
Abstract
Background:
Patients with multiple myeloma (MM) and renal impairment (RI), particularly those requiring dialysis, have historically experienced poor outcomes. Despite advancements in targeted therapies, the prognosis of dialysis-dependent MM and factors influencing dialysis independence remain unclear.
Objectives:
This study aimed to provide a comprehensive analysis of the clinical manifestations and treatment outcomes of dialysis-dependent MM patients in China, and to explore the factors associated with dialysis independence and long-term survival.
Design:
We conducted a multicenter, retrospective, real-world cohort study.
Methods:
This multicenter, retrospective study included 122 MM patients requiring chronic hemodialysis (⩾28 days of treatment) at 4 comprehensive hospitals in China from January 2012 to November 2023. Hemodialysis resulting from causes other than MM was excluded. Logistic regression was employed for multivariate analysis of factors associated with dialysis independence, and Kaplan–Meier survival curves and Cox proportional hazard models were utilized for survival analysis.
Results:
Among the 122 patients, 74 patients (60.7%) were male, with a median age of 65 (39–87) years. Of these, 71.3% (n = 87) had newly diagnosed MM (NDMM), and 28.7% (n = 35) had relapsed/refractory MM (RRMM). Dialysis independence was achieved in 27 patients (22 with NDMM and 5 with RRMM). Proteasome inhibitors were used in 80.3% of patients (n = 98), while 13.9% (n = 17) received daratumumab-based regimens. After a median follow-up of 43.7 months, the median progression-free survival (PFS) was 14.4 months (95% confidence interval (CI): 3.6–25.2), and the median overall survival (OS) was 27.4 months (95% CI: 6.9–47.9). Dialysis-independent patients had significantly longer PFS (36.7 vs 9.4 months, p = 0.006) and OS (62.6 vs 17.7 months, p < 0.001). Factors associated with dialysis independence included achieving a very good partial response (VGPR), receiving daratumumab-based regimens, reduction in serum-free light chain ⩾80% after the first chemotherapy cycle, and age <65 years.
Conclusion:
In the era of new drugs, dialysis-dependent MM still has a poor prognosis, although dialysis independence improves survival.
Plain language summary
Patients with multiple myeloma (a type of blood cancer) who also have severe kidney damage, especially those needing dialysis, often face poor health outcomes. While newer treatments have improved care, it remains unclear how these patients fare long-term or what factors might help them stop dialysis. This study followed 122 patients (average age: 65) who required dialysis when diagnosed or during relapse. Most patients (71%) were newly diagnosed, while 29% had relapsed or resistant disease. Treatments included medications like proteasome inhibitors (used in 80% of patients) and daratumumab-based therapy (used in 14%). After a median follow-up of 44 months, 27 patients (22 newly diagnosed, 5 relapsed) were able to stop dialysis. Those who stopped dialysis lived significantly longer, with an average progression-free survival of 36.7 months (vs. 9.4 months for those still on dialysis) and overall survival of 62.6 months (vs. 17.7 months). Factors linked to stopping dialysis included: achieving a strong response to treatment (very good partial response); using daratumumab-based therapy; a large drop (⩾80%) in blood markers of cancer (free light chains) after the first treatment cycle; being under age 65. Although newer drugs are available, dialysis-dependent myeloma patients still face challenges. However, stopping dialysis is possible for some and is strongly tied to better survival. Early, effective treatment and specific therapies may improve outcomes for these patients.
Introduction
Multiple myeloma (MM) is a plasma cell neoplasm characterized by anemia, osteolytic bone lesions, hypercalcemia, and renal impairment (RI). 1 Additional complications such as hyperviscosity syndrome (due to elevated monoclonal protein levels) and rare manifestations like priapism have also been documented, further contributing to disease morbidity.2,3 Up to 50% of patients with MM present with RI at diagnosis, defined by an estimated glomerular filtration rate (eGFR) of less than 60 mL/min/1.73 m2.1,4 Among these, approximately 10% develop severe RI requiring kidney replacement therapy. 5 Renal failure in MM patients is associated with increased treatment-related mortality and morbidity compared with patients with preserved renal function, 6 highlighting the critical impact of RI on clinical outcomes in MM.
Recent advances in treatment options, including proteasome inhibitors (PIs; e.g., bortezomib, carfilzomib), immunomodulatory agents (e.g., pomalidomide), and monoclonal antibodies (e.g., daratumumab), have demonstrated safety and efficacy in patients with MM and RI, leading to notable improvements in overall survival (OS) and renal recovery.1,7 –9 Clinical studies, such as those from Greece and the Netherlands, have shown that bortezomib-based triplet regimens may enhance renal responses and increase dialysis independence compared to single-agent therapies.10,11 Despite these advancements, patients with an eGFR below 30 mL/min/1.73 m2—particularly those requiring dialysis—are frequently excluded from large-scale prospective clinical trials. Consequently, factors influencing dialysis independence and long-term survival in this population remain poorly understood, especially with limited data available from Chinese cohorts.
In this multicenter study, we aimed to address this gap by analyzing clinical and treatment-related predictors of dialysis independence in Chinese patients with MM requiring hemodialysis. We also examined the factors associated with dialysis independence and long-term survival, aiming to enhance clinical management and outcomes in this high-risk MM population.
Materials and methods
Patients
This multicenter retrospective study included patients with MM who required chronic hemodialysis at the First Affiliated Hospital of Zhejiang University School of Medicine, Anji People’s Hospital, Quzhou People’s Hospital, and Haining People’s Hospital, China, from January 2012 to November 2023 (Figure 1). The inclusion criteria for patients were as follows: (1) had a confirmed diagnosis of MM, (2) ⩾18 years of age, and (3) were dialysis dependent, as defined by an eGFR of <15 mL/min/1.73 m2, with the requirement for hemodialysis treatment for ⩾28 days.10,12 Patients were excluded if they fulfilled any of the following conditions: (1) had known advanced chronic kidney disease (CKD), (2) received hemodialysis due to light chain deposition disease, light chain amyloidosis, or other non-MM-related conditions, (3) had an uncontrolled malignant disorder, active infection, or peripheral neuropathy, (4) were suffering from psychiatric disorders, (5) did not receive any anti-myeloma therapy within 6 months of diagnosis, or (6) had incomplete data. The follow-up endpoint was June 1, 2024, which marked either the date of the last follow-up or the date of death. Demographics, disease characteristics, and clinical outcomes were extracted from the electronic medical record database of the hospitals. The diagnosis of MM was based on the International Myeloma Working Group (IMWG) criteria. 13 The initiation of hemodialysis was recommended for patients exhibiting hyperkalemia, metabolic acidosis, fluid overload, or symptoms of uremia. 14 To evaluate the impact of dialysis dependence on survival, patients were divided into two groups: those who were dialysis dependent and those who were dialysis independent. Dialysis independence was defined as the restoration of renal function, resulting in dialysis cessation for at least two consecutive months after the initial treatment.10,15 The ethics committees at all four participating medical centers approved this multicenter, retrospective cohort study. The reporting of this study conforms to the STROBE guidelines 16 (Supplemental Material).

Flowchart of patient selection.
Clinical, laboratory, and cytogenetic data
Clinical data, including demographic information, clinical presentations, coexisting medical conditions, laboratory and cytogenetic testing results, imaging findings, hemodialysis status, therapeutic regimens, and clinical outcomes, were collected. Laboratory data at the time of diagnosis and dialysis initiation included serum protein electrophoresis, serum/urine immunofixation electrophoresis, free light chain (FLC) levels, uric acid, total serum protein, serum albumin, blood urea nitrogen, creatinine, eGFR, calcium (Ca), hemoglobin, bone marrow plasma cell (BMPC) percentage, lactate dehydrogenase (LDH), C-reactive protein, serum β2-microglobulin (β2-MG), urine volume, and urinary protein. Cytogenetic abnormalities were identified using fluorescence in situ hybridization (FISH), as previously described,17,18 performed on CD138+ sorted plasma cells from bone marrow samples, identified via cytoplasmic immunoglobulin staining. The Chronic Kidney Disease Epidemiology Collaboration equation (CKD-EPI) Creatinine Equation was used to estimate GFR. 19 The serum free light chain (sFLC) ratio normal range reported in the literature (0.37–3.1) for patients with CKD was applied in our cohort. 20
Treatment and outcome
Patients were categorized into one of the following four groups based on the type of first-line induction chemotherapy: (1) PI only, (2) immunomodulatory drug (IMiD) only, (3) PI and IMiD combination, or (4) daratumumab-based regimens. All patients were followed up every 1–2 months. Hematological and renal responses were evaluated according to criteria established by the IMWG.21,22 OS was defined as the time from diagnosis to death or the last follow-up. Progression-free survival (PFS) was calculated from the date of diagnosis to the date of disease progression, relapse, death from any cause, or the last follow-up.
Statistical analysis
Categorical variables are presented as numbers and percentages (n, %), while continuous variables are expressed as medians and ranges (median, range). Categorical variables were compared using the chi-square test or Fisher’s exact test. The nonparametric Mann–Whitney U test was used to compare continuous variables between the groups. Logistic regression analysis was performed to identify factors influencing the reversibility of dialysis dependence. Kaplan–Meier curves were generated for survival analysis, and group comparisons were performed using the log-rank test. Factors associated with PFS and OS in dialysis-dependent patients with MM were analyzed using a Cox proportional hazards model for multivariate analysis. Statistical significance was defined as a two-sided p value of less than 0.05. Data analysis was performed using GraphPad Prism version 9.0 (GraphPad Software, San Diego, CA, USA) and IBM SPSS Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Patient characteristics
A total of 122 patients with MM requiring hemodialysis were enrolled in this study between January 2012 and November 2023. The baseline patient characteristics are presented in Table 1. Overall, 74 patients (60.7%) were men, with a median age of 65 years (range: 39–87 years). Hemodialysis was initiated in 87 patients with newly diagnosed multiple myeloma (NDMM; 71.3%) and 35 patients with relapsed/refractory MM (RRMM; 28.7%). The median eGFR for all patients was 7.0 mL/min/1.73 m2 (range, 2.7–23.0 mL/min/1.73 m2), and the median 24-h urine protein quantification was 2.11 g/24 h (range, 0.11–23.93 g/24 h). Severe proteinuria (24-h urine protein quantification ⩾3.5 g/24 h) was observed in 29.8% of the patients (n = 25). In total, 96.7% (n = 122) of the patients were classified as International Staging System (ISS) stage III, and 72.5% (n = 102) were Revised ISS (R-ISS) stage III. Among the 94 patients with available FISH test results, 51 (54.3%) had high-risk cytogenetic abnormalities. Compared to the dialysis-independent group, patients in the dialysis-dependent group were older (67 vs 63 years, p = 0.018) and had higher β2-MG levels (26.4 vs 15.6 mg/L, p < 0.001). In addition, a greater proportion of patients in the dialysis-dependent group had ISS stage III (98.9% vs 88.9%, p = 0.034) and R-ISS stage III (81.8% vs 44.0%, p < 0.001). No significant differences were observed in other baseline characteristics between the two groups.
Clinical and laboratory characteristics of patients with severe renal failure requiring hemodialysis.

High-risk FISH, defined as the presence of any of del17p, t(4;14), and/or t(14;16).
p < 0.05. **p < 0.01. ***p < 0.001.
ASCT, autologous stem cell transplantation; BMPC, bone marrow plasma cell; eGFR, estimated glomerular filtration rate; FISH, fluorescence in situ hybridization; Hb, hemoglobin; IMiDs, immunomodulatory drugs; ISS, International Staging System; LDH, lactate dehydrogenase; MM, multiple myeloma; NA, not available; PI, proteasome inhibitors; R-ISS, revised international staging system; sFLC, serum free light chain; VCd, bortezomib plus cyclophosphamide and dexamethasone; Vd, bortezomib plus dexamethasone; VGPR, very good partial response; VPd, bortezomib plus pomalidomide and dexamethasone; VRd, bortezomib plus lenalidomide and dexamethasone.
Treatment and response to first-line therapy
The treatment strategies for patients with dialysis-dependent MM are presented in Table 1. A total of 59.8% of the patients received PI-cyclophosphamide–dexamethasone regimens, while 20.5% were treated with a combination of PIs and IMiDs. In total, 13.9% of the patients received daratumumab-based regimens. A small proportion (5.7%) received IMiD-based therapies, with lenalidomide doses adjusted according to creatinine clearance levels. Patients on hemodialysis should start lenalidomide at 5 mg/day post-dialysis, with potential dose escalation to 15 mg/day if no significant adverse effects occur. Notably, the proportion of patients who received daratumumab-based treatment was significantly higher in the dialysis-independent group than in the dialysis-dependent group (33.3% vs 8.4%, p = 0.003). Two patients underwent autologous stem cell transplantation, and both achieved dialysis independence successfully.
Hematological and renal responses were analyzed in both groups. The dialysis-independent group exhibited a significantly higher hematological response rate (⩾very good partial response (VGPR): 77.8% vs 24.2%, p < 0.001) and a greater likelihood of achieving deep responses. By contrast, none of the dialysis-dependent patients achieved a major renal response, whereas 48.1% of the dialysis-independent patients achieved this milestone. After the first chemotherapy cycle, the median reduction rate of the involved sFLC level was 38% (range, 1%–77%) in the dialysis-dependent group and 84% (range, 40%–99%) in the dialysis-independent group (p < 0.001). Seventeen patients (81.0%) in the dialysis-independent group achieved a sFLC level of less than 700 mg/L after one cycle of chemotherapy compared to 21 patients (27.3%) in the dialysis-dependent group (p < 0.001; Table 1).
Dialysis independence
In this cohort, 27 patients (22.1%) achieved renal recovery and became dialysis-independent following anti-MM treatment. This group included five patients who were initially dialysis dependent at the time of relapse. The median time to achieve dialysis independence was 2.2 months (range, 1.2–29.3 months).
Univariate and multivariate logistic regression analyses identified several factors significantly associated with dialysis independence: achieving a hematological response of at least VGPR (odds ratio (OR): 3.895; 95% CI: 1.922–9.793; p = 0.005), receiving daratumumab-based treatment (OR: 3.027; 95% CI: 1.374–6.774; p = 0.032), reduction in sFLC ⩾80% after 1 cycle of chemotherapy (OR: 5.076, 95% CI: 2.351–10.489, p = 0.010), and age <65 years (OR: 1.618, 95% CI: 1.102–2.033, p = 0.015; Table 2).
Multivariate logistic regression analysis of factors associated with achieving dialysis independence.
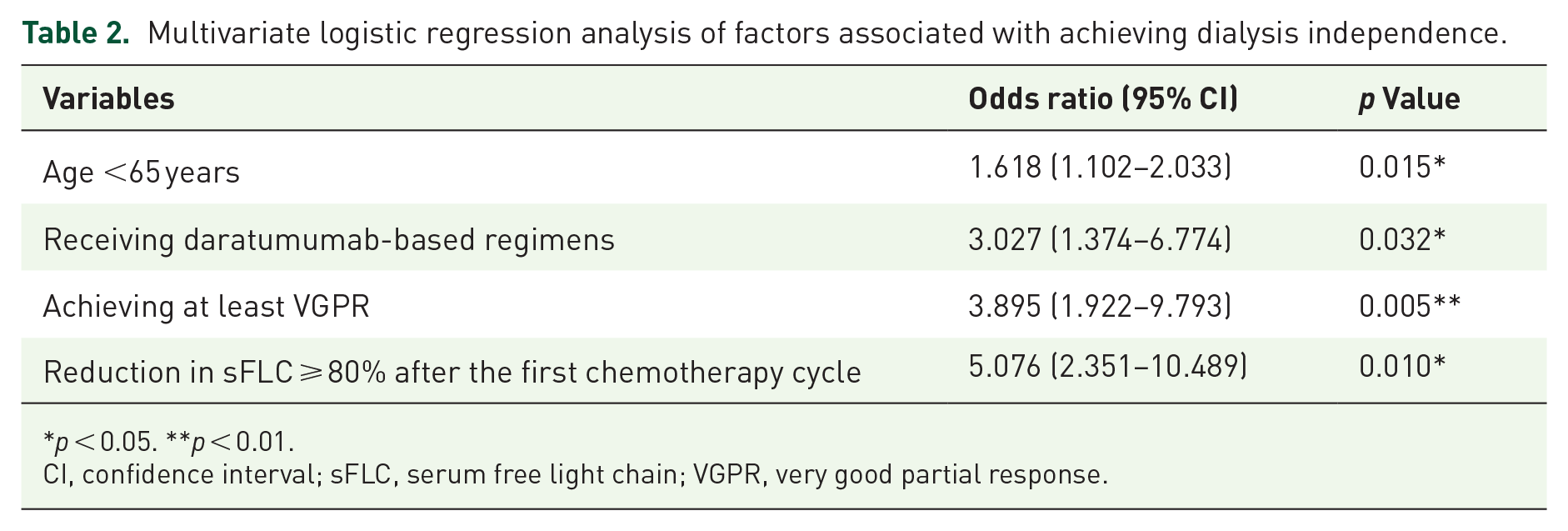
p < 0.05. **p < 0.01.
CI, confidence interval; sFLC, serum free light chain; VGPR, very good partial response.
Survival outcomes
During a median follow-up of 43.7 months (range, 2.1–113.0 months), the median PFS and OS for the entire cohort were 14.4 months (95% CI: 3.6–25.2) and 27.4 months (95% CI: 6.9–47.9), respectively. Compared to NDMM, RRMM with severe renal failure requiring hemodialysis showed poorer PFS (2.6 vs 24.4 months, p < 0.001) and OS (4.2 vs 43.0 months, p < 0.001). Reversal of dialysis dependence and improvement in renal function were associated with significantly better outcomes (PFS: 36.7 vs 9.4 months, p = 0.006; OS: 62.6 vs 17.7 months, p < 0.001; Figure 2(a) and (b).

Survival outcomes in myeloma patients with dialysis dependence and dialysis independence. PFS (a) and OS (b) in all patients (n = 122). PFS (c) and OS (d) in the NDMM patients (n = 87). PFS (e) and OS (f) in the NDMM patients (n = 35).
Among patients with NDMM, although PFS did not differ significantly between the dialysis-independent and dialysis-dependent groups (38.1 vs 23.6 months, p = 0.128), those who achieved dialysis independence demonstrated a significantly prolonged OS (65.1 vs 26.7 months, p = 0.002; Figure 2(c) and (d)). Univariate analysis revealed that high-risk cytogenetic abnormalities and elevated LDH (⩾250 U/L) had a negative effect on the prognosis of NDMM. At the same time, a ⩾80% reduction in sFLC after the first chemotherapy cycle was associated with a favorable prognosis (Tables 3 and 4). Multivariate analysis revealed that dialysis independence (p = 0.039), achieving at least VGPR (p = 0.018), and age <65 years (p = 0.036) were independent predictors of improved OS in patients with dialysis-dependent NDMM (Table 4). Notably, post-dialysis urine output and baseline sFLC levels did not affect prognosis.
Univariate and multivariate analyses of factors associated with PFS among NDMM patients with severe renal failure requiring hemodialysis.

High-risk FISH, defined as the presence of any of del17p, t(4;14), and/or t(14;16).
p < 0.05. **p < 0.01. ***p < 0.001.
BMPC, bone marrow plasma cells; CI, confidence interval; FISH, fluorescence in situ hybridization; HR, hazard ratio; LDH, lactate dehydrogenase; NDMM, newly diagnosed multiple myeloma; PFS, progression-free survival; sFLC, serum free light chain; VGPR, very good partial response;
Univariate and multivariate analyses of factors associated with OS among NDMM patients with severe renal failure requiring hemodialysis.
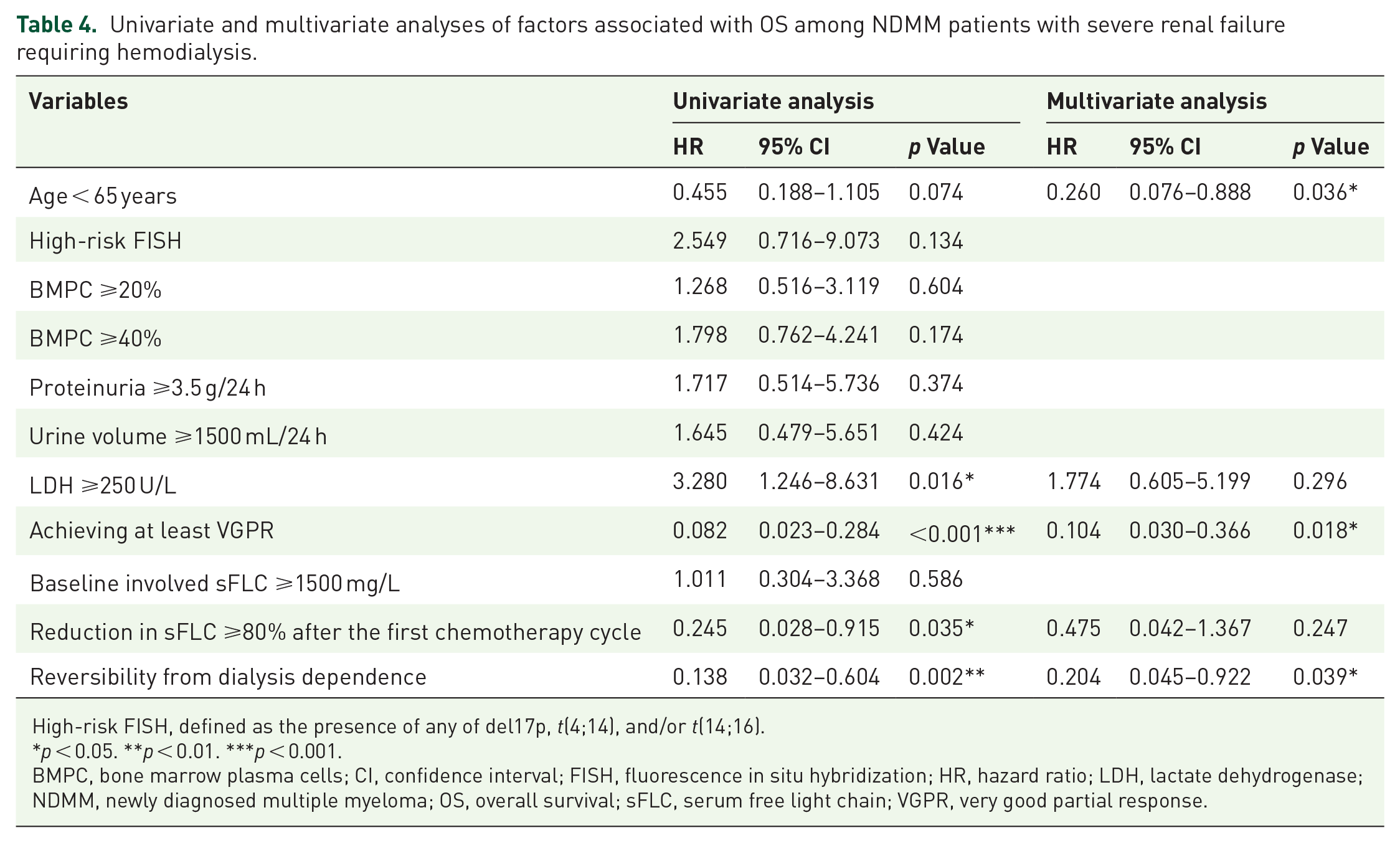
High-risk FISH, defined as the presence of any of del17p, t(4;14), and/or t(14;16).
p < 0.05. **p < 0.01. ***p < 0.001.
BMPC, bone marrow plasma cells; CI, confidence interval; FISH, fluorescence in situ hybridization; HR, hazard ratio; LDH, lactate dehydrogenase; NDMM, newly diagnosed multiple myeloma; OS, overall survival; sFLC, serum free light chain; VGPR, very good partial response.
Dialysis-independent RRMM patients had better PFS (14.0 vs 2.4 months, p = 0.008) and OS (27.4 vs 4.5 months, p = 0.005) compared to dialysis-dependent patients (Figure 2(e) and (f)). In RRMM patients, high-risk cytogenetic abnormalities, BMPC ratio ⩾50%, and elevated LDH levels (⩾250 U/L) were associated with poorer PFS (Table 5). Multivariate analysis identified dialysis independence (p = 0.027), reduction in sFLC ⩾80% after 1 cycle of chemotherapy (p = 0.046), and LDH <250 U/L (p = 0.014) as independent predictors of improved OS (Table 6).
Univariate and multivariate analyses of factors associated with PFS among RRMM patients with severe renal failure requiring hemodialysis.

High-risk FISH, defined as the presence of any of del17p, t(4;14), and/or t(14;16).
p < 0.05. **p < 0.01.
BMPC, bone marrow plasma cells; CI, confidence interval; FISH, fluorescence in situ hybridization; HR, hazard ratio; LDH, lactate dehydrogenase; PFS, progression-free survival; RRMM, relapsed/refractory multiple myeloma; sFLC, serum free light chain; VGPR, very good partial response.
Univariate and multivariate analyses of factors associated with OS among RRMM patients with severe renal failure requiring hemodialysis.

High-risk FISH, defined as the presence of any of del17p, t(4;14), and/or t(14;16).
p < 0.05. **p < 0.01.
BMPC, bone marrow plasma cells; CI, confidence interval; FISH, fluorescence in situ hybridization; HR, hazard ratio; LDH, lactate dehydrogenase; OS, overall survival; RRMM, relapsed/refractory multiple myeloma; sFLC, serum free light chain; VGPR, very good partial response.
Discussion
Up to 10% of patients may develop severe RI requiring hemodialysis, which is associated with a high early mortality rate. 23 However, the survival outcomes and factors influencing dialysis independence in hemodialysis-dependent patients with MM remain poorly understood, particularly in the Chinese population. This study examined the clinical characteristics and survival outcomes of patients with hemodialysis-dependent MM in a multicenter cohort. The findings indicate that achieving at least a VGPR, undergoing daratumumab-based treatment, achieving a reduction in sFLC of ⩾80% after one cycle of chemotherapy, and being younger than 65 years are all significantly associated with dialysis independence. Patients achieving dialysis independence demonstrated improved OS compared to those who remained dialysis-dependent due to MM-induced renal failure. Renal recovery following standardized anti-myeloma therapy is achievable, even in patients with RRMM.
Despite significant advancements in survival outcomes for patients with MM in the era of new therapeutics, the prognosis of patients with dialysis dependence remains notably poor. Haynes et al. 24 reported a median OS of only 10.2 months in 107 patients, 88 of whom required dialysis. Similarly, a nationwide study in the Netherlands observed a median OS of only 1.74 years among 278 dialysis-dependent patients treated with bortezomib-based regimens. 10 In this study, the median OS for all hemodialysis-dependent patients was 27.4 months, with the worst median OS of 4.2 months observed in patients who experienced relapse while still undergoing dialysis. The extended survival observed in this cohort may be attributed to the widespread use of bortezomib-based triplet induction therapy. Bortezomib-based combination therapy is the cornerstone of the first-line treatment for MM. Numerous studies have shown that bortezomib-based regimens induce rapid and profound hematologic and renal responses, potentially reversing renal dysfunction and reducing the need for dialysis.15,25 In our study, 44.4% of patients receiving bortezomib-based treatment achieved at least VGPR compared to 14.3% of those receiving IMiD-based therapy, resulting in a significantly higher overall response rate in the bortezomib-treated group. Furthermore, a study comparing bortezomib-based doublet and triplet regimens in MM patients with RI suggested that the bortezomib–cyclophosphamide–dexamethasone triplet regimen may provide superior renal responses compared to bortezomib–dexamethasone. However, the difference was not statistically significant. 26 Similarly, a study in Greece proposed that bortezomib-based triplet regimens may enhance renal responses and increase dialysis independence relative to bortezomib–dexamethasone. 11 In our study, 65.6% of patients received bortezomib–cyclophosphamide–dexamethasone or bortezomib–lenalidomide–dexamethasone triplet regimens, which may have contributed to the improved prognosis. Nevertheless, the overall prognosis of dialysis-dependent MM patients remains poor, particularly for those with high-risk cytogenetic abnormalities, elevated LDH levels, a high proportion of BMPCs, and moderate to severe proteinuria.
Daratumumab has been demonstrated to be both safe and effective in treating RRMM with RI in dialysis-dependent patients.27 –29 A phase II clinical trial reported an overall response rate of 47% in 17 patients with MM undergoing dialysis and treated with daratumumab and dexamethasone. 30 Furthermore, a phase III trial showed that the daratumumab–bortezomib–dexamethasone regimen improved PFS compared to bortezomib–dexamethasone in RRMM patients with creatinine clearance between 20 and 60 mL/min/1.73 m2. 31 Recent studies have investigated daratumumab and PI combinations in front-line induction settings for MM therapy.31,32 However, these studies excluded patients with renal insufficiency and a creatinine clearance of less than 40 mL/min. In our study, 41.2% of patients treated with bortezomib and daratumumab achieved at least VGPR, with the highest proportion observed among patients who recovered from dialysis dependence. This finding suggests that daratumumab and PI-based regimens may hold significant promise for patients with dialysis-dependent MM. Despite these promising results, daratumumab-based regimens carry specific limitations in dialysis-dependent populations, including poor mobilization of hematopoietic stem cell in transplant-eligible MM patients 33 and increased risks of infusion-related reactions, especially in fluid-restricted patients. 34
Autologous hematopoietic stem cell transplantation (HSCT) has been shown to improve renal function in up to one-third of patients and restore dialysis independence in over one-quarter of cases.35,36 The ability of high-dose therapy to enhance responses in patients with dialysis-dependent MM warrants recognition. In our cohort, two patients underwent autologous HSCT, achieved complete response (CR), and successfully attained dialysis independence. Similarly, data from the French transplant registry, as reported by Augeul-Meunier et al., 37 indicated that 43% of patients undergoing dialysis achieved CR following autologous HSCT compared with only 5% achieving CR prior to transplantation.
Importantly, our findings highlight that renal recovery should not be viewed merely as a secondary outcome, but rather as a pivotal biomarker for evaluating both treatment efficacy and remission status in MM. The strong association between dialysis independence and survival outcomes (OS: 62.6 vs 17.7 months, p < 0.001; PFS: 36.7 vs 9.4 months, p = 0.006) underscores its clinical relevance. Notably, the 27 patients who achieved renal recovery exhibited significantly higher rates of deep hematologic responses (⩾VGPR: 77.8% vs 24.2%, p < 0.001), suggesting that profound tumor burden reduction facilitates renal recovery, while restored kidney function may improve treatment responses. Multivariate analysis further revealed that dialysis dependence was associated with shorter OS, consistent with previous findings. In our study, achieving at least VGPR, a reduction in sFLC of ⩾80% after one cycle of chemotherapy, and an age of less than 65 years were strongly associated with dialysis independence. Early and profound hematological responses are fundamental to renal recovery and independence from dialysis. β2-MG is a critical prognostic factor in MM, reflecting both renal function and tumor burden. 38 Our study confirmed that β2-MG levels are predictive of renal recovery and dialysis independence in patients with MM.
Almost all studies emphasize that the renal response depends on an early, substantial reduction in serum FLCs. 39 In the MYRE study, sFLC concentrations below 500 mg/L after the first chemotherapy cycle were independently associated with renal response in dialysis-dependent patients. 40 However, in end-stage renal disease, reduced renal clearance may alter sFLC kinetics, potentially overestimating tumor burden or confounding prognostic interpretation. 41 Reduction in sFLC ⩾80% after 1 cycle of chemotherapy was also related to dialysis dependence and better survival in our NDMM and RRMM cohorts. Unfortunately, continuous FLC monitoring was not performed for all patients in this study, which is a limitation. This study’s retrospective design and classification of dialysis status after treatment initiation may introduce survivorship bias, as patients achieving renal recovery inherently survived long enough to discontinue dialysis. While we adjusted for baseline covariates, unmeasured confounders related to time-varying dialysis status could persist. Future studies with prospective design may address this issue properly.
Conclusion
This study is among the largest investigations on dialysis-dependent patients with MM at diagnosis and relapse in the Chinese population. Severe RI, such as patients with MM undergoing dialysis, whether upfront or at relapse, is a potentially reversible condition that requires prompt treatment. Achieving a good hematological response and dialysis independence are critical goals for ensuring the long-term survival of patients with MM with severe renal failure requiring dialysis.
Supplemental Material
sj-pdf-1-tam-10.1177_17588359251357682 – Supplemental material for Dialysis dependence is associated with poor prognosis in multiple myeloma: a multicenter retrospective cohort study
Supplemental material, sj-pdf-1-tam-10.1177_17588359251357682 for Dialysis dependence is associated with poor prognosis in multiple myeloma: a multicenter retrospective cohort study by Ji-nuo Wang, Chenyun Wang, Jinping Ying, Gaofeng Zheng, Xiaoyan Han, Peng An, Gang Wang, Fei Chen, Li Yang, Yang Yang, Donghua He, Jingsong He, Yuanshuai Chen, Wenjun Wu and Zhen Cai in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors thank all patients and their families for their trust, respect, and support. They also acknowledge all the clinicians for their help in accomplishing this work.
Declarations
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.