
Abstract
Background:
The effect of claudin 18.2 (CLDN18.2) expression on the outcomes of a first-line immune checkpoint inhibitor (ICI)-containing chemotherapy (ICI-chemo) in patients with human epidermal growth factor receptor 2 (HER2)-negative, proficient mismatch repair (pMMR), and programmed death-ligand 1 (PD-L1)-expressing metastatic or recurrent gastric or gastroesophageal junction cancers (mGC/GEJC) remains unclear.
Objectives:
We assessed the effects of CLDN18.2 expression on the outcomes of first-line ICI-containing chemotherapy in patients with HER2-negative, pMMR, and PD-L1-expressing mGC/GEJC.
Patients and methods:
Medical records of patients with HER2-negative, pMMR, and PD-L1 combined positive score (CPS) ⩾1 unresectable/metastatic or recurrent GC/GEJC who received first-line ICI-chemo or chemotherapy alone (chemo-alone) between January 2016 and August 2024 were retrospectively analyzed. The impact of CLDN18.2 status on the clinical outcomes was evaluated in patients receiving ICI-chemo and chemo-alone to assess the prognostic significance of CLDN18.2 in the absence of ICI.
Results:
A total of 150 patients were treated with ICI-chemo, whereas 313 patients received chemo-alone. CLDN18.2 positivity (⩾2+ in ⩾75% tumor cells) was identified in 42 patients (28.0%) in the ICI-chemo group and 94 patients (30.0%) in the chemo-alone group. There were no significant differences in the objective response rate (ORR; 68.3% vs 70.3%, p = 0.842), disease control rate (DCR; 92.7% vs 94.1%, p = 0.718), progression-free survival (PFS; hazard ratio (HR) 1.01, p = 0.955), or overall survival (OS; HR 1.12, p = 0.615) between CLDN18.2-positive and CLDN18.2-negative patients in the ICI-chemo group. Similarly, the DCR, ORR, PFS, and OS outcomes were comparable between the CLDN18.2-positive and -negative patients in the chemo-alone group.
Conclusion:
CLDN18.2 expression exerted no impact on outcomes of first-line ICI-chemo and chemo-alone in patients with HER2-negative, pMMR, and PD-L1 CPS ⩾1 mGC/GEJC.
Keywords
Introduction
Following the successful results of the CheckMate-649, KEYNOTE-859, and RATIONALE-305 trials, platinum doublet chemotherapy plus an immune checkpoint inhibitor (ICI) has become the global standard first-line option for patients with human epidermal growth factor receptor 2 (HER2)-negative metastatic or recurrent gastric or gastroesophageal junction cancer (mGC/GEJC).1 –3 These pivotal studies demonstrated the survival benefit of adding ICI to chemotherapy, regardless of the programmed cell death-ligand 1 (PD-L1) combined positive score (CPS). However, the Oncologic Drugs Advisory Committee of the Food and Drug Administration voted for major benefits of ICIs among patients with higher levels of PD-L1 CPS and against the risk-benefit with PD-L1 CPS <1, following discussions and data combinations from three key clinical trials, the first-line use of ICIs with chemotherapy is not approved for patients with PD-L1 CPS <1 by several regulatory authorities and clinical guidelines.4 –8
Claudin 18 isoform 2 (CLDN18.2) is an emerging therapeutic target. 9 Based on the positive outcomes of the global, randomized phase III SPOTLIGHT and GLOW trials, zolbetuximab, a first-in-class monoclonal antibody targeting CLDN18.2, in combination with chemotherapy, has already been established as a treatment option for patients with HER2-negative, CLDN18.2-positive mGC/GEJC.10,11 Although for patients with HER2-negative, CLDN18.2-positive, and PD-L1 CPS ⩾1, both chemotherapy with ICI and zolbetuximab are available, it remains unclear whether treatment outcomes of ICI-based therapy vary according to CLDN18.2 expression.
A previous study showed that CLDN18.2 expression did not influence the clinical outcomes of patients with mGC/GEJC who received first- and second-line cytotoxic chemotherapy alone or later-line ICI monotherapy.12 –16 Furthermore, a recent single-center retrospective study demonstrated similar efficacy of nivolumab plus chemotherapy in CLDN18.2-positive and CLDN18.2-negative patients. 16 However, that study included patients with deficient mismatch repair (dMMR) or PD-L1 CPS <1 mGC/GEJC. Patients with dMMR GC/GEJC are recognized to have a highly immunogenic subtype, and the preferential use of ICIs is recommended by several clinical guidelines.4 –8
Therefore, in this study, we aimed to evaluate the impact of CLDN18.2 status on clinical outcomes of patients with HER2-negative, proficient MMR (pMMR), PD-L1 CPS ⩾1 mGC/GEJC receiving first-line ICI-containing chemotherapy.
Patients and methods
Patients
Medical records of HER2-negative, pMMR, PD-L1 CPS ⩾1 patients with mGC/GEJC who received first-line ICI-containing platinum doublet chemotherapy (ICI-chemo) or platinum doublet chemotherapy alone (chemo-alone) from January 2016 to August 2024 at the Department of Gastroenterology and Gastrointestinal Oncology, National Cancer Center Hospital East, Kashiwa, Chiba, Japan, were retrospectively analyzed. The eligibility criteria were as follows: patients (i) with histologically or cytologically confirmed gastric or GEJ adenocarcinoma, (ii) with unresectable/metastatic or recurrent disease, (iii) with no prior systemic anticancer treatment, (iv) with an Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0–2, (v) who received platinum doublet chemotherapy at our institute, (vi) with known biomarker status of HER2, CLDN18.2, PD-L1 CPS, MMR proteins (MutL homolog 1 (MLH1), MutS homolog 2 (MSH2), MutS homolog 6 (MSH6), and postmeiotic segregation increased 2 (PMS2)), and Epstein–Barr Virus (EBV), and (vii) who provided written informed consent for the systemic chemotherapy and biomarker study (UMIN000019129). The study protocol was approved by the ethics committee of our institution, the National Cancer Center Hospital East Certified Review Board, and was conducted in accordance with the guidelines for biomedical research stipulated in the Declaration of Helsinki.
Biomarker status
Biomarkers, including HER2, CLDN18.2, PD-L1, CPS, MMR, and EBV, were evaluated using formalin-fixed paraffin-embedded tissue specimens. CLDN18 (Clone 43-14A; Roche Ventana, Oro Valley, AZ, USA) expression was used to assess the expression of CLDN18.2 by immunohistochemistry (IHC). The standard of CLDN positivity was defined as moderate-to-strong expression in ⩾75% of tumor cells. IHC for HER2, MMR (determined by the expression levels of MLH1, MSH2, MSH6, and PMS2 by IHC), and in situ hybridization of Epstein–Barr-encoded RNA were performed as previously reported. 17 The expression of PD-L1 was evaluated by IHC using an anti-PD-L1 monoclonal antibody (clones SP142 and SP263; Ventana, Tucson, AZ, USA, 22C3 or 28-8; Agilent Technologies, Santa Clara, CA, USA). The details of the IHC experiment are shown in Table S1.
Treatment procedures
All patients received at least one cycle of either ICI-containing platinum-based doublet chemotherapy or chemotherapy alone. The platinum doublet regimens used included SOX, CAPOX, or FOLFOX. The treatment schedule and dose were similar to those reported in previous pivotal clinical trials. Treatment was continued until disease progression, unacceptable toxicity, withdrawal of consent, or death occurred.
Outcome assessment
Treatment outcomes, including tumor response, progression-free survival (PFS), and overall survival (OS), were evaluated. Radiological assessment was performed according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 in patients with at least one measurable lesion. The objective response rate (ORR) was determined as the proportion of patients with the best overall response of complete response (CR) or partial response (PR) according to the investigators’ assessment. PFS was defined as the time interval from treatment initiation to the first radiologically or clinically confirmed progression disease (PD), death, or censored at the last non-PD confirmation date. OS was defined as the time from the initiation of first-line treatment to death due to any cause or censored at the last follow-up.
Statistical analysis
All statistical analyses were performed using the R software (Version 4.1.1; the R Foundation for Statistical Computing, Vienna, Austria) and GraphPad Prism version 9.0.0 for Windows (GraphPad Software, San Diego, CA, USA). Differences in baseline characteristics and ORR between the CLDN18.2-positive and CLDN18.2-negative groups were compared using Fisher’s exact test or t test. The Kaplan–Meier method was used to estimate the survival curves of PFS and OS, and the 95% confidence intervals (CIs) of median survival were calculated. The log-rank test was used to compare survival differences. Hazard ratios (HRs) were estimated by univariate and multivariate Cox proportional hazards models to determine the prognostic value in PFS and OS. Statistical significance was defined as a two-sided p value less than 0.05.
Results
Patient characteristics
As demonstrated in the patient selection flow (Figure 1), a total of 1450 treatment-naive patients were treated with systemic therapy during the study period. Among them, 990 patients initiated treatment at our institute, and 463 patients were included in this study, of whom 150 received ICI plus chemotherapy and 313 received chemotherapy chemo-alone.
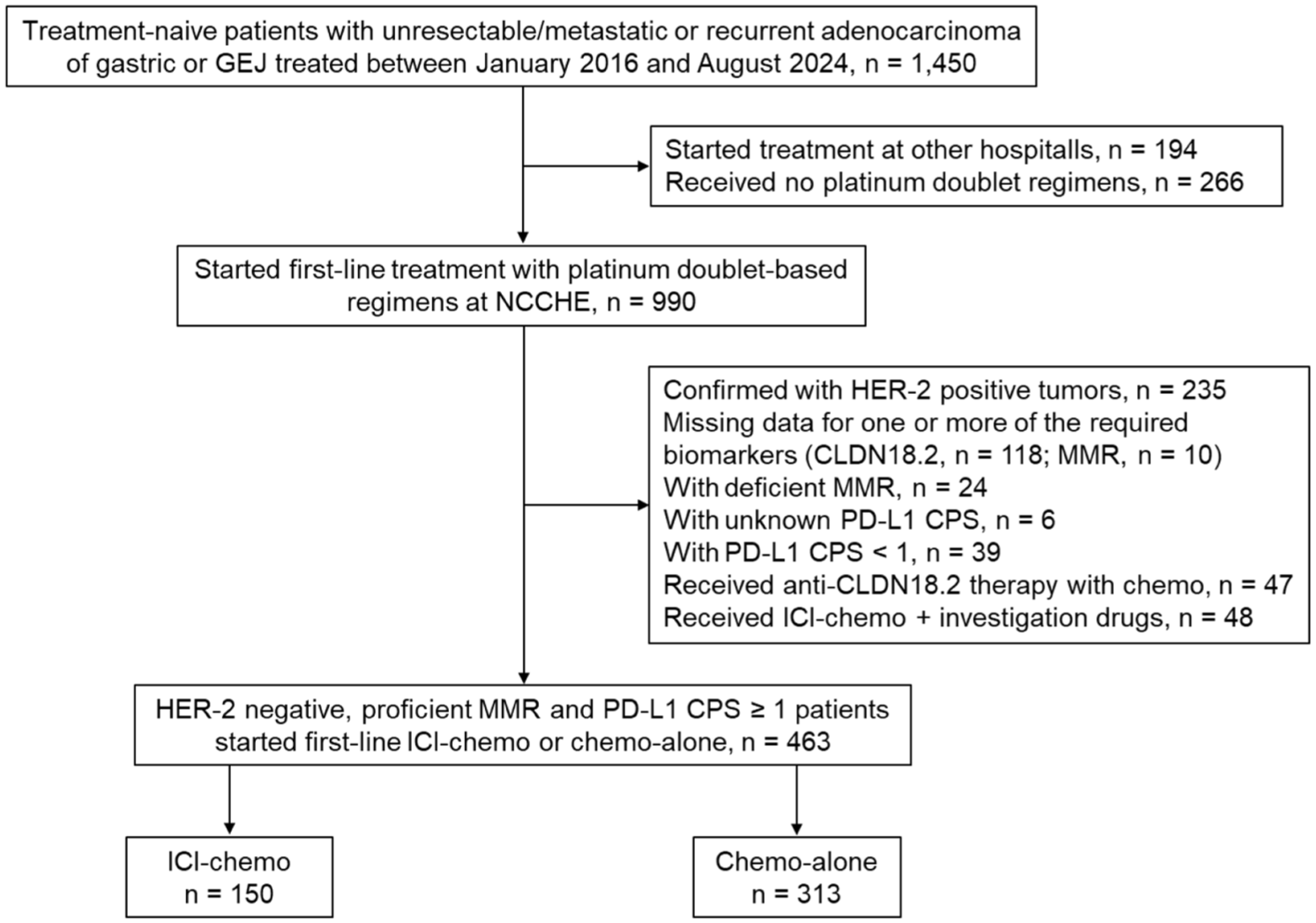
Patient selection flow.
The baseline characteristics of the patients who received ICI-chemo are shown in Table 1. Among the 150 patients in the ICI-chemo group, the CLDN18.2 positivity rate was 28.0% (n = 42). Patients with CLDN18.2-positive tumors tended to have a higher proportion of patients aged <65 years (47.6% vs 32.4%, p = 0.092), primary GEJ tumors (21.4% vs 9.3%, p = 0.057), and EBV-positive tumors (9.5% vs 2.8%, p = 0.096) than those with CLDN18.2-negative tumors, although these differences were not statistically significant. Similar trends were observed in the entire cohort (n = 463). Furthermore, among 463 patients, peritoneal metastasis was more frequently observed in patients with CLDN18.2-positive GC/GEJC (n = 74, 54.4%) than in those with CLDN18.2-negative tumors (n = 103, 31.5%; p < 0.001).
Baseline characteristics of the patients according to CLDN18.2 expression in the ICI-chemo group (n = 150) a .

Characteristics at first diagnosis of recurrence or metastatic disease.
Using Fisher’s exact test, except for age (range).
Using t test.
Detailed PD-L1 CPS information was available for 40 CLDN-positive (95.2%) and 92 CLDN-negative (85.2%) patients in the ICI-chemo group.
Chemo, chemotherapy; CLDN, claudin; CPS, combined positive score; EBV, Epstein–Barr virus; ECOG, Eastern Cooperative Oncology Group; GEJ, gastroesophageal junction; ICI, immune checkpoint inhibitor; ICI-chemo, ICI-containing chemotherapy; mGPS, modified Glasgow prognostic score; PD-L1, programmed death-ligand 1; PS, performance status.
The baseline characteristics of the patients who received chemo-alone are shown in Table S2. The CLDN18.2 positivity rate was 30.1% (n = 94), which was comparable to that in the ICI-chemo group. Similarly, patients with CLDN18.2-positive tumors in the chemo-alone group showed a higher proportion of younger age (44.7% vs 24.7%, p < 0.001) and EBV positivity (8.5% vs 1.8%, p = 0.008) than those with CLDN18.2-negative tumors, which is consistent with the trends observed in the ICI-chemo group. In addition, more patients in the CLDN18.2-positive group had peritoneal metastasis (58.5% vs 47.7%, p < 0.001), and PD-L1 CPS ⩾1 and <10 were observed (92.9% vs 81.4%, p = 0.035).
Treatment outcomes of first-line ICI-containing chemotherapy according to CLDN18.2 expression
The median follow-up time was 31.1 months (95% CI: 24.7–37.4 months). No statistically significant differences were observed in median PFS (7.8 vs 7.2 months; HR 1.01, 95% CI: 0.68–1.51; p = 0.955) or OS (15.6 vs 20.4 months; HR 1.12, 95% CI: 0.71–1.78; p = 0.615) between CLDN18.2-positive and CLDN18.2-negative patients in the ICI-chemo group (Figure 2(a) and (b)). In addition, these trends were consistent even when limiting the analysis to patients with CPS ⩾5 (data not shown). Moreover, the ORRs (68.3% vs 70.3%, p = 0.842) and disease control rates (DCRs; 92.7% vs 94.1%, p = 0.718) were comparable regardless of the CLDN18.2 status (Table 2).
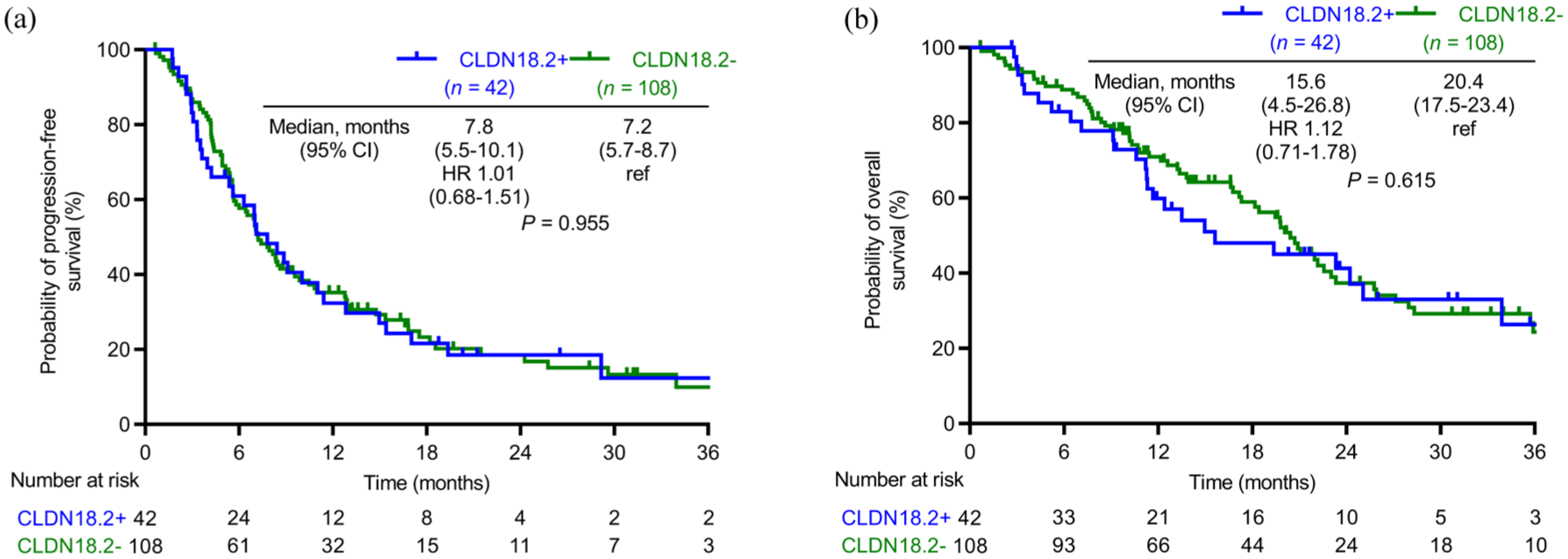
Kaplan–Meier curves for (a) PFS and (b) OS according to CLDN18.2 expression in the ICI-chemo group (n = 150).
Treatment response according to CLDN18.2 expression in the ICI-chemo group (n = 150).

Univariate and multivariate analyses revealed that CLDN18.2 expression had no impact on either PFS (HR 1.04, 95% CI: 0.69–1.56; p = 0.850) or OS (HR 1.13, 95% CI: 0.71–1.78; p = 0.613) in the ICI-chemo group (Tables 3 and 4).
Using Fisher’s exact test.
CI, confidence interval; CLDN, claudin; CR, complete response; DCR, disease control rate (CR + PR + SD); HR, hazard ratio; ICI-chemo, ICI-containing chemotherapy; NE, not evaluated; ORR, objective response rate (CR + PR); OS, overall survival; PD, progression disease; PFS, progression-free survival; PR, partial response; SD, stable disease.
In the multivariate analysis, ECOG PS ⩾1 (p = 0.032 for PFS and p < 0.001 for OS), signet ring cell histology (p < 0.001 for both PFS and OS), liver metastasis (p = 0.002 for PFS and p = 0.039 for OS), and mGPS 2 (p = 0.015 for PFS and p < 0.001 for OS) were identified as independent poor prognostic factors for both PFS and OS (Tables 3 and 4).
Univariate and multivariate analyses of progression-free survival in the ICI-chemo group (n = 150).

CI, confidence interval; CLDN, claudin; CPS, combined positive score; EBV, Epstein–Barr virus; ECOG, Eastern Cooperative Oncology Group; GEJ, gastroesophageal junction; HR, hazard ratio; ICI-chemo, ICI-containing chemotherapy; mGPS, modified Glasgow prognostic score; NA, not applicable; PD-L1, programmed death-ligand 1; PS, performance status.
Univariate and multivariate analyses of overall survival in the ICI-chemo group (n = 150).

CI, confidence interval; CLDN, claudin; CPS, combined positive score; EBV, Epstein–Barr virus; ECOG, Eastern Cooperative Oncology Group; GEJ, gastroesophageal junction; HR, hazard ratio; ICI-chemo, ICI-containing chemotherapy; mGPS, modified Glasgow prognostic score; NA, not applicable; PD-L1, programmed death-ligand 1; PS, performance status.
Treatment outcomes of first-line chemotherapy alone according to CLDN18.2 expression
Consistent with findings from the ICI-chemo group, the DCRs (47.9% vs 40.3%, p = 0.326), ORRs (83.6% vs 78.5%, p = 0.326), median PFS (5.5 vs 4.9 months; HR 0.87, 95% CI: 0.68–1.11; p = 0.273), and OS (15.5 vs 13.0 months; HR 0.96, 95% CI: 0.73–1.26; p = 0.768) were comparable between patients with CLDN18.2-positive and CLDN18.2-negative tumors in the chemo-alone group (Table S3 and Figure 3).

Kaplan–Meier curves for (a) PFS and (b) OS according to CLDN18.2 expression in the chemo-alone group (n = 313).
Discussion
This is the first study to assess the influence of CLDN18.2 status on the outcomes of first-line ICI-chemo in patients with HER2-negative, pMMR, and PD-L1 CPS ⩾1 mGC/GEJC.
In the current study, CLDN18.2 positivity (⩾2+ in ⩾75% of tumor cells using the 43-14A VENTANA assay) was defined according to the same criteria as those used in the SPOTLIGHT and GLOW trials. The CLDN18.2 positivity rates were 28.0% in the ICI-chemo group and 30.0% in the chemo-alone group, which was lower than the rate reported in the SPOTLIGHT and GLOW trials (38.4%).10,11 This discrepancy may be mainly attributed to the exclusion of 47 patients with CLDN18.2-positive mGC/GEJC who received chemotherapy in combination with anti-CLDN18.2 therapy from relevant clinical trials outside this study. If these 47 patients were included among the 463 eligible patients in this study, the CLDN18.2 positivity rate would have been 35.9% (183/510), which is comparable to that reported in pivotal studies.10,11
The distribution of PD-L1 CPS high and low was nearly identical between patients with CLDN18.2-positive and CLDN18.2-negative mGC/GEJC in the ICI-chemo group, regardless of whether the cutoff was set at 5 or 10. The overall proportion of CPS ⩾5 was 60.1% (80/132); however, it is challenging to accurately determine whether this proportion is high or low. Corresponding data on the proportion of patients with PD-L1 CPS ⩾5 in pMMR, HER2-negative, CLDN18.2-positive, and PD-L1 CPS <1 mGC/GEJC are not available. Similar to previous studies, the proportion of patients with EBV-associated mGC/GEJC was higher among CLDN18.2-positive patients than that among CLDN18.2-negative patients.16,18 However, because the number of patients with EBV-associated mGC/GEJC was very limited in both groups (n = 4 in the CLDN18.2-positive group and n = 3 in the CLDN18.2-negative group), their impact was unlikely to significantly influence the prognosis of patients receiving ICI-chemo. In this study, the effect of CLDN18.2 on ICI efficacy was evaluated after excluding key confounding biomarkers, namely dMMR, which is strongly associated with a favorable response, and CPS <1, which is linked to poor efficacy. Moreover, with the minimal imbalance in CPS-high and EBV-positive cases, this analysis provides a more refined assessment of the impact of CLDN18.2 status on ICI-chemo. Furthermore, multivariate analysis incorporating key clinicopathological factors did not demonstrate a significant association between CLDN18.2 status and clinical outcomes (PFS and OS).
First, as a tight junction protein, CLDN18.2 itself does not directly regulate immune checkpoints or immune cell activity. 16 However, previous studies have indicated that distinct immunological features may influence responses to ICIs.19,20 One study has reported more CD8+ T cells in patients with CLDN18.2-positive mGC/GEJC than those in patients with CLDN18.2-negative. 19 Another study using multiplex IHC analysis of 80 GC specimens supported these findings, showing a higher proportion of CD8+ T cells in CLDN18.2-positive tumors. 20 However, this study also demonstrated a lack of expression of immune checkpoint molecules and their associated ligands, such as PD-1, PD-L1, LAG-3, and TIM-3, suggesting limited immune cell infiltration and an immunosuppressive TIME in CLDN18.2-positive mGC/GEJC. 20
However, a recent preclinical study suggested that CLDN18.2 itself actively contributed to immune cell recruitment and activation by modifying tumor cell adhesion properties and the immunological synapse. 21 Nevertheless, these perspectives did not align with the findings on the prognosis of nivolumab monotherapy. 15 This discrepancy may be attributed to the differences in CLDN18.2-positivity assessment methods between translational research and clinical practice, the limited sample size, and the restricted evaluable area in TIME analysis using tissue microarrays. Further comprehensive investigations based on standardized diagnostic methods are required to clarify the immunogenicity of CLDN18.2-positive GC/GEJC.
This study has certain limitations that should be addressed when interpreting the results. First, this was a retrospective study with a relatively small number of patients at a single institution. Accordingly, the results of the multivariate analysis should be interpreted with particular caution. Second, patients with CLDN18.2-positive tumors were more likely to participate in clinical trials targeting CLDN18.2; thus, the potential risk of patient selection bias may have affected the results. Third, this study was conducted over nearly 8 years, during which practice-changing results were introduced in both first-line and later-line treatments for mGC/GEJC.
In conclusion, CLDN18.2 expression had no significant impact on the outcomes of first-line ICI-chemo or chemo-alone in patients with HER2-negative, pMMR, and PD-L1 CPS ⩾1 mGC/GEJC. These findings suggest that CLDN18.2-positive patients may derive a survival benefit from the addition of ICI that is comparable to that observed in the overall population.
Supplemental Material
sj-docx-1-tam-10.1177_17588359251369042 – Supplemental material for Impact of claudin 18.2 expression on treatment outcomes of first-line immunochemotherapy in patients with HER2-negative, proficient MMR, PD-L1 CPS ≽1 metastatic gastric/gastroesophageal junction cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359251369042 for Impact of claudin 18.2 expression on treatment outcomes of first-line immunochemotherapy in patients with HER2-negative, proficient MMR, PD-L1 CPS ≽1 metastatic gastric/gastroesophageal junction cancer by Fei Zhang, Izuma Nakayama, Naoya Sakamoto, Dai Okemoto, Amane Jubashi, Yuki Matsubara, Yu Miyashita, Seiya Sato, Shinpei Ushiyama, Akinori Kobayashi, Ukyo Okazaki, Kazumasa Yamamoto, Saori Mishima, Daisuke Kotani, Akihito Kawazoe, Tadayoshi Hashimoto, Yoshiaki Nakamura, Yasutoshi Kuboki, Hideaki Bando, Takashi Kojima, Takayuki Yoshino, Takeshi Kuwata and Kohei Shitara in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors thank all patients and their families for participating in the study, as well as their colleagues, especially M. Narikiyo, for her assistance with the preparation of pathological specimens for evaluation, and all the nurses involved. We acknowledge Dr Wakabayashi for his professional insights and guidance regarding the statistical analysis. We would like to thank Editage (![]() ) for English language editing.
) for English language editing.
Declarations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.