
Abstract
Uterine malignancies represent a broad and heterogeneous group of neoplasms, which collectively account for the majority of gynaecological malignancies in developed countries. For a significant proportion of these, mortality rates and clinical outcomes are of major concern, owing to complex molecular profiles and aggressive phenotypes that are largely refractory to conventional therapeutic approaches. Recent advancements in precision medicine and the development of targeted therapies have been transformative for several common cancer types; however, the same benefits are yet to be realised for many uterine cancers. This review comprehensively details the diverse molecular features characterising the various subtypes of uterine malignancies. Furthermore, we have examined the therapeutic approaches actively investigated to target these unique molecular features, identifying pathways and treatments that offer the greatest potential patient benefit. Among increasingly personalised strategies, particular promise is shown by HER2-targeted therapies for HER2-positive malignancies (e.g. trastuzumab deruxtecan). Additionally, targeting TP53 wild-type tumours with selinexor, as well as addressing AKT and DNA repair pathways in both uterine carcinomas and sarcomas (i.e. AKT inhibitor and poly(ADP-ribose) polymerase inhibitor combinations), represents key advancements. Furthermore, anti-angiogenic and immune checkpoint inhibitor combinations hold significant promise for future therapeutic strategies.
Plain language summary
Uterine malignancies represent a common and complex group of cancers affecting many individuals. Unfortunately, a significant proportion of these are very aggressive and challenging to treat with standard methods. Recent progress in matching treatments based on DNA and molecular changes in individual malignancies have been transformative for several common cancer types, however the same benefits are yet to be shown for many uterine malignancies. In this review, we explore new treatments that are currently being studied to specifically target these genetic and molecular features, highlighting the personalised approaches that show the most promise for patients.
Keywords
Background of uterine malignancies
Pathological subtypes and incidence
Uterine malignancies collectively account for the majority of gynaecological cancers in developed countries (second to cervical cancers, when considered globally). 1
The uterus comprises three tissue layers: (i) the perimetrium (mucus layer protecting the outside of the uterus); (ii) the myometrium (muscular middle layer) and (iii) the endometrium (inner lining which is shed during menstruation). 2 The vast majority of uterine malignancies originate from the endometrium (approximately 95% of cases), arising from epithelial cells and are classified into four histological types: (i) endometrioid carcinomas (EC; 83%–86%), (ii) uterine serous carcinomas (USC; 4%–6%), (iii) uterine carcinosarcomas (UCS; 4%–7%) and (iv) clear cell endometrial carcinomas (CCEC; 1%–4%). 3 Malignant cells of origin from the myometrium have a mesenchymal derivation and are histologically classified as (i) uterine leiomyosarcoma (uLMS; 60%–80%), (ii) uterine adenosarcoma (UAS; 5%–9%), (iii) uterine stromal sarcoma (USS; previously low-grade USS; 6%–20%) and (iv) undifferentiated uterine sarcoma (UUS; previously high-grade USS; 5%), with the remaining 5% being made up of rarer subtypes such as uterine perivascular epithelioid cell tumour (PEComa).4,5 These uterine myometrial malignancies, collectively referred to as uterine sarcomas, are rare and account for just 3%–8% of all uterine malignancies.4,6
Survival rates
Patients with EC generally have a favourable prognosis, with a 5-year survival (5-YS) rate exceeding 90%, as the majority have usually not spread beyond the uterus. 3 Patients with the remaining, rarer types of uterine malignancies (USC, UCS and CCEC), unfortunately often face much poorer prognoses owing to aggressive and highly invasive phenotypes with numerous genetic aberrations. This, combined with late-stage diagnosis (~70% of non-EC endometrial cancers are FIGO Stage III/IV at diagnosis) and therapy resistance, results in 5-YS rates of only 18%–62% for non-EC endometrial carcinomas.1,7 Notably, confinement of endometrial carcinoma to the uterus is an important determinant for patient prognosis, as extrauterine invasion is associated with significantly poorer survival outcomes for all patients. For all types of endometrial cancer, the overall 5-YS rate falls to 70% (from 95%) with regional extrauterine invasion, with a 5-YS rate as low as 19% for metastatic disease. 8
Prognosis for uterine sarcomas is also dependent on histological subtype and grading, with the 5-YS for USS and UAS being 96% and 80%, respectively, whereas for UUS and uLMS, 5-YS is only 43% and 38%, respectively. 9 This is largely attributable to the poor differentiation and high grade of these types of uterine malignancies, which contribute to increased invasiveness and frequent late-stage diagnosis. As for carcinomas, 5-YS outcomes for sarcomas are generally worse when extrauterine invasion is involved. The 5-YS rate for all uterine sarcoma types (excluding USS) ranges between 60% and 70% where the malignancy is localised to the uterus, but falls to 37% where regional invasion has occurred, and 12%–18% for metastatic disease. 8
Current standard treatment strategies
Current first-line treatment for endometrial cancer, depending on the stage and subtype, includes surgery and radiotherapy, often with concurrent radio-sensitising platinum-based chemotherapy, which may be followed by carboplatin + paclitaxel chemotherapy, with or without anti-angiogenic therapy, immunotherapy (i.e. immune checkpoint inhibitors; ICI) or hormone therapy. 10 Surgery alone often suffices for well-differentiated and non-advanced endometrial carcinomas (most commonly the EC subtype), conferring excellent prognosis. 3 Aggressive subtypes and the presence of extrauterine disease require the addition of chemotherapy and/or radiation. 10 Hormone therapy, like megestrol acetate, may palliate advanced endometrial carcinomas, although likely benefiting individuals with EC only due to hormone receptor expression.3,7 First-line treatment for metastatic mismatch repair deficiency (MMRd)/microsatellite instability (MSI) endometrial cancer (common in EC and CCEC) now includes an ICI (pembrolizumab or dostarlimab) with carboplatin–paclitaxel, based on recent trials. 10 In the second-line setting (excluding prior ICI), pembrolizumab plus lenvatinib is approved, though some regions restrict this to mismatch repair proficient (MMRp)/microsatellite stable (MSS) due to distinct approvals for MMRd/MSI-H disease. 10 Specific trial results will be discussed in detail below and are summarised in Table 4.
For uterine sarcomas, surgery (total hysterectomy and bilateral salpingo-oophorectomy) is the standard of care. 11 Adjuvant radiation, chemotherapy, hormone therapy and immunotherapy are frequently used, but evidence for their statistically significant benefit is limited, preventing their universal standard-of-care designation. 11 Chemotherapeutic options include anthracyclines (e.g. doxorubicin), nucleoside analogues (e.g. gemcitabine), DNA alkylating agents (e.g. ifosfamide dacarbazine, temozolomide and trabectedin) and taxanes. 11
This review aims to provide a critical summary of the molecular characterisation of uterine malignancies and the evidence of matched treatments from clinical trial data, highlighting those therapies that have shown tangible improvements in patient outcomes.
Genomic landscape of uterine malignancies
Classification of endometrial carcinomas into four new molecular categories has allowed a greater clinical understanding of prognosis and potentially of therapeutic susceptibility: (i) Polymerase epsilon (POLE) ultramutated, (ii) MSI hypermutated, (iii) copy-number low and (iii) copy-number high. The POLE-ultramutated group had the best progression-free survival (PFS), followed by the MSI hypermutated group and the copy number low group, respectively, while the copy number high group had the worst PFS. 12 Uterine malignancies generally exhibit a high degree of molecular complexity and a significant number of molecular aberrations. While the specific genomic alterations relevant to each type differ somewhat, recurring patterns of genomic alterations include mutations in tumour suppressor genes such as PTEN and TP53, activation of oncogenes such as PIK3CA and KRAS, and significant chromosomal alterations where gains or losses of entire chromosome regions are observed. 13 Specific molecular alterations for each type of uterine malignancy are summarised in Tables 1–3.
Frequencies of SNVs across uterine malignancy types.

Due to a small number of cases in some studies, some mutation frequencies may be abnormally high.
CCEC, clear cell endometrial carcinoma; EC, endometrioid carcinoma; NR, not reported; PEComa, perivascular epithelioid cell tumour; SNVs, small nucleotide variants; UAS, uterine adenosarcoma; UCS, uterine carcinosarcoma; uLMS, uterine leiomyosarcoma; USC, uterine serous carcinoma; USS, uterine stromal sarcoma; UUS, undifferentiated uterine sarcoma.
Gene amplification frequency in uterine malignancies.

Due to a small number of cases in some studies, some amplification frequencies may be abnormally high.
CCEC, clear cell endometrial carcinoma; EC, endometrioid carcinoma; NR, not reported; UAS, uterine adenosarcoma; UCS, uterine carcinosarcoma; uLMS, uterine leiomyosarcoma; USC, uterine serous carcinoma; USS, uterine stromal sarcoma; UUS, undifferentiated uterine sarcoma.
Gene deletion frequency in uterine malignancies.
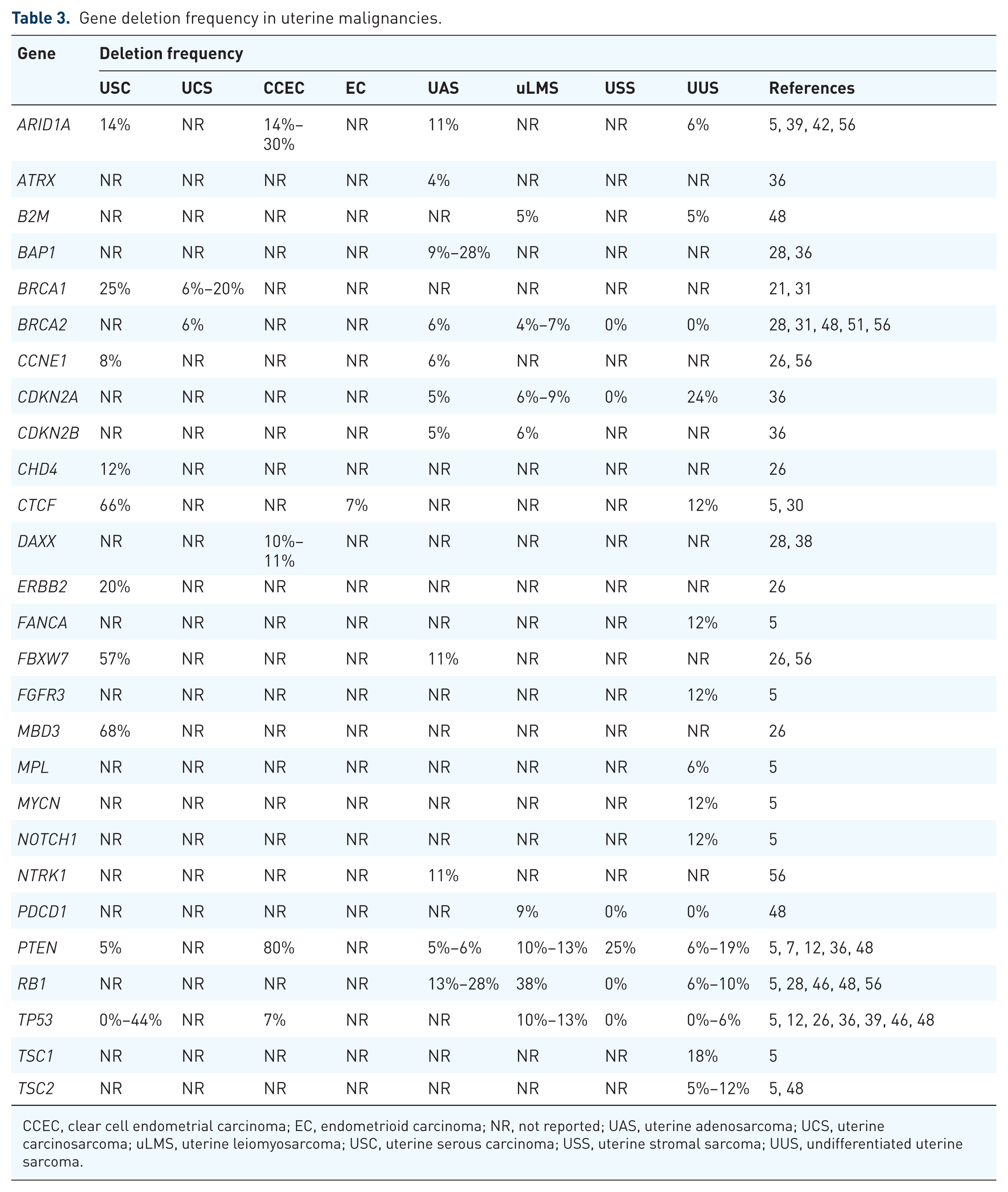
CCEC, clear cell endometrial carcinoma; EC, endometrioid carcinoma; NR, not reported; UAS, uterine adenosarcoma; UCS, uterine carcinosarcoma; uLMS, uterine leiomyosarcoma; USC, uterine serous carcinoma; USS, uterine stromal sarcoma; UUS, undifferentiated uterine sarcoma.
The risk of developing endometrial cancer is doubled with a family history of endometrial cancer, 13 and individuals with Lynch syndrome (germline mutations in MLH1, MSH2, MSH6, PMS2, EPCAM or TGFBR2) face a 20%–70% lifetime risk, 14 accounting for 3%–5% of uterine carcinoma cases. 13 Cowden syndrome (germline PTEN mutations) also elevates risk (25%–30% lifetime). 15 Other gene alterations associated with increased risk include POLD1, POLE and BRCA1.12,16
Key mutations in the EC type of uterine malignancy occur in PTEN (54%–85%), PIK3CA (40%–60%), PIK3R1 (37%–50%), ARID1A (25%–50%), KRAS (16%–40%), CTNNB1 (23%–27%) and TP53 (10%–26%).7,13,14,17,18 Generally, copy number changes are not common, but PIK3CA (12%) and CCNE1 (6%) are the most commonly amplified genes.19,20 MSI, indicative of MMRd, is detected in 25%–40% of EC. 13 Hormone receptor (oestrogen and progesterone) expression is common, reflecting their role in EC pathogenesis.3,7
The aggressive USC type of endometrial cancer shares several similarities with high-grade serous ovarian carcinoma (HGSOC), basal-like breast cancer (BLBC) and triple-negative breast cancer (TNBC), including frequent alterations in TP53 (67%–90%) and extensive chromosomal instability with significant copy number alterations (CNAs) and loss of heterozygosity.12,16 MMRd and MSI are rare (2%). 12 Besides TP53, frequently mutated genes include PPP2R1A (20%–43%), PIK3CA (16%–35%), ATM (25%), FBXW7 (20%), CHD4 (20%) BRCA1 (11%–50%).7,21 –27 Amplifications in USC are common, including PIK3CA (45%–52%), CCNE1 (22%–45%), ERBB2 (13%–44%), MYC (40%) and CHD4 (28%).7,26,28,29 While less frequent than in HGSOC and BLBC, USC often displays features of Homologous Recombination Deficiency (HRD), or defective DNA repair, such as alteration in HR genes (i.e. BRCA1 and BRCA2) or presence of mutational signature 3. 16 The optimal method and cut-off for classifying a USC malignancy as being HRD has not yet been validated. Additional common deletions found in USC involve MBD3 (68%), CTCF (66%), FBXW7 (57%) and TP53 (0%–44%).12,26,30
The mutational profile of UCS overlaps with EC and USC, with mutations commonly found in TP53 (53%–90%), PTEN (19%–47%), PIK3CA (28%–41%), FBXW7 (11%–40%), MLL3 (29%), KRAS (10%–29%), PPP2R1A (13%–28%), RAD51D (25%) and ARID1A (13%–25%).7,13,17,21,25,28,31–37 Frequent amplifications occur in CCNE1 (42%–45%), MDM2 (38%), SOX17 (25%) and ERBB2 (8%–20%), and BRCA1 deletions are reported to occur in 6%–20% of UCS cases.7,19,21,28,29,31,34 Mutational signature 3 is dominant in ~7% of UCS cases, while MMRd occurs in 3%–6% of cases. 16
CCEC has limited genomic data. Frequently mutated genes include TP53 (29%–47%), PIK3CA (14%–40%), PPP2R1A (16%–37%), FBXW7 (27%), ARID1A (7%–27%), PIK3R1 (16%–23%) and KMT2D (20%),7,17,25,38–40 with MMRd rates of 10%–20%. 41 Frequently amplified genes include CCNE1 (17%–18%) and ERBB2 (9%–16%), and frequently deleted genes include PTEN (80%), ARID1A (14%–30%) and DAXX (10%–11%).7,12,28,38,39,42,43 CCEC resembles several features of clear cell ovarian carcinoma, including low hormone receptor expression and frequent expression of PD-L1. 41
Uterine sarcomas generally exhibit a lower mutational burden than endometrial carcinomas, but are associated with higher rates of recurrence, metastasis and mortality.44,45 uLMS frequently harbours mutations in TP53 (46%–67%), RB1 (10%–42%), ATRX (31%), PTEN (5%–16%) and MED12 (10%–13%).25,36,46–48 uLMS exhibits high-level CNAs and chromothripsis/chromoplexy, in conjunction with reduced inflammatory response gene expression and low leukocyte fraction.44,49,50 Deletions can occur in RB1 (38%) and in PTEN and TP53 (both 10%–13%).28,36,48 In addition, HR pathway aberrations are seen in up to 13% of uLMS, and dominant COSMIC mutational signature 3 is observed in ~25%.51,52 Promoter methylation of BRCA1 or RAD51C in uLMS has not been reported to date. 50 MMRd is reported in 22% of uLMS, and hormone receptor expression is common (40%–80%). 44
Genomic analyses of UAS reveal common mutations in KMT2C (36%–52%), AHNAK (28%–42%), MAGEC1 (34%–37%), DCHS2 (31%), MDM2 (26%), ATRX (5%–22%), TP53 (24%) and BCOR (21%).36,46,53–55 The PTEN/AKT/PI3K pathway is frequently altered (72%), suggesting a potential therapeutic avenue. 56 Amplifications of MDM2 (10%–27%), CDK4 (22%) and TERT (21%) have been reported, as well as deletions of RB1 (13%–28%) and BAP1 (9%–28%).28,36,46,48,56,57
USS frequently express hormone receptors and have recurrent chromosomal translocations involving JAZF1.11,58 Variants in MDM2 (9%), PTEN (9%) and TP53 (0%–6%) have been reported, with MMRd in 14% of cases.36,48,58 Amplification of CDK4 (25%) and MDM2 (25%) and deletion of PTEN (25%) have also been described.36,48 UUS are also characterised by chromosomal translocations, with the gene rearrangement YWHAE::NUTM2 (previously known as YWHAE::FAM22) being the most common. 45 Neurotrophic tyrosine receptor kinase (NTRK) gene fusions have also been observed in various case reports for UUS, however the frequency is not reported. 59 Other frequent mutations occur in TP53 (14%–37%), RB1 (5%–21%), PTEN (5%–12%) and NF1 (17%), and amplification of RIT1 (24%) and deletion of CDKN2A (24%) and PTEN (6%–19%) have been reported.25,36,45,48 MMRd rates in UUS vary (1%–25%), and they are usually CD10, ER and partial response (PR) negative.11,45
Uterine PEComas express HMB45 and/or Melan-A and limited genomic data generally (not specific to uterine cases) suggests frequent mutations in TP53 (15%), TSC2 (35%), TSC1 (10%–45%) and ATRX (15%).5,60
Molecularly matched therapies for uterine malignancies
Molecular profiling offers opportunities for targeted therapies in uterine malignancies. In endometrial carcinomas, MMRd/MSI-H and POLE-mutated tumours may respond to ICIs.61,62 HER2-directed therapies are relevant for p53-mutant/HER2-positive malignancies (frequently USC, UCS, CCEC and UAS), while other actionable co-alterations, including vulnerabilities in cell cycle regulation or DNA damage response (DDR) pathways, are potentially targetable with DDR inhibitors (DDRi), including Poly(ADP-ribose) polymerase (PARP) inhibitor therapy (PARPi).63,64 The RAINBO trials aim to answer many of these questions by stratifying therapy based on the endometrial carcinoma molecular subgroups: ICI (MMRd-GREEN), de-escalation for POLE ultra-mutated (POLEmut-BLUE, TAPER trial), hormonal therapy for no specific molecular profile (NSMP-ORANGE) and the addition of maintenance olaparib following standard adjuvant chemoradiation (p53abn-RED). 65 Subgroup-specific outcome reporting helps refine treatment, especially for aggressive p53-mutant MMRp (HER2-negative) EC potentially benefiting from ICI-chemotherapy combinations. 66
In uterine sarcomas, the landscape is more complex. While hormonal therapy is relevant for ER/PR-positive USS and uLMS, its role in UUS is limited due to low hormone receptor expression.48,67,68 PARPi shows promise in uLMS, which frequently harbour BRCA1/2 or other HR gene disruptions (refer to Tables 1 and 3). PI3K/AKT/mTOR inhibitors are under investigation across uterine malignancies, including sarcomas, given the frequent dysregulation of this pathway.44,48 The role of ICIs in sarcomas is less defined, often requiring specific biomarker identification (i.e. high tumour mutational burden, specific fusion proteins). 62
Despite the limited application of targeted therapies in uterine malignancies thus far, the extensive mutational burden across the spectrum of the various subtypes, in conjunction with the marked genomic similarities between uterine malignancies and other cancer types, highlights the translational opportunities for several targeted therapies. Molecular stratification is crucial to personalise treatment and improve outcomes for uterine malignancy patients. This review will discuss clinical trials with 30 or more patients with uterine malignancies that showed potential for patient benefit, with a summary provided in Table 4. Some trials with fewer than 30 patients are also included because they led to larger, important follow-up trials or were deemed to have significant potential for patient benefit. Trials with underwhelming results were largely excluded unless their inclusion was necessary for providing a broader context.
Summary of clinical trials involving uterine malignancies and targeted therapies where clinical benefit has been observed.

This table summarises 30 clinical trials (phase I: 1; phase I/II: 3; phase II: 20; phase III: 6) which were examined in this review. We have included trials with at least 30 patients with uterine malignancies, along with some smaller trials that either served as a basis for important larger trials or were identified as having a significant potential for patient benefit. The number of evaluable patients with uterine malignancies in each trial (n) is indicated in parentheses in the third column of this table. Each clinical trial in this table includes a citation reference in the final column, with the year of publication provided in parentheses.
ADCs, antibody–drug conjugates; BICR, blinded independent central review; CI, confidence interval; CR, complete response; Dato-DXd, datopotamab deruxtecan; FAS, full analysis set; HR, hazard ratio; IHC, immunohistochemistry; IQR, interquartile range; MMRd, mismatch repair deficient; MMRp, mismatch repair proficient; MSI-H, microsatellite instability-high; MSS, microsatellite stable; NA, not available; NE, not evaluable; NR, not reached; ORR, objective response rate; OS, overall survival; PARP, poly(ADP-ribose) polymerase; PD-1, programmed cell death protein 1; PDGFR, platelet-derived growth factor receptor; PFS, progression-free survival; PR, partial response; SD, stable disease; T-DXd, Trastuzumab–deruxtecan; TKI, tyrosine kinase inhibitor; TROP2, trophoblast cell surface glycoprotein 2; UCS, uterine carcinosarcomas; USC, uterine serous carcinomas; VEGFR, vascular endothelial growth factor receptor.
Immunotherapy
The ICIs pembrolizumab and dostarlimab have been approved as first-line combination therapy with carboplatin and paclitaxel for advanced, persistent or recurrent endometrial carcinomas, which are MMRd/MSI-H. 10 These monoclonal antibody (mAb)-based drugs target the cell surface receptor, programmed cell death protein 1 (PD-1), blocking its interaction with PD-L1. 69 This stimulates immune reactivity and surveillance to promote a T-cell-mediated immune response. 69
Single-agent ICI
Several clinical trials have evaluated the ICIs, pembrolizumab or dostarlimab (PD-1 inhibitors; PD-1i), either as monotherapy or in combination therapies in endometrial cancers. Limited efficacy was shown for pembrolizumab as a monotherapy in previously treated, advanced, PD-L1-positive endometrial carcinoma in the phase Ib trial KEYNOTE-028 (NCT02054806), 70 with more encouraging results seen for those with previously treated, advanced endometrial carcinoma which was MMRd in the phase II trial KEYNOTE-158 (NCT02628067). 71 The GARNET phase I clinical trial (NCT02715284) of dostarlimab as a single agent in advanced previously treated endometrial cancer also demonstrated encouraging activity in the MMRd population, with limited benefit in the MMRp population, suggesting the necessity of exploring combination regimens. 72
ICI combined with chemotherapy
In a phase II study (NCT02549209), patients with Stage III or IV recurrent endometrial carcinoma treated with pembrolizumab, carboplatin and paclitaxel achieved a longer overall median PFS of 10.6 months (median PFS of 8.8 months vs not reached for MMRp vs MMRd, respectively). 73 These earlier trials led to three phase III trials of ICI in combination with chemotherapy in the first-line setting, two of which have reported results. The NRG-GY018 phase III trial (NCT03914612) confirmed benefit of the combination of pembrolizumab with chemotherapy, followed by 2 years of maintenance pembrolizumab, in primary advanced Stage III or IV or first recurrent endometrial cancer, treated in the first-line setting. 74 Importantly, NRG-GY018 was powered to evaluate benefit in both the MMRd and MMRp patient cohorts. 74 NRG-GY018 met its primary endpoint in both cohorts, with a 70% reduction in the risk of disease progression or death in the MMRd cohort (HR 0.30). 74 In the MMRp cohort, median PFS was 13.1 months with pembrolizumab and 8.7 months with placebo (HR 0.54). 74 In the phase III RUBY/ENGOT-EN6/GOG-3031/NSGO trial (NCT03981796), in a similar setting, the benefit of adding dostarlimab to chemotherapy, followed by dostarlimab maintenance was examined and met its primary endpoint in the overall population, with both PFS and overall survival (OS) benefits in MMRp as well as MMRd endometrial cancer. 75 With 51% maturity, RUBY met the dual primary endpoint for OS at the second interim analysis, with a reduction in the risk of death (HR 0.69) in patients receiving dostarlimab versus chemotherapy alone. The risk of death was lower in the MMRd/MSI-H population (HR 0.32), with a trend in favour of dostarlimab in the MMRp/MSS population (HR 0.79). 75
ICI combined with TKI
The phase Ib/II clinical trial KEYNOTE-146 (NCT02501096) tested the receptor tyrosine kinase inhibitor (RTKi), lenvatinib (which targets vascular endothelial growth factor receptor (VEGFR), fibroblast growth factor, platelet-derived growth factor receptor (PDGFR), c-KIT and RET), in combination with pembrolizumab in a range of solid tumour types, including endometrial carcinoma (subtypes EC, USC, CCEC). 76 For patients with endometrial cancer, pembrolizumab combined with lenvatinib resulted in a median PFS of 7.4 months. 76 The subsequent KEYNOTE-775 phase III trial (NCT03517449) tested pembrolizumab in combination with lenvatinib in endometrial cancer patients (subtypes EC, USC, CCEC) which were MMRp, compared with standard chemotherapy regimens (doxorubicin and paclitaxel). 77 Pembrolizumab combined with lenvatinib resulted in a longer PFS (7.2 months compared with 3.8 months). 77
ICI with radiotherapy
In the ongoing RAINBO MMRd-GREEN sub-trial (NCT05255653; phase III), the addition of an adjuvant PD-L1 inhibitor (PD-L1i; durvalumab) to standard radiotherapy is being evaluated. 78 The trial will assess whether this combination improves recurrence-free survival (RFS) in patients with MMRd endometrial cancer. 78 This trial is currently recruiting, and results are eagerly anticipated, with the first major data readouts expected from 2028 onward.65,78
The synergistic potential of combining PD-1/PD-L1i with targeted agents, such as PARPi, which interfere with fundamental DNA repair pathways, is increasingly being explored. A discussion of these approaches follows in the next section.
DNA repair
Inhibition of essential DDR pathways presents an emerging and highly promising avenue of targeted cancer therapy. For cancer cells with deficiencies in redundant DDR mechanisms, pharmacologic inhibition of the cellular machinery involved in the DDR can induce a level of genomic instability that overwhelms the cell, ultimately impacting cell fate decisions, including cell death and senescence. 79
Poly(ADP-ribose) polymerase inhibitor
For some cancer types (notably HGSOC and BLBC/TNBC), which harbour defects in HR DNA repair, the advent of PARPi has been transformational. 80 Alterations in the HR DNA repair pathway for some types of uterine malignancies (particularly USC and uLMS) have highlighted these as potential candidates for PARPi. 16
Clinical trials evaluating PARPi as monotherapies are ongoing in advanced solid cancers. For uterine malignancies, recent investigations have largely focused on their use in combination with chemotherapy (or chemoradiotherapy) as maintenance or concurrent treatments, or in conjunction with ICIs, growth factor inhibitors, or other DDRi (these combinations are discussed in the next section). A significant clinical challenge is the development of acquired PARPi resistance, which has been reported in 40%–70% of other cancer types. 81 While the underlying mechanisms are complex and beyond the scope of this review, identifying combination therapies to mitigate resistance is an area of intense investigation.
PARPi with ICI and/or anti-angiogenics
A phase II trial (NCT03476798) combined the PARPi rucaparib with the VEGF inhibitor (VEGFi) bevacizumab in recurrent endometrial/cervical carcinomas or carcinosarcomas. While this trial showed limited overall benefit (median PFS was just 3.8 months), it suggested improved responses for patients with ARID1A mutations. 82 Other phase II trials (NCT03016338, NCT03951415) have, or are currently, evaluating PARPi and ICI combinations in the context of uterine cancers.83,84 The rationale for combining PARPi and ICI is that PARPi-induced DNA damage can upregulate PD-1/PD-L1 expression, potentially enhancing immune priming and targeted toxicity of HRD cancer cells. 85 The phase II trial NCT03016338 (dostarlimab and niraparib (PARPi)) showed modest activity (14% objective response rate (ORR) in all patients irrespective of MMR status), 83 while the trial NCT03951415 (durvalumab and olaparib (PARPi)) did not satisfy the pre-specified efficacy threshold (50% 6-month PFS) for this combination. 84 The phase II EndoBARR trial (NCT03694262) evaluated rucaparib and bevacizumab combined with atezolizumab (PD-L1i), demonstrating an ORR of 39%, with notable responses observed for MMRd tumours. 86 Several other trials have also explored combining PARPi with ICIs, some also with the addition of anti-angiogenic agents. A triplet combination of talazoparib (PARPi), avelumab (PD-L1i) and axitinib (inhibitor of VEGFR, c-KIT and PDGFR), was evaluated in a phase II trial (NCT02912572) specifically for MMRp endometrial cancers. 87 There was an 11.4% ORR, which was markedly less impressive than the results reported in EndoBARR, highlighting the likely influence of MMR status differences between the study populations. 87
PARPi with or without chemotherapy or ICI
DNA-damaging therapies such as platinum-based chemotherapies and DNA alkylating drugs have also been paired with PARPi. The first-line phase III trial, DUO-E (NCT04269200), in the setting of newly diagnosed advanced or recurrent endometrial cancer, examined the addition of the ICI durvalumab to carboplatin and paclitaxel chemotherapy, followed by first-line maintenance therapy with durvalumab combined with olaparib, compared with the addition of durvalumab to chemotherapy followed by durvalumab maintenance or chemotherapy alone. 88 Interim OS results (maturity ~28%) were supportive of the primary outcomes (durvalumab vs control: HR 0.77; durvalumab + olaparib vs control: HR 0.59). 88 The trial was not designed to enable the comparison of chemotherapy plus durvalumab and olaparib versus chemotherapy plus durvalumab. 88 Similarly, part 2 of the phase III RUBY trial (NCT03981796) involved the addition of the PARPi, niraparib, to dostarlimab (chemotherapy plus dostarlimab, followed by first-line maintenance therapy with dostarlimab plus niraparib for up to 3 years) compared with chemotherapy alone. 89 RUBY part 2 met its primary endpoint with an improvement in PFS in the overall and MMRp populations (MMRp: HR 0.63) with the combination of ICI and PARPi added to chemotherapy. 89 The interpretation of both the DUO-E and RUBY part 2 trials is challenging as neither included a chemotherapy plus PARPi arm; in addition, the optimal method and cut-off for classifying a USC malignancy as being HRD has not been validated. Therefore, as it remains unclear which patients derived benefit from the addition of PARPi, the uptake of the addition of PARPi to chemotherapy plus ICI in endometrial cancer has not been widely adopted.
The ongoing adjuvant phase III RAINBO-RED sub-trial (NCT05255653) is currently evaluating the addition of maintenance olaparib following standard adjuvant chemoradiation. This trial aims to determine whether this combination improves RFS in patients with endometrial carcinoma molecularly classified as p53-abnormal. 65 Given that this molecular subgroup is highly aggressive and associated with the poorest survival and highest risk of recurrence, the results of RAINBO-RED are eagerly anticipated, with initial data expected from 2028 onward.12,65
PARPi with other agents
The phase I/II ENDOLA trial (NCT02755844) examined olaparib with cyclophosphamide (DNA alkylating agent) and metformin (diabetes related medication, with PI3K/AKT/mTOR pathway inhibitory activity) in 26 patients, reporting a preliminary ORR of 20.8% and a 66.6% disease control rate in advanced/recurrent endometrial cancers. 90 The NSMP and TP53 altered groups had the best responses, indicating this could be a viable treatment option for the most aggressive endometrial cancers. 90 This represents an important step in translational research, moving findings from molecular subtypes into clinical application. The phase II COPELIA trial (NCT03570437) is investigating weekly paclitaxel in combination with either olaparib or cediranib (VEGFR-1 inhibitor) in 116 women with endometrial carcinoma subtypes. Initial results suggest that the olaparib combination is less effective than the cediranib combination or paclitaxel alone (refer to Table 4). 91
Cell cycle checkpoints
In addition to the inhibition of key molecules that mediate DNA repair via the DDR pathway, another promising approach is the inhibition of gatekeeper molecules that regulate cell cycle progression in response to DNA damage. The protein kinase ataxia telangiectasia and rad3-related (ATR) is one such gatekeeper, which signals through checkpoint kinase 1 (CHK1) and CHK2 to maintain replication fork stability and regulate the cell cycle. 63 In the phase II ATARI trial (NCT04065269), the ATR inhibitor (ATRi) ceralasertib is being tested alone and with olaparib in several gynaecological cancer types, including CCEC, EC and UCS. Preliminary results for all enrolled cancer types (ovarian, uterine and cervical) show the ORR for combination treatment was 24% for non-clear cell cancer types and 14% for clear cell carcinomas. 92 While trial results for the ATRIUM phase I trial (NCT05338346) are not available at the time of writing, the ATRi ATG-018 is being evaluated as a monotherapy for several advanced tumour types, including uterine cancers. WEE1 is another gatekeeper molecule, which plays a critical role in the DDR as a key regulator of the G2/M and S-phase checkpoints. 79 The WEE1 inhibitor adavosertib is being evaluated as a monotherapy in recurrent USC/UCS.93,94 While promising anti-tumour activity has been observed in phase II trials, including ORRs of 29.4% (NCT03668340) and 26.0% (NCT04590248), tolerability issues have been noted in the latter ADAGIO study.93,94
EGFR family
Within uterine malignancies, EGFR family alterations (ERBB1/EGFR, ERBB2/HER2 and ERBB3/HER3) exhibit distinct patterns between carcinomas and sarcomas. ERBB1 alterations are generally rare in both (refer to Tables 1–3); however, EGFR expression (non-mutant) is frequently observed.95,96 ERRB2 amplification is more frequent in uterine carcinomas than in sarcomas (refer to Table 2).
Small molecule inhibitors, including RTKi, targeting EGFR and HER2, have been explored in uterine cancers. Erlotinib and gefitinib are RTKi of EGFR, while lapatinib is an RTKi targeting both EGFR and HER2. In a phase II study (NCT00030485) of erlotinib in advanced/recurrent endometrial cancer, 59% were found to express EGFR by immunohistochemistry (IHC). 97 Of the EGFR-positive cases, 16% (3/19) achieved PR, compared with 12.5% (4/32) overall, suggesting no association with EGFR status. 97 Notably, no EGFR mutations were identified in responders and response was independent of gene amplification. 97 Phase II studies of gefitinib (NCT00027690) and lapatinib (NCT00096447) in persistent/recurrent endometrial cancer yielded similarly disappointing results, suggesting the need for alternative approaches (ClinicalTrials.gov identifier: NCT00096447). 98 – 100 mAbs targeting EGFR (cetuximab and panitumumab) and HER2 (trastuzumab and pertuzumab) have been, or are currently being investigated in EGFR and HER2-positive endometrial cancers, respectively. Trastuzumab monotherapy in a phase II trial (NCT00006089) for advanced/recurrent endometrial cancer yielded minimal benefit, with no objective tumour response observed (the best response was SD for 12/34 patients (35%)). 101 However, combining trastuzumab with carboplatin and paclitaxel in a phase II study (NCT01367002) for advanced/recurrent HER2-overexpressing USC significantly improved responses. 102 Overall median PFS was 12.9 months for the trastuzumab arm versus 8.0 months for the chemotherapy-alone arm. 102 The PFS benefit was most pronounced in first-line treatment for Stage III–IV disease, with a median PFS of 17.7 months for the trastuzumab arm versus 9.3 months for the chemotherapy-alone arm. 102 By contrast, only minimal benefit was observed in the relapsed setting. 102 This led to the current NRG-GY026 non-blinded, three-arm randomised phase II/III study evaluating the efficacy of trastuzumab and hyaluronidase-oysk or a fixed dose combination of pertuzumab, trastuzumab and hyaluronidase-zzxf in combination with paclitaxel/carboplatin in patients with HER2-positive USC or UCS (NCT05256225). 103
Antibody–drug conjugates (ADCs) are emerging as a therapeutic option, with their role in HER2-positive uterine malignancies currently under investigation. A more detailed discussion of these and other ADCs is included below.
PI3K/AKT/mTOR pathway
The PI3K/AKT/mTOR signalling axis is frequently dysregulated in uterine cancers, promoting uncontrolled growth and survival.13,34,46 Several clinical studies have examined inhibitors of this pathway.
The mTOR inhibitor (mTORi) temsirolimus was tested as a monotherapy in a phase II study (NCT00072176) of 33 patients, achieving a median PFS of 7.3 months and ORR of 13.8% in chemotherapy-naïve advanced/recurrent endometrial cancer, with outcomes being less favourable in previously treated patients (ClinicalTrials.gov identifier: NCT00072176). 104 Combining temsirolimus with bevacizumab in a phase II trial (NCT01010126) yielded a median OS of 11.5 months and ORR of 31% for the endometrial cancer cohort (ClinicalTrials.gov identifier: NCT01010126). 105 In a similar phase II trial (NCT00723255) combining temsirolimus with bevacizumab, the median OS was 16.9 months and the ORR was 24.5% in endometrial cancer patients (ClinicalTrials.gov identifier: NCT00723255). 106 The mTORi, everolimus, has been investigated in a phase II trial (NCT00087685), with SD being the best response observed (45% of endometrial cancer participants), suggesting temsirolimus may have greater activity than everolimus, at least in this setting. 107 These limited outcomes are likely attributable to the challenging patient profile, characterised by heavy pre-treatment and advanced-stage cancer.
Despite frequent aberrations in the PI3K/AKT/mTOR pathway in endometrial cancer, clinical responses to mTOR and PI3K inhibitors, as monotherapies or in combinations, have generally been modest. Two exceptions are the promising preliminary results from the phase I/II trial (NCT02208375) evaluating olaparib with either the mTORC1/2 inhibitor (mTORC1/2i), AZD2014, or the AKT inhibitor (AKTi), AZD5363, in gynaecological cancers (including endometrial carcinoma).108,109 The endometrial cancer cohort achieved ORRs of 44.4% for AZD2014 plus olaparib and an encouraging 50% for AZD5363 plus olaparib.108,109
MAPK pathway
Mutational activation of KRAS frequently occurs in several types of uterine cancer, including EC, UCS, CCEC and UAS (refer to Table 1). Inhibition of targets in the MAPK pathway is therefore clinically relevant for these cancer types, with various agents being assessed across a number of clinical trials. Despite this, several agents that target this pathway, including the MEK1/2 inhibitor (MEKi) selumetinib (AZD6244) and sorafenib (targeting MAPK pathway, VEGFR and PDGFR) have yielded underwhelming results in clinical trials evaluating these in uterine malignancies (NCT01011933, NCT00238121).110,111
A phase I study (NCT03905148) is currently evaluating the combination of lifirafenib (BGB-283; dual EGFR/RAF inhibitor) and mirdametinib (PD-0325901; MEKi) in several cancer types with BRAF and KRAS/NRAS aberrations, including some uterine cancers. 112 The results are of interest, with one uterine case achieving PR (1/7; 14.3%) and the remaining six experiencing SD (85.7%). 112
Additional trials (NCT04305249, NCT04985604 and ACTRN12620000861954) involving other inhibitors of the MAPK pathway (ATG-017, tovorafenib, pimasertib, vemurafenib and cobimetinib) are either ongoing or recently completed with results pending. 113
Antibody-drug conjugates
ADC-based delivery of a wide range of payloads is yielding outstanding results in various solid cancer types. 114 ADCs directed to HER2 via trastuzumab are being tested in clinical trials, either currently active or recently completed. Trastuzumab deruxtecan (T-DXd) delivers a topoisomerase I inhibitor payload (an exatecan derivative) to HER2-expressing cells. T-DXd monotherapy has demonstrated impressive activity in the DESTINY-PanTumor02 phase II trial (NCT04482309), with a 57.5% ORR for all endometrial tumours. 115 Responses were best for patients with higher tumour expression of HER2 (IHC 3+), achieving an ORR of 84.6%. 115 This has led to pan-tumour approval by the FDA in 2024.116,117
SYD985 is another HER2-targeting ADC, with trastuzumab bound to the DNA alkylating agent duocarmycin via a cleavable linker. 114 SYD985 was assessed in a phase II trial (NCT04205630) in patients with HER2-expressing (1+, 2+ or 3+ IHC scores) recurrent, advanced or metastatic endometrial carcinoma, reporting an ORR of 32.8% (ClinicalTrials.gov identifier: NCT04205630).
Combinations of HER2 ADCs and ICIs are also being explored. These were initially rationalised due to ADC-mediated stimulation of innate and adaptive immune responses, via increased antigen presentation, released micro-vesicles and induction of antibody-dependent cell-mediated cytotoxicity. 114 The HER2 targeting ADC, T-DM1, has been paired with the ICI, atezolizumab (PD-L1i), in the ongoing EndoMAP phase IB/II trial (NCT04486352) for recurrent/persistent endometrial cancer, alongside other biomarker-matched therapies (targeting AKT, VEGF, T-cell immunoreceptor with Ig and ITIM domains (TIGIT), PI3K or CDK4/6). BDC-1001 is an immunostimulatory ADC, or immune-stimulating antibody conjugate, which targets HER2 via a mAb (a trastuzumab biosimilar; EG12014) conjugated via a non-cleavable linker to a proprietary agonist of toll-like receptors 7 and 8. 118 BDC-1001 is being tested alone and with nivolumab (PD-1i) in a phase I/II trial (NCT04278144) in HER2-positive tumours (IHC 2+ or 3+), showing preliminary anti-tumour activity. 118 For all tumour types, there were two PR from the monotherapy cohort and three PR from the combination cohort; however, the best response achieved for patients with endometrial cancer was SD. 118 Several other HER2-ADCs (disitamab vedotin, NCT06003231; BL-M07D1, NCT06293898; BNT323/DB-1303, NCT06340568) have entered clinical trials for HER2-expressing uterine malignancies.
ADCs to targets other than HER2 are under investigation. Mirvetuximab soravtansine (MIRV, IMGN853) is based on a mAb targeting folate-receptor-a (FRa), attached via a cleavable disulfide linker to the cytotoxic payload maytansinoid DM4 and has received FDA approval in HGSOC. 114 In a phase I trial (NCT03552471), when combined with rucaparib, there was a 67% ORR in FRα-positive endometrial cancer (2/3 patients) and 50% ORR for all cohorts (6/12 patients; endometrial, ovarian, fallopian tube and primary peritoneal). 119 MIRV has also shown promising preliminary results in combination with the ICI, pembrolizumab (NCT03835819) and the anti-metabolite, gemcitabine (NCT02996825).120,121 The MIRV/gemcitabine combination was evaluated in ovarian carcinoma, TNBC and endometrial carcinoma in a phase I trial, with the endometrial cohort reporting an ORR of 50%. 120 The phase II trial combining MIRV and pembrolizumab has reported an ORR of 37.5%. 121 Other trials involving MIRV in uterine malignancies are also ongoing (NCT03832361, NCT06390995), with results eagerly anticipated.
Other novel ADCs include sacituzumab tirumotecan (also called Sac-TMT, SKB264 and MK-2870) and datopotamab deruxtecan, both targeting the trophoblast cell surface glycoprotein 2, which is highly expressed in the majority of endometrial and ovarian malignancies. 122 In a phase II trial (NCT04152499), Sac-TMT demonstrated a median PFS of 5.7 months and an ORR of 34.1% in advanced endometrial cancer. 123 Preliminary data from a phase II trial (NCT05489211) in endometrial and ovarian cancers revealed a median PFS of 6.3 months and an ORR of 27.5%. 124
Other targets
Selinexor (KPT-330) is an Exportin 1 (XPO1) inhibitor and has shown promise in endometrial cancer trials (NCT02025985, NCT03555422, NCT05611931).125–127 XPO1 is overexpressed in uterine malignancies, where it exports tumour suppressor proteins, including p53. 128 Selinexor inhibits XPO1, leading to nuclear retention and stabilisation of p53, selectively killing TP53 wild-type (TP53wt) oncogenic cells. 128 A phase II trial (NCT02025985) reported a median PFS of just 2.8 months for selinexor monotherapy in the endometrial cancer cohort, but participants were not stratified by their tumours TP53 mutational status or histological subtype. 125 By contrast, two separate phase III trials (SIENDO, NCT05611931; XPORT-EC-042, NCT03555422) did stratify participants by TP53 status and subtype.126,127 In SIENDO, the median PFS for selinexor was 5.7 months (3.8 months for placebo) for all participants irrespective of TP53 status. 127 However, for TP53wt tumours, this increased to 13.7 months (3.7 months for placebo). 127 Results were even more impressive in the XPORT-EC-042 trial, which revealed a striking median PFS of 28.4 months for selinexor maintenance therapy in TP53wt endometrial cancer (compared to 5.2 months with placebo). 126 The substantial difference in PFS between the phase II and phase III studies likely stems from the phase II cohort’s lack of TP53 stratification, suggesting a higher proportion of TP53 mutant tumours, which respond poorly to selinexor. For all three studies, nearly all enrolled patients had received prior platinum-taxane chemotherapy, with Stage I and II disease being predominant for NCT02025985 and advanced disease being predominant in SIENDO and XPORT-EC-042.125–127 While both SIENDO and XPORT-EC-042 comprised EC, USC and UCS subtypes, a greater proportion were EC type in XPORT-EC-042 relative to SIENDO (84.4% and 55.2%, respectively).126,127 As EC-type tumours are generally less aggressive than the other subtypes, 7 this likely explains the extended PFS observed in XPORT-EC-042.
Ribociclib (CDK4/6 inhibitor) and letrozole (oestrogen and gonadotropin inhibiting compound) were combined in a phase II trial (NCT02657928) for endometrial and ovarian cancers. Some activity was observed in endometrial cancer patients, particularly those with grade 1/2 tumours. While not all patient responses were provided, three (15%) endometrial patients were shown to have either complete response or PR, and median PFS was 5.4 months (ClinicalTrials.gov identifier: NCT02657928). 129
Larotrectinib, entrectinib and repotrectinib are tropomyosin receptor tyrosine kinase (TRK) inhibitors that have each received tumour-agnostic approval for use in solid tumours harbouring NTRK fusions. 116 Generally, NTRK fusions are reported to occur in less than 2% of uterine sarcomas, though they have been specifically noted in UUS in particular.59,130 These agents have yielded outstanding results in trials for other tumour types, even though uterine-specific malignancies are not yet included.131–133 These impressive results suggest their clinical relevance for uterine sarcoma types harbouring NTRK fusions.
Discussion
Although the number of clinical trials available for patients with uterine malignancies has improved, these have mainly been limited to endometrial carcinomas. Clinical trial access for all types of uterine sarcoma significantly lags behind other gynaecological cancers, and despite recent improvements, has not kept pace with other, more common cancer types. Therefore, while new and effective therapeutic approaches have been highlighted for patients with endometrial carcinomas, there are few new options for patients with uterine sarcoma.
This review focuses on trials of targeted agents that have demonstrated efficacy for uterine malignancies. For many genomically matched therapies for endometrial carcinomas and for the majority of uterine sarcomas, it is necessary to report the outcomes of single-arm studies. Single-arm trials should only be considered as a trial design method when randomised controlled trials are not feasible, due to their limitations: without a parallel control group there may be biases in interpreting results; the use of external historical controls or contemporaneous cohort study controls introduces some bias as the subjects may not be comparable; without the principles of randomisation and blinding additional bias may be introduced.
Targeting HER2-positive endometrial carcinomas with HER2-targeted agents has demonstrated efficacy across several trials and will be particularly relevant for a significant proportion of endometrial carcinoma patients, particularly when HER2-low (IHC 1+) cases are included. Indeed, the impressive results from the DESTINY-PanTumor02 trial led to the FDA’s pan-tumour approval of the HER2 targeting ADC, T-DXd, in 2024. 114 This reflects a broader trend, with the FDA granting pan-tumour approvals to eight other agents.111,114 Notable examples relevant to uterine malignancies, including pembrolizumab and dostarlimab for MMRd tumours (frequently observed in endometrial carcinomas) and larotrectinib, entrectinib and repotrectinib for tumours with NTRK fusions (relevant for uterine sarcoma and UUS specifically). Such approvals are vital for uterine and rare gynaecological cancers, simplifying treatment access and minimising the reliance on rare subtype-specific trials.
Targeting TP53wt endometrial carcinomas with selinexor may also prove to be beneficial, with early data demonstrating it may be clinically relevant for patients who are not candidates for, or have progressed on other therapies. While therapies targeting the PI3K/AKT/mTOR pathway were expected to show promise due to the frequent and extensive aberrations of this pathway present in endometrial carcinomas, they have generally yielded modest clinical responses as both monotherapies and in combinations. An exception is the promising combination of the AKTi AZD5363 with the PARPi olaparib, which warrants further investigation in endometrial carcinomas given its encouraging initial results. Equally, this is warranted for uterine sarcomas, as they also frequently display somatic aberrations in the PI3K/AKT/mTOR axis, but patients are often precluded from entering relevant trials or were not included during trial enrolment, due to the rarity of these types. Trials involving anti-angiogenic and/or ICI combinations also demonstrated the potential of these therapeutic approaches, with promising responses observed, irrespective of MMR status. Indeed, the reporting of the four major molecular subgroups of endometrial carcinomas remains the highest priority, to clarify which patients are likely to benefit most from which treatments, followed by additional useful molecular markers, such as HER2, ER and others.
Acquired drug resistance continues to be a major obstacle in identifying effective targeted therapies and therapeutic combinations across uterine malignancies. As participants need to have received prior chemotherapy, and sometimes ICI with or without anti-angiogenic therapy, prior to being eligible for many clinical trials, mechanisms of pan-drug resistance may have been acquired prior to commencing therapy on a trial. This could mask the potential efficacy of therapeutic combinations, necessitating consideration of early exposure studies to improve the development of treatments for patients.
Conclusion
The treatment landscape for uterine malignancies is rapidly evolving, with targeted therapies offering increasingly personalised approaches and driving progress in patient outcomes. Increased pre-clinical and translational analyses are essential to enable new targets to be identified. The integration of targeted therapies, particularly ADCs, into standard clinical practice will undoubtedly transform the management of these complex malignancies, leading to more durable responses and improved quality of life for patients.