
Abstract
This narrative review aims to demonstrate and summarize the complex relationship between Ehlers-Danlos syndromes (EDS) and temporomandibular disorders (TMD) by reviewing the results of observational studies and case reports. EDS are a set of hereditary connective tissue disorders, where generalized joint hypermobility (GJH), especially in the hypermobile subtype (hEDS), is a key symptom. Mutations have been identified in genes that impact the production or assembly of collagen for all subtypes except hEDS. While the correlation between GJH and TMD has been analysed in various studies, fewer studies have examined TMD in patients with EDS, with most showing an increased prevalence of TMD. In case–control studies, an elevated prevalence of myalgia, arthralgia and disc-related disorders was found in individuals with EDS. Various therapeutic interventions have been reported within the literature in the form of case reports and observational studies, but there are no long-term clinical trials with results on the efficacy of different therapeutic approaches to date. This review demonstrates the high prevalence of different TMDs in different subtypes of EDS, but also shows that little is known about the success of treatment thus far. Further clinical research is necessary to provide adequate guidance on targeted treatment.
Introduction
Ehlers-Danlos syndromes (EDS) are a group of inherited connective tissue disorders characterized by a variety of clinical manifestations ranging from skin hyperextensibility to joint hypermobility and connective tissue fragility. 1 Most of the 13 currently known subtypes have underlying defects affecting collagen production and assembly, resulting in a range of symptoms.1,2 Joint hypermobility is a central feature of a number of EDS subtypes and is associated with a range of musculoskeletal problems that extend beyond their immediate impact on mobility and function. 3 A particularly complex but often neglected problem relates to the temporomandibular joint (TMJ), where joint hypermobility and altered connective tissue can present a particular challenge in EDS patients. 4
Understanding the association between EDS and temporomandibular disorders (TMD) is crucial for enhancing the quality of life among those affected. Although there has been progress in describing the pathophysiological mechanisms underlying EDS-related joint hypermobility and pain, the precise interplay between genetic factors, collagen changes and the development of TMD remains poorly understood. 5 Nevertheless, it is now evident that the prevalence of TMD is higher among patients with EDS, particularly the hypermobile subtype (hEDS), compared with the general population. 6 The management of TMD among patients with EDS remains challenging due to the abnormal connective tissue structure and its consequences.
The purpose of this review is to conduct a thorough investigation of the existing literature on the complex association between EDS and TMD. The aim is to elucidate the possible underlying mechanisms that may contribute to TMD susceptibility, while highlighting the important diagnostic and management strategies required to address these complex challenges. This review aims to synthesize the evidence from observational studies and case reports.
Based on the existing literature, TMD among EDS has been assessed by a few studies and without considering the heterogeneity of EDS.4,7–9 However, the classification of EDS was changed considerably in 2017, and apart from hEDS, 10 other subtypes are considered as rare diseases. In the past, the different subtypes have often been studied collectively. Therefore, EDS is referred to as a whole in the following sections. However, if information concerning individual subtypes was accessible, it will be mentioned accordingly.
On 23 August 2023, a comprehensive search of the PubMed®, Scopus® and Web of Science™ databases was undertaken to examine literature relating to TMD in patients with EDS. Relevant keywords and Boolean operators that were suitable to the research question were used. The syntax was appropriately adjusted to each database. The database searches were performed in duplicate and independently by two authors (O.O. & M.C.M). Detailed information regarding the search strategies can be found in the supplementary materials (see supplementary materials, file 1). In addition, reference lists and study registries were searched and a thorough search of the grey literature was conducted to identify additional relevant sources. This review is guided by the Scale for the Assessment of narrative review articles. 11
Joint hypermobility in EDS
One of the core symptoms of EDS is joint hypermobility (JH), which is defined as excessively mobile joints that move beyond their normal range of motion.1,12 JH is most commonly measured using the Beighton Score, a simple test where each hypermobile joint or movement is given a point, resulting in a scale of 0–9.13,14 For the purpose of diagnosing generalized joint hypermobility (GJH) in EDS more reliably, the index was modified in 2017 with clear cut-off values based on different age groups. 1 The prevalence of GJH ranges from 12% to 28% in the general population, depending on age and sex, with children and women more commonly affected. 15 GJH can result in serious consequences such as joint instability and associated trauma, as well as chronic pain. 3
As early as 1988, JH was associated with the development of TMD. 16 Subsequent studies have confirmed and highlighted the relationship between JH and TMD.4,17 In a cohort study, 69% of GJH participants (formed from Marfan and EDS patients) reported myofascial pain. 4 To understand the development of TMD among patient with EDS, an understanding of the TMJ, the surrounding tissue and its function plays a key role.
The TMJ and the development of TMD
The TMJ is a complex, specialized synovial joint that facilitates crucial functions such as mastication, speech and facial expression. 18 The complicated design and mechanics of the TMJ render it susceptible to disruptions, even in individuals with structurally physiological connective tissues. However, in individuals with EDS, the intricate balance between joint stability, ligamentous support and functional mobility becomes further complicated. 19 Recurrent TMJ dislocations and subluxations are common. 3 These can cause damage to the delicate temporomandibular system, for example to the capsular ligaments and articular disc resulting in the development of TMD.20,21 Bruxism and other parafunctional habits have been proposed as factors associated with TMD among the general population. 22 Since 2014, TMD has been recommended to be diagnosed based on the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD), which provide criteria for the most common TMD disorders. 23 A taxonomic overview of TMD can be seen in Figure 1. 23
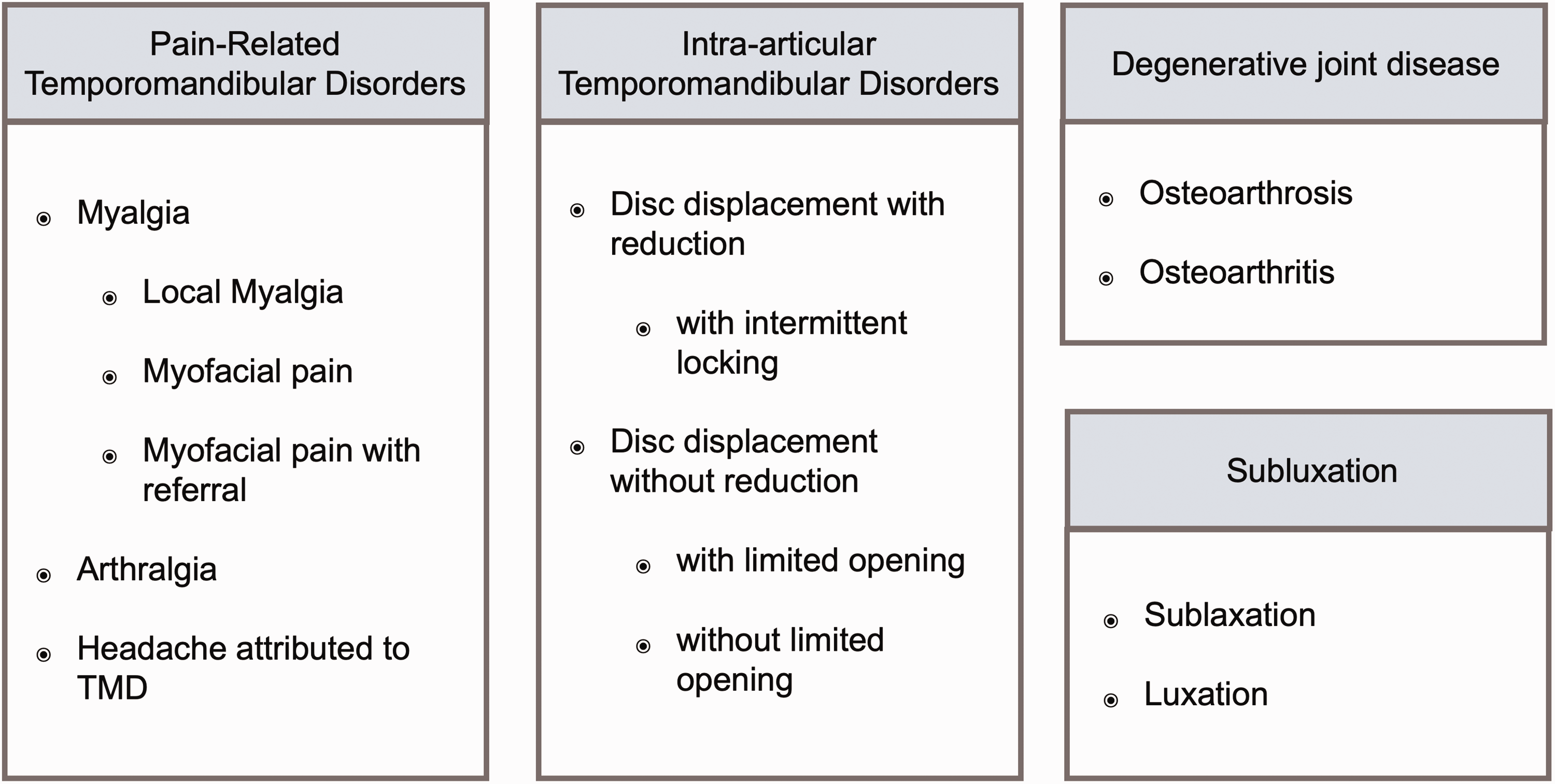
Taxonomic classification of temporomandibular disorders (TMD). 23
TMD in EDS
The preceding sections demonstrated that patients with EDS have an increased susceptibility to TMD. TMD is one of the most commonly described oral manifestations of EDS and has been described in numerous case reports. There has been interest in the research regarding TMD and EDS in recent years with a notable improvement in the quality of evidence, with the conduction of larger cohort studies and widespread dissemination of knowledge regarding TMD in EDS.
A case–control study presented a higher prevalence (myalgia: 5 versus 0; arthralgia: 5 versus 0; headache attributed to TMD: 13 versus 0) of TMD diagnoses based on DC/TMD among hEDS (n = 26) compared with the control group. 7 A recent systematic review based on 12 included studies estimated the mean prevalence of TMD manifestations in EDS patients at approximately 65% (range, 26.6–100%), with hEDS being most commonly affected. 24 Our review highlights a major shortcoming of the current literature on TMD in EDS, namely the use of a variety of methods to assess TMD. Only a small number of the studies included in our review used the currently recommended DC/TMD scheme, while others used the outdated RCD/TMD, the medical record or patient self-reporting. There is still uncertainty about the specific causes of TMD in patients with EDS. However, as demonstrated in preceding sections, GJH may be the key factor in the complex and multifactorial cause.
As the literature surrounding the various forms of TMD in EDS is diverse, this review will categorize the current literature according to the taxonomic classification and attempt to present it in a structured manner.
Myalgia, arthralgia and myofacial pain
Generally, EDS patients experience orofacial pain at a high frequency based on various case–control studies.6,7,25 In a study among hEDS (n = 14), myalgia was diagnosed in 97% while 64% were diagnosed with arthralgia. In the same study, 57% of the included hEDS patients were diagnosed with disc-related disorders, which was significantly higher in comparison with the 1.7% of non-EDS controls diagnosed with such disorders. 6 Notably, within the EDS population, there were higher occurrences of complicated cases featuring various disorders such as arthralgia, myalgia and/or disc disorders. Conversely, in the control group, isolated diagnoses from one of the aforementioned three categories were present. 6 These findings align with comparable research, which presented a higher prevalence of orofacial pain based on DC/TMD in hEDS patients compared with controls. 7 In a large case–control study, 62% of patients diagnosed with hEDS/Hypermobile Spectrum Disorder (HSD) exhibited TMJ pain. 26 They also examined possible links between fibromyalgia and hEDS/HSD by comparing the symptoms reported among patients. Intriguingly, TMD symptoms were less frequent among hEDS/HSD than in the group that was affected by fibromyalgia and hEDS/HSD (87.7%). 26
In a study of 114 women with EDS in Sweden, there was a significantly greater incidence of pain reported in the orofacial region compared with controls. 27 Another study found that 47% of EDS patients reported pain in the masticatory muscles compared with only 4% of matched controls, with 65% of EDS patients additionally experiencing hypermobility of the TMJ during mouth opening. 25
Limited data is available about other subtypes of EDS. A singular study examined TMD in 17 patients with vascular EDS (vEDS) and found a significantly higher prevalence of arthralgia in patients with vEDS compared with controls. 28
A cohort study conducted in 38 EDS patients demonstrated that 71% experienced arthralgia based on DC/TMD, with a further 92% being diagnosed with myalgia. 8 A questionnaire-based study conducted on over 250 participants with classical (cEDS) or hEDS found that 85% of respondents reported pain in their masticatory muscles. 29 Those suffering from TMD were at a 2.5-fold higher likelihood of suffering from chronic pain.
Disc-related disorders and subluxations
In addition to myalgia and arthralgia of the temporomandibular system, patients with EDS also experience disc-related disorders such as disc displacement with or without reduction and luxations or dislocations of the TMJ due to hypermobility.30–34 In a study of 38 patients with EDS, 60% were diagnosed with disc displacement with reduction according to DC/TMD, 79% had subluxations and 22% were diagnosed with degenerative joint disease. 8 A cohort of individuals diagnosed with vEDS, who were matched to healthy controls, showed a significantly higher prevalence of disc disorders, with a prevalence of 71%. 28 Radiological assessment revealed a greater proportion (44%) of early arthritic remodelling of the TMJ articulating surfaces among participants with vEDS in comparison with the control group. 28 In another sample of 18 female patients with EDS suffering from TMD, TMJ clicking and locking were observed in one-third of the cases, while seven patients experienced dislocations. 35 All patients reported pain in the TMJ area. 35
A total of 49% of patients with cEDS/hEDS reported pain or restricted movement of the jaw in a previous study. 29 In a case–control study, individuals with hEDS had reduced pain-free mouth opening and a reduced maximum opening compared with controls. 7 In contrast, a single patient diagnosed with dermatosparaxis EDS exhibited limited horizontal movements and had an increased mouth opening of more than 50 mm; 36 compared with the mean maximum mouth opening of an adult male of 44.2 mm or an adult female of 40.29 mm without EDS in the Turkish population. 37
Other contributing factors
A questionnaire-based cross-sectional study demonstrated the impact of TMD on oral health-related quality of life (OHRQoL) by comparing Oral Health Impact Profile scores of EDS patients with and without oral involvement. 38 The group affected by TMD showed significantly reduced OHRQoL. 38 Another study demonstrated similar findings on OHRQoL in patients with EDS. 39 Participants who reported experiencing pain often or very often had significantly reduced OHRQoL. 39 The results highlight the significant influence of pain on OHRQoL. 39 Another study investigating eating behaviour and disorders in EDS has suggested that TMD could be a potential co-factor that could contribute to the development of an eating disorder. 40
Treatment of TMD in EDS patients
The literature on the treatment of TMD in EDS patients is scarce. The following paragraphs present a structured overview of the currently published literature. See Figure 2 for an overview.

Conservative therapy
A case report on the treatment of a 33-year-old woman with hEDS and myalgia in the masseter region and arthralgia in the TMJ reported that she also showed subluxation of the TMJ and an excessive mouth opening of 52 mm. 41 The patient was treated using splint therapy and osteopathic therapy. 41 After 18 months of treatment, the patient reported that she no longer had pain in the TMJ and masseter region. 41 A recent study investigated the treatment outcomes of individuals with hEDS and cEDS. 42 The study found that splint therapy resulted in positive outcomes for over 50% of the participants. 42 In addition, jaw training and occlusal adjustments were found to be effective in 50% of cases each. 42 In another study, 16 of 18 patients benefitted from habit unlearning, application of heat and massage in the masticatory region and physiotherapy. 43
Minimally-invasive therapy
Arthroscopy and arthrocentesis were performed in 18 female patients with EDS and TMD who had not achieved the desired results after conservative treatment. 35 All 18 patients presented pain prior to treatment: seven trismus, seven dislocation, six clicking, six locking, two crepitation, two swelling and one bruxism. Arthroscopy was performed, arthrocentesis with saline solution was conducted, balloon dilation was implemented, and, ultimately, intra-articular morphine injections were administered. Postoperative patients were prescribed analgesics and antimicrobials or steroids as indicated. Patients were followed for a mean of 62 months and were free of symptoms at the end of follow-up. Another study performed arthrocentesis for recurrent acute TMJ locking associated with reduced mouth opening and joint pain, and follow-up was also uneventful in this case. 43
Arthroscopic discopexy was performed on a patient suffering from pain in the masticatory region and a tendency to luxation of the TMJ at extreme mouth openings. 43 The procedure significantly reduced hypermobility and pain symptoms without complications in this case.
Invasive therapy
Discectomy with reconstruction by temporalis muscle osteofascial flap and recontouring of the condyle was performed in a 40-year-old patient with recurrent anterior disc location due to posterior ligament laxity, complete disruption of the right temporomandibular joint disc in addition to significant degenerative changes of the condyle. 44 The osteofascial flap was chosen to provide bone–bone contact and evade possible soft tissue healing complications due to EDS. After a 2.5-year follow-up, the patient presented with improved symptoms and increased range of motion. A myofascial temporalis flap and recontouring of the condyle was performed on two other patients with subluxation, clicking, locking and chronic pain. 45 The patients recovered without any issues, and at the 1.5-year follow-up, they reported no recurring symptoms of TMJ.
Arthroplasty of the TMJ was performed in an 18-year-old patient with EDS and laxity in the TMJ. 46 A 1 × 1 × 1 cm cube of cryopreserved cranial bone was secured with a screw under the zygomatic arch. 46 One year after surgery, the patient experienced no complications and their oral aperture increased to 3 cm with no recurrence of dislocations.
Condylectomy was performed on an EDS patient with recurring (already 26 times) left-sided TMJ dislocation. 47 Prior attempts of conservative and minimally-invasive treatments were unsuccessful. A left-sided condylectomy at the most caudal level of the eminence was executed, and the patient underwent intermaxillary fixation for 4 weeks. At the 18-month follow-up, the patient reported no additional dislocations or symptoms. It should be noted that this procedure sparked controversy in scientific literature thereafter.48,49
Bimaxillary surgery was conducted on a 47-year-old woman with pain present in both TMJs due to hEDS. 50 Preoperative imaging showed disc displacement and degenerative joint disease. The patient was stable post-operatively, with no need for blood transfusions, and healing was uneventful. One month after surgery, the patient reported no TMJ pain and reported decreased orofacial pain during masticatory movements.
Total TMJ replacement was carried out on a female EDS patient experiencing refractory TMD symptoms that failed to improve under conservative and invasive therapy. 51 The decision to opt for total joint replacement was made in the final stages of the degenerative joint disease. A double-sided total joint replacement was performed. While the left side healed without any complications, the right side developed complications in the following years, so that the prosthesis had to be removed and replaced after healing. However, this replacement prosthesis also produced complications and was subsequently removed. Ultimately, reconstruction was achieved using a free fibular flap, which also experienced complications but did not require replacement. Despite these efforts, the patient continued to experience chronic pain. It is hypothesized that the complications on the right side were linked to the EDS and incomplete healing of the soft tissue.
Conclusion and future directions
Temporomandibular disorders are a frequent diagnosis in EDS patients. TMD compromises EDS patients with pain as well as disc and capusle related symptoms. The OHRQoL of EDS patients is generally considered to be lower compared with the general population. Treating patients with EDS and TMD is an ongoing challenge. The literature in this field is scarce. Currently, there are primarily case reports and only a few observational studies of TMD-specific therapy without long-term results. There is a lack of literature regarding the treatment, especially conservative treatment, of TMD in EDS patients. Unfortunately, only one clinical trial is currently recruiting patients for the assessment of the effectiveness of conservative treatment - TMD specific physiotherapy (ClinicalTrials.gov ID: NCT05757960). In order to provide clear treatment recommendations for this condition and to enhance the OHRQoL of affected patients, further research is required. This will also assist physicians in prescribing suitable patient-specific treatment for TMD in EDS.
Supplemental Material
sj-zip-1-imr-10.1177_03000605241242582 - Supplemental material for Temporomandibular disorders among Ehlers-Danlos syndromes: a narrative review
Supplemental material, sj-zip-1-imr-10.1177_03000605241242582 for Temporomandibular disorders among Ehlers-Danlos syndromes: a narrative review by Ole Oelerich, Linda Daume, Negin Yekkalam, Marcel Hanisch and Max C. Menne in Journal of International Medical Research
Footnotes
Acknowledgements
We thank Jan Dirk Raguse, Head of Department of Oral and Maxillofacial Surgery, Fachklinik Hornheide, for constructive criticism of the manuscript.
Author contributions
O.O., M.H. and M.C.M. conceived of the study. O.O. and M.C.M. helped in the acquisition of the existing literature. O.O., L.D., N.Y., M.H. and M.C.M. interpretated the existing literature. O.O. and M.C.M. visualized the data in the form of the figures. O.O. and M.C.M. drafted the manuscript. O.O., L.D., N.Y., M.H. and M.C.M. participated in the revision of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
O.O. received funding from the Deutsche Forschungsgemeinschaft (DFG, German Research Foundation; Project number 493624047).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.