
Abstract
Background
An ageing population and increasing chronic health disorders explain the predicted rise in hand surgeries. Preoperative care has the potential to optimise patients’ psychological and physical status, making it a promising area for enhancing surgical outcomes. Despite its established use in other surgical specialties, preoperative therapy in hand surgery remains underexplored.
Objective
This study uses an anonymous survey to gather therapists’ opinions on the hand procedure whose outcomes benefit most from preoperative therapy. The research focuses on five common elective hand procedures: Carpal Tunnel Release (CTR); Cubital Tunnel Release (CuTR); Dupuytren’s Fasciectomy (DF); Trapeziectomy (TZ); and Trigger Finger Release (TFR).
Method
British Association of Hand Therapy members were targeted in an online survey. Thirty-seven respondents (5% response rate) participated over 3 months. Questions explored how preoperative therapy improves surgical outcomes, the efficacy of postoperative therapy, and the importance of patient compliance postoperatively.
Results
TZ emerged as the procedure with the highest potential for preoperative therapy benefit, TZ and DF as top procedures for postoperative therapy requirements and importance of patient engagement and compliance. CTR had contradictory responses, while TFR and CuTR received the fewest endorsements for preoperative therapy benefits.
Conclusion
The survey offers insight into hand therapists’ perspectives on preoperative therapy. TZ and DF stand out as having significant potential for optimisation. Uncertainty surrounding efficacy of therapy on Dupuytren’s Disease indicates the necessity for further research. Education is considered an essential preoperative component. The small sample size warrants caution when interpreting results.
Introduction
Hand surgery combines the sub-specialties of orthopaedics and plastic surgery with the aim of improving or restoring hand function. The demand for specialised hand surgery has surged due to factors such as an ageing population, increasing prevalence of chronic conditions, and increased awareness of and expectations for management options in healthcare. 1 This trend is forecast to continue, with the combined operative workload for common elective hand surgeries projected to double between 2011 and 2030.1,2
Common conditions requiring surgical intervention include Dupuytren’s disease, carpal tunnel syndrome, cubital tunnel syndrome, trigger finger, and carpometacarpal osteoarthritis. Dupuytren’s disease, a fibroproliferative condition, leads to progressive digital flexion contracture. 3 Carpal and cubital tunnel syndromes, caused by nerve compression, result in pain, sensory impairment, and paresis.4,5 Trigger finger, or stenosing tenosynovitis, involves tendon sheath narrowing that restricts motion. 6 Carpometacarpal osteoarthritis, a degenerative condition affecting the first carpometacarpal joint, can result in up to 50% impairment of upper extremity function in severe cases. 7 While early stages of these conditions can be managed conservatively, they may progress or fail to respond to such interventions, and thus remain among the most common hand surgeries. 2
The role of postoperative therapy in enhancing hand surgery outcomes by reducing pain and inflammation, improving mobility and strength, and optimising functional ability is well-established and embedded in hand therapy practices. 8 However, the potential of preoperative therapy to further enhance postoperative recovery remains insufficiently explored, as evidenced by a 2024 systematic review. 9 This gap exists despite hand experts recognising the importance of addressing patients’ anxiety, pain, and expectations prior to carpal tunnel surgery, 10 and evidence supporting preoperative interventions in other surgical specialties.11,12 Key areas requiring investigation include how preoperative therapy interventions influence the need for postoperative therapy, as well as their impact on patient compliance and engagement in the recovery process.. Additionally, it is important to determine which surgeries have the highest and lowest potential to benefit from preoperative therapy, exploring the reasons behind variations and investigating any correlation between perceived benefit of preoperative therapy and postoperative therapy burden.
Preoperative hand therapy should involve a range of interventions designed to optimise a patient’s physical and psychological condition before surgery. These interventions include procedures to reduce swelling, exercise and splinting to improve range of motion and strength, 13 techniques to reduce pain, 14 information to educate and manage expectations,15–19 and strategies to alleviate anxiety. 14 These interventions aim to enhance surgical outcomes by promoting faster recovery, increasing postoperative therapy adherence and reducing postoperative complications.
Despite limited exploration in hand surgery, preoperative therapy holds significant promise for improving outcomes in this growing patient population. Addressing this research gap requires input from clinicians, whose expertise is essential in identifying which procedures are most likely to benefit from preoperative therapy interventions. This targeted approach ensures that future research efforts are strategically directed toward surgeries where preoperative therapy can have the greatest impact.
Objective
The primary aim of this survey was to gather therapists’ opinions on the potential of preoperative therapy to enhance surgical outcomes and identify which procedures stand to benefit most. This survey focuses on five common elective hand procedures: carpal tunnel release (CTR), cubital tunnel release (CuTR), Dupuytren’s fasciectomy (DF), trapeziectomy (TZ), and trigger finger release (TFR). Participants were asked to share their views on how preoperative therapy can improve surgical outcomes, the efficacy of postoperative therapy, and the role of patient engagement and compliance in achieving optimal results.
Key objectives of the survey include: (1) Assessing the potential of preoperative therapy to improve outcomes for CTR, CuTR, DF, TZ, and TFR. (2) Identifying reasons for variations in the perceived benefits of preoperative therapy. (3) Determining which surgeries have the highest and lowest potential to benefit from preoperative therapy. (4) Evaluating the need for postoperative therapy for each surgery. (5) Examining the role of patient compliance and engagement in postoperative success.
Methodology
Study design
A prospective cross-sectional online survey was conducted to gather hand therapists’ opinions on preoperative therapy (supplemental file 1). Closed and open-ended questions, developed with guidance from an academic supervisory team, and guided by established survey design principles, were used.20,21 Data analysis was conducted using a mixed-methods approach to integrate both qualitative and quantitative insights.
Ethics
Ethical approval was received from Bournemouth University’s Science, Technology and Health Research Ethics Panel in July 2023 (Ethics Identification Number 51005).
Sampling
Hand therapists were recruited using convenience sampling, This is appropriate for exploratory research to refine hypotheses and objectives. 22
Eligibility
Eligibility was determined through questions in the participant information and consent section of the survey. Participation required internet access and computer literacy.
Inclusion criteria: (1) HCPC (Health and Care Professions Council) registered physiotherapists and occupational therapists currently working as hand therapists in the United Kingdom (UK).
Exclusion criteria: (1) Previous completion of the survey
Recruitment
Recruitment was primarily through the British Association of Hand Therapists (BAHT) website and social media platforms. Additionally, face to face recruitment was carried out at BAHT 2023 annual conference.
Survey instrument
The JISC online survey system was used for survey distribution and analysis. Initially designed to gather extensive data on hand therapy practices and surgical pathways, the survey was streamlined to ensure a completion time of 10 minutes, enhancing engagement and response quality.23,24 Incentives were deemed unnecessary, as the participants were hand therapists with a vested interest in outcomes. To boost response rates, presentations and an online flyer with a survey link were distributed to targeted BAHT groups.
Data collection and analysis
Retrospective data collection was carried out through the JISC online survey tool, allowing data to be gathered from across the UK, where protocols and clinical pathways vary. The survey was open from 30th September 2023 to 31st December 2023.
Quantitative data from closed questions were analysed using descriptive statistics with frequencies and percentages calculated. Participants rated ranking questions from one to five, with one being the most favourable. Ensuring clarity in interpreting rankings, scores were transformed by subtracting the reported score from six, so that a higher mean score indicated a more favourable ranking for preoperative therapy benefit, postoperative therapy input, and patient compliance. Qualitative data from open-ended questions were analysed using manual content analysis. The first author (TBM) familiarised themselves with the data by reviewing responses multiple times. An inductive coding approach was adopted, allowing themes and categories to emerge directly from the data. The first and second authors (TBM and CC) grouped codes into broader categories based on similarities, which formed the basis for identifying overarching themes aligned with the study’s objectives.
Results
Participants
A total of 38 hand therapists started the online survey and 37 completed. This equates to approximately 5% of BAHT members at the time of the study. 25 Data presented was for fully completed surveys. All respondents were currently practising hand therapists with HCPC registration.
Participant characteristics.
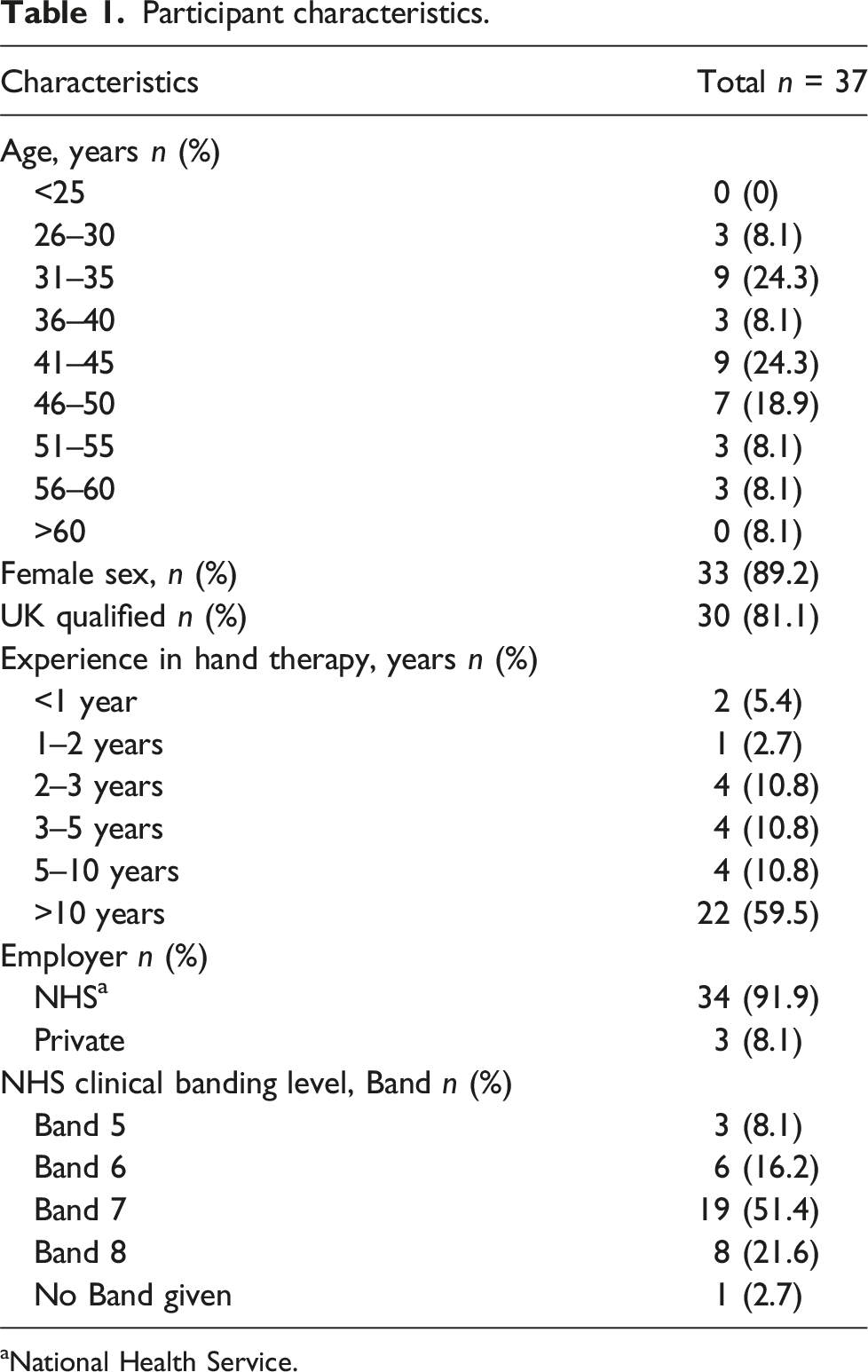
aNational Health Service.
Perceived benefit of a preoperative therapy intervention
Responses to the question of whether there is a perceived benefit for a preoperative therapy intervention for each surgical procedure.
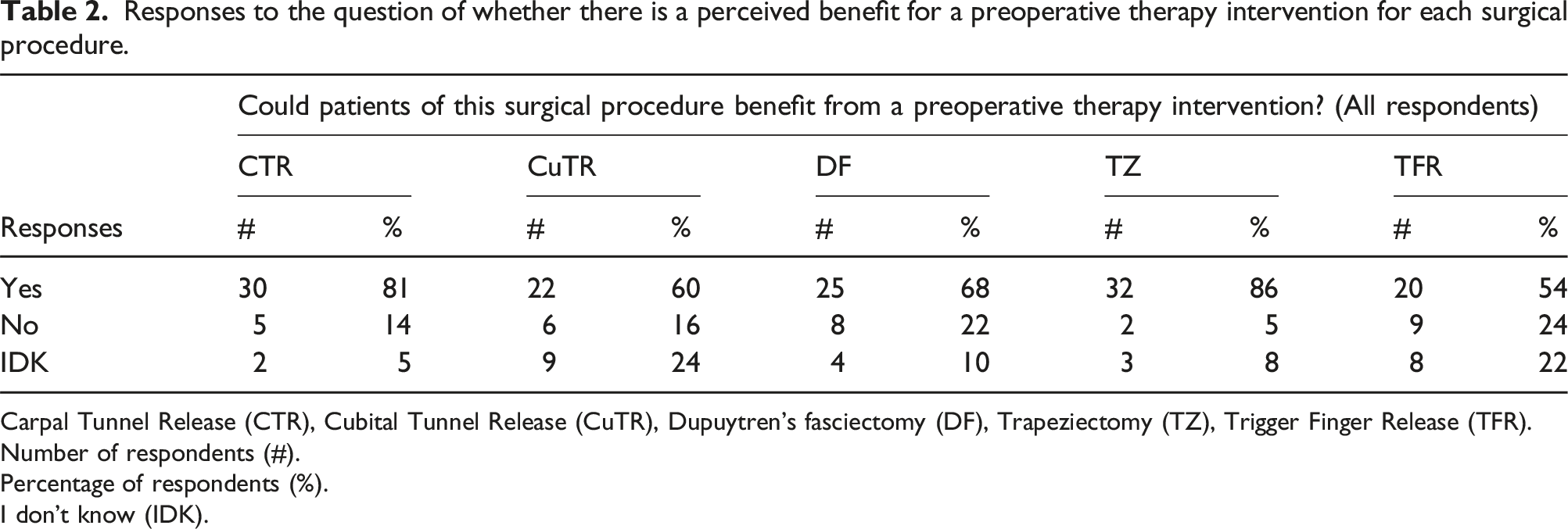
Carpal Tunnel Release (CTR), Cubital Tunnel Release (CuTR), Dupuytren’s fasciectomy (DF), Trapeziectomy (TZ), Trigger Finger Release (TFR).
Number of respondents (#).
Percentage of respondents (%).
I don’t know (IDK).
For all procedures, preoperative education, information, and expectation setting were identified as the primary reasons for anticipated benefits, with responses as follows: DF (68%), TZ (65%), CuTR (64%), CTR (60%), and TFR (35%). Exercise, splinting, and acquisition of baseline measurements were amongst other reasons cited.
TFR and DF received the highest proportion of responses indicating preoperative therapy provides no benefit (TFR 24%; DF 22%), while TZ had the lowest (5%). In cases where therapists reported no benefit, explanations typically referenced lack of evidence, low complication rates, or belief that a simple leaflet would suffice for preoperative information.
Greatest uncertainty about the value of preoperative therapy was noted for CuTR (24%), followed by TFR (22%), DF (11%), TZ (8%), and CTR (3%), with most responses offering no explanation.
Ranking of surgical procedures
The procedure that would benefit most from a preoperative therapy intervention
Responses to the ranking questions.
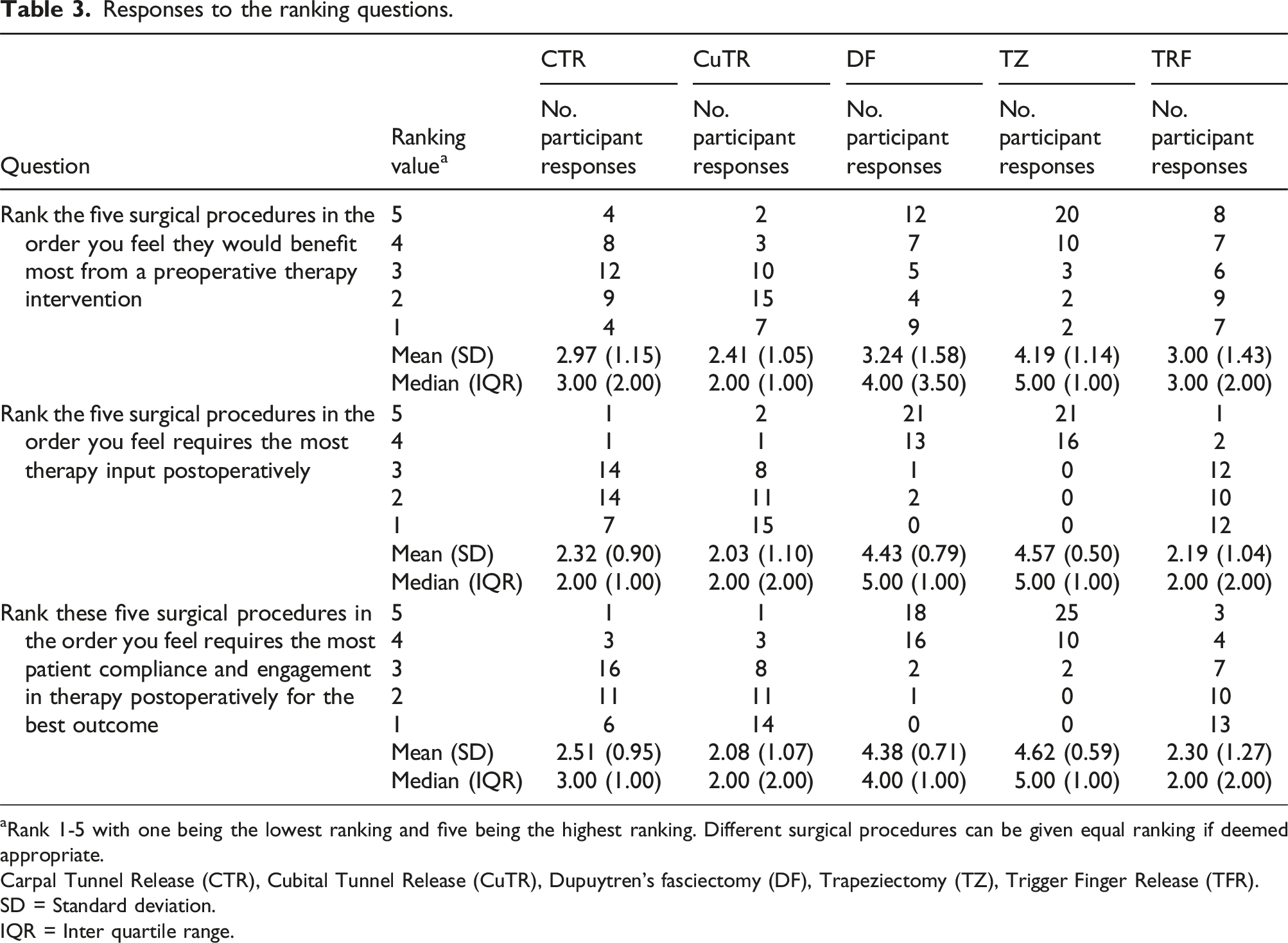
aRank 1-5 with one being the lowest ranking and five being the highest ranking. Different surgical procedures can be given equal ranking if deemed appropriate.
Carpal Tunnel Release (CTR), Cubital Tunnel Release (CuTR), Dupuytren’s fasciectomy (DF), Trapeziectomy (TZ), Trigger Finger Release (TFR).
SD = Standard deviation.
IQR = Inter quartile range.
The procedure that requires the most therapy intervention postoperatively
Ranking procedures based on level of postoperative therapy requirements, TZ and DF were ranked highest, with mean scores of 4.57 (SD = 0.50) and 4.43 (SD = 0.79) respectively. In contrast, CTR, TFR, and CuTR received lower rankings, with scores of 2.32 (SD = 0.90), 2.19 (SD = 1.04), and 2.03 (SD = 1.10) respectively (Table 3).
The procedure that requires the most compliance and engagement postoperatively
In terms of postoperative patient compliance and engagement, TZ and DF ranked highest with mean scores of 4.62 (SD = 0.59) and 4.38 (SD = 0.71) respectively. The remaining three surgeries scored significantly lower, with CTR at 2.51 (SD = 0.95), TFR at 2.30 (SD = 1.27), and CuTR at 2.08 (SD = 1.07) (Table 3).
Discussion
The primary aim of this survey was to determine which hand procedure would benefit most from a preoperative therapy intervention to enhance surgical outcomes among five prioritised procedures. Results indicated that preoperative interventions could enhance outcomes for all surgeries, with the most recommended interventions centring on education, information dissemination, and expectation setting, followed by exercise, splinting, and the acquisition of baseline measurements. This aligns with the limited research on preoperative interventions in hand surgery, where the focus has mainly been on education and expectation management. 9
Of the 37 respondents, the majority possessed over 10 years’ experience in hand therapy and held a clinical banding of seven or higher. This highlights the advanced expertise of the participants, whose input is informed by extensive clinical practice and a comprehensive understanding of hand therapy interventions. While response numbers are low, the insight provided by these experienced professionals adds significant value to the study and helps ensure the findings are grounded in practical, real-world expertise.
Information, education, and expectation setting were consistently identified as the most beneficial preoperative interventions across all five procedures. TZ was noted for its higher potential benefit from preoperative exercise, while DF favoured preoperative splinting. These variations highlight the need to tailor preoperative strategies for each procedure.
Trapeziectomy emerged as the procedure most likely to benefit from preoperative therapy intervention, and it ranked highest for both postoperative therapy requirements and patient compliance and engagement. Interestingly, this finding stands in contrast to the majority of existing research exploring the effect of preoperative therapy in hand surgery, which has primarily focused on carpal tunnel release. 9 Given the established importance of optimising physiological, physical, and mental status prior to surgery, 26 it follows that procedures requiring more postoperative therapy and patient compliance have the most to gain from preoperative intervention.
Conversely, TFR and CuTR ranked lowest in terms of postoperative therapy needs and patient engagement, as well as ranking lowest for perceived benefits of preoperative therapy intervention. TFR had the highest number of responses suggesting no benefit from preoperative therapy intervention. This suggests that procedures with less postoperative burden require less preoperative input.
However, not all procedures align with the same rationale. Despite ranking closely to TZ for postoperative therapy and patient compliance, DF ranked second to TFR in responses indicating no benefit from preoperative therapy. This inconsistency may be linked to the National Institute of Health and Care Excellence (NICE) Clinical Knowledge Summaries, which guide healthcare professionals on managing Dupuytren’s Disease. The 2022 update advises surgical intervention only for patients with contracture or significant loss of function, while excluding conservative management at any stage of the condition due to limited evidence of its efficacy.27,28 This may contribute to the perception that if therapy is seen as ineffective in conservative management, it is unlikely to be effective as a preoperative intervention.
Survey responses for CTR also showed some contradictions. While CTR scored higher than DF in perceived benefit from preoperative therapy, it ranked lower when participants were asked which procedure would benefit most from such therapy. These discrepancies can perhaps be explained thus. The initial positive responses may reflect respondents’ general belief in the value of conservative therapy for Carpal Tunnel Syndrome, supported by NICE clinical guidelines that recommend a conservative treatment pathway for mild to moderate cases. 29 Familiarity with these guidelines likely influenced the higher positive response. However, when asked to rank procedures based on perceived preoperative therapy benefits, respondents likely considered factors such as surgical complexity, expected postoperative challenges, and the significance of postoperative therapy adherence for optimal outcomes. This more nuanced analysis led respondents to recognise that DF, with its more demanding postoperative rehabilitation, may stand to benefit more from preoperative therapy thus altering the perceived hierarchy of benefit during the ranking exercise.
For ranking questions evaluating the need for postoperative therapy and patient compliance, TZ and DF emerged as the procedures requiring the most. Both also ranked highest in perceived benefit from preoperative therapy, although DF’s position is less definitive. This uncertainty is highlighted by the moderate number of positive (67.5%), and the second-highest number of negative responses regarding the potential benefit of preoperative therapy. This ambiguity may be attributed to the absence of conservative therapy treatment for Dupuytren’s Disease, as outlined by NICE guidelines. Although the question does not refer to conservative management but rather preoperative management, the nuanced distinction, crucial as it is, has likely proved challenging, despite a detailed description of terms in the survey introduction and information section. This section was densely worded, which may have limited the clarity and emphasis of this distinction. Given the importance of accurately distinguishing between preoperative and conservative management for interpreting the survey questions, including a clearer and more prominent definition directly within the survey questions could have reduced confusion and improved the accuracy of responses.
To address the primary aim of this survey several key objectives were explored, though not all were fully resolved:
Assessing the potential of preoperative therapy to improve outcomes
Results showed general agreement that all five surgeries could benefit from preoperative therapy interventions, with education, information dissemination, and expectation setting consistently recommended across procedures. However, the perceived degree of benefit varied significantly. Education, in particular, holds potential to shape patient expectations, which could lead to improved satisfaction and adherence to postoperative therapy, ultimately enhancing surgical outcomes.
Identifying reasons for variations in perceived benefits
The survey results suggest that procedures with lower postoperative burdens are perceived as less likely to benefit from preoperative therapy, potentially explaining surgery-dependent variations in the perceived value of such interventions. However, approximately 60% of responses indicating no benefit to preoperative therapy provided no explanation, making it challenging to reliably interpret the reasons behind these differences. Further exploration is needed to understand the underlying rationale for these perceptions.
Determining surgeries with the highest and lowest potential for benefit
The ranking questions highlight TZ and DF as the procedure with the most potential to benefit from preoperative therapy, and CuTR as the least. However, these rankings do not fully align with responses to the non-ranking question on preoperative therapy benefits. While TZ consistently ranks highest, the positions of the other four procedures vary. This discrepancy underscores the complexity of the data and suggests factors like surgical complexity, postoperative burden, or therapist experiences may shape these perceptions. Further investigation is needed to clarify these inconsistencies.
Evaluating the need for postoperative therapy and the role of patient compliance and engagement
Ranking questions indicate that TZ and DF require the most postoperative therapy and patient commitment, while CuTR and TFR require the least. If preoperative therapy can enhance postoperative compliance and engagement, TZ and DF are likely to benefit the most. This highlights the value of focusing preoperative therapies on surgeries with higher postoperative demands, where improved engagement could have the greatest impact on outcomes.
Limitations
A major limitation of this study is the small sample size, with only 37 participants recruited over a 90-day period, despite targeted strategies such as outreach initiatives, conference presentations, and engagements at advanced clinical practitioner meetings. Thus, the findings may not reflect opinions of the majority of UK practising hand therapists. While response rates align with a survey of BAHT members in 2016, 30 more recent survey publications suggest this constitutes a relatively low response rate. 31 This may be partly due to preoperative therapy not being common practice in hand therapy, leading some clinicians to perceive limited relevance or benefit. Additionally, the timing of the survey launch coincided with the release of two other surveys at the same conference, which may have contributed to survey fatigue among attendees.
The absence of incentives for participation assumed that practicing hand therapists would have a vested interest in study outcomes. Low response rate suggests this assumption may not have fully addressed all factors influencing participation. Future studies might consider incentives or alternative strategies to improve response rates and enhance generalisability.
Thematic analysis of responses to the question of whether there is a perceived benefit from a preoperative therapy intervention for each surgical procedure.
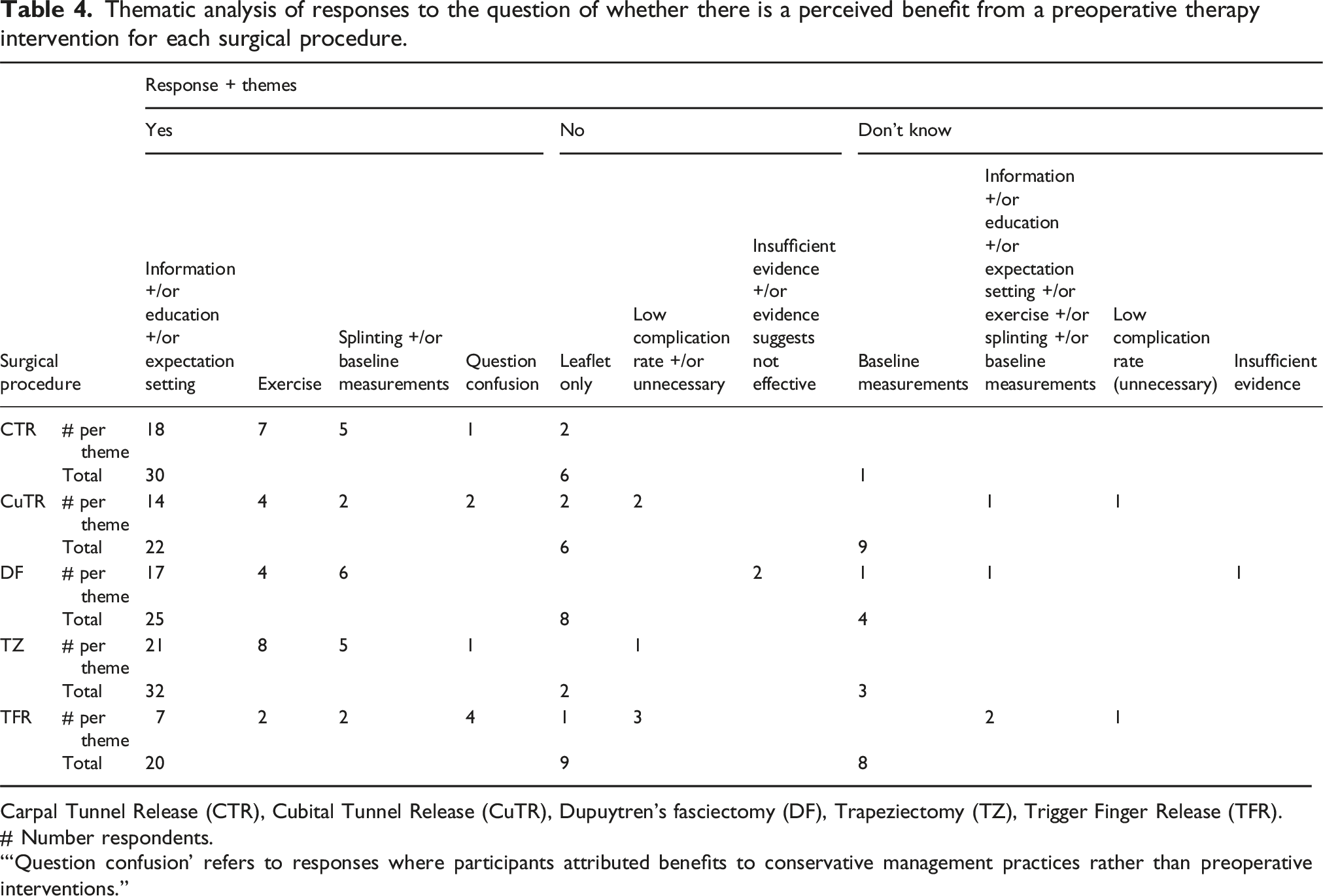
Carpal Tunnel Release (CTR), Cubital Tunnel Release (CuTR), Dupuytren’s fasciectomy (DF), Trapeziectomy (TZ), Trigger Finger Release (TFR).
# Number respondents.
“‘Question confusion’ refers to responses where participants attributed benefits to conservative management practices rather than preoperative interventions.”
Given these challenges, future research would benefit from pre-testing and refining the survey to ensure more accurate responses. One should also critically assess the suitability of surveys for addressing nuanced and opinion-driven research questions. Context plays a crucial role in understanding participants’ perspectives on the treatment of specific conditions, yet this is often missed in surveys. While survey responses are valuable, they may not fully capture the richness of participants' opinions, especially in meaningful numbers.
As such, caution is warranted when interpreting the results of this study. Nevertheless, the findings suggest a role for preoperative hand therapy, particularly education, in reducing postoperative pain and complications. Given the established benefits of preoperative therapy in other surgical specialties, further research is needed to assess its impact on recovery in hand surgery.
Conclusion
This survey aimed to identify the hand surgery most likely to benefit from preoperative therapy interventions to improve surgical outcomes. The findings carry clinical significance, particularly as they reflect the insights of therapists uniquely positioned to assess the value of such interventions. To our knowledge, therapists’ opinions have not been sought on this matter previously, making these clinical messages particularly poignant.
Responses from experienced therapists highlight the perceived value of preoperative therapy among clinicians with extensive expertise. Despite low response rates this highlights the relevance and credibility of the survey findings.
TZ and DF emerged as the procedures most likely to benefit from preoperative therapy interventions, though responses for DF showed greater variability. TFR and CuTR were viewed as having fewer postoperative demands and received the fewest positive responses.
Education consistently emerged as the most significant component of preoperative therapy across all procedures. Further research is needed to identify the most effective educational content and understand its impact on outcomes such as pain management and functional recovery.
Future studies should focus on evaluating the effectiveness of preoperative therapy interventions, particularly for procedures with high postoperative demands, to maximise potential improvements in surgical outcomes.
Supplemental Material
Supplemental Material - Which elective hand surgery would benefit most from preoperative therapy interventions to enhance surgical outcomes? A survey of hand therapists
Supplemental Material for Which elective hand surgery would benefit most from preoperative therapy interventions to enhance surgical outcomes? A survey of hand therapists by Tahra Babiker-Moore, Carol J. Clark, Emma Kavanagh and Timothy B. Crook in Hand Therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.