by the FDA in March 2014 for the treatment of PsA based on results from four phase III RCTs, PALACE 1–4. Overall, 1493 adults patients with active PsA, with 76% and 22% who had exposure to conventional or biological DMARDs, were enrolled in PALACE 1–3 trials [Kavanaugh et al. 2014a; Cutolo, 2013; Edwards et al. 2014]. Apremilast improved signs and symptoms, physical function and skin psoriasis compared to placebo (Table 1). Pooled data from PALACE 1-3 trials demonstrated improvements in enthesitis and dactylitis [Gladman et al. 2013]. In the PALACE 4 trial, superiority of apremilast over placebo was demonstrated in DMARD naïve PsA patients, suggest that apremilast may be equally effective as monotherapy as in combination with existing DMARDs [Wells, 2013]. The most common adverse reactions reported in clinical trials were diarrhea (12.2%), nausea (10.1%), and headache (8.0%) [Kavanaugh et al. 2014a]. Rates of cardiac events, serious or opportunistic infections, malignancies or laboratory abnormalities were not increased in the apremilast-treated patients. Apremilast was associated with a small rate of weight decrease, which was not dose-dependent, and without apparent association with gastrointestinal adverse effects and any overt clinical sequelae [Mease et al. 2014b].
Conclusion
PsA is a distinct chronic multisystem inflammatory condition associated with several comorbidities and can lead to significant disability and decreased quality of life. Development and validation of classification criteria and outcome measures have facilitated clinical trials to inform treatment response in DMARDs and anti-TNFs therapies. Current treatment paradigms emphasize early diagnosis, early treatment and a strategic treat-to-target approach for the various domains of the disease. Breakthrough in the understanding of immunopathogenesis has led to novel therapies beyond anti-TNFs. Further development and validation in outcome measures, including that of composite scores that capture various disease domains, will help better define outcomes in clinical trials to inform the best treatment.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.