
Abstract
Background
Hand surgery is commonly required for conditions like Dupuytren’s disease, carpal tunnel syndrome, and carpometacarpal osteoarthritis. Hand experts agree that patient education and managing expectations can optimise surgical outcomes. With an aging population, and rising rates of diabetes and obesity, a significant increase in elective hand surgeries is anticipated over the next decade.
Objective
To assess the effectiveness of preoperative therapy interventions on improving postoperative outcomes following elective hand surgery.
Method
A systematic search of six databases accessed journals from January 2011 to April 2024. Included studies assessed postoperative outcomes following preoperative therapy intervention.
Results
Seven articles met the inclusion criteria: six randomised controlled trials (RCTs) and one retrospective cohort study. Five RCTs explored effects of opioid education on postoperative consumption, all reporting statistically significant differences in favour of the intervention, with one showing a decrease of 49.7 morphine equivalent units (95% CI: 11.9 to 87.5), representing a 34.7% decrease between intervention and control. All RCTs scored poorly for risk of bias with the exception of one which assessed the effects of a neuroscience pain education on postoperative pain, reporting a non-significant decrease of 7.7% favouring the control.
Conclusion
There is a lack of quality research assessing preoperative interventions and outcomes for hand surgery. There was some indication of favourable outcomes following preoperative opioid education; however, number of studies were small, the evidence quality was poor, and data were limited. Further research is required to address these gaps and identify the most effective preoperative interventions.
Introduction
Hand conditions such as Dupuytren’s disease, carpal tunnel syndrome, and carpometacarpal osteoarthritis are becoming increasingly prevalent, partly due to an aging population and rising chronic health disorders. 1 The socioeconomic impact of impaired hand function and pain due to these conditions is substantial, affecting individuals’ social, personal, and mental capacities.2,3
Specialist hand surgery is often required to restore function, and the number of such surgeries is expected to rise significantly in the UK over the next decade. 1 Various postoperative rehabilitation interventions are available following hand surgery, including exercise, education, massage, splinting, ultrasound, and corticosteroid injections. However, preoperative interventions are not routinely implemented, despite consensus among hand experts that addressing patients’ anxiety, pain, and expectations preoperatively is crucial to achieving optimal outcomes.4,5 It is suggested that this preoperative focus should involve expectation setting, and education around post-operative exercise prescription, oedema reduction, scar management, and advice on activities of daily living prior to surgery. 4
In constrast, an invasive preoperative surgical intervention has demonstrated improved outcomes for Dupuytren’s fasciectomy. 6 This intervention uses an external fixator in a preliminary operative procedure to facilitate progressive soft tissue distraction at the proximal interphalangeal joint, showing promising results in enhancing extension gains post-fasciectomy. Given the success of conservative management for even longstanding flexion contractures, this raises the question of whether similar outcomes could be achieved with non-invasive methods, such as serial casting or a static progressive thermoplastic splint applied preoperatively. 7
Optimal postoperative outcomes in musculoskeletal surgeries often hinge on the interplay of reduced pain, enhanced knowledge, and increased adherence to postoperative therapy, all of which are intricately connected.8,9 Education can significantly influence a patient’s perception and understanding of pain, thereby shaping both their pain experience and psychological response. 10 Effective pain management not only alleviates discomfort but also promotes better adherence to therapy regimens. Patients experiencing lower pain levels are more likely to engage actively in rehabilitation exercises, leading to improvements in both clinical outcomes and functional recovery. 11 Achieving these outcomes requires implementing behaviour change strategies, facilitated by strong therapeutic alliances between therapists and patients. 12 Engagement in preoperative therapy lays the foundation for cultivating these alliances and prepares patients mentally and physically for postoperative recovery. This systematic review aims to assess existing evidence for the effectiveness of preoperative therapy interventions on improving postoperative outcomes following elective hand surgery.
Method
Search strategy
The review protocol was registered with PROSPERO (CRD42023394946) and conducted in accordance with PRISMA guidelines.
13
A systematic search of the literature was conducted in April 2024, identifying articles within six electronic databases: MEDLINE Complete; CINAHL Complete; Academic Search Ultimate; Scopus; Web of Science; and Cochrane Library. The reference list of included studies was also searched, while unpublished studies were not pursued. A Boolean search strategy was used to achieve a comprehensive identification of the available literature, using terms key to the research question, along with their synonyms (supplemental table 1). Both free-text terms and subject headings were used where possible. The complete search strategy was first created in a separate log document and then copied and pasted into the relevant databases. Following removal of duplicates, articles identified through initial searches were assessed and screened for eligibility by title and abstract by the first author (TBM). The first and second authors (TBM and CC) then independently undertook a full text evaluation of remaining articles. Reasons for omission of excluded articles were recorded (Figure 1). Prisma diagram showing paper selection method.
Selection criteria (inclusion and exclusion)
Inclusion and exclusion criteria.
Data collection
Study details for the 7 included articles.
Study outcomes for the 7 included articles.
MEU: morphine equivalent units; OME: oral morphine equivalents; MME: morphine milligram equivalents.
aPain intensity was measured on a visual analog scale (VAS; 0–10).
bSatisfaction measured with a five-point response scale from “no improvement” to “eliminated symptoms completely” (scores 0–4).
Despite five of the included studies evaluating a similar intervention, a meta-analysis was not feasible due to differences in the timing, nature, and duration of outcome assessments. The studies lacked standardisation in outcome measures, with none reporting effect sizes, and some providing insufficient data for calculating effect sizes for primary outcomes. Consequently, a narrative synthesis of findings was adopted.
Quality appraisal
Assessment of study quality using a modified version of the Downs and Black Checklist 14 facilitated comparison across the two study designs included in this review. However, to mitigate against misleading review findings, and to ensure accurate inferences regarding risk of bias assessments for the included RCTs, the Cochrane Risk of Bias tool for randomised trials (RoB2) was employed. 15 This dual approach ensures a comprehensive and rigorous evaluation of study quality across all included studies.
The Downs and Black checklist provides a general global score for study quality alongside individual scores for quality of reporting, internal and external validity, and power to detect effect. With a maximum score of 28, each paper was assigned the corresponding grade: excellent (24–28 points); good (19–23 points); fair (14–18 points); or poor (<14 points). 16 Only studies grading fair, good or excellent were deemed robust and reliable enough to be included for review (supplemental table 2).
The RoB2 tool provides domain level and overall study judgement about risk of bias in the findings of a single outcome for RCTs (supplemental tables 3 and 4). The tool is structured into five domains through which bias might be introduced, including bias arising from the randomisation process; bias due to deviations from intended interventions; bias due to missing outcome data; bias in measurement of the outcome; bias in selection of the reported result. Judgements using the tool assessed the primary study outcome under review, categorising biases as either ‘Low’ risk, ‘High’ risk, or indicating ‘Some concerns’ within each of the specified domains 17 (supplemental Tables 3 and 4). Assessment of quality was reviewed by the first and second authors.
Results
Included studies
The search generated a total of 2724 articles of which only seven were considered appropriate for review (Figure 1). Six studies were randomised control trials (RCTs) of which five were conducted in the USA,18–22 and one in Chilie. 24 The seventh study was a retrospective observational cohort study conducted in Finland. 23 The six RCTs were all educational interventions, five exploring the impact of a standardised preoperative patient education programme designed to reduce opioid use after surgery,18–22 and one assessing the efficacy of a single preoperative pain neuroscience education session on reducing postoperative pain, kinesiophobia and upper limb function. 24 The one retrospective cohort study explored the effect of conservative therapies before and after surgery on improving symptoms and patient satisfaction postoperatively. 23
Quality assessment
Quality assessment scores ranged from 14 to 25 points on the Downs and Black modified checklist (supplemental table 2). One RCT rated ‘excellent,’ scoring 25 points, 24 five RCTs fell within the ‘good’ classification with four scoring 19 points18,19,21,22 and one scoring 22. 20 The final study was the only retrospective observational cohort study and classified as ‘fair’ scoring 14 points. 23 Despite overall quality scores of fair or above for all included studies, none of the RCTs reported an effect size with confidence interval for primary outcomes. Three studies provided sufficient data for calculating an effect size on their primary outcome,19,21,24 while the remaining three studies lacked adequate information for at least one primary outcome measure.18,20,22
The risk of bias assessment using the RoB2 tool revealed a high overall risk of bias for five of the included RCTs18–22 and a low risk of bias for only one 24 (supplemental tables 3 and 4). The most significant contributors to the high risk of bias were found in two key areas: bias due to missing outcome data, which was evident in four of the six RCTs,19–22 and bias in the measurement of outcomes, observed in three of the six studies.18,19,21 The latter was primarily due to the potential influence of knowledge of the intervention received on the assessment of outcomes. Additionally, concerns regarding bias in the selection of reported results were raised in three studies, primarily due to insufficient information on a pre-specified data analysis plan.18,20,21
Study characteristics
Table 2 lists study details for all included studies.
Sample population
The seven studies included a total of 875 patients. However, in the study by Multanen et al., 23 multiple intervention groups were assessed. When comparing only patients who received a preoperative intervention to those with no intervention, the total number of participants across all studies was 700. Five of the six RCTs evaluated the impact of a preoperative patient education programme aimed at reducing opioid use after surgery,18–22 with sample sizes ranging from 40 18 to 191 20 patients. The gender distribution was relatively balanced, with females comprising 50.3% on average, and the mean age was 58.3 years. The sixth RCT examined the postoperative effects of a single preoperative pain neuroscience education on 30 patients, with a female majority of 66.7% and a mean age of 54.2 years. 24 The one retrospective cohort study explored conservative therapy usage before and after carpal tunnel release in 259 patients, with a female majority of 66% and a mean age of 62 years. 23
Although all five RCTs evaluating a preoperative opioid education intervention assessed outcomes following a form of upper extremity surgery, inclusion criteria regarding type and location of surgery differed. One examined outcome following all elective outpatient upper extremity surgeries, including bone and soft tissue procedures of the wrist, elbow, and shoulder. 21 This was the only study to include shoulder surgery. Stepan et al. 20 assessed non-minor elective hand surgery and included procedures of the hand, wrist, and elbow, whereas Zohar-Bondar et al. 22 looked only at minor soft tissue procedures of the wrist and hand. The remaining two opioid studies examined outcome following carpal tunnel release only, one, a mini-open procedure 18 and the other, an endoscopic procedure. 19 The RCT examining the efficacy of a preoperative pain neuroscience education reported outcomes following carpal tunnel surgery only, 24 as did the 2021 retrospective cohort study examining the use of conservative therapies before and after surgery. 23
Intervention and control
The opioid educational interventions in all five opioid studies presented similar content. This encompassed education on the opioid epidemic and its ramifications, detailed information on the properties of opioids, guidelines for safe consumption practices, an overview of expected post-surgical pain levels, and a structured approach to pain management. This approach emphasised the use of non-opioid pain management strategies as the primary line of defence, underscoring the significance of mitigating opioid dependence. Four studies delivered the intervention electronically via webinar or pre-taped video,19–22 with two also providing a written summary post-surgery20,22 and one granting access to the webinar link for the duration of postoperative recovery 19 (Table 2). The fifth opioid study involved a brief review with the surgeon immediately prior to surgery. 18 The RCT assessing efficacy of preoperative pain neuroscience education consisted of a single 30-min, one-on-one pain neuroscience teaching session, using examples and metaphors to describe neurophysiological and biopsychosocial aspects of pain via audio and visual instruction. 24 Three RCTs described routine preoperative education for both intervention and control groups,20,22,24 while three did not specify any preoperative intervention for controls.18,19,21 The retrospective study discussed various preoperative conservative therapies like splinting and massage but lacked details on frequency or duration. The study compared outcomes among patients receiving different therapy interventions and those receiving none. 23
Study outcomes
Outcomes were assessed with a focus on the primary measures consistently reported across the included studies, or those most closely related, to ensure comparability and relevance to this review’s objectives. However, due to the varied interventions and the lack of consensus on the most appropriate outcome measures, the results were not always comparable across studies. This necessitated the segmentation of review findings, with discussion grouping outcomes as follows: postoperative opioid consumption and (where possible) postoperative pain and the proportion of patients who took opioids postoperatively for the opioid studies; postoperative pain for the pain neuroscience education study; patient satisfaction with treatment for the conservative therapy cohort study.
Outcome data table – effect size.
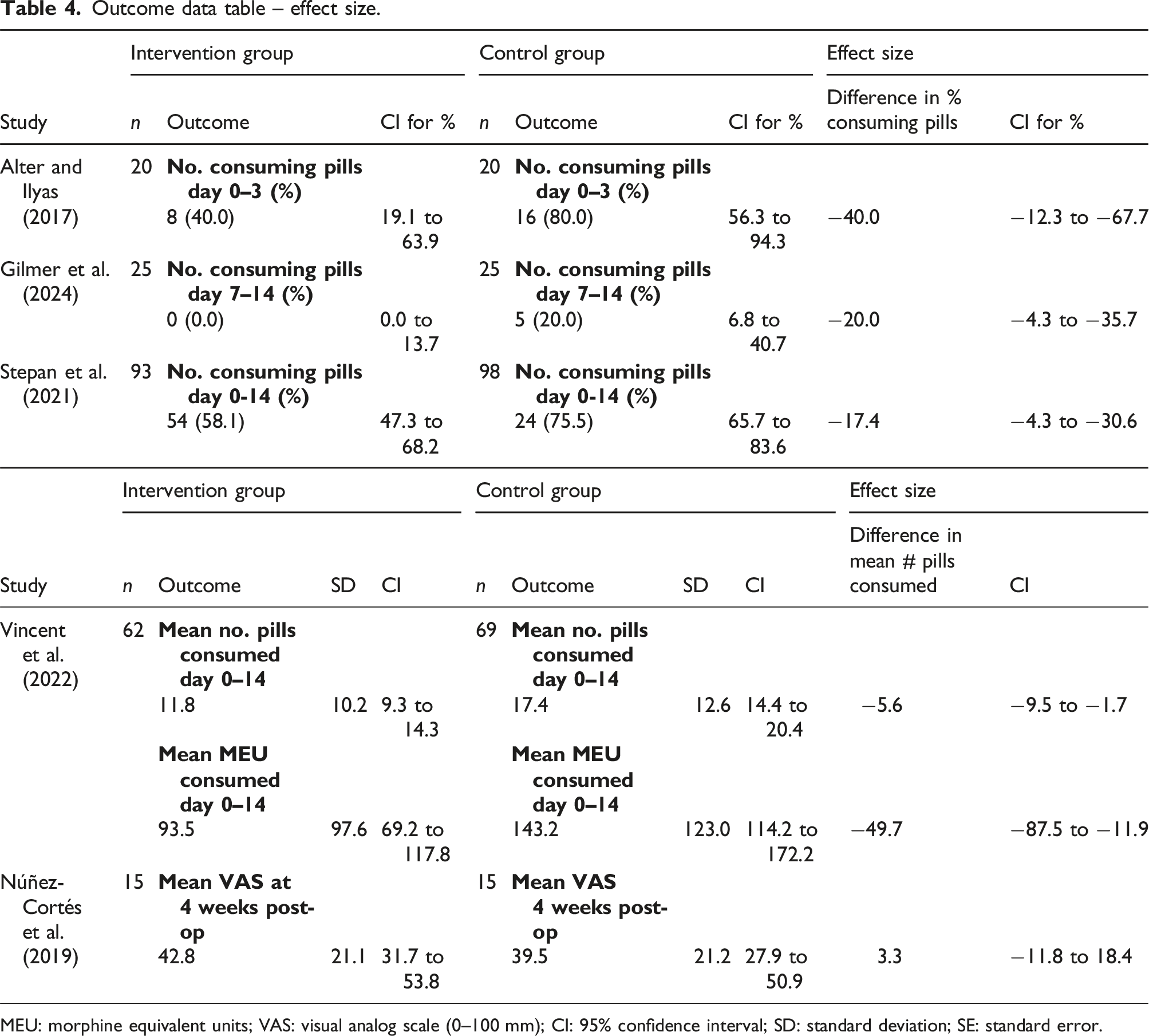
MEU: morphine equivalent units; VAS: visual analog scale (0–100 mm); CI: 95% confidence interval; SD: standard deviation; SE: standard error.
The single study on pain neuroscience education found no significant differences in perceived pain at 4 weeks postoperatively, with between group difference calculated on the VAS as 3.3 (95% CI: −11.8 to 18.4), equating to a non-statistically significant difference of 7.7% in pain score favouring the control. Additionally, there was also no significant difference in pain catastrophising, kinesiophobia, or upper extremity function at weeks four and 12 postoperatively. 24
Multanen et al. 23 examined the use of conservative therapy before and after surgery on levels of patient satisfaction measured with a five-point response scale to the question “Did the surgery improve the condition of your hand or wrist?.” Results reported higher treatment satisfaction in patients receiving only preoperative conservative therapies compared to other groups.
Discussion
This systematic review aimed to investigate the efficacy of preoperative therapy interventions on postoperative outcomes following elective hand surgery. While evidence suggests positive outcomes from such interventions in lower limb surgery,25,26 research in the context of hand surgery is limited. Assuming results of lower limb research can be applied to the upper limb is problematic as the upper and lower limb differ in function, anatomy and neurology. Despite the anticipated rise in elective hand surgeries, 2025 is only predicted to see numbers reach 145,000 jointly in the UK. 27 This relatively small number of procedures presents challenges for conducting robust research, including high costs associated with multi-centre trials. This review identified only seven studies meeting the inclusion criteria and as a result highlights the need for further research to explore the effects of preoperative interventions on the outcomes of hand surgery specifically.
The Downs and Black Checklist revealed variations among the included studies. Three of the six RCTs lacked blinding of study subjects, increasing risk of ascertainment bias. Notably, none of the included studies adequately reported on sample representativeness, potentially impacting the generalisability of findings.
While randomisation minimises the risk of bias, two of the included studies lacked adequate concealment of randomised group assignment, potentially introducing selection bias.18,21 Inadequate reporting quality was evident across all studies, with some failing to provide essential data on outcome measures and effect size. Reporting of effect size is important to establish not only the direction of the effect but also its size. 28 Quantifying the difference in outcomes between the intervention and control groups and placing emphasis on the size of that difference also provides a measurable means of establishing clinical significance. While statistical significance is important for interpreting research, understanding clinical significance is crucial to establishing outcomes that are meaningful to patients. 29 However, this component of the reporting subscale was only marked down on the Downs and Black quality assessment tool on the three studies that failed to provide enough data for effect size to be calculated on all their primary outcomes (Table 4). Furthermore, insufficient study power compromised the ability to draw accurate conclusions from the sample data, as evidenced by relatively small sample sizes and wide confidence intervals. Downs and Black summary score indicated good or excellent study quality for the six RCTs and fair quality for the cohort study. However, these relatively high scores, are misleading. A targeted assessment using the RoB2 tool for the primary outcome judged only one RCT to be at low risk of bias. Relying solely on global assessment of study quality risks masking critical biases across the studies and can lead to inaccurate conclusions about the credibility of study outcomes. 15 These limitations underscore the need for improved methodological rigour in future research on preoperative interventions in hand surgery.
Preoperative opioid education was examined in five of the included studies, all conducted in the United States.18–22 This focus is unsurprising given the magnitude of the ongoing opioid epidemic in the country, which originated from excessive prescription and misuse of pain medication. 30 Upper extremity surgeons in the United States commonly prescribe opioids for postoperative pain management, potentially in unnecessary quantities. 31 Despite efforts to curb access to prescription drugs following the introduction of the Centres for Disease Control and Prevention’s 2016 opioid prescribing guidelines, the issue persists. 32 While the UK is not facing the same opioid crisis, the effectiveness of educational interventions remains pertinent. If preoperative education can effectively reduce opioid consumption, similar intervention principles may be applied to other educational initiatives.
Despite three of the opioid studies evaluating very similar interventions assessed in terms of the same outcome measure, quantitative synthesis was not possible because outcomes were assessed over different time periods following surgery.
The opioid study that provided sufficient data for calculating the effect size for the number of pills consumed postoperatively, demonstrated an intervention effect showing over a 34% reduction in opioid consumption compared to the control group (Table 4). Consensus-based recommendations for initiating opioid tapering has been recommended as five to 10 percent of MEU every one to 4 weeks. 33 This difference exceeds consensus-based recommendations for opioid tapering, indicating clinical significance. However, due to the lack of data from other studies, the importance and relevance of effect size remain uncertain.
The only RCT in this review that did not report any intervention effect for any outcome, assessed a preoperative pain neuroscience education intervention. A point estimate of intervention efficacy was calculated from the data provided (Table 4). Núñez-Cortés et al. 24 concluded no intervention effect based on finding no statistically significant difference between groups. However, the lack of statistically significant difference could be attributed to insufficient study power, as indicated by the wide confidence intervals of all reported outcome measures. As a result, and despite rating this study highest among all included studies and the only one to receive a low risk of bias assessment, meaningful conclusions cannot be drawn from the results obtained.
Levels of patient satisfaction were the sole outcome reported for participants receiving only a preoperative intervention in the cohort study investigating the impact of conservative therapies on postoperative outcomes. 23 While this study reported higher satisfaction with treatment in the preoperative intervention group, it is crucial to note that this was an observational study. Without randomisation, any observed differences between groups cannot be conclusively attributed as causal effects of the intervention.
The studies in this review were unable to consistently demonstrate robust and statistically significant effects of preoperative interventions on postoperative outcomes across all evaluated measures and populations. Despite significant variations in study design, quality, and risk of bias among the included studies, a consistent finding across this review emerges: insufficient evidence. This gap may explain why the National Institute of Health and Care Excellence (NICE) currently lacks preoperative clinical guideline recommendations for elective hand surgery, unlike its clear recommendations for preoperative rehabilitation in hip and knee arthroplasty.26,34 Similarly, there is a dearth of guidance for shoulder replacements, with NICE instead calling for further research in this area. 34 This highlights the underexplored nature of preoperative interventions in upper limb surgery. By contributing to the existing body of evidence, this review emphasises the need for rigorous research to assess the effectiveness of preoperative interventions in elective hand surgery.
Considering the clinical implications of this study, several key recommendations emerge. Firstly, the lack of robust evidence emphasises the critical need for clinicians to approach preoperative care in hand surgery cautiously, acknowledging the absence of clear guidelines or strong evidence-based recommendations. Patient-centred care is crucial, with a focus on shared decision-making and comprehensive patient education to optimise postoperative outcomes.
Moreover, this review underscores the necessity for increased emphasis on conducting high-quality research in this domain. Clinicians should prioritise participation in well-designed studies that rigorously evaluate the efficacy and safety of various preoperative strategies. By supporting such research endeavours, clinicians can contribute to bridging existing knowledge gaps and advancing towards evidence-based practices.
Limitations
This study is not without limitations. The exclusion of non-English journal articles presents the possibility of selection bias. Although all included studies were classified as either fair, good or excellent on assessment of study quality, all bar one study was judged to be at least at some risks to bias. Reasons for bias include failure to blind participants, absence of intervention assignment concealment and lack of provision of a sample size calculation. The absence of a reported effect size estimate, along with a precision of that estimate, and the resultant reliance on the p value for statistical analysis means the effect of the intervention and its relevance cannot be judged. The potential for publication bias should also be considered, as studies with negative or inconclusive results may be underreported. Finally, the lack of standardised protocols and outcome measures across studies makes it challenging to establish consistent and reliable conclusions. Varying levels of detail in reporting further complicate the assessment of the interventions’ true impact.
These limitations collectively reduce the quality of the assessed evidence, affecting the ability to draw reliable conclusions. Therefore, study findings should be interpreted with caution, and there is a clear need for more rigorous, well-designed studies in this area to provide stronger evidence and more definitive recommendations.
Conclusion
The aim of this systematic review was to explore the effect of preoperative interventions on postoperative recovery following elective hand surgery. Using a GRADE approach to evidence rating 35 the results compiled for this review indicate very low-quality evidence, suggesting very little confidence in any effect size demonstrated. The small number of available studies highlights the need for further research.
Future researchers are advised to carefully consider the clinical significance of effect sizes prior to data collection and analysis, facilitating clearer interpretation of results. Additionally, establishing consensus on appropriate outcome measures, follow-up intervals, and protocols before evaluating combinations of preoperative interventions following specified surgical procedures is crucial. This presents a significant opportunity for future research to generate high-quality evidence. While this study consolidates existing evidence and highlights gaps in knowledge, clinicians should interpret these findings as a call to action to drive research forward and refine clinical practices in preoperative interventions for elective hand surgery.
Supplemental Material
Supplemental Material - The effect of preoperative interventions on postoperative outcomes following elective hand surgery: A systematic review
Supplemental Material for The effect of preoperative interventions on postoperative outcomes following elective hand surgery: A systematic review by Tahra Babiker-Moore, Carol J Clark, Emma Kavanagh and Timothy B Crook in Journal of Hand Therapy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.