
Abstract
Background:
The presence of level IV/V metastasis is a significant prognostic factor for patients with oral and oropharyngeal cancer, while level IV lymphadenopathy defines the N3 stage in nasopharyngeal carcinoma. However, the current staging system for hypopharyngeal squamous cell carcinoma (HPSCC) does not consider the location of involved nodes.
Objectives:
To evaluate the risk factors and prognostic impact of level IV/V metastasis in patients with HPSCC.
Methods:
The analysis included 2740 HPSCC patients from the SEER (Surveillance, Epidemiology, and End Results) database, followed by a validated study on 232 patients with pathologically positive nodes (pN+) at our center.
Results:
Of the 2740 patients, 1961 presented with metastatic lymph nodes (LNs), 20.8% and 14.1% had nodal involvement in level IV and level V, respectively. Multivariate analysis revealed that N3 and M1 stages were independently associated with level IV/V metastasis. Level IV metastasis was the sole independent adverse factor for overall survival (OS) among all LN regions (p < 0.05). Regarding cancer-specific survival (CSS), only level IV and V involvement were independent predictors of prognosis (p < 0.05). The rate of pN+ at levels IV and V in our center was 35.8% and 16.4%, respectively. The advanced pN stage was independently associated with metastasis to level IV or V. Patients with level IV/V metastasis had significantly higher rates of regional recurrence and distant metastases (p < 0.001). Multivariate analysis confirmed a significant association regarding OS, CSS, locoregional relapse-free survival (LRFS), or distant metastasis-free survival between patients with and without level IV metastasis (p < 0.05). Patients with level IV/V disease exhibited decreased survival rates across stages pN1 to pN3. Postoperative chemoradiotherapy improved LRFS in patients with level IV lymphadenopathy and OS/CSS in patients with level V metastasis.
Conclusion:
Metastasis to level IV/V was associated with a worse prognosis in HPSCC patients. The level IV/V should be considered for future improvements to the staging system.
Design:
A retrospective study.
Keywords
Introduction
Due to the extensive lymphatic drainage network and atypical symptoms associated with hypopharyngeal squamous cell carcinoma (HPSCC), over 80% of patients are diagnosed with locoregionally advanced disease (stages III–IV) at presentation. 1 Cervical lymph node (LN) metastasis holds significant prognostic implications for patients with HPSCC. To achieve better treatment outcomes, it is necessary to acquire information on the distribution patterns of cervical nodal metastasis, and whether the lower neck involvement is associated with a worse prognosis. 2 Notably, the presence of extranodal extension (ENE), multiple LN metastases, and lymphatic invasion has been proven to correlate with worse prognosis in head and neck squamous cell carcinoma (HNSCC).2–4 Our previous research has shown that the existence of three or more positive LNs (NPLN ⩾ 3) and an LN ratio above 0.138 (LN ratio ⩾ 0.138) are independent prognostic indicators for HPSCC. 5 In addition, the presence of LN metastases in lower neck levels appears to be associated with a poorer prognosis and an increased risk of developing distant metastases in oral cancer.6,7 Based on the treatment outcomes in the EORTC trial, 3 the presence of levels IV and V lymphadenopathy in patients with oral and oropharyngeal cancer is regarded as a significant prognostic factor.4,8 Therefore, the National Comprehensive Cancer Network (NCCN) guidelines classified level IV/V metastasis as an intermediate risk factor for recurrence in the oral cavity or oropharyngeal cancers.3,4,9 However, the characteristics and outcomes of HPSCC patients who have level IV/V metastasis were not comprehensively reported up to date. Treatment recommendations for this specific population among HPSCC are also lacking in NCCN guidelines.
The involvement of neck nodes in tumors does not occur randomly.7,10,11 A detailed analysis of LN involvement patterns is crucial to assess the prognostic value of level IV/V metastases. For nasopharyngeal carcinoma, level IV lymphadenopathy is defined as the N3 stage. However, for HPSCC, the current staging system does not take into account the location of involved nodes. The previous studies have relied, to some extent, solely on clinical or radiological data from a heterogeneous patient population. To reveal the impact of level IV/V lymphadenopathy on the prognosis of HPSCC, we analyzed the patterns of nodal spread using information from the SEER (Surveillance, Epidemiology, and End Results) database. In addition, the significant multivariate relationships among risk factors for level IV/V metastasis were investigated. To verify the findings from the SEER database, we further explored the prognosis of HPSCC patients with pathologically positive LNs (pN+) treated with pharyngolaryngectomy and neck dissection in our center. Moreover, the role of adjuvant therapy in improving the prognosis according to these risk factors was studied.
Materials and methods
SEER database
The patient data from 2004 to 2015 were collected using the SEER software available at “https://seer.cancer.gov.” The selection process is provided in Figure 1. The records were based on the following primary sites: C129, C130, C131, C132, C138, and C139 as per the site codes of ICD-O-3. Exclusion criteria were as follows: AJCC stage status unavailable; not squamous cell carcinomas; without positive histology; without complete survival information; not the first tumor; total number of tumors was not 1; TNM stage status unavailable; and the variable of CS (Collaborative Stage, which allows combined pathological and clinical “mixed” or “best” stages to be captured) site-specific factor 3/4/5/6 was 999 (lacking information on LN metastasis was excluded). After screening, 2740 patients were included.

Data selection process from SEER database.
The analysis covered clinical and sociodemographic characteristics as well as treatment modalities (Table 1). The correlation between surgery and radiation was extracted from the variables of radiation sequence with surgery, the reason for no cancer-directed surgery, and radiation recode. The type of surgery of the primary site was extracted from the variable of RX Summ-Surg Prim Site (1998+). The neck dissection was extracted from the variable of regional nodes examined (1988+). The distribution of metastases in cervical LNs was determined by the variable of CS site-specific factors 3, 4, 5, and 6. The HPSCC cancer-specific survival (CSS) and non-CSS were extracted from the SEER variables of cause-specific death classification and other causes of death classifications.
Patient characteristics in SEER database.

SEER, Surveillance, Epidemiology, and End Results.
Patient data in our center
We selected the verification cohort with the following criteria for our study: (1) HPSCC patients who underwent pharyngolaryngectomy as the primary surgery combined with neck dissection, followed by postoperative radiotherapy or concurrent chemoradiotherapy (CCRT), (2) HPSCC patients with pN+ and no evidence of distant metastasis, and (3) treated at the Eye & ENT Hospital, Fudan University from November 2011 to December 2020. Exclusion criteria were as follows: any T4b stage; those who underwent induction chemotherapy or any antitumor treatment prior to surgery; patients presenting with a synchronous second primary tumor; recurrent HPSCC; patients who failed to complete the treatment; and incomplete clinical data or follow-up information.
After screening, 232 patients with pN+ were eligible for inclusion. All patients underwent electronic laryngoscopy, neck computed tomography (CT) and/or magnetic resonance imaging (MRI), esophageal gastroscopy, abdominal ultrasonography, as well as chest radiography. The histopathological specimens, including primary and neck dissection samples, were thoroughly examined by pathologists dedicated to head and neck tumors. Special attention was paid to record the margins, ENE, perineural invasion, vascular/lymphatic invasion, and pathological node status (numbers of total and positive LNs, specific regions of LN metastasis). The LN ratio was calculated as the ratio of positive LNs to the exact number of LNs removed, regardless of whether bilateral or unilateral neck dissection was performed.
The decision regarding postoperative adjuvant therapy was made by a multidisciplinary team. Restaging was performed according to the 8th edition of the AJCC for HPSCC. Three-dimensional conformal radiotherapy, intensity-modulated radiotherapy, or volumetric modulated arc therapy at a curative dose of 54–70 Gy was delivered based on radiologic or pathologic characteristics. Cisplatin alone was prescribed for concurrent chemotherapy depending on the adverse prognostic features and also the patient’s tolerance during radiotherapy.
Information on tumor control and survival status was obtained through outpatient visits or telephone follow-ups. Electronic laryngoscopy and MRI/CT scans were performed regularly. Follow-up time started from the first treatment to December 2023. The median follow-up time was 74.37 months (range, 5.77–145 months). The reporting of this study conforms to the ESMO Guidance for Reporting Oncology Real-World evidence (GROW) statement 12 (Supplemental Files).
Statistical analysis
The Chi-square test and Fisher’s exact test were performed to compare categorical variables among different groups. Multivariate analysis with logistic regression was conducted to determine the odds ratio (OR) and independent factors by including significant variables identified in the univariate analysis. Kaplan–Meier method was used to estimate the overall survival (OS), CSS, locoregional relapse-free survival (LRFS), and distant metastasis-free survival (DMFS). Survival was calculated as the date of first administration of therapy to the date of the event or last follow-up. The log-rank test and Cox hazard model were used in univariate and multivariate analyses, respectively. Only variables with a p-value less than 0.05 in the univariate analyses were included in the multivariate Cox proportional hazard regression analyses. All statistical analyses were carried out using SPSS 29.0 (SPSS, Chicago, IL, USA), and a two-sided p-value less than 0.05 was deemed statistically significant.
Results
Patient characteristics in the SEER database
A total of 2740 patients were enrolled (Table 1), including 2236 males and 504 females, with a median age of 62.5 years. The majority of patients were white (75.6%), originating from the pyriform sinus (52.4%), with moderately differentiated tumors (41.6%) and stage IVA cancer (48.2%).
The distribution of regional LN spread is shown in Table 2. The overall metastasis rates in level I–VII and retropharyngeal LNs were 10.8%, 45.4%, 32%, 14.9%, 10.1%, 1.9%, 0.9%, and 2.6%. Among the 1961 patients with LN involvement, 407 (20.8%) and 277 (14.1%) developed metastasis in level IV and level V, respectively. Univariate analysis (Supplemental Table 1) revealed a significantly higher rate of N3 status and M1 status in patients with level IV or V metastasis than those without (p < 0.05). The multivariate analysis (Table 3) demonstrated that race of black (OR = 1.381), male (OR = 1.474), N3 status (OR = 1.482), involvement of levels III (OR = 3.509), V (OR = 2.42), and VI (OR = 2.15) were independently associated with level IV metastasis. Race of others (OR = 1.728), N3 status (OR = 1.882), M1 status (OR = 1.609), involvement of levels IV (OR = 2.413), VI (OR = 2.329), and retropharyngeal LNs (OR = 5.222) were independently associated with level V metastasis.
Distribution of cervical lymph node metastases in SEER database.

N+, lymph node metastasis; SEER, Surveillance, Epidemiology, and End Results.
Multivariate analysis of independent correlators for level IV/level V metastasis among patients with N+ status in SEER database.

p Value in bold statistically significant.
CI, confidence interval; N+, lymph node metastasis; OR, odds ratio; SEER, SEER, Surveillance, Epidemiology, and End Results.
Relationship between level IV/V metastasis and survival rate in the database
Among the entire cohort, patients with level IV metastasis exhibited worse survival outcomes, the 5-year OS and CSS rates were 22.8% and 28%, respectively. Conversely, patients without level IV metastasis demonstrated higher 5-year OS and CSS rates, 30.8% and 39.9%, respectively (p < 0.001). Similarly, those with level V metastasis had a lower survival rate, the 5-year OS and CSS rates were 19.2% and 22.3%, respectively. By contrast, patients without level V metastasis achieved better outcomes, the 5-year OS and CSS rates were 30.8% and 40.1%, respectively (p < 0.001). For a more detailed analysis of survival rates, please refer to Table 4. Multivariate analysis (Table 4) revealed a significant association between OS or CSS and age, race, year of diagnosis, primary subsite, T status, N status, M status, neck dissection, surgery to primary lesion, radiotherapy, chemotherapy, and marital status (p < 0.05). Furthermore, level IV involvement was the sole independent prognostic factor for OS (hazard ratio (HR) = 1.167, p = 0.029) among all metastatic LN regions. In terms of CSS, only level IV involvement (HR = 1.176, p = 0.036) and level V (HR = 1.216, p = 0.021) were independent predictors of prognosis.
Univariate and multivariate analyses predicting OS and CSS for all the patients in the SEER database.

p value in bold statistically significant.
CI, confidence interval; CSS, cancer-specific survival; HR, hazard ratio; OS, overall survival; SEER, Surveillance, Epidemiology, and End Results.
The survival rates of patients with level IV/V involvement were compared separately to those without level IV/V metastasis. The 5-year OS and CSS of patients with level IV metastasis (IV+) (Figure 2(a)) were both inferior to those with IV stages N0 to N2 (p < 0.001), but without significant difference compared to patients with N3 (OS: 22.8% vs 19.1%, p = 0.123; CSS: 28% vs 23.4%, p = 0.138). These results indicated that patients with level IV metastasis should be defined as the N3 stage. The survival rates of patients with level V metastasis (V+) consistently demonstrated worse outcomes compared to those with V− stages N0 to N2 (p < 0.001; Figure 2(b)), but without significant difference compared to patients with N3 (p > 0.05). These results suggested that patients with level V metastasis should also be defined as the N3 stage.

Comparison of overall survival and cancer-specific survival between patients with and without level IV/V metastasis in the SEER database. (a) The survival curves were compared among patients with and without level IV metastasis (IV+ vs IV−), stratified by N staging categories (N0, N1(IV−), N2(IV−), N3(IV−)). (b) The survival curves were compared among patients with and without level V metastasis (V+ vs V−), stratified by N staging categories (N0, N1(V−), N2 (V−), N3(V−)).
To investigate the therapeutic approaches that may enhance the survival outcomes of patients with metastasis in level IV/V, we conducted univariate/multivariate analyses (Supplemental Table 2). The findings demonstrated that the administration of neck dissection (HR = 0.555; HR = 0.582), radiotherapy (HR = 0.492; HR = 0.522), and chemotherapy (HR = 0.412; HR = 0.408) independently and significantly (p < 0.001) improved survival rate.
General clinical data analysis in our center
The staging and LN distribution patterns from the SEER database were predominantly based on clinical diagnosis rather than pathological information. Distant metastasis, LN involvement, and multimodality therapy significantly impact the survival outcomes. To minimize statistical bias and to further validate the impact of level IV/V metastasis, we conducted an evaluation on a cohort of patients from our center.
The general information of the patients is shown in Supplemental Table 3. The study population included 232 men aged 39–74 years. The majority of tumors originated from the pyriform sinus (83.6%), with a moderate differentiation level in pathology (81%), unilateral positive LNs (82.8%), and stage IVA disease (62.9%). ENE/pN3/IVB stage was observed in 49 patients (21.1%).
The distribution of the LN spread is shown in Figure 3. Based on pathologic diagnosis, the LNs metastasis rates to level I–VI, retropharyngeal LNs, and parotid LNs were 5.6%, 82.3%, 76.7%, 35.8%, 16.4%, 7.3%, 9.1%, and 1.3%, respectively. A total of 83 and 38 patients developed metastasis in level IV and level V (Table 5), respectively. Bilateral positive LNs, NPLN ⩾ 3, LN ratio ⩾ 0.138, esophageal invasion, pT3/pT4, pN2/pN3 (ENE), involvement of level III, V, VI, and parotid nodes were more frequent in patients with level IV metastasis than those without (p < 0.05). Bilateral positive LNs, NPLN ⩾ 3, LN ratio ⩾ 0.138, positive margin, perineural invasion, pN3 (ENE), involvement of level I, III, IV, VI, retropharyngeal LNs, and parotid LNs were more frequent in patients with level V metastasis (p < 0.05). The multivariate analysis (Supplemental Table 4) demonstrated that LN ratio ⩾ 0.138, esophageal invasion, pT3/pT4, pN2/pN3 (ENE), and involvement of level V were independently associated with metastasis to level IV. pN3 (ENE) and involvement of level IV were independently associated with metastasis to level V.

Distribution of LN metastasis among 232 patients with pathologically positive LNs in our center.
The correlation between clinical factors and level IV/level V metastasis for 232 patients with pathologically positive lymph nodes in our center.

p value in bold, statistically significant.
ENE, extranodal extension; LN, lymph node; NPLN, the number of positive lymph nodes.
Survival outcomes and the prognostic factors
As indicated in Supplemental Table 3, local recurrence, regional recurrence, and distant metastases were observed in 61, 63, and 69 patients, respectively. Among the patients with distant metastasis, 43 had lung/mediastinum-specific metastases, while the remaining 26 had metastases involving multiple organs or organs other than lungs/mediastinum. Interestingly, level V involvement increased the risk of distant metastasis to multiple organs or non-lung/mediastinum organs (54.2% vs 28.9%, p = 0.039, Supplemental Table 5). The 5-year LRFS rate of patients with and without level IV disease was 24.4% versus 74.4% (p < 0.001) and the 5-year DMFS was 37.5% versus 80.5% (p < 0.001; Supplemental Table 6). The 5-year LRFS rate of patients with and without level V involvement was 20.7% versus 64.3% (p < 0.001) and the 5-year DMFS rate was 25.2% versus 74.8% (p < 0.001, Supplemental Table 6). The multivariate analyses (Table 6) in predicting LRFS showed that postcricoid region (HR = 2.762), bilateral positive LNs (HR = 1.667), positive margin (HR = 1.706), level IV (HR = 4.687), and retropharyngeal nodes involvement (HR = 1.984) were significantly correlated with worse outcomes (p < 0.05). Bilateral positive LNs (HR = 1.803), ENE (HR = 4.026), level IV (HR = 2.569), and level V (HR = 1.875) lymphadenopathy were independently correlated with poorer DMFS (p < 0.05).
Multivariate Cox regression analyses predicting OS, CSS, LRFS, and DMFS for 232 patients with pathologically positive lymph nodes in our center.

p value in bold, statistically significant.
CI, confidence interval; CSS, cancer-specific survival; DMFS, distant metastasis-free survival; ENE, extranodal extension; HR, hazard ratio; LN, lymph node; LRFS, locoregional relapse-free survival; NPLN, the number of positive lymph nodes; OS, overall survival; R, reference.
By the end of the last follow-up, 116 patients had died, with 106 (91.4%) deaths caused by the progression of HPSCC, while 10 patients (8.6%) died from secondary primary cancer or cardiovascular disease. Both level IV and V lymphadenopathy had a significantly adverse impact on the 5-year OS (level IV: 18.4% vs 70.6%; level V: 18% vs 59%) and CSS rate (level IV: 20.9% vs 73.6%; level V: 18.8% vs 62.6%; p < 0.001, Supplemental Table 6). The multivariate analyses of factors to predict OS and CSS showed that postcricoid region (HR = 3.072; HR = 3.319), bilateral positive LNs (HR = 2.067; HR = 2.154), vascular/lymphatic invasion (HR = 2.076; HR = 2.017), level IV (HR = 4.634; HR = 4.687), and retropharyngeal nodes involvement (HR = 1.847; HR = 2.028) significantly correlated with inferior outcomes (p < 0.05, Table 6).
Relationship between level IV/V metastasis and N stage
Among the whole cohort, patients with level IV/V metastasis exhibited the worst survival outcomes (p < 0.001, Figure 4(a) and (b)). The 5-year OS, CSS, LRFS, and DMFS rates were significantly lower in patients with level IV or level V metastasis compared to those without level IV or level V metastasis, regardless of N stage (N1 to N3, p < 0.001). Our results indicated that patients with level IV or V metastasis should be defined as more than the N3 stage. Subsequently, a separate analysis was conducted to investigate the impact of level IV/V lymphadenopathy on survival outcomes in the N3 stage. Surprisingly, even at the N3 stage, patients with level IV/V involvement demonstrated significantly worse 5-year OS, CSS, and LRFS (p < 0.05) compared to those without level IV/V disease (Figure 5(a) and (b)).
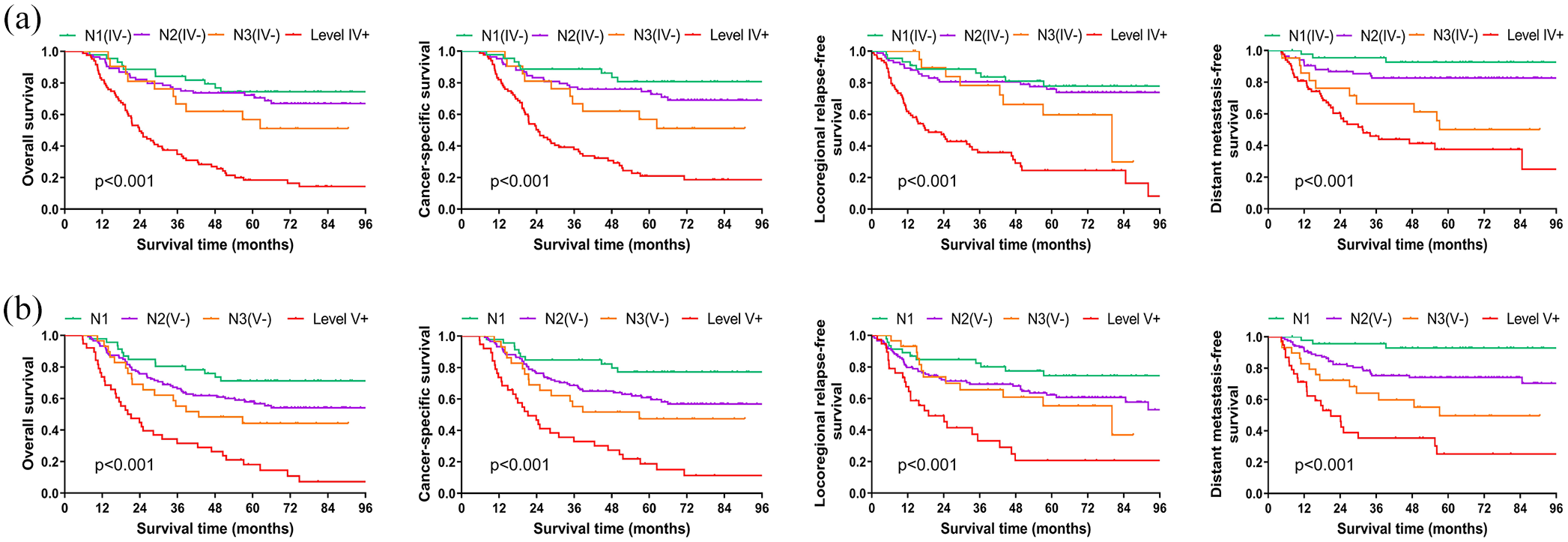
Comparison of overall survival, cancer-specific survival, locoregional relapse-free survival, and distant metastasis-free survival between patients with and without level IV/V metastasis in our center. (a) The survival curves were compared among patients with and without level IV metastasis (IV+ vs IV−), stratified by N staging categories (N1(IV−), N2(IV−), N3(IV−)). (b) The survival curves were compared among patients with and without level V metastasis (V+ vs V−), stratified by N staging categories (N1, N2(V−), N3(V−)).

At the N3 stage, a comparison was conducted to assess overall survival, cancer-specific survival, locoregional relapse-free survival, and distant metastasis-free survival between patients with and without level IV/V metastasis in our center. (a) Level IV− versus level IV+. (b) Level V− versus level V+.
The role of CCRT
Despite the lack of a significant benefit from CCRT compared to radiotherapy alone (Supplemental Table 6) in the entire cohort, a different scenario emerged when we analyzed two subgroups based on the involvement of level IV/V. The patients with level IV metastasis who received CCRT after surgery had a significantly better 5-year LRFS (34.7% vs 10.6%, p = 0.033) compared to those who received radiotherapy alone (Figure 6(a)). On the contrary, CCRT did not present an advantage over radiotherapy alone in patients without level IV metastasis (Figure 6(b)). Moreover, the patients with level V metastasis who received CCRT had a significantly better 5-year OS (28.6% vs 0%, p = 0.007) and CSS (28.6% vs 0%, p = 0.014) compared to those who received radiotherapy alone (Figure 7(a)). However, CCRT did not contribute a significant advantage over radiotherapy alone in patients without level V lymphadenopathy (Figure 7(b)).

Overall survival, cancer-specific survival, locoregional relapse-free survival, and distant metastasis-free survival curves according to patients’ postoperative treatment modality (CCRT vs RT alone). (a) Patients with level IV metastasis (IV+). (b) Patients without level IV metastasis (IV−).

Overall survival, cancer-specific survival, locoregional relapse-free survival, and distant metastasis-free survival according to patients’ postoperative treatment modality (CCRT vs RT alone). (a) Patients with level V metastasis (V+). (b) Patients without level V metastasis (V−).
Discussion
The presence of LN metastasis is considered one of the most significant prognostic factors, leading to the classification of patients as stage III or IV disease for HNSCC. 2 Notably, N2 stage, ENE, multiple pN+, LN ratio, as well as lymphatic invasion have been correlated with unfavorable clinical outcomes.9,13–15 However, evidence is lacking in terms of whether the location of the involved LN might impact the prognosis of HPSCC. For the first time, our study demonstrated that the presence of level IV/V lymphadenopathy significantly outweighs other parameters associated with LNs in predicting the prognosis for HPSCC.
The current research on the distribution of LN metastasis and its impact on prognosis remains limited in patients with HPSCC. The patterns of LN spread in 244 newly diagnosed HPSCC patients were assessed using pre-treatment MRI. 16 The overall lymph node metastasis (LNM) rates to levels II–VI and retropharyngeal LNs were 59.0%, 52.9%, 14.3%, 1.6%, 2.9%, and 16.4%, respectively. However, it should be noted that clinical diagnosis may not necessarily align with pathological diagnosis, especially regarding the rate of cervical LN involvement, potentially leading to an underestimation of metastasis rate in level IV/V. The metastatic pattern of LNs in HPSCC was investigated in another study, which assessed 75 dissected lateral neck specimens. The study found that the order of metastatic ratio was level II (90.5%), level III (76.2%), level IV (41.3%), level V (15.9%), level I (7.9%), and level VI (3.2%). 17 These findings were in close accordance with our real-world study. It is generally believed that level IV/V metastasis in HPSCC occurs secondarily to level II–III involvement.11,18,19 Consequently, the vast majority of patients exhibiting metastasis in the level IV/V also presented with multiple LN involvement within the regional LNs.7,20–22 In our study, a higher N stage was identified as a significant risk factor for level IV/V metastasis, which was consistent with previous reports of oral cancer.23,24 More significantly, our research has revealed a close correlation between level IV/V metastasis and ENE, thereby indicating an unfavorable prognosis for level IV/V lymphadenopathy.6,23,24
The NCCN guidelines for HNSCC specifically address the risk of level IV/V metastasis related to oral and oropharyngeal cancer, where it is regarded as an intermediate risk factor for recurrence. Therefore, postoperative radiotherapy or CCRT is recommended for such cases.2,9 The presence of level IV/V metastases in oral cancer was associated with an elevated risk of neck recurrence and signifies an unfavorable prognosis.23–26 In our study, only level IV and level V among all metastatic LN regions were found to be independent predictors of prognosis in the SEER database. More importantly, cases with level IV/V involvement have worse outcomes in the subgroups of patients with pN1-N3 disease in our center. Studies of oral cancer have revealed that even in patients with ENE/pN3b, there remains considerable variation in prognosis.6,27 Notably, individuals with metastasis to the IV/V region exhibited the worst prognosis and should therefore be classified as high risk within the N3b population.6,27 Following neck LN dissection, the presence of IV/V metastasis still remains a significant risk factor for regional recurrence.24,28 Level IV/V represents a critical LN region, and the presence of level IV/V lymphadenopathy is indicative of an elevated risk for occult metastases in the subsequent lymphatic drainage pathway and distant metastasis. 6
It is widely acknowledged that a high frequency of distant metastases occurs predominantly in patients with advanced LN involvement.29–31 The study of 111 patients with HNSCC 32 revealed through univariate and multivariate analyses that level IV lymphadenopathy had an independent impact on pulmonary metastases. The currently accepted theory suggests a sequential metastasis through the locoregional lymphatics into the bloodstream.32–34 In our study, level IV/V involvement was significantly associated with distant metastasis at initial presentation and after treatment. It has been observed that the involvement of level V increases the likelihood of distant metastasis to multiple organs. Thus, if level V lymphadenopathy was detected, the cancer should be considered highly aggressive. 6 Due to the high risk of regional recurrence and distant metastasis associated with IV/V involvement in HPSCC, patients diagnosed as pN1 or pN2 after surgery should still be considered at an elevated risk level. An aggressive and intensified therapeutic approach might be suitable for these patients.
Unlike oral cancer or oropharyngeal cancer, the NCCN guidelines do not provide specific recommendations for patients with level IV/V metastasis in HPSCC. The SEER database demonstrated that patients who underwent neck dissection exhibit a better prognosis compared to those who did not receive neck dissection. A consensus has yet to be reached regarding the application of postoperative adjuvant therapy. Our previous research indicated that patients with an NPLN of 3 or higher who underwent postoperative CCRT exhibited significantly improved OS, CSS, and LRFS compared to those who received radiotherapy alone, 5 which was consistent with other relevant studies on HNSCC. 35 Those findings suggested that LN metastasis burden seemed to be an appropriate selection criterion for CCRT. Li analyzed patients with HNSCC who underwent surgical treatment, specifically focusing on those with LN metastasis but without positive margins or ENE. 35 In patients with levels IV/V involvement, adding chemotherapy to postoperative radiotherapy resulted in a 24% reduction in recurrence risk and a 20% decrease in mortality risk. In our study, postoperative CCRT significantly improved the rates of LRFS and OS in patients with level IV/V metastasis. The administration of CCRT, however, did not yield a significant improvement in DMFS. The poor survival of the patients with level IV/V involvement may be explained by the high incidence of distant metastasis (level IV: 50.6%; level V: 63.2%). It is worthwhile to explore other potential adjuvant therapies to decrease the rate of distant metastasis.
It is important to acknowledge the limitations of our current study. The first point is that our study was retrospective, and not all patients underwent nodal dissections ranging from level I to level VI. The second point was radiation dose, 54–70 Gy was delivered to the neck based on pathologic information and also at the discretion of the supervising physician. Whether different dose levels might impact OS, DMFS, and LRFS needs to be explored in the future.
Conclusion
To our knowledge, this study is the first to demonstrate that metastasis to level IV/V was significantly associated with a poorer prognosis in HPSCC patients. Therefore, adjuvant therapy (radiotherapy or CCRT) is strongly recommended following surgery for patients presenting with level IV/V metastasis. We suggest taking into account the location of lymphadenopathy for the staging system in the future. Our results indicated that patients with level IV or V metastasis should be defined as ⩾N3 stage.
Supplemental Material
sj-docx-1-tam-10.1177_17588359241312079 – Supplemental material for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma
Supplemental material, sj-docx-1-tam-10.1177_17588359241312079 for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma by Ruichen Li, Qi Wang, Siyuan Ma, Ji Li, Yang Zhao and Xiaoshen Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-2-tam-10.1177_17588359241312079 – Supplemental material for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma
Supplemental material, sj-docx-2-tam-10.1177_17588359241312079 for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma by Ruichen Li, Qi Wang, Siyuan Ma, Ji Li, Yang Zhao and Xiaoshen Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-3-tam-10.1177_17588359241312079 – Supplemental material for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma
Supplemental material, sj-docx-3-tam-10.1177_17588359241312079 for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma by Ruichen Li, Qi Wang, Siyuan Ma, Ji Li, Yang Zhao and Xiaoshen Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-4-tam-10.1177_17588359241312079 – Supplemental material for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma
Supplemental material, sj-docx-4-tam-10.1177_17588359241312079 for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma by Ruichen Li, Qi Wang, Siyuan Ma, Ji Li, Yang Zhao and Xiaoshen Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-5-tam-10.1177_17588359241312079 – Supplemental material for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma
Supplemental material, sj-docx-5-tam-10.1177_17588359241312079 for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma by Ruichen Li, Qi Wang, Siyuan Ma, Ji Li, Yang Zhao and Xiaoshen Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-docx-6-tam-10.1177_17588359241312079 – Supplemental material for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma
Supplemental material, sj-docx-6-tam-10.1177_17588359241312079 for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma by Ruichen Li, Qi Wang, Siyuan Ma, Ji Li, Yang Zhao and Xiaoshen Wang in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pdf-7-tam-10.1177_17588359241312079 – Supplemental material for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma
Supplemental material, sj-pdf-7-tam-10.1177_17588359241312079 for The association between level IV/V metastasis and the recurrence, distant metastasis, and survival outcomes in hypopharyngeal squamous cell carcinoma by Ruichen Li, Qi Wang, Siyuan Ma, Ji Li, Yang Zhao and Xiaoshen Wang in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.