
Abstract
Introduction
The first web space of hands has been understood to be important in daily activities involving the motions of cylindrical grasp and pinch. However, surgical and rehabilitation decision-making based on first web deficiency is challenging without clear definitions of function. This study aimed to evaluate the methods used to measure first web space and synthesize the evidence on its functional definition in children up to 18 years old.
Methods
This review followed Arksey and O’Malley’s six-stage framework operationalized by the Joanna Briggs Institute (JBI) methodology for conducting a scoping review. In conjunction with a medical librarian, 4440 term combinations were searched on MEDLINE from inception until January 2023. Title/abstract and full-text screening processes were conducted, followed by charting, collating, and summarizing included articles by two independent reviewers.
Results
Of 162 studies screened, 20 studies were included. The first web space was most commonly measured in palmar abduction (50%) of the carpometacarpal angle (45%) radiographically (30%). Systematic methods were rarely used (5%) to evaluate activity and participation function of first web limitations. Definition of a cutoff angle or first-web span that represented sufficient functional outcome was difficult to synthesize due to a lack of standard measurement methods.
Discussion
While the first web function was quantified in the studies, these values are problematic due to inconsistent measurement methods. A standardized assessment of first web space impairment and its relationship with activity and participation function is clinically significant for evaluating the need and meaningful outcomes of surgical and therapy interventions in children.
Introduction
The thumb accounts for 40 to 50 percent of the hand’s function.1,2 The first web space is an anatomical region of the hand that is essential for performing functional prehensile patterns using the thumb, including cylindrical grasp and pinch motions.
3
It is often defined as a triangular-shaped space between the first and second metacarpal distal to the carpometacarpal (CMC) joint, with both functional and aesthetic importance.
3
Traumatic injuries, including burns, crush injuries, and brachial plexus injury, as well as congenital hand and upper limb differences can cause impairments of the first web space. These impairments may include bone and joint, motor, and sensory deficits that negatively affect a child’s ability to grasp objects.
3
Contrasted in Figure 1 is a child with a typical first web space (Figure 1(a)) and two children with first web space impairments (Figure 1(b) and (c)). (a) Typical first web space, (b) Child with thumb hypoplasia with narrowed first web space and instability of the metacarpophalangeal joint, and (c) Child with a total brachial plexus injury with deficient first web space function from thumb abduction and extension motor impairment.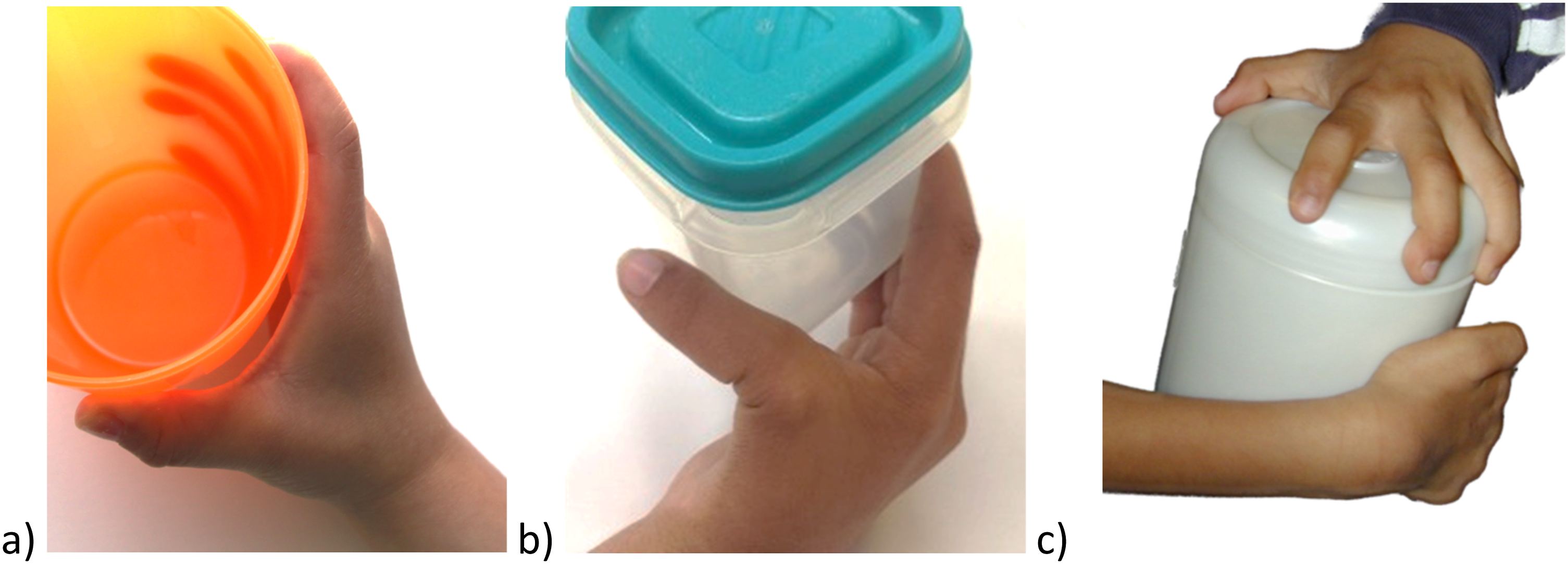
Rehabilitation interventions (e.g., stretches, wedge-shaped or web-spacer orthoses, and functional thumb orthoses) 4 and reconstructive surgical options (e.g., skin grafting, z-plasty soft tissue releases, joint arthrodesis, and tendon transfers)5,6 can increase the first web span and/or augment thumb abduction or extension function. However, it is unclear what degree of first web space impairments equate with negative functional impacts for the child. According to the International Classification of Functioning, Disability and Health (ICF) framework, it is important to understand activity and participation along with body function and structure to determine how impairments affect daily activities. 7 Activity is defined as the execution of tasks, and in the context of the first web space, includes opening containers, grabbing a water bottle, and using utensils. 8 Participation is defined as the involvement in life situations reflecting meaning and relevance for the individual, and in the context of the first web space, includes whether a child can open containers aligned with the expectations of their school environment. 8 Activity and participation components bidirectionally interact with each other and influence quality of life. 7 Therefore, interventions that improve impairment that are identified to improve activity have the potential to positively influence participation.
There are two purposes of this scoping review: (1) to evaluate the methods used to quantify the measurement of the anatomical first web space of the hand and (2) synthesize what is known about the definition of functional and deficient first web space. As the ICF considers function as the dynamic interaction between their health conditions, environmental factors, and personal factors, this review defines ‘functional’ first web space as upper limb activity capacity and performance of cylindrical grasp and participation. Participation in daily activities is dependent on developmental stage, occupation, and/or life context, making it difficult to measure its direct relationship to first web space impairment; however, it is important to determine child-specific interventions that translate to meaningful impacts on their day-to-day function. In contrast, ‘deficient’ first web space refers to impairment in its body function and structure. 7 The findings from this scoping review will help guide clinicians who provide surgical and rehabilitation interventions to children affected by first web space deficiency.
Methods
This scoping review used Arksey and O’Malley’s framework operationalized by the Joanna Briggs Institute (JBI) methodology for conducting a scoping review.9,10 A scoping review was conducted due to the broad nature of the topic on first web space function and no unified definition and measurement methods for this anatomical region. Through the six-stage scoping review framework, the literature on what is known about the definition and measurement of functional first web space was explored. 9 For this scoping review, the optional sixth step involving a consultation exercise was not conducted. The protocol for this review was not published in the public domain; one secondary question (i.e., reliability of methods) was added after data extraction was complete. The data were re-reviewed at that time, and no further changes were made.
Stage 1: Identifying the research question
Two primary research questions were identified in the paediatric population between ages 0 to 18 years: (1) What methods are used to quantify measurement of anatomical deficiency of the first web space? and (2) How are the definitions of functional and deficient first web space characterized? This review also addressed two secondary questions: (1) What is the reliability of the methods used to measure first web space? and (2) What is the cutoff for good surgical results or targeted outcome for functional first web space?
Stage 2: Identifying relevant studies – Search strategy
Relevant studies were identified in collaboration with a medical librarian at the Hospital for Sick Children, Toronto, Ontario, Canada. The JBI Population, Concept, and Context (PCC) approach was used for the search strategy. 11 The search was conducted on Ovid MEDLINE(R) and Epub Ahead of Print, In-Process, In-Data-Review & Other Non-Indexed Citations and Daily <1946 to January 18, 2023>, with 20 population terms, six concept terms and 38 context terms. 12 The population terms specified a paediatric population between ages 0 to 18 years, the concept terms specified first web space, and the context terms specified function and measurement of first web space and cylindrical grasp. See Appendix for PCC and search strategy. Additional articles were identified after Stage 3 by reviewing references of key articles with the highest study quality as determined by the Appraisal tool for Cross-Sectional Studies (AXIS) scores. 13 All records of the identified studies were recorded and displayed using the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) diagram. 14
Stage 3: Study source of evidence selection
Two independent reviewers (KK, EH) participated in the study selection process based on predetermined inclusion and exclusion criteria. The studies had to meet the following inclusion criteria: (1) involved paediatric population aged 0 to 18 years, (2) studies of the first web space of the hand, and (3) studies that measured and reported outcomes of overall hand function, cylindrical grasp, or first web space on more than one participant. The following exclusion criteria were also used to filter studies that only: (1) included descriptive information about hand function and first web space, and (2) measured other parts of the hand unrelated to first web space. Limitations were not placed on the date of publication to review the entire breadth and depth of the topic from the inception of the database to January 2023. Only studies written in English were chosen. Two independent reviewers (KK, EH) conducted the title and abstract review followed by full-text review using the Covidence software. 15 Reviewers met at the beginning, midpoint, and final stages of the review process to discuss and resolve challenges and uncertainties related to study selection. 16 The breakdown of reviewed, excluded and included studies in this review is presented in the PRISMA diagram. 14
Stage 4: Data extraction
A data extraction form on Microsoft Excel software was developed and piloted by the research team based on the primary and secondary questions, as well as collecting publication details. 17 Through the iterative process of charting data, the following sub-questions were generated as data variables to answer the primary and secondary questions: 1(a) How many studies quantitatively measured the first web and/or had author’s criteria on what is functional first web space based on their opinion or anecdotal evidence and interpretation of the literature? 1(b) What thumb abduction position (i.e., radial, palmar) was used to measure first web space? 1(c) For each thumb abduction position, how many studies measured soft tissue opening, clinical thumb CMC joint angle, or radiographic CMC joint angle? 2(a) What are functional and deficient first web space angles? 2(b) How many studies used pre- and post-first web space angle in measuring surgical outcomes? and 2(c) What is reported as the qualitative definition of functional first web space? Data were extracted from each article by two independent researchers (KK, FB). Any discrepancy in extraction was resolved through discussion between the two reviewers. Concurrently, quality appraisal was completed on the included studies to increase the rigor of this scoping review, using the AXIS, as lack of quality assessment in scoping reviews has been limiting the interpretation and uptake of the findings.13,16 All 20 items of the AXIS are weighted equally and answered either 1 = yes, 0 = no, or do not know. 13 Two reviewers were involved in rating each study (KK, FB). Any discrepancy was resolved through discussion. For this review, the overall quality of the study was interpreted using the following guidelines: low quality = 1–7; medium quality = 8–14; high quality = 15–20.18,19 Additional questions based on AXIS addressing important qualities relevant to the scoping review topic (see Appendix) were scored for each paper. The scores from these additional questions (greater than 4 out of 5) were used to determine the key articles to review their references and include additional articles in this review as mentioned above. All studies were considered for analysis irrespective of the results of quality assessment.
Stage 5: Data analysis and reporting the results
The data from the included studies were collated, summarized, and reported as results using Microsoft Excel based on pre-determined primary and secondary questions. 17 Detailed data collection and synthesis were conducted to address the sub-questions outlined in Stage 4 with particular attention given to ensure diverse findings were reported across studies. PRISMA Extension for Scoping Reviews (PRISMA-ScR) reporting guideline was followed. 20 The main study details were organized into a figure, including descriptive data from across the studies based on the identified questions in appendix. The primary and senior authors discussed the best methods of presenting the findings in tables and figures. The reported results aimed to provide a comprehensive picture of the breadth and depth of the research area on functional and deficient first web space. Gaps in knowledge based on this review were identified to provide recommendations for future practice and research regarding functional first web space.
Results
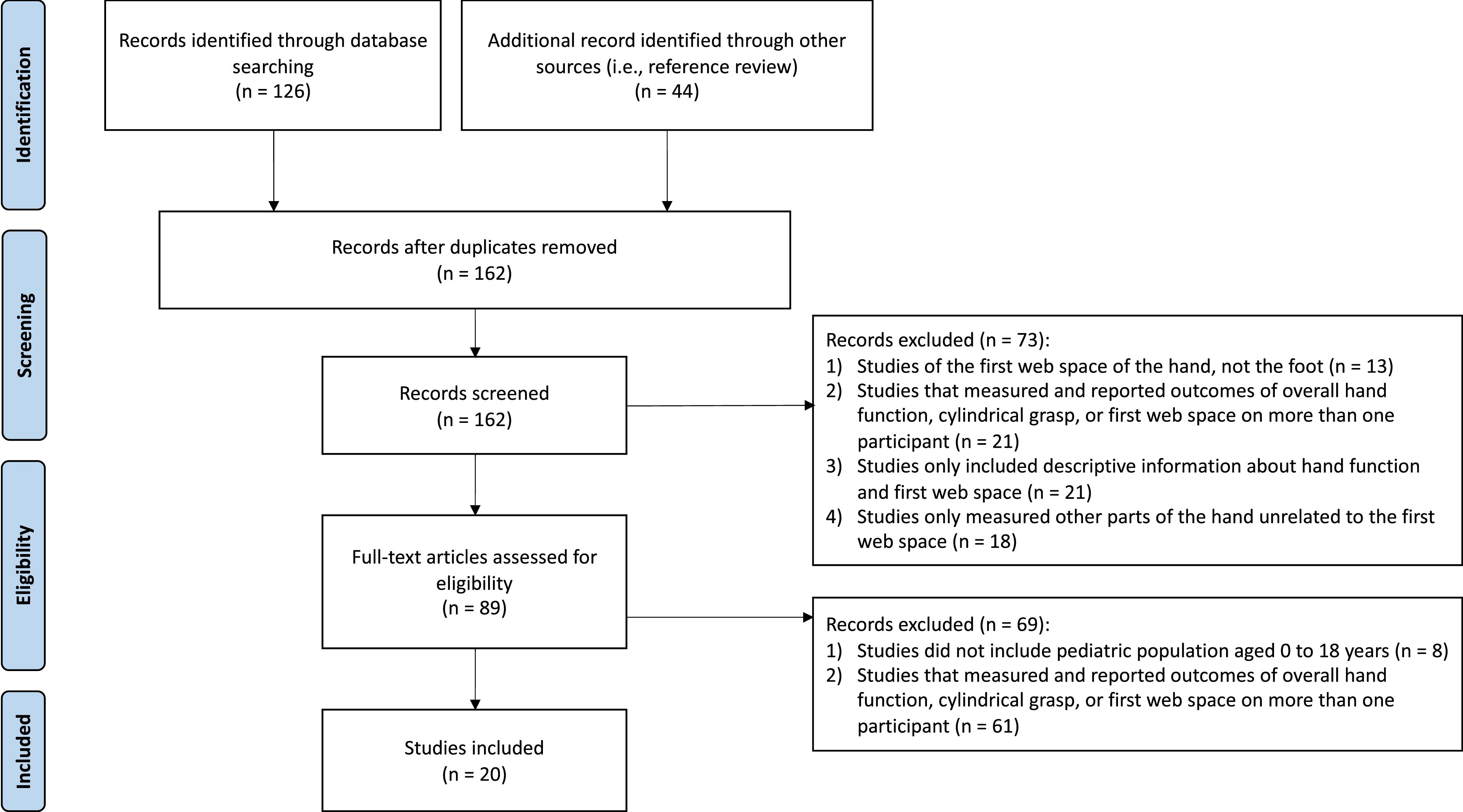
The search strategy resulted in 126 articles and the reference review of the key articles resulted in 44 additional articles, totalling 162 articles that were screened after eight duplicates were excluded. After the title and abstract review, 73 articles were excluded, and after the full-text review, 61 articles were excluded, resulting in 20 included studies as shown in Figure 2. The main reason for the exclusion was not meeting the third inclusion criterion, which was “studies that measured and reported outcomes of overall hand function, cylindrical grasp, or first web on more than one participant.” The PRISMA flow diagram from the study selection
14
.
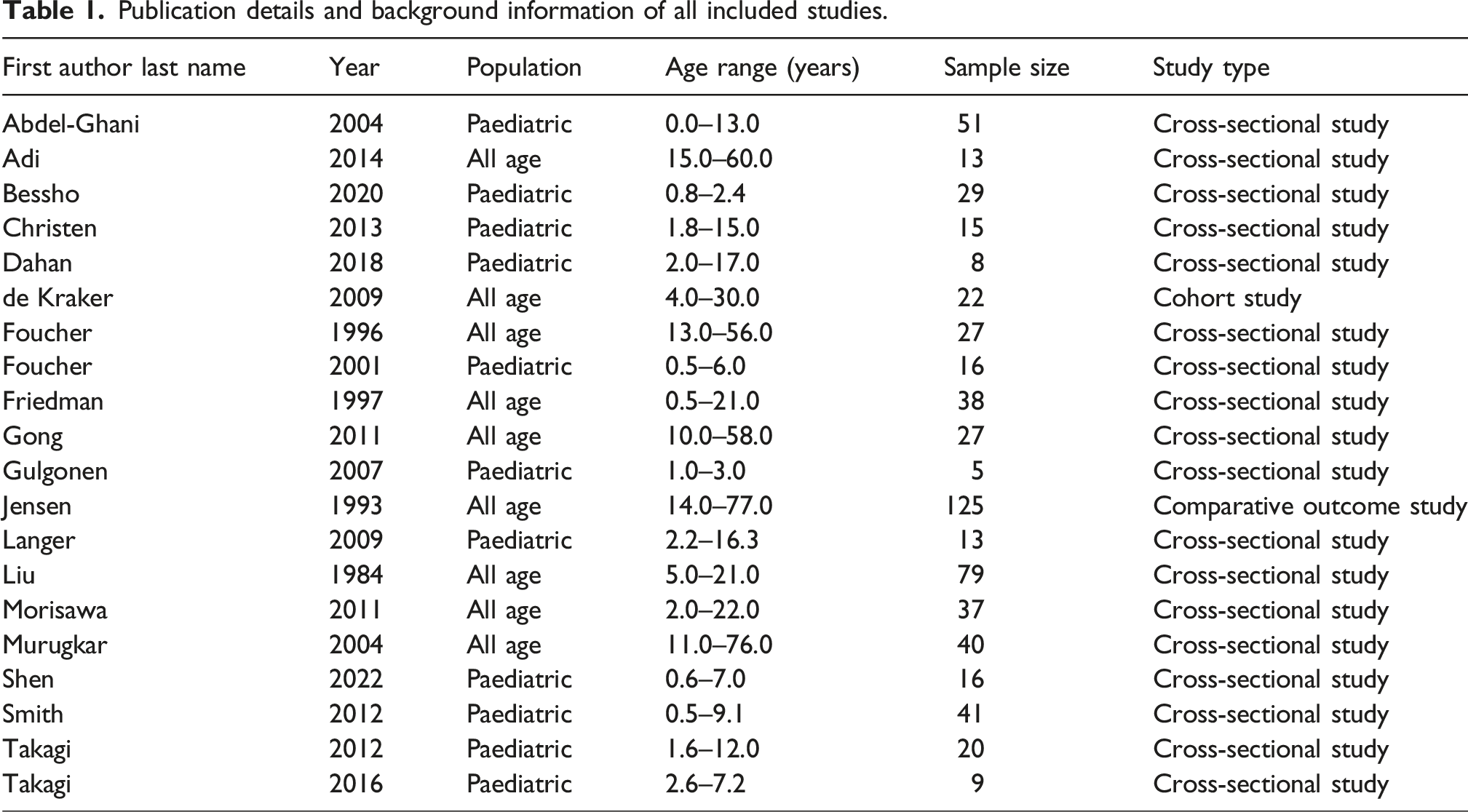
Publication details and background information of all included studies.
AXIS quality assessment results of the included studies.
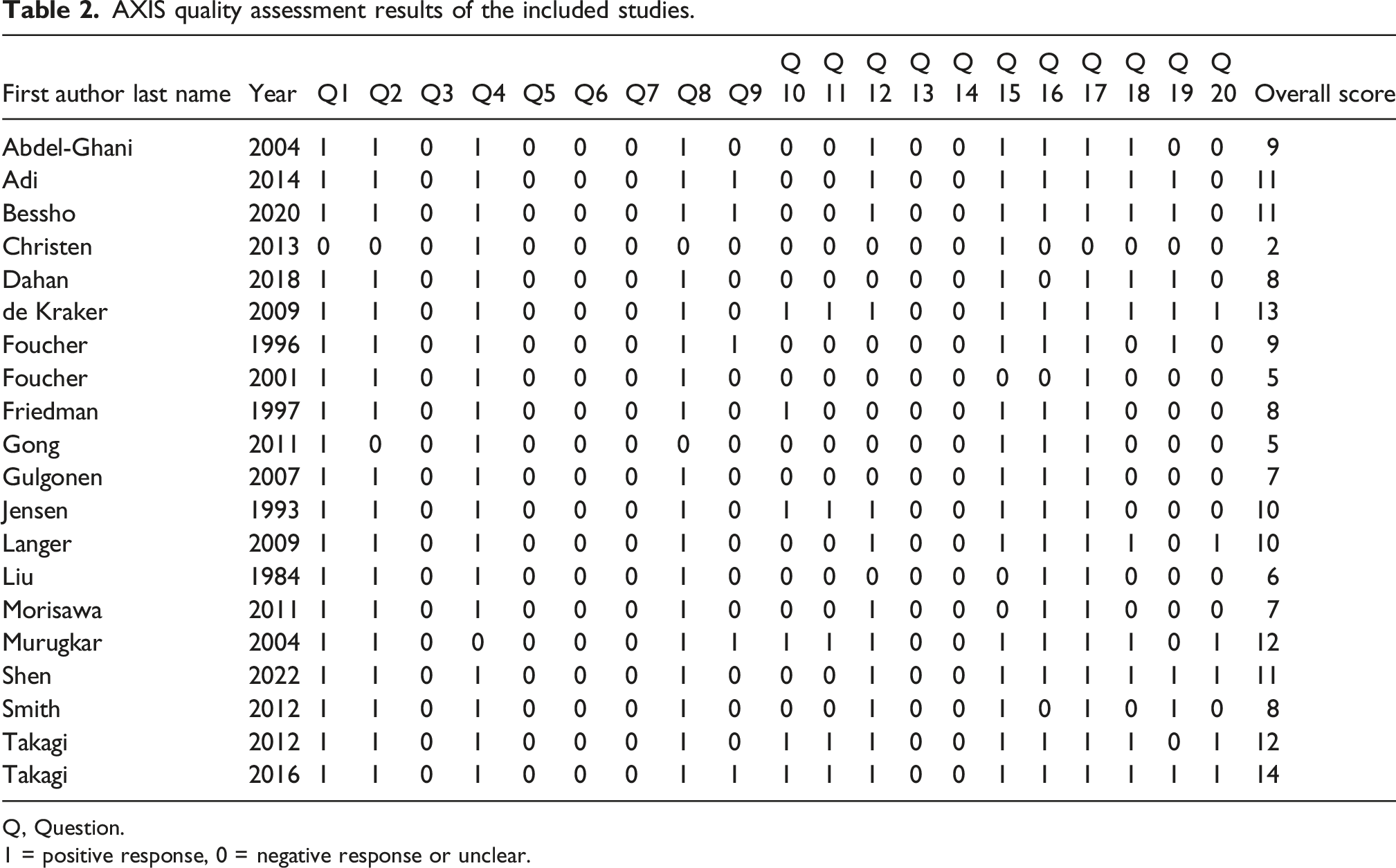
Q, Question.
1 = positive response, 0 = negative response or unclear.
Additional AXIS questions answered specifically for this scoping review.
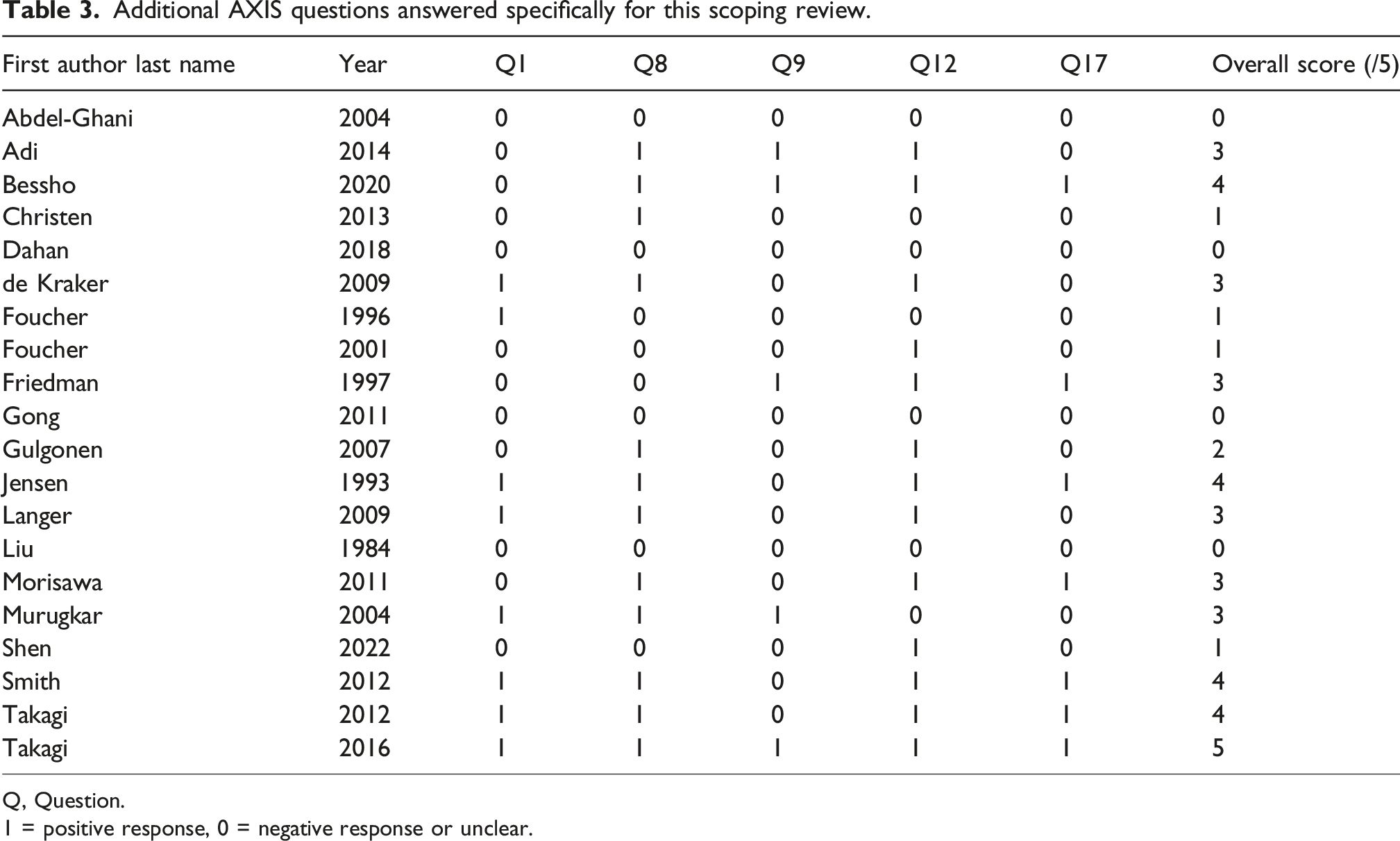
Q, Question.
1 = positive response, 0 = negative response or unclear.
Aim 1: Quantified measurement methods of the first web space
In paediatric populations between ages 0 to 18 years, quantified measurement of the first web space was reported in 95% (n = 19) of studies, and 70% (n = 14) of studies included the authors’ criteria on what was defined as a functional first web space based on opinion, anecdotal evidence, and/or interpretation of the literature (Figure 3). The overall methods used to quantify the measurement of the first web space were highly variable across studies. Figure 3 illustrates that the lack of consensus on methods used, contributed by: (1) varied thumb abduction position, (2) varied use of soft tissue vs bone and joint landmarks, (3) differing clinical and radiographic approaches, and (4) lack of functional activity measurements. Flow diagram on the various methods used to quantify measurement of first web space based on (1) varied thumb abduction positions, (2) varied used of soft tissue vs CMC joint, (3) clinical vs radiographic measurement, (4) measured in angle vs length, and (5) functional measurement.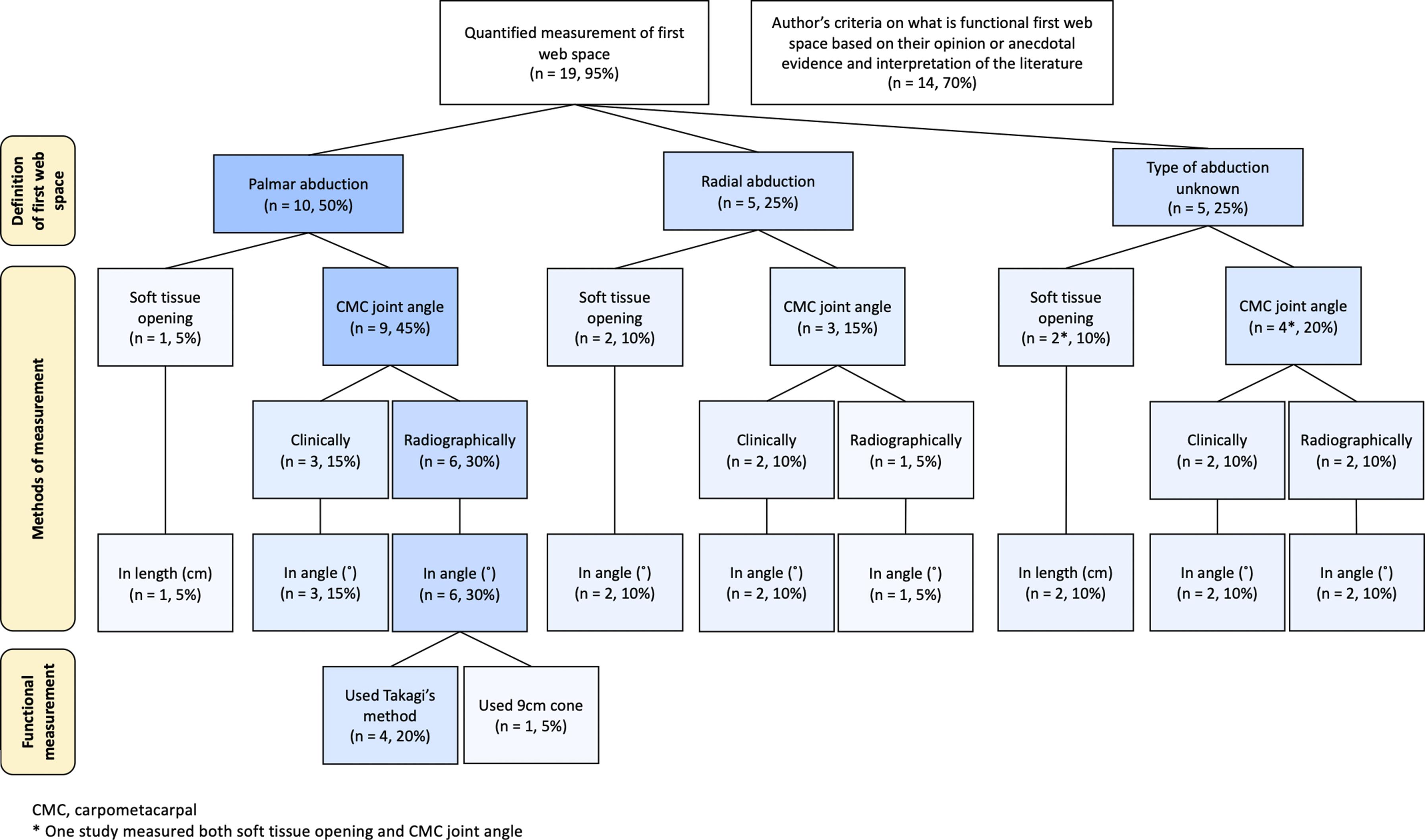
Among all studies reviewed, the most common quantitative approach (30%, n = 6) was to measure the intermetacarpal angle (i.e., degrees) of the CMC joint radiographically in palmar abduction (Figure 3). In terms of the reliability of the methods, two studies, Murugkar et al. 2004 and de Kraker et al. 2009, assessed them in measuring the first web space. Murugkar et al. indicated good inter-rater reliability (intraclass correlation coefficient (ICC) > 0.80) and clinically useful test-retest range with measuring the intermetacarpal distance using a caliper (i.e., separation between middorsal points on the subcutaneous surfaces of the first and second metacarpal heads in millimeters), and poor reliability for the conventional method that uses a goniometer. 21 De Kraker et al. found inter-rater reliability using the Pollexograph, a novel tool to measure palmar abduction as defined by the angle between the palm and the tip of the thumb, as excellent (ICC = 0.98–0.99), which was also greater than conventional goniometry. 22
In relation to measuring function, four studies (20%) used Takagi et al. (Takagi’s method) of holding a cone to radiographically measure CMC joint angles (Figure 3). 23 In this approach, the child is asked to hold onto a styrene foam cone (10 cm base diameter, height 25 cm) at the largest circumference of the cone in which their thumb and index finger still maintain circumferential contact. 23 One additional study used a 9 cm cone to measure a cylindrical grasp. 5 Takagi’s method was the only documented standardized method of measuring the activity capacity function of cylindrical grasp.23–26 Takagi et al. 2012 assessed the validity of imaging using the cone and showed that measuring the thumb to index finger metacarpal angle enables evaluation of the severity of first web space narrowing and radial instability of the CMC joint in children with type II and IIIB thumb hypoplasia. 23 However, the largest circumference was not documented.
In accordance with the ICF, only Christen et al. included outcomes that measured both activity and participation of functional first web space. Their study involved measuring the CMC angle in palmar abduction using Takagi’s method (i.e., activity capacity) and child/parental satisfaction rating of function and appearance (i.e., the subjective component of participation in its consideration of perceived function in the context of the child’s life) post first web space reconstruction. 25 The authors reported a mean 15 degrees of CMC angle improvement, but they did not report the post-operative angle. The three other studies that used Takagi’s method (i.e., activity capacity function) found improvements in first web space from pre- to post-procedure and reported an average post-operative CMC palmar abduction angle of 52.6, 59.4 (4.0 SD), and 45.4 (3.9 SD) degrees.23,24,26
Five studies obtained child/parental feedback regarding their satisfaction post-procedure and participation in daily activities.27–31 However, the informal nature of these data limited its use and interpretation (See Appendix for details).27–31
Aim 2: Functional and deficient first web space
Definitions of deficient first web space (i.e., impairments) were stated by most published studies. Nearly half (45%, n = 9) of the studies used the difference in pre- and post-procedure angle as an indicator of positive surgical or rehabilitation outcomes. Nine (45%) studies identified a cutoff first web space CMC angle; however, the range of this cutoff angle varied from 30 to 100 degrees with varying ages. Overall, sufficient data were found that represented changes in impairment and cutoff values of the first web space. However, due to the heterogeneous nature of these data with respect to what was measured (e.g., CMC joint angle, soft tissue), how it was measured (e.g., palmar vs radial abduction), types of measurement (e.g., clinical, radiographic), and lack of standardization of procedures (e.g., landmarking), it was difficult to synthesize, and pooling of results is not supported.
Lastly, qualitative descriptions of the level of functional first web space were stated in 45% (n = 9) of the studies, and the impairment level of deficient first web space was stated in 60% (n = 12) of the studies. See Appendix for details. Although they provide important insight into how researchers and clinicians classified functional and deficient first web space, these data are inconsistent and difficult to synthesize.
Discussion
Through this scoping review, 20 included studies identified a limited standardized and reliable methods for measuring children’s first web space. Little is known about what is deemed functional first web space in relation to a child’s activity capacity and participation. What the studies mainly focused on was reporting postoperative CMC angles (i.e., impairment). Most data support the definition of deficient first web space in relation to preoperative values, commonly measured as CMC palmar abduction angle using radiographs. Some cutoff angles representing impairment of the first web space were below the range of 30 and 40 degrees; however, heterogeneity and poor overall study quality limit the interpretation and use of these values. With insufficient quality in the included studies based on the AXIS, this review highlights gaps in knowledge on comprehensive, standardized, and reliable methods of assessing functional first web space.
This review identified and summarized all the methods used to quantify the first web space on paediatric population. Identifying a single best method was not possible due to the diversity of methods used and the lack of reliability testing. For instance, positioning of the thumb in abduction was inconsistent. While the studies did not justify their measurement methods, the use of radial abduction by some studies may be due to the radiographic positioning of the hand, parallel to the image receptor. 32 Moreover, while the use of X-rays may provide more accuracy, clinically measuring hands and using soft tissue angles may have been used to avoid radiographic exposure. Among diverse methods of measurement, most studies measured the CMC joint angle in degrees using X-rays, which would show consistency and accuracy. Next, most studies that measured first web space positioned the thumb in palmar abduction, which more appropriately aligns with pinch (i.e., pincer) and grasp (i.e., cylindrical, radial digital) movement than radial abduction.32,33 However, it is important to note that a lack of reliability in these methods could lead to misleading data. There were only two studies that looked at the reliability of the methods used to measure first web space, and they mainly focused on reliability of different tools to clinically measure the CMC joint angle.21,22 It was interesting to note these studies showed that using calipers or the Pollexograph was more reliable compared to conventional goniometry. However, the Pollexograph used by de Kracker et al. would be difficult to use in clinical practice due to its large size. 22 Although these two studies are a good start for testing the reliability of the first web space measurement, given the poor quality assessment and the published date of their papers (i.e., 2004 and 2009), more research is necessary. There were no studies that looked at the reliability of radiographic measurement of palmar abduction of the CMC joint angle. While radiographically measuring the CMC joint angle in palmar abduction was the most common and valid approach to measuring the first web, the quantitative outcomes reported in the studies reviewed should be interpreted with caution as more research is necessary to properly validate this method.
Regarding measuring function, Takagi’s method was the only systematic method used to measure activity capacity. 23 While Takagi et al. 2012 mentions the validity of their method, 23 the validity was not systematically tested using proper statistical methods, and it is unclear if it is valid for measuring function and impairment level of first web space in all paediatric patients. Thus, the next steps in validating the Takagi method would be to establish its reliability and determine its relationship to the child’s function in daily activities and their hand sizes by age. Lastly, refinement of Takagi’s method by adding documentation of the minimum cone circumference achieved may help define a cutoff score of functional and deficient first web space at a certain stage of development. Currently, in the absence of these data, Takagi’s cone with a base circumference of 10 cm appears to be the best guidance. 23
While some studies asked parents and patients how they felt about their first web space, their methods were informal. This shows evidence of attempts to incorporate patient-reported outcome measure (PROM); however, their methods and relation to quantified first web space measurement are unknown. Overall, more research is needed to identify an effective method of measuring functional first web space in relation to activity capacity (e.g., grasp) with the plans of establishing its relevance to participation through validation with PROM on hand function. As the child may have different hand sizes based on their growth, 34 the satisfaction with the object they can and want to carry might vary, and capturing this information would be of benefit in determining an effective way of measuring the first web space function that matters to them. The use of validated PROM such as the Patient Reported Outcomes Measurement Information System (PROMIS) Upper Extremity or the ABILHANDS-Kids is recommended.35,36
It was evident throughout the included studies that most authors defined function and deficient first web space as impairment when children with poorer CMC joint angles needed surgery. For example, the cutoff CMC angles by Gilbert’s method of assessment of thumb are good (3°–40°) and excellent (40°–45°). 27 However, these data should be interpreted with caution due to 1) the poor quality of included studies, 2) no paediatric normative data to support the interpretation, and 3) the varied etiology of the restricted first web space from congenital to traumatic conditions. While a few studies compared outcomes to unaffected healthy hands, most studies reported functional improvements when post-operative angles were larger than pre-operative; which is problematic because these results lack contextual meaning to the child’s day-to-day function. Additionally, the only reported soft tissue angle for unaffected functional hands is 100°.29,37 This value was derived from Jensen’s study that measured the average soft-tissue angles. 37 Having this value as the only cutoff for a functional hand is problematic because there was no reliability and standardization in the methods.
Furthermore, first web space outcomes were assessed, measured, and defined by physicians and/or surgeons in most of the included papers. The definition of what is deemed functional and deficient might vary based on professional training. The surgical perspective and clinical practice may differ from the rehabilitation lens of therapists. Overall, there was a lack of information in the current literature to clearly define functional or deficient first web space in the paediatric population based on activity and participation. The current knowledge gap poses a difficulty in making shared decisions on rehabilitation and surgical treatments of deficient first web space based on what is meaningful to paediatric patients and their families.
Overall, based on what is known, radiographically measuring CMC joint angle in palmar abduction was most used and Takagi’s method 23 was the only approach that also measured activity function. This finding can be applied to better assess the need for rehabilitation plans or reconstructive surgery and contribute to the development of standardized assessment tools for paediatric population. More specifically, the Brachial Plexus Outcome Measure (BPOM) 38 and the Thumb Grasp and Pinch Assessment (T-Gap)39,40 are validated upper limb function performance outcome measures that include cylindrical grasp assessment items. For children ≥4 years of age, the BPOM evaluates cylindrical grasp activity function using a five-inch circular container. 38 A container of bubbles (approximately 1.5 inches) and a peanut butter jar (approximately 2.9 inches) are items on the T-Gap assessment that are used to evaluate cylindrical grasp in children 18 months to 4 years and 5 to 18 years respectively.39,40 This illustrates the variability of objects used to determine functional first web space and the importance of Takagi’s work as a starting reference point to validate the assessment items used in such standardized measures.
The limitations of this scoping review pertain to including only English papers because of the languages known to the research team. The exclusion of non-English studies may have restricted valuable insights from diverse contexts and introduced language bias. It is recommended that future reviews include a multilingual team to include studies written in other languages in the review. The decision not to include the optional sixth-step consultation of Arksey and O’Malley’s framework was made prior to the data collection due to limited resources and time as this scoping review was conducted as graduate work. When the contents of the included studies were unclear, the authors of those studies were not contacted to clarify their methods, which it would have been difficult to contact authors from over 20 years ago. 28 This could have prevented practical insights, and it is recommended that future studies consider consultation with clinicians and affected population to maximize the applicability. Moreover, as the search was performed from inception to capture all data, radiographic imaging, surgical options, and measurement tools (e.g., high-definition or electronic goniometry) have advanced over the past years, which could have affected how first web space improvement was measured and reported. However, the comprehensive database searches ensured that a broad range of evidence was considered, maximizing consistency and transparency in data collection and synthesis. While the included studies resulted in not most recently conducted studies, this reinforces the importance of further research in this area. Future research may be able to capture any technological advancement that could help with standardized measurement of first web space. Lastly, although this review aimed to focus on the paediatric population, synthesizing the knowledge from adult literature may have provided additional insights.
Conclusion
Through this review, it was evident that most clinicians and researchers define functional and deficient first web space based on impairment level and methods of measuring such impairment and anatomical structure of first web space vary and are unreliable to date. More normative studies and investigation on methods that measure activity capacity and test their reliability and validity, potentially incorporating PROM and considering their growth, would be encouraged to enhance treatment protocols and patient care approaches. Such measurement tools could potentially benefit day-to-day decision-making in hand therapy, selecting most appropriate rehabilitation interventions and reconstructive surgical options. Additionally, collaboration among surgeons, therapists, and researchers in this area could further enhance the measurement and definition of functional or deficient first web space in treating children with an interdisciplinary approach. Based on the discussion, further research would allow patient-oriented care based on each child’s need and benefit the standardization of measurement tools for children with upper limb differences that affect hand function.
Supplemental Material
Supplemental Material - Definition and measurement of functional first web space: A scoping review
Supplemental Material for Definition and measurement of functional first web space: A scoping review by Kate Kyuri Kim, Farah Bacchus-Misir, Darcy Fehlings, Karen Wong and Emily S. Ho in Hand Therapy.
Footnotes
Authors contributions
Kate Kyuri Kim: Conceptualization, methodology, data collection, formal analysis, writing – original draft, reviewing and editing. Farah Bacchus-Misir: Data collection, data analysis, review and editing. Darcy Fehlings: Methodology, review and editing. Karen Wong: Methodology, review and editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Rehabilitation Sciences Institute at the University of Toronto; Sick Kids Division of Plastic and Reconstructive Surgery; University of Toronto Connaught New Researcher Fund; and Canadian Institutes of Health Research Canada Graduate Scholarship – Master’s Program.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.