
Abstract
Objectives:
To determine the frequency and clinical associations of hypermobility spectrum disorders in a central orthopedic hospital.
Methods:
A clinical epidemiological, prospective hospital-based cross-sectional design was employed. Kuwait Ministry of Health Ethics Board approved the study (ref. no. 2022/2233). The Beighton score and the 2017 hypermobility spectrum disorders classification framework were used for screening over a 7-month period.
Results:
A total of 270 patients were examined, revealing a hypermobility spectrum disorder frequency of 21.1%; 31.7% in women and 4.7% in men. The mean age ± standard deviation was 39.4 ± 16.9 years, and 91.2% of identified cases were women. Among individuals with hypermobility spectrum disorders, 63.2% were classified as generalized hypermobility spectrum disorders, 26.3% as localized hypermobility spectrum disorders, and 10.5% as peripheral hypermobility spectrum disorders. The most frequent primary diagnosis or injury involved the knee (45.3%), hand (19.4%), and foot and ankle (19.4%). The most frequent secondary diagnosis or injury involved the knee (40.6%) and foot and ankle (28.1%). The most frequent tertiary diagnosis or injury involved the knee (50.0%) and the spine (20.0%). Management was most commonly directed toward the knee (45.7%), followed by the foot and ankle (12.7%). Statistically significant associations were identified between the Beighton score and primary diagnosis or injury (p = 0.032, r = 0.284), secondary management (p = 0.003, r = 0.516), and tertiary management (p = 0.027, r = 0.690).
Conclusion:
Hypermobility spectrum disorder was frequently observed in a central orthopedic hospital and showed significant associations with orthopedic diagnoses and management pathways, indicating a substantial clinical burden and implications for orthopedic service planning.
Introduction
Hypermobility spectrum disorders (HSD) are complex and chronic connective tissue disorders characterized by excessive mobility of the synovial joints in the absence of systemic inflammation etiologically related to genetic or pathologic factors.1,2 HSD is a diagnostic terminology introduced in 2017 to replace the previously used terminology of joint hypermobility syndrome (JHS), with the 2017 classification framework categorizing HSD into generalized, peripheral, localized, and historical.1,2 HSD are characterized by altered collagen structure and connective tissue mechanical properties, which may influence joint stability and musculoskeletal function.3–6 Consequently, HSD is considered a multisystemic disorder with a potential of wide-ranging involvement of the musculoskeletal, cardiovascular, gastrointestinal, and autonomic systems. This multisystem involvement may also affect the psychological health, and contribute to complex symptoms such as migraine headaches, fatigue, and sleep disturbances. 7 However, the symptomatic manifestations of HSD predominantly affect the musculoskeletal system, as collagen is a major constituent of the musculotendinous structures, leading to chronic joint pain, joint instability, hypermobility, and a range of secondary orthopedic and musculoskeletal injuries.1,2,8 The clinical complexity of HSD lies in its wide spectrum of severity, which may range from localized joint pain to significant functional impairment, including loss of independent ambulation and limitations in activities of daily living. 9 Importantly, identification of HSD in clinical practice, along with appropriate examination and diagnosis, is often challenging and may be overlooked by clinicians who are not hypermobility-focused, as the underlying condition can be masked by pain and the presentation of acute injuries. 9
HSD is a complex and potentially disabling condition, and establishing clinical epidemiological figures is essential for determining the clinical burden of the condition thereby directing effective management strategies. Reported prevalence rates of HSD vary across geographical regions, a variation that has traditionally been attributed to ethnic determinants; however, emerging evidence suggest that environmental exposure, occupational demands, and the clinical context in which individuals are evaluated may also play a substantial role. 3 Determining the prevalence of HSD within the general population is challenging, as most existing figures are derived from clinical cohorts, which reflect the frequent presentation of HSD within healthcare settings. 10 In adult clinical and healthcare settings, frequency estimates demonstrate marked variability. Foundational epidemiological surveys reported a frequency of 8.7% among Maori adults responding to a population-based rheumatic diseases survey. 11 Slightly higher frequency figures have been reported among adults referred to a rheumatology clinic in Northern India (9.95%) and among Nigerian undergraduate students (12.91%).11,12 In rheumatology clinic cohorts from Colombia, a frequency of 15% has been reported. 13 Notably, higher frequency rates have been highlighted in musculoskeletal care settings, including 30% among patients attending a musculoskeletal triage clinic in London. 14 Similarly, higher figures of 38.5% and 25.4% were reported among Iraqi female and male university students, respectively, presenting with musculoskeletal complains. 15 The highest frequency figures (exceeding 50%) have been reported in respondents to joint pain surveys in Nigeria and women attending physiotherapy in Oman.16,14,17 Collectively, these studies indicate that HSD is disproportionately represented in clinical musculoskeletal practice compared with the general population, highlighting the importance of context-specific clinical epidemiological investigation. 3 Despite consistent evidence of high frequency across rheumatology, physiotherapy, and musculoskeletal triage settings, no study has specifically examined the frequency of HSD with an orthopedic hospital setting, where patients frequently present with acute orthopedic injuries, advanced structural pathology, recurrent injuries, and post-operative or surgically managed conditions. This gap in clinical epidemiology of HSD directly underpins the rationale for the present study. Notably, the percentages reported are intended to describe the clinical occurrence of HSD within different clinical settings, rather than to estimate population prevalence or to enable direct comparison with epidemiological studies based on predefined Beighton score cut-offs.
Orthopedic surgery and subsequent post-surgical rehabilitation may have a detrimental impact on individuals with HSD. The musculoskeletal system is the most affected system in HSD; therefore, complex orthopedic injuries present a major clinical concern. Hypermobility has been associated with a threefold increase in shoulder injuries, a 4.45-fold increase in anterior cruciate ligament injuries injuries, and an increased risk of ankle sprains and hand osteoarthritis.18–21 Furthermore, a wide range of other conditions, including joint dislocations, sprains, recurrent soft-tissue injuries, tendon, and muscle ruptures, have also been associated with hypermobility.18–21 Establishing clinical epidemiological figures of HSD within orthopedic hospitals and determining its frequency and clinical associations would provide valuable insight into the burden of HSD in this setting, thereby informing healthcare needs assessment and resources allocation. More importantly, clinical epidemiological exploration may support improved planning and monitoring of managerial and clinical approaches within the orthopedic services. Identification of high frequency rates could prompt health authorities to implement more intensive efforts, including earlier HSD identification within orthopedic care pathways, targeted referral to specialized rehabilitation services, and informed clinical decision-making in the management of acute and surgically managed orthopedic conditions. Additionally, identifying frequency patterns and clinical associations may help guide preventive strategies, clarify trends in disease distribution, and ultimately reduce complications while optimizing management outcomes. Accordingly, the purpose of the present study is to determine the clinical epidemiological figures of HSD within a central orthopedic hospital, focusing on its frequency and associated clinical characteristics.
Methods
Design and ethics
A clinical epidemiological, prospective hospital-based cross-sectional screening research design was employed using universal sampling, since all patients presenting during the specified study period were included. 22 A clinical epidemiological research design is a well-established methodology for studying disease patterns within a defined patient cohort, which focuses on patients in a clinical setting to improve diagnosis, prognosis, and patient care.23–25
The study was conducted following approval from the Ethics Board of the Kuwait Ministry of Health (ref. no. 2022/2233), in accordance with the Declaration of Helsinki. Patient privacy and confidentiality of personal information were strictly maintained. Informed consent was formally waived by the Institutional Review Board because the data (hypermobility screening) is part of routine, mandatory institutional clinical practice and not an additional research-specific intervention. Therefore, a waiver of individual informed consent is ethically appropriate and supported by numerous international guidelines. 26
Equity, diversity, and inclusion statement
This study was conducted with a commitment to principles of equity, diversity, and inclusion. Careful consideration was given to minimizing bias, ensuring a representative sample in terms of age, gender, socioeconomic status, and background. Efforts were made to ensure equitable access to participation and to reduce barriers for underrepresented groups. All data collection processes were designed and conducted respectfully and inclusively, with transparency in communication and adherence to cultural sensitivities.
Setting, data sources, and inclusion and exclusion criteria
The central orthopedic hospital of Kuwait (Al-Razi Orthopedic Hospital) was the main research site. It is a level II trauma center and the primary national orthopedic referral hospital in Kuwait. The hospital is a specialized institution that primarily manages acute orthopedic injuries and surgically treated orthopedic conditions, rather than chronic or self-referred musculoskeletal conditions. All the patients sustaining orthopedic injuries are referred to Al-Razi Hospital Orthopedic Rehabilitation Department following recent injury or post-operative orthopedic management, whether treated conservatively (e.g. immobilization with plaster of Paris) or surgically, through referral from orthopedic surgeons. Consequently, HSD assessment was conducted during the rehabilitation phase, following recent injury or surgical intervention. The data for the present study was obtained directly from routine clinical care. The screening for joint hypermobility using the Beighton score is a mandatory, hospital-wide policy implemented for all patients referred for orthopedic rehabilitation. Hypermobility screening in not a procedure that was implemented for this study; however, it is a standard-of-care triage protocol. This institutional policy ensures early identification of patient with hypermobility and referral to the specialized hypermobility clinic for appropriate management, thereby serving as a quality assurance and patient safety measure. The data were accessed by the hypermobility clinic team who are part of the research team, and they have routine permission to access the data.
The inclusion criteria comprised all the patients referred from the orthopedic surgery department of Al-Razi Hospital to the rehabilitation department within the same institution. Patients were screened for hypermobility using the nine-point Beighton score, which is routinely included with orthopedic rehabilitation referrals to facilitate appropriate triage to Al-Razi Hypermobility Clinic when indicated. As the study employed universal sampling, no exclusion criteria were specified. According to the 2017 classification framework, generalized HSD is defined by hypermobility in five or more joints, localized HSD by hypermobility in one to fewer than five joints, and peripheral HSD by hypermobility affecting the hand and/or feet.1,2 Joint hypermobility assessment was conducted within a post-injury or post-surgery orthopedic context once patients were deemed clincally fit to commence rehabilitation. Accordingly, hypermobility was identified either at the injured joint or at joints remote from the injury site, reflecting generalized or peripheral hypermobility patterns. Localized hypermobility was categorized only when the 2017 diagnostic criteria were fulfilled, and the joint was symptomatic. In cases where acute symptoms limited range of motion assessment, the affected joint was excluded from scorning, and evaluation was based on unaffected joints. This approach minimized misclassification related to post-injury or post-surgery limitations.
Data collection
The Beighton test for joint hypermobility was used as a screening tool. This is a nine-point scoring system based on the performance of specific maneuvers, including bilateral passive thumb apposition to the forearm, bilateral passive hyperextension of the fifth metacarpophalangeal joints (>90°), bilateral active elbow hyperextension (>10°), bilateral active knee hyperextension (>10°), and the ability to flex the spine to place the palms flat on the floor with knees fully extended, as originally described by Beighton et al., and supported by subsequent clinical studies.27–30 The Beighton test is a highly reliable clinical tool, demonstrating excellent intra- and inter-rater reliability. 31 Following attachment of the Beighton screening form to all referrals to the Orthopedic Rehabilitation Department, referrals were distributed to the departmental physiotherapists for scheduling rehabilitation appointments. The Beighton score was completed by the assigned physiotherapist during the initial rehabilitation assessment. All the physiotherapists involved in data collection received standardized training in the application of the Beighton score. Data were obtained from prospectively collected hypermobility screening forms completed during routine clinical assessments between May 1, 2022, and December 31, 2022. Data were accessed by designated members of the hypermobility clinic research team who hold routine clinical authorization to access patient records. All the patients screened during this predefined period were included. The results of the Beighton score, including both positive and negative findings, were systematically recorded at the time of evaluation and monitored on an ongoing basis throughout the study period to ensure completeness and minimize missing data, permitting accurate estimation of HSD frequency within the screened cohort. Screening tests were considered positive if at least one joint demonstrated hypermobile, consistent with the localized subtype of the 2017 HSD classification framework.1,2 Consequently, Beighton scores ranging from one to nine were considered positive for screening purposes. Patients with positive screening results were referred to the Hypermobility Clinic of the Central Orthopedic Hospital through the standard referral pathway. At the Hypermobility Clinic, each diagnosis was confirmed by a hypermobility specialist using the 2017 HSD diagnostic framework.1,2 For the purpose of this study, individuals meeting diagnostic criteria for hypermobile Ehlers–Danlos syndrome (hEDS) and those classified as having HSD were considered together as a single symptomatic hypermobility cohort. The full 2017 hEDS diagnostic checklist was applied as part of the clinical evaluation. Joint hypermobility was initially screened using the Beighton score, and symptomatic hypermobility predating the index orthopedic injury was clinically verified to exclude individuals with asymptomatic generalized joint hypermobility.
According to the 2017 classification framework, generalized HSD is defined by hypermobility in five or more joints, localized HSD by hypermobility in one to fewer than five joints, and peripheral HSD by hypermobility affecting the hand and/or feet.1,2 Joint hypermobility assessment was conducted within a post-injury or post-surgery orthopedic context once patients were deemed clinically fit to commence rehabilitation. Accordingly, hypermobility was identified either at the injured joint or at joints remote from the injury site, reflecting generalized or peripheral hypermobility patterns. In cases where acute symptoms limited range of motion assessment, the affected joint was excluded from scorning, and evaluation was based on unaffected joints. This approach minimized misclassification related to post-injury or post-surgery limitations. Demographic and general clinical characteristics of the patients with confirmed HSD were recorded using a designated Excel spreadsheet, and data entry accuracy was verified three times by two researchers. Recorded demographic variables included age, gender, nationality (Kuwaiti and non-Kuwaiti), height, and weight. HSD classification outcomes (generalized, peripheral, and localized HSD) were documented. Historical HSD (five-point questionnaire) was not collected, and no age-related historical adjustment points were applied; Beighton scores were analyzed as recorded at the rehabilitation assessment using a single uniform threshold. Primary, secondary, and tertiary orthopedic diagnoses or injuries were recorded according to their chronological order of occurrence. Similarly, primary, secondary, and tertiary management approaches were recorded to reflect the sequence of care. Anesthesia and hospitalization data, as well as any missing information, were retrieved from medical records and the Hypermobility Clinic database.
Statistical analysis
Prior to statistical analysis, all identifiable data were removed, and coded dataset was generated. De-identified dataset was stored on a password-protected institutional computer. The Statistical Package for Social Sciences (SPSS) was used for datal analysis (version 23.0; IBM SPSS Statistics for Windows, Armonk, NY, USA). Normality of the data was assessed using the Shapiro–Wilk test, which demonstrated a non-normal distribution (p = 0.031). Accordingly, non-parametric statistical methods were applied. Spearman’s rank correlation coefficients were used to examine relationships between variables and explore clinical associations. The Beighton score (0–9) was analyzed as a continuous variable, reflecting the number of hypermobile joints. Primary, secondary, and tertiary diagnoses and management categories were numerically coded for analysis. Management categories reflect the type of orthopedic management. A p < 0.05 was defined as statistically significant. Frequencies were calculated for each orthopedic diagnosis or injury and for the total frequency of affected anatomical regions, including the spine, upper limbs, and lower limbs. Frequencies of orthopedic management approaches were reported according to specific procedures and by affected anatomical region of the spine, upper limbs, and lower limbs.
Results
The results showed a total referral number of 270 patients using the 2017 HSD diagnostic criteria. The overall frequency of HSD was 21.1% with 57 patients meeting the diagnostic criteria. Specifically, the frequency of HSD in women was 31.7%; of the 164 female patients screened, 52 met the diagnostic criteria. In contrast, the frequency of HSD among men was 4.7%; of the 106 male patients screened, five met the diagnostic criteria.
The demographic characteristics of patients identified with HSD included age, gender, nationality, height, and weight (Table 1). The mean age ± standard deviation was 39.4 ± 16.9 years. The majority of patients were women (91.2%) and 68.4% were Kuwaiti nationals (Table 1). Patients’ height and weight are also presented in Table 1. With respect to HSD classification, 63.2% of patients were classified as generalized HSD, 26.3% as localized HSD, and 10.5% as peripheral HSD (Table 1). The median nine-point Beighton score was 4.0 (interquartile range 3–5), with a range of 1–9. The highest positive Beighton maneuver was passive apposition of the left thumb to the forearm (58.5%), while the lowest was active right elbow hyperextension >10° (30.2%; Table 1).
Demographic characteristics, diagnostic indicators, and classification of people with HSD (n = 57).

Data were presented in mean ± standard deviation or frequency (%) as indicated. For the Beighton score data is presented in median (interquartile range). The frequencies of the Beighton score tests (1–9) show the percentages of patients who scored positive for each test.
HSD: hypermobility spectrum disorders.
The most frequent primary orthopedic diagnosis or injury among individuals with HSD involved the knee (45.3%), followed by the hand (19.4%), and the foot and ankle (19.4%; Table 2). For knee involvement, the most frequent primary diagnoses or injuries were osteoarthritis (27.7%), anterior cruciate ligament tear (8.8%), meniscal tear (7.0%), and patellar dislocation (1.8%). For the hand, the most frequent diagnoses or injuries included De Quervain’s syndrome, flexor digitorum profundus tendon injury, hand fracture, and triangular fibrocartilage complex tear, each accounting for 3.5% (Table 2). For the foot and ankle, the most frequent diagnoses or injuries were ankle fractures (10.5%) and pes planus (5.3%; Table 2). Secondary orthopedic diagnoses or injuries were identified in 32 patients, with the knee (40.6%) and foot and ankle (28.1%) being most commonly affected sites (Table 2). Tertiary orthopedic diagnoses or injuries were identified in 10 patients, occurring most frequently at the knee (50.0%), followed by the spine (20.0%; Table 2). Table 2 summarizes the distribution of primary, secondary, and tertiary orthopedic diagnoses or injuries across affected joints. In terms of primary management, 80% of the recorded patients required orthopedic surgical intervention. For secondary management, 67.7% required surgical procedures, while for tertiary management, 40% required surgical intervention.
Orthopedic diagnosis and injury of patients with hypermobility spectrum disorders.
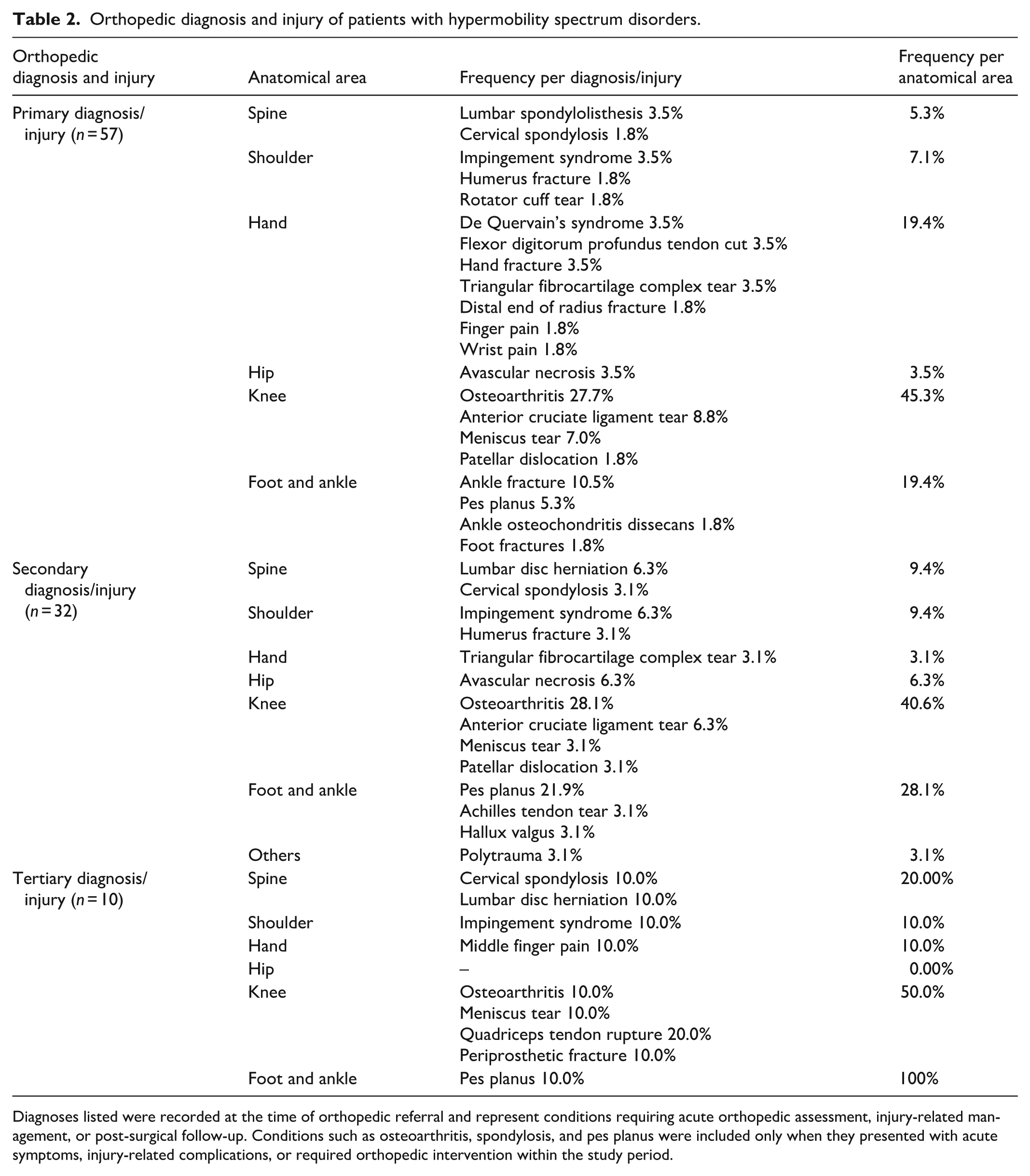
Diagnoses listed were recorded at the time of orthopedic referral and represent conditions requiring acute orthopedic assessment, injury-related management, or post-surgical follow-up. Conditions such as osteoarthritis, spondylosis, and pes planus were included only when they presented with acute symptoms, injury-related complications, or required orthopedic intervention within the study period.
Orthopedic management approaches for patients with HSD were most commonly directed toward the knee joint (45.7%), followed by the foot and ankle joints (12.7%; Table 3). With respect to knee management, total knee arthroplasty was the most frequently required intervention (20.0%), followed by anterior cruciate ligament reconstruction (10.9%), knee arthroscopy (7.5%), and meniscectomy (7.3%; Table 3). For foot and ankle, the most commonly required management approaches were open reduction and internal fixation (9.1%), accessory navicular accession, and flat feet correction, each accounting for 1.8% (Table 3). Secondary orthopedic management was reported in 31 patients and was most frequently required for the knee joint (38.7%), followed by the shoulder joint (9.7%; Table 3). Ten patients required tertiary orthopedic management, which primarily involved conservative management (60.0%) and interventions directed at the knee joint (40.0%; Table 3). Table 3 summarizes the primary, secondary, and tertiary orthopedic management approaches. Anesthesia data were available for 42 patients. Of these, 81.0% required general anesthesia, 16.7% required spinal anesthesia, and 2.4% required local anesthesia. The mean post-operative hospitalization duration was 7.9 ± 6.6 days, with a range of 1–20 days (Table 3).
Orthopedic management approaches for patients with hypermobility spectrum disorders.

Spearman’s rank correlation analysis demonstrated statistically significant associations between the Beighton score and primary orthopedic diagnosis or injury (p = 0.032 and r = 0.284), secondary orthopedic management (p = 0.003 and r = 0.516), and tertiary orthopedic management (p = 0.027 and r = 0.690). No other significant associations were identified between the Beighton score and orthopedic diagnoses, injuries, or management categories. Age was significantly associated with orthopedic diagnosis or injury and management. Statistically significant correlations were identified between age and secondary orthopedic diagnosis or injury (p = 0.019 and r = −0.413), primary management (p = 0.010 and r = −0.344), and secondary management (p = 0.001 and r = −0.648). No significant associations were identified between patient nationality and orthopedic diagnoses, injuries, or management. Patient weight was significantly associated with primary orthopedic diagnosis or injury (p = 0.010 and r = 0.455), and HSD classification was significantly associated with secondary management (p = 0.009 and r = −0.461).
Discussion
This study is the first to determine the clinical epidemiological figures of HSD in a central orthopedic hospital, examining the frequency of orthopedic diagnoses, injuries, and management pathways. The study also explored clinical associations to assess potential burdens on the health system and to inform healthcare planning and resource needs. The overall frequency of HSD was 21.1% (31.7% in women and 4.7% in men), indicating a substantial clinical occurrence within this setting. In terms of demographic characteristics, individuals identified with HSD in this orthopedic hospital cohort had a mean age of 39.4 years, reflecting the age at which patients commonly present for orthopedic services, and the condition was more frequent in women (91.2%). With regards to HSD classification, generalized HSD was the most frequent subtype (63.2%), followed by the localized HSD (26.3%) and peripheral HSD (10.5%). This clinical epidemiological study demonstrated that HSD was associated with a wide range of orthopedic diagnoses and injuries, as well as with diverse orthopedic management approaches, including surgical and conservative interventions, affecting joints throughout the body. These included the spine, upper limb joints, and lower limb joints. Importantly, higher Beighton scores were associated with greater number of primary orthopedic diagnoses and injuries, and secondary and tertiary management. Advancing age demonstrated inverse associations with secondary diagnoses and both primary and secondary management. Higher body weight was positively associated with primary orthopedic diagnosis and injury. Additionally, HSD classification was inversely associated with secondary management, indicating that patients classified with generalized HSD demonstrated higher secondary management burden compared to localized and peripheral subtypes. Collectively, these findings highlight important implications for the orthopedic community including stakeholders, decision makers, and both surgical and rehabilitation services.
This is the first clinical epidemiological study conducted within a central orthopedic hospital reporting an HSD frequency of 21.1%; therefore, direct comparison with previous studies is challenging. Nevertheless, studies from other clinical settings have reported comparable frequencies of HSD, providing contextual support for the observed findings. For example, the frequency of JHS, the diagnostic terminology used to define HSD prior to the 2017 criteria, has been reported to range from 8.7% to 15% in rheumatology practices and epidemiological surveys of rheumatic diseases.32,12,13 Furthermore, a frequency of 30% has been reported among patients attending a musculoskeletal triage clinic. 14 Within a physiotherapy setting involving patients presenting with musculoskeletal symptoms, up to 55% were diagnosed with JHS. 14 Despite differences in clinical settings and diagnostic criteria across these studies, the findings collectively indicate that HSD is commonly encountered in clinical practice. Moreover, the present study found that HSD predominantly affected women (91.2%), which is consistent with previous reports demonstrating a higher occurrence of hypermobility-related presentations among females.4,33,34
In the present study, orthopedic diagnoses and injuries were observed to involve the spine as well as upper and lower limb joints in individuals with HSD. Collagen and connective tissue mechanical alterations in HSD may affect the entire musculoskeletal system, as joints relay on collagen-based structures to provide both static and dynamic stability for efficient and safe function.3–6 Such collagen deficiency may reduce musculotendinous stiffness, whereby joint hypermobility and instability become prominent features of HSD and have been linked to orthopedic injury presentation.6,18–21,35 Moreover, several symptomatic manifestations associated with HSD may further contribute to susceptibility to orthopedic injury, including muscle weakness, proprioceptive deficit, fatigue, impaired balance, dizziness, and postural orthostatic tachycardia.7,36,37 In the present cohort, knee-related conditions were the most frequently observed orthopedic diagnoses and injuries. The finding may be explained by the biomechanical and functional demands placed on the knee joint, which is weight-bearing and relies heavily on ligamentous, tendinous, and neuromuscular structures for stability. As tissue stiffness and proprioception control may be compromised in HSD, the knee joint may be particularly vulnerable to orthopedic pathology.6,19,38 Similarly, involvement of the foot and ankle was commonly observed, which may relate to the dependence of ankle stability on ligament integrity and proprioceptive input – both of which may be altered in individuals with HSD.35,36,39 Hand-related injuries were also frequently encountered and may reflect the high functional demands placed on the hand during daily and occupational activities, in addition to its biomechanical complexity.40,41 Beyond the distribution of affected joint, a substantial proportion of patients experienced multiple orthopedic diagnoses, requiring secondary and, in some cases, tertiary orthopedic management. In addition, statistically significant associations were observed between the Beighton score and recorded orthopedic diagnoses and management approaches, suggesting that greater degrees of joint hypermobility may be clinically relevant in orthopedic presentations among individuals with HSD.
Regardless of relative frequencies, orthopedic involvement affected joints throughout the body, with a wide spectrum of injuries observed in individuals with HSD. Notably, 56.1% of patients with a primary orthopedic diagnosis or injury also sustained secondary diagnoses or injuries, and 17.5% developed tertiary orthopedic diagnoses or injuries. Consequently, a range of orthopedic management approaches was required. In terms of primary management, 80% of recorded patients required orthopedic surgical intervention, which was predominantly directed toward the knee joint (45.7%). The next highest frequencies of primary management involved the foot and ankle (12.7%) and the hand (9.0%). More than half of the patients who required primary management (54.3%) subsequently required secondary orthopedic management. Again, the knee joint demonstrated the highest frequency (38.7%). Importantly, a statistically significant association was observed between secondary management and the Beighton score, which may help explain the high proportion of patients progressing to require secondary interventions. Furthermore, 17.5% of patients who underwent primary and secondary management required a tertiary orthopedic management, which was also significantly associated with the Beighton score. This finding is consistent with the systematic review by Yeung et al., which identified ligamentous laxity as a contributing factor to post-orthopedic surgery complications, including joint dislocation rates of up to 11.1%. 42 One potential explanation for the need for multiple management stages is the abnormal healing responses in HSD as a connective tissue disorder. 43 This highlight the need for special consideration in orthopedic surgical planning and rehabilitation. For example, capsular management has been suggested as a strategy to address capsular laxity and restore adequate joint stability in individuals with hypermobility-related conditions.44,45 Accordingly, HSD should be regarded as an important clinical consideration in orthopedic practice, as the need for repeated management places a substantial burden on healthcare systems and may negatively affect patient outcomes. These considerations are also economically significant. For instance, revision of total knee arthroplasty was frequently observed as a part of tertiary management in the current study. Given that the estimated cost of each revision Total Knee Arthroplasty is ~USD 49.000, annual hospital charges of USD 2.7 billion have been reported and are projected to exceed USD 13 billion annually. 46
Clinical implications
Hypermobility was identified in the present study as a clinically relevant characteristic associated with orthopedic diagnoses, injuries, and the need for multiple orthopedic management approaches. Accordingly, recognition of hypermobility is important for orthopedic clinicians, surgeons, rehabilitation professionals, and relevant stakeholders when managing patients presenting with musculoskeletal conditions. It is therefore valuable to screen patients for hypermobility so that appropriate procedures and precautions can be tailored to individual care needs. Moreover, HSD was predominantly identified in women (91.2%), and was most frequently observed in individuals in their late thirties, reflecting the age at which patients commonly present for orthopedic care. Consequently, healthcare system efforts could be more efficiently directed toward these identified clinical associations and toward the most common diagnoses, injuries, and management pathways. HSD and other related conditions remain underrecognized, 9 despite the efforts of specialized centers, clinics, and international associations to provide targeted care and raise awareness of complex and potentially serious impact of HSD. Nevertheless, many communities, including orthopedic institutions, continue to require greater access to specialized services and awareness initiatives. Preventive strategies should also be considered to reduce the occurrence of primary diagnoses and injuries. Joint hypermobility, as a prominent symptomatic feature in HSD, may be detected from childhood through national school-based screening programs. Early identification and parental education could play a vital role in promoting strengthening programs, and appropriate long-term management. Furthermore, increasing awareness within the medical community is essential to reducing the risk of multiple injuries and complications through timely referral to specialized centers and clinics.
Limitations
The study is limited by the absence of a formal sample size power calculation. However, the use of universal sampling represents a methodological strength, as all eligible referrals within the specified study period were included, thereby minimizing selection bias and reflecting real-world clinical practice. Due to the cross-sectional design, post-operative outcomes and recurrence rates following specific surgical procedures could not be evaluated. Nevertheless, the observed requirement for secondary and tertiary orthopedic interventions highlights the ongoing clinical challenges associated with managing individuals with HSD in orthopedic settings. Recent injury or surgery may have influenced joint hypermobility assessment; however, this reflects the inherent clinical reality of research conducted within an orthopedic hospital setting. Importantly, assessments were performed during the rehabilitation phase, when acute symptoms had largely settled, allowing reliable hypermobility testing, with joint hypermobility still identified at the involved joint in most cases. Further research is required to determine the burden of HSD in relation to orthopedic surgery and rehabilitation, particularly given the invasive nature of many orthopedic procedures and the potential vulnerability of the connective tissues. Tailored rehabilitation protocols and extended healing timeframes may be necessary to ensure safe progression through rehabilitation stages. Early recognition of HSD within orthopedic hospital settings is therefore critical to optimize patient care and outcomes.
Conclusion
In conclusion, this study describes the frequency and clinical characteristics of HSD among individuals presenting to a tertiary orthopedic hospital. Musculoskeletal involvement was commonly observed across the spine, upper, and lower limb joints, with a broad range of orthopedic management approaches being documented. Within the hypermobile subgroup, higher Beighton scores demonstrated statistically significant clinical associations with multiple orthopedic diagnoses, injuries, and surgical complexity within this referral-based cohort. These findings highlight the clinical relevance of recognizing hypermobility in orthopedic practice; however, as no comparison with non-hypermobile individuals was performed, conclusion cannot be extended to the general population.
Footnotes
Ethical considerations
The Ethics Board of Kuwait Ministry of Health (ref. no. 2022/2233).
Author contributions
N.A.: study design, ethics application, data collection, statistical analysis, and writing for publication. A.A.: data collection and approving the article. B.M.: data collection and approving the article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.