
Abstract
Objective:
In this case study, biomechanical alterations induced by neuromuscular taping (NMT) were quantified, during walking, in a patient with joint hypermobility syndrome/Ehlers–Danlos syndrome hypermobility type (JHS/EDS-HT).
Methods:
A female JHS/EDS-HT patient underwent NMT applications over the low back spine and bilaterally to the knee. Quantitative gait analyses were collected before the NMT application and at the end of the treatment (2 weeks after the first application of NMT).
Results:
At the end of treatment following the NMT application, left step length showed improvements in cadence and velocity, the left knee showed a reduction in its flexed position at initial contact, and the right ankle joint improved its position at initial contact and in the swing phase. Improvements were also found in kinetics, in terms of the ankle moment and power.
Conclusions:
Results show that NMT seems to be a promising low-cost intervention for improving gait strategy in patients with JHS/EDS-HT. Further investigations are needed to assess the effects of this treatment intervention on pathological symptoms.
Introduction
Joint hypermobility syndrome (JHS) is a relatively common, although largely under diagnosed, clinical entity characterized by congenital contortionism and musculoskeletal complaints [Steinmann et al. 2002]. There is significant clinical overlap between JHS and various heritable connective tissue disorders, mainly the Ehlers–Danlos syndrome(s) (EDS) [Grahame et al. 2000]. These similarities are so stringent that, recently, an international group of experts stated that JHS and EDS hypermobility type (HT) are the same clinical entity that should be distinguished from other types of EDS [Tinkle et al. 2009]. Accurate prevalence data are still lacking for JHS/EDS-HT. However, this condition seems to affect no less than 1 in 10,000 in the general population [Steinmann et al. 2002] and is dramatically more common in women [Castori et al. 2010]. The diagnosis of JHS/EDS-HT is clinical in essence as no validated genetic test is yet available [Callewaert et al. 2008]. Major features include joint hypermobility, joint complications and minor skin features (e.g. skin hyperextensibility), while the presence of additional cutaneous, vascular, skeletal and ocular symptoms moves the diagnosis towards other EDS variants. Although laxity of tendons and ligaments is considered the major determinant for musculoskeletal complaints in JHS/EDS-HT, the muscle itself seems to be frequently affected in terms of hypotonia, muscle cramps and pain, fibromyalgia, and chronic fatigue [Voermans et al. 2010]. In these patients, poor postural control and abnormal gait can be also affected by frequent orthopaedic complications involving the lower limbs [Celletti et al. 2012, 2013; Cimolin et al. 2011; Galli et al. 2011a, 2011b; Rigoldi et al. 2012, 2013; Stanitski et al. 2000]. As recently demonstrated in a qualitative scoring study, widespread involvement coupled with impaired proprioception [Hall et al. 1995; Sahin et al. 2008] contribute to posture and gait anomalies in JHS [Booshanam et al. 2011]. Proprioception refers to the sense of both static position and movement of the limbs and the body without using vision. It comprises the sense of stationary position of the limbs (limb-position sense) and the sense of limb movement (kinaesthesia). These sensations are important for controlling limb movements, manipulating objects that differ in shape and mass, and maintaining an upright posture [Kandel et al. 2000]. Lack of proprioception seems a prominent feature in JHS [Galli et al. 2011b; Sahin et al. 2008]. Although its relationship with the underlying joint hypermobility is still largely obscure, a handful of studies suggest that improvement of proprioception may be effective for ameliorating both the functional status, including balance, and chronic pain [Ferrell et al. 2004; Celletti et al. 2011]. However, as JHS is a systemic, progressive and chronic condition, physical therapy very probably suffers major treatment limitations, such as necessary intensive and lengthy treatment sessions and short-lasting effects.
Over the last 5 years in Europe, proprioceptive neuromuscular taping (NMT) technique has become a mainstream treatment protocol in postoperative, oncological, neurological care of patients and in sports medicine [Costantino et al. 2012]. This innovative taping application is based on eccentric stimulation of the skin, muscle tissue, tendons, neurological vessels, lymphatic and vascular pathways improving their functioning. Unlike other forms of taping, NMT provides passive stretching through the application, with eccentric techniques, of a tape encouraging flexibility and coordination and bettering range of movement in patients suffering with lack of muscle coordination due to different clinical conditions. It has been claimed that the effects may be due to modification of sensorimotor and proprioceptive feedback mechanisms. It has been hypothesized that the application of NMT is able to stimulate cutaneous mechanoceptors. These receptors activate nerve impulses when mechanical loads (touch, pressure, vibration, stretch and itch) create deformation. Their activation by an adequate stimulus causes local depolarization, which triggers nerve impulses along the afferent fibres travelling toward the central nervous system. The NMT technique is applied by a physiotherapist trained in eccentric taping applications. A cotton-based elastic adhesive and paper backed tape is applied in less than 15 minutes for complex multiple applications making it a nonexpensive and noninvasive treatment option well tolerated by the patients, in particular children.
Application of this technique was found in multiple sclerosis [Costantino et al. 2012] and in cerebral palsy [Camerota et al. 2013] with encouraging results on gait pattern and upper limb functionality; no applications support the use of this type of taping method to improve the lower-limb functionality in subjects with JHS/EDS-HT. The aim of this case study presentation is to use motion analysis approach to evidence, in a quantitative way, the biomechanical improvement in gait function induced by the NMT taping intervention in a patient with JHS/EDS-HT.
Case report
The participant is a woman aged 35 years and is affected by JHS/EDS-HT. JHS/EDS-HT was diagnosed by using published criteria [Beighton et al. 1998; Grahame et al. 2000]. The patient complained of chronic generalised joint pain with fatigue and reduced stamina; her main symptoms was referred to as difficulty and pain during walking - walking was limited to only a few minutes, and pain that was mainly localized in the lower back and knees. Clinical evaluation showed that the patient had a reduction of force in the lower limb muscles with knee pain during flexion and extension (numeric rating scale [NRS] pain 8/10), and passive motion reduction of the spine associated with muscular paraspinal lower back pain. No neurological deficit had been observed and no acute trauma had been referred.
The tape was applied in a particular way that characterized the NMT application with the aim to rise the skin in a wave, amplifying the stretching/contraction effect of the skin itself. NMT was applied by the same physical therapist during the study. According to the symptomatology referred by the patient, NMT was applied over the low back spine and bilaterally to the knee; the lumbar spine application (lumbar spine standard protocol treatment), consisted of two tapes of 25 cm in length and 5 cm width applied, with no tension applied to the tape, laterally to the spine from the intergluteal fold to the last dorsal vertebra with the patient maintaining a lumbar flexion at 45° in a standing position during the complete application [Blow, 2012] (Figure 1); for the knee application (functional knee standard protocol treatment), a complex combination of two strips of 25 cm in length and 2.5 cm in width along the collateral ligament using 50% tape tension applied distally to proximal, a horizontal tape below the patella 25 cm in length and 2.5 cm in width applied with 25% tension and lastly a Y tape 30 cm in length and 5 cm in width cut with 5 cm as an initial base applied laterally to the patella with no tape tension [Blow, 2012] (Figures 2 and 3). The taping was applied constantly and changed every 3 days by the same physiotherapist for a total of five applications; the patient was invited to walk normally during this period without changing her habits. No additional rehabilitative treatment was done during this period.

Taping application on low back spine.

Taping application on the right knee.

Taping application on the right knee.
The analysis consisted of a preliminary clinical examination followed by three-dimensional gait analysis (3D-GA). The analysis was conducted at the time of enrolment before the application of NMT and was repeated at the end of the treatment (2 weeks after the first application of NMT).
The 3D-GA was carried out using a 12-camera optoelectronic system (ELITE2002, BTS S.p.A., Milan, Italy) with passive markers positioned according to Davis and colleagues [Davis et al. 1991], for recording of movement evaluation, two force platforms (Kistler, CH), for movement kinetic evaluation, and a synchronic video system (BTS S.p.A., Milan, Italy). Anthropometric data were collected and passive markers were placed at anatomical landmarks. The patient walked barefoot at her self-selected and convenient speed along a 10 m walkway. At least seven trials were recorded during each session. The data were computed according to Davis and colleagues using Euler angles [Davis et al. 1991]. Some parameters were identified and calculated from kinematic and kinetic data (ankle moment and power): spatiotemporal parameters, joint-angle values at a specific instant of the gait cycle and peaks in ankle moment and power graphs (Table 1).
Gait parameters and descriptors.

The mean values (standard deviation) of kinematic and kinetic parameters are shown in detail in Table 2 in pre- and post-sessions as well for an age-matched normal (control group [CG]) [Rigoldi et al. 2012]. The control group database refers to a group of 20 subjects (age range 30-45 years) acquired with the 3DGA using the same experimental set-up described previously and using the same equipment of the same laboratory.
Gait analysis parameters of the case study and the control group (CG).
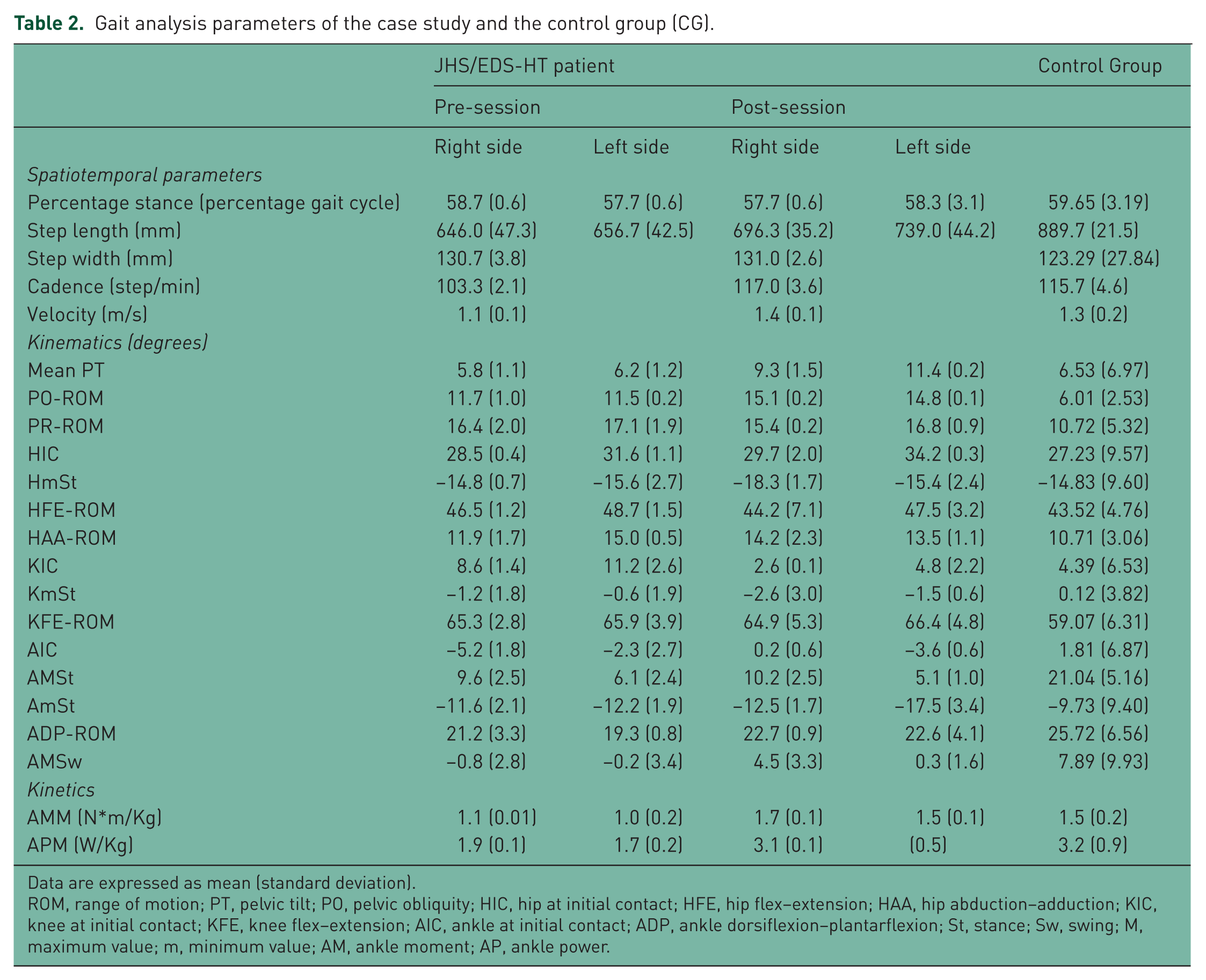
Data are expressed as mean (standard deviation).
ROM, range of motion; PT, pelvic tilt; PO, pelvic obliquity; HIC, hip at initial contact; HFE, hip flex–extension; HAA, hip abduction–adduction; KIC, knee at initial contact; KFE, knee flex–extension; AIC, ankle at initial contact; ADP, ankle dorsiflexion–plantarflexion; St, stance; Sw, swing; M, maximum value; m, minimum value; AM, ankle moment; AP, ankle power.
Before the treatment, the patient showed a limited step-length bilaterally, with low cadence and velocity in comparison with CG. In terms of kinematics, pelvic movements on the transversal (PR-ROM index) and frontal plane (PO-ROM index) were higher than in healthy subjects. The hip joint showed a physiological gait pattern. Left knee position at initial contact (KIC index) was flexed comparing with the CG. The ankle joint showed a plantar flexed position at the initial contact on the right side (AIC index), and a bilateral low dorsiflexion ability during stance (AMSt index) and swing phase (AMSw index). In terms of ankle kinetics, we observed a limited maximum of plantar flexion moment and of ankle power at the terminal stance. After NMT intervention, spatiotemporal parameters improved (left step length, cadence and velocity) reaching values closer to GC. With regards to kinematics, mean pelvic tilt increased its value towards the anterior position, remaining inside the normal range; a slight increase of ROM at pelvic rotation was observed after the intervention. The left knee improved its flexed position at initial contact and some changes were displayed at the right ankle joint, which improved its position at initial contact and in swing phase. Improvements were also found in kinetics, in particular in ankle moment and ankle power (both showed increased values). Patients reported a reduction of knee pain (NRS 3/10) and more stamina particularly during walking.
Discussion
This case report aimed to quantify the effects of NMT in the walking strategy in a patient with JHS/EDS-HT. Our results showed a general gait ability improvement when NMT was used. In particular, our data showed that, after treatment, spatiotemporal parameters improved, in particular the step length, the cadence and the velocity. Positive changes were observed in terms of kinematics, especially at ankle joint, which after NMT removal was in a more normal position and the kinetics showed an improvement in push-off ability during terminal stance. A slight worsening was observed in terms of PR-ROM. This modification, with a worsening at proximal joints and improvements at distal ones, may be due to the initiation of a new control strategy after the intervention: the modifications at distal joints, directly connected to treatment, probably induce adjustment at the pelvis.
NMT application was also shown to be effective as follows. It is noninvasive and is not a time-consuming procedure; thus, it is cost-effective while not requesting specific patient collaboration. Its hypothetical mechanism of action, if merely speculative, should be that NMT may play a role as a sensitive input that is integrated by the central nervous system and used for assisting motor program execution process known as sensorimotor integration.
It has recently has been hypothesized that taping seems to stimulate cutaneous mechanoreceptors resulting in physiological changes in the taping area [Yoshida et al. 2007]; mechanoreceptor stimulation may improve proprioceptive inputs for muscles to perform task-specific functions [Kaya Kara et al. 2014].
We cannot compare our result with other literature results because this study represents a first-case attempt to quantify NMT effects on gait improvement in a patient with JHS/EDS-HT. However, encouraging effects on gait after this kind of intervention were found in NMT applied in patients with multiple sclerosis [Costantino et al. 2012] while other taping methods were used in children with cerebral palsy [Iosa et al. 2010] and on healthy subjects [Halseth et al. 2004; Murray and Husk, 2001]. No studies to our knowledge use 3D-GA assessments to evaluate the NMT effects in patients with JHS/EDS-HT.
This case report could be considered an observational pilot study with the prospect to inform clinical practice. Further randomized controlled investigations on more subjects are certainly needed to assess effectively the effects of NMT intervention on movement and on the generalized debilitating symptoms associated with the pathology. In addition, it would be interesting to assess whether the improvements are maintained over time. The limitations of this study are related to having data only for one subject and only using the 3D-GA test. The lack of clinical scales pre- and post-treatment is a limitation of this study, which was mainly focused on the quantification of the improvement of gait walking for this subject. Pain during walking and generalized fatigue represented the major underlying symptoms for this patient. Another limit is related to the 3D-GA in that this study did not include electromyography (EMG) signal evaluation. EMG signal evaluation could be useful in the description of muscle activity modification during the gait and to better explain the observed improvements in terms of kinematics and kinetics. Future studies should also investigate NMT evaluating not only the gait characteristics but also, with the use of clinical scales, the modification of functional abilities, reduction of pain and improvements of quality-of-life issues. Nevertheless, the fact that walking strategy improved after the treatment period suggests that NMT seems to be a promising intervention for improving gait strategy in patients with JHS/EDS-HT.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement
None of the authors have any conflicts of interest to declare.