
Abstract
Background:
Patients with perihilar cholangiocarcinoma (pCCA) have high postoperative mortality and a poor prognosis. A reliable preoperative marker is needed to determine whether these patients are likely to benefit from surgical treatment.
Objectives:
This study aimed to verify the predictive value of preoperative albumin-bilirubin (ALBI) grades for 90-day mortality and long-term outcomes in these patients.
Methods and design:
This retrospective, multicenter, cohort study included patients with pCCA, surgically treated between January 2012 and December 2023. Patients were divided into ALBI 1–2 and ALBI 3 groups according to preoperative ALBI grade. Logistic and Cox regression analyses evaluated risk factors for 90-day death and overall survival (OS), respectively.
Results:
Of the 828 included patients, 243 (29.3%) had ALBI grade 3. In total, 744 (89.9%) and 89 (10.1%) patients underwent radical resection and palliative surgery, respectively. The 90-day mortality rate was 8.9% for the entire cohort and 16.5% for patients with ALBI 3, higher than that of ALBI 1–2 (5.8%). Age, extended hemihepatectomy, and ALBI 3 were independent risk factors for 90-day mortality. Patients with ALBI 3 had a higher postoperative intra-abdominal bleeding, bile leakage, and acute organ dysfunction. The median OS of patients with ALBI 3 (21.0 months) was shorter than that of ALBI 1–2 (29.0 months). In the radical resection subgroup, the median OS of ALBI 3 was 23.0 months, poorer than that of ALBI 1–2 (33.0 months).
Conclusion:
Preoperative ALBI grades can identify patients with pCCA who may benefit from surgical resection. Patients with ALBI 3 had a high risk of postoperative complications, 90-day mortality, and poorer long-term survival, and may benefit only marginally from surgical treatment.
Trial registration:
ChiCTR2500102958 (Medical Research).
Introduction
Perihilar cholangiocarcinoma (pCCA) has a poor prognosis, with a median overall survival (OS) of approximately 30 months after radical resection, and a 5-year survival rate of approximately 30%. 1 However, achieving curative surgery for pCCA is challenging because the tumor is located at the hepatobiliary and vascular confluence. The postoperative 90-day mortality of pCCA is approximately 20%, 2 ranking it one of the malignancies with the highest surgical mortality.
A preoperative index capable of evaluating postoperative mortality risk and long-term survival would have significant clinical value in determining which patients with pCCA may benefit from surgical treatment. The Child-Pugh (C-P) classification remains an important standard for assessing hepatic resection risk. However, its preoperative utility in pCCA is limited; most pCCA patients lack cirrhosis and instead exhibit hyperbilirubinemia-predominant hepatic injury, a profile poorly reflected in the C-P scoring. 3 Similarly, the indocyanine green retention rate at 15 min, despite being valuable for assessing the functional liver reserve, demonstrates compromised accuracy in obstructive jaundice. Consequently, the indocyanine green retention rate at 15 min is generally avoided in hyperbilirubinemic cases. 4 Several studies have developed prognostic models incorporating variables such as lymph node status, vascular invasion, and tumor differentiation; however, these postoperative parameters make them unsuitable for preoperative risk assessment.5–7 The albumin-bilirubin (ALBI) grade is an evaluation system based on serum albumin and bilirubin levels and has been verified as a discriminatory model to assess liver function in patients with hepatocellular carcinoma. 3 An elevated level of bilirubin is the main characteristic of pCCA and is a key factor that affects hepatic reserve; hence, the ALBI grade may be a potential indicator for liver function assessment in patients with pCCA.
In this study, we aimed to analyze the 90-day postoperative mortality and long-term survival in patients with pCCA undergoing surgical treatment to determine which patient subgroups are most likely to benefit from surgical intervention and thereby optimize clinical decision-making.
Patients and methods
Patient selection
The reporting of this study conforms to the STARD 2015 guideline: an updated list of essential items for reporting diagnostic accuracy studies statement. 8 All patients who underwent surgical treatment, including radical resection or palliative surgery, for pCCA between January 2012 and December 2023 at three hospitals (Zhengzhou University People’s Hospital, Affiliated Cancer Hospital of Zhengzhou University, and Southwest Hospital) were enrolled. The study was approved by the Ethics Committees of all participating hospitals and conducted in accordance with the Declaration of Helsinki. The requirement for obtaining individual informed consent was waived by the Ethics Committee of Zhengzhou University People’s Hospital (Approval No. 2024-137). Trial Registration: ChiCTR2500102958 (Medical Research). Patients were excluded if they had coexisting malignant tumors that affected their lifespan or incomplete follow-up information.
Data collection
Personal information, medical history, and laboratory indicators were collected from the medical archives. Personal information collected included age, sex, and body mass index. Medical history included diabetes, cardiovascular diseases, and surgical information (operative duration and perioperative bleeding). The laboratory indicators included preoperative alanine aminotransferase, albumin, total bilirubin, and carbohydrate antigen 19-9. ALBI index was calculated using the following equation: (log10 bilirubin µmol/L × 0.66) + (albumin g/L × −0.085). The ALBI grade was defined as grade 1 (<−2.60), grade 2 (−2.60 to −1.39), and grade 3 (>−1.39). For patients who underwent percutaneous transhepatic cholangial drainage (PTCD), the ALBI grade was reanalyzed using the albumin and total bilirubin obtained 1 week after PTCD.
Definitions and outcomes
Radical resection included partial or no liver resection, hemihepatectomy, and extended hemihepatectomy with R0 or R1 resection margins. Palliative surgery was defined as choledochojejunostomy, with or without liver resection and R2 resection margins. The Bismuth–Corlette classification was defined in accordance with the ESMO Clinical Practice Guidelines. 9 Left and right hemihepatectomy were classified as H234 and H5678, respectively, based on the “New World Terminology.” 10 In addition, extended left and extended right hemihepatectomy were defined as described in our previous publication. 11 Furthermore, 90-day mortality was defined as death within 90 days of surgery. The major postoperative complications were defined as ⩾grade III based on the Clavien–Dindo classification. 12 OS was defined as the interval between surgery and the date of death or last follow-up.
Statistical analysis
Statistical analyses were conducted using IBM Statistical Package (IBM, Chicago IL) for the Social Sciences version 22.0 and R 4.2.3. (R Development Core Team, Vienna, Austria) Normal distribution was assessed using the Shapiro–Wilk test for continuous variables. Non-normally distributed continuous variables were analyzed using Mann–Whitney U tests and reported as median and interquartile range (IQR). Qualitative variables were analyzed using the Chi-square test and reported as numbers and percentages (%). Logistic regression analysis was used to predict the 90-day mortality. Risk ratios were presented as odds ratios (OR) and 95% confidence intervals (CIs). Cox proportional hazards regression analysis was used to assess the factors predicting OS. Risk ratios are reported as hazard ratios (HRs) and 95% CI. p < 0.05 was considered statistically significant.
Results
Patient characteristics
In total, 1023 patients diagnosed with pCCA were selected from the registry. After 195 patients were excluded for recurrent cholangiocarcinoma (23), coexisting other active malignant tumors (15), distant metastases (26), and incomplete follow-up information (131), 828 patients were enrolled in the analysis. The median patient age was 65 (56–70) years. The 90-day mortality rate was 8.9% (74 of 828), and the median OS was 24.5 months. Among them, 257 (31.0%) patients had ALBI 3, 439 (53.0%) had C-P grade B, 744 (89.9%) underwent radical resection, 322 (38.9%) underwent hemihepatectomy, 56 (6.8%) underwent extended hemihepatectomy, 146 (17.6%) had Bismuth–Corlette IV, and 230 (27.8%) underwent PTCD.
The baseline patient characteristics are shown in Table 1. Compared with patients with ALBI 1–2, patients with ALBI 3 had an older age of 67 (IQR 60–71), a higher rate of PTCD (40.9%), and a higher carbohydrate antigen 19-9 level (269.7 (IQR 118.7–784.0) U/mL).
Comparative baseline characteristics of patients with different ALBI grades in perihilar cholangiocarcinoma.
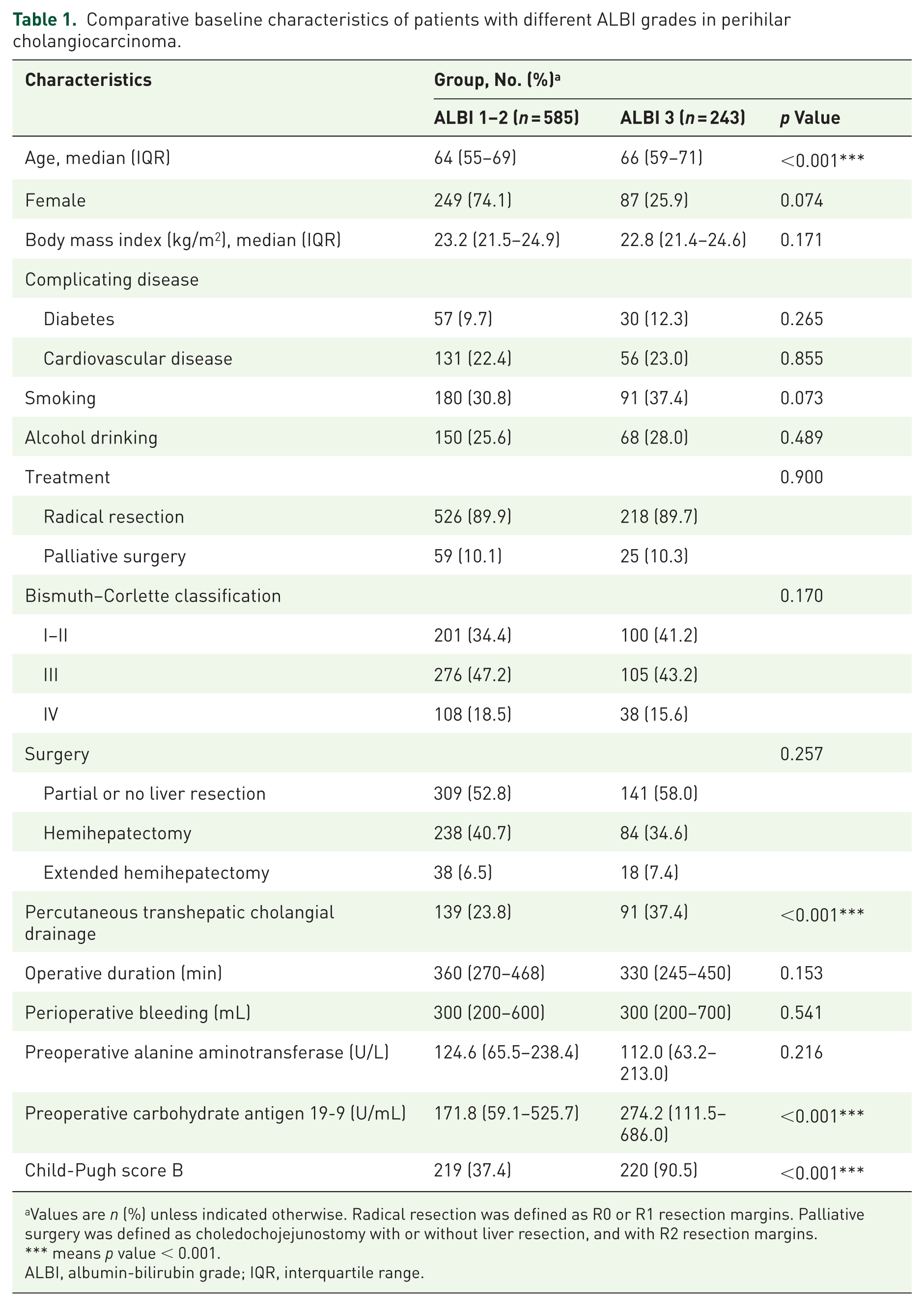
Values are n (%) unless indicated otherwise. Radical resection was defined as R0 or R1 resection margins. Palliative surgery was defined as choledochojejunostomy with or without liver resection, and with R2 resection margins.
means p value < 0.001.
ALBI, albumin-bilirubin grade; IQR, interquartile range.
Risk factors analysis for 90-day mortality
In the entire cohort, the 90-day mortality rate of C-P grade B (11.6%) was higher than that of grade A (5.7%), p < 0.001. The 90-day mortality rate of ALBI 3 was 16.3%, which was higher than that of ALBI 1–2 (5.6%; p < 0.001). Patients who underwent extended hemihepatectomy had the highest 90-day mortality (19.6%), followed by patients who underwent hemihepatectomy (9.9%) and those who underwent partial or no liver resection, p = 0.005.
Univariable and multivariable logistic regression analyses showed that age (OR = 1.04, 95% CI: 1.01–1.07), extended hemihepatectomy (OR = 3.11, 95% CI: 1.34–7.23), and ALBI 3 (OR = 2.57, 95% CI: 1.36–4.82) were independent risk factors for 90-day mortality (Table 2). C-P grade B was not an independent risk factor for 90-day mortality.
Univariable and multivariable logistic regression analyses of 90-day mortality (n = 828).

Values in parentheses are 95% confidence intervals.
means p value < 0.05, ** means p value < 0.01, *** means p value < 0.001.
ALBI, albumin-bilirubin grade; OR, odds ratio.
Multivariable logistic regression analyses of risk factors associated with 90-day mortality in patients receiving radical resection (n = 744) showed that age (OR = 1.05, 95% CI: 1.02–1.08, p = 0.002), extended hemihepatectomy (OR = 3.50, 95% CI: 1.57–7.81, p = 0.002), and ALBI 3 (OR = 2.53, 95% CI: 1.32–4.79, p = 0.005) were independent risk factors (Table 3). The 90-day mortality rate of patients with ALBI 3 was 17.6%, which was higher than that of ALBI 1–2 (5.9%) who underwent radical resection, p < 0.001. In patients who underwent palliative resection, Age and ALBI 3 were not independent risk factors for 90-day mortality.
Univariable and multivariable logistic regression analyses of factors associated with 90-day mortality in patients receiving radical resection (n = 744).

Values in parentheses are 95% confidence intervals.
means p value < 0.01, *** means p value < 0.001.
ALBI, albumin-bilirubin grade; OR, odds ratio.
Postoperative complications analysis
The morbidity rates of intra-abdominal infection, intra-abdominal bleeding, bile leakage, and acute organ dysfunction within 90 days after surgical treatment in patients with ALBI 3 were 13.6%, 8.9%, 16.3%, and 10.9%, respectively, which were significantly higher than those in patients with ALBI 1–2 (6.3%, 4.4%, 8.2%, and 2.6%, respectively; Supplemental Table 1).
The effect of PTCD on 90-day mortality of patients with ALBI 3
A total of 257 patients were classified into the ALBI 3 group according to serum albumin and bilirubin levels before PTCD treatment. The 90-day mortality showed no statistical difference between patients who underwent PTCD (16.2%) and those who did not undergo PTCD (16.4%, p = 0.956).
Further analysis showed that 47.6% patients with ALBI 3 pre-PTCD showed improvements and were classified into ALBI 2 after PTCD. However, 28.8% patients with ALBI 1–2 pre-PTCD progressed to ALBI 3 after PTCD. Serum bilirubin levels decreased from 250.1 (178.8–365.7) to 137.8 (76.6–215.9) μmol/L following PTCD treatment, p < 0.001. Similarly, serum albumin levels showed a decrease following PTCD, from 35.6 (32.0–39.1) to 34.2 (30.6–38.0) g/L, p = 0.033 (Supplemental Table 2).
Long-term OS analysis
Patients with OS >90 days (n = 754) were selected to analyze long-term OS. The median OS was 26.0 (95% CI: 22.9–29.1) months, the 1-year OS rate was 72.1%, and the 5-year OS rate was 9.4%. In patients who underwent radical resection, the median OS was 31.7 (95% CI: 28.1–35.3) months, the 1-year OS rate was 76.9%, and the 5-year OS rate was 11.1%.
Univariable and multivariable Cox regression analyses showed that patients who underwent radical resection had a better OS (HRs = 0.12, 95% CI: 0.09–0.16, p < 0.001). The independent risk factors for OS were age (HRs = 1.01, 95% CI: 1.00–1.02, p = 0.022) and ALBI 3 (HRs = 1.37, 95% CI: 1.12–1.67, p = 0.002; Table 4). In the radical resection subgroup, ALBI 3 was an independent risk factor for OS with HRs of 1.30 (95% CI: 1.03–1.64), p = 0.026.
Univariable and multivariable survival analyses of factors associated with overall survival of patients with perihilar cholangiocarcinoma (n = 754).

Values in parentheses are 95% confidence intervals.
means p value < 0.05, ** means p value < 0.01, *** means p value < 0.001.
ALBI, albumin-bilirubin grade; HR, hazard ratios.
In the total cohort with OS >90 days, patients with ALBI 3 had worse OS of 20.0 (95% CI: 16.8–23.2) months compared with 30.3 (95% CI: 26.6–34.0) months in patients with ALBI 1–2, p = 0.001 (Figure 1(a)). In the radical resection subgroup, the median OS of ALBI 3 was 23.0 (95% CI: 20.4–25.6) months, which was worse than that of ALBI 1–2 of 34.0 (95% CI: 30.6–37.4) months, p = 0.002 (Figure 1(b)).

Kaplan–Meier survival analysis curves of patients with perihilar cholangiocarcinoma according to ALBI grade. (a) Kaplan–Meier curves of the total patients with OS >90 days (n = 754). (b) Kaplan–Meier curves of patients who underwent radical resection with OS >90 days (n = 673).
Discussion
Patients with pCCA usually have poor liver function due to obstructive jaundice, which may result in postoperative mortality when surgical resection is performed. Previous studies have reported a 30-day mortality rate of 5%, a 90-day mortality rate of 13%, and postoperative complications ranging from 26% to 68% in patients with pCCA.13,14 In this study, we analyzed 828 patients with pCCA who underwent surgery, and our results showed the following: 90-day mortality rate, 8.9%; median OS, 24.5 months; and extended hemihepatectomy resulted in the highest 90-day mortality risk, 19.6%. In the radical resection subgroup, the median OS (31.7 months), 1-year OS (76.9%), and the 5-year OS rate (11.1%) were similar to previous studies.2,13–15
The ALBI grades screened a more accurate group of patients with ALBI grade 3 (29.3%) than those with C-P grade B (53.0%), which was consistent with a report that the ALBI grade was more accurate in predicting postoperative liver failure and OS than the C-P grades in patients with hepatocellular carcinoma. 16 Most patients with pCCA do not have liver cirrhosis. Bilirubin and albumin were the two most prominent factors in liver function tests. Persistently high bilirubin levels affect the mitochondrial function of liver cells and inhibit liver regeneration capacity. 17 Hypoalbuminemia leads to tissue edema and delayed anastomotic healing, which increases the risk of bile leakage and bleeding. Albumin is associated with anti-inflammatory effects and organ failure morbidity.18,19 Thus, ALBI grades provide a superior assessment of liver function compared with C-P scores. In this study, the 90-day mortality rate of patients with ALBI grade 3 was 16.5% in the total cohort, which attained 17.9% in patients receiving radical resection, more than double the rate observed in ALBI grade 1–2 (5.8%).
This mortality differential persisted in long-term outcomes, where patients with ALBI 3 experienced a clinically significant 8-month reduction in median OS (21.0 vs 29.0 months), even in patients achieving radical resection (23.0 vs 33.0 months). Patients with an ALBI grade of 3 had high carbohydrate antigen 19-9 levels. This indicates that the ALBI grade may reflect the tumor burden and invasiveness. Moreover, patients with ALBI 3 experienced a higher incidence of postoperative complications, which often delayed or hindered the timely implementation of subsequent adjuvant treatments that might improve the survival of patients with pCCA. 20 Patients with ALBI grade 3 have limited resection margins, and the functional reserve of the residual liver after surgery is relatively poor. Inflammatory and immunosuppressive states in the liver microenvironment may contribute to tumor recurrence and metastasis. 21 Therefore, for patients with ALBI 3 and other high-risk factors (such as advanced age and requiring extended hemihepatectomy), nonsurgical options should be prioritized, such as stent placement to relieve biliary obstruction, combined with systemic therapy as the initial treatment. 22
Notably, among patients with ALBI 3 in this study, PTCD did not decrease 90-day mortality. This may be attributed to the fact that although serum bilirubin levels decreased significantly after PTCD treatment, serum albumin levels also declined. In fact, 28.8% patients with ALBI 1–2 before PTCD progressed to ALBI 3 during bilirubin drainage. Malnutrition has been shown to correlate with a high incidence of postoperative complications and mortality in patients with liver cancer. 23 Therefore, nutritional support should be considered an essential part of perioperative treatment in patients who have undergone PTCD and are planned for radical resection. Moreover, neoadjuvant therapy may be an appropriate alternative for patients with ALBI 3. A systematic review summarizing seven studies of patients with pCCA who underwent neoadjuvant chemoradiotherapy suggested potential benefits in terms of R0 resection rate and pathological complete response. However, the precise role of neoadjuvant chemotherapy in pCCA remains uncertain and requires further robust evidence. 24 Our study had limitations inherent to its retrospective design and lack of standardized adjuvant therapy. Nevertheless, the multicenter design and large sample size provided robust real-world evidence.
Conclusion
Preoperative ALBI grade serves as a strong indicator to distinguish patients with pCCA who benefit from surgery from those who are at risk of operative morbidity without survival gain. ALBI 3 identifies a vulnerable subgroup with 2.6-fold higher 90-day mortality and limited survival benefits for radical resection. Future trials should test neoadjuvant approaches in high-risk patients with ALBI to convert them into surgical candidates.
Supplemental Material
sj-docx-1-tam-10.1177_17588359261417647 – Supplemental material for Value of albumin-bilirubin grade for 90-day mortality and long-term outcomes in patients with perihilar cholangiocarcinoma: a multicenter retrospective cohort study
Supplemental material, sj-docx-1-tam-10.1177_17588359261417647 for Value of albumin-bilirubin grade for 90-day mortality and long-term outcomes in patients with perihilar cholangiocarcinoma: a multicenter retrospective cohort study by Qiankun Luo, Huiyuan Tian, Zhipeng Liu, Zhiyu Chen, Xianzhou Zhang and Tao Qin in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.