
Abstract
Objective
We aimed to develop a nomogram to predict cancer-specific survival (CSS) in patients with hypopharyngeal squamous cell carcinoma (HSCC) treated with primary surgery to provide more accurate risk stratification for patients.
Methods
We retrospectively collected data of 1144 eligible patients with HSCC from the Surveillance, Epidemiology, and End Results (SEER) database between 2004 and 2015. Patients were randomly divided into training and validation groups (ratio 6:4) and we used univariate and multivariate Cox analysis. We developed and validated a nomogram using calibration plots and time-dependent receiver operating characteristic, Kaplan–Meier, and decision curves.
Results
Age; marital status; T, N, and M stage; and postoperative adjuvant therapy were independent factors associated with CSS, which were included in the nomogram. The nomogram’s C-index was 0.705 to 0.723 in the training group and 0.681 to 0.736 in the validation group, which were significantly higher than conventional American Joint Committee on Cancer (AJCC) staging. Calibration curves showed good agreement between prediction and observation in both groups. Kaplan–Meier and decision curves suggested the nomogram had better risk stratification and net benefit than conventional AJCC staging.
Conclusions
We established a nomogram that was superior to conventional AJCC staging in predicting CSS for HSCC.
Keywords
Introduction
Hypopharyngeal squamous cell carcinoma (HSCC) is a rare type of cancer accounting for approximately 2% to 5% of head and neck neoplasms; however, the incidence and mortality of HSCC continue to increase yearly.1,2 Because of its special anatomical position, primary HSCC is usually asymptomatic in the early stage. Approximately 80% of patients have progressed to stage III (22.6%) or IV (57.4%) at the time of diagnosis.3,4 Thus, their prognosis is relatively poor, with 5-year overall survival of 30% to 35% reported in a previous study. 5
Although non-surgical treatments, including definitive chemoradiotherapy (CRT) and chemotherapy followed by radiotherapy (RT), have become more common in treating many types of head and neck cancer, surgery remains the mainstay option for most surgeons, especially for patients who are in advanced stages2,6 In patients with HSCC treated with primary surgery, accurate risk prediction is important not only to select appropriate postoperative adjuvant treatment (POAT) but also to accurately inform patients about their long-term prognosis.
The American Joint Committee on Cancer (AJCC) stage classification is widely used for risk stratification in clinical practice. However, evidence shows that factors including age, ethnicity, blood parameters, marital status, and treatment methods can also affect prognosis.7–10 Thus, the AJCC stage may not be sufficient to conduct accurate risk stratification. Moreover, previous prognostic models were mainly developed using population-based studies and non-surgical treatment, which may limit their application in those treated with surgery owing to different treatment modalities.7,8 Therefore, in our study, we aimed to develop and validate a nomogram that could accurately predict the survival in patients undergoing primary surgery, which can help clinicians perform better risk stratification.
Methods
Patient selection and data collection
The Surveillance, Epidemiology, and End Results (SEER) program (1973–2015) is a cancer registry that contains information on patients with cancer and is supported by the National Cancer Institute and Centers for Disease Control and Prevention. A case listing session was created from the SEER database using the SEER * Stat 8.3.9 (https: //seer.cancer.gov/seerstat). Patients who were diagnosed with HSCC (tumor, node, metastasis [TNM] 7/CS v0204 + Schema = ‘Hypopharynx’) between 2004 and 2015 were retrospectively selected. Primary surgery was defined as patients treated with surgery as a primary modality and with curative intent. Thus, the exclusion criteria were (1) other histologic subtype, except for squamous cell carcinoma; (2) treated with non-surgical methods; (3) no surgery at the primary site or surgery site uncertain; and (4) receiving systematic adjuvant therapy before surgery. The patient selection process is illustrated in Figure 1. Finally, the data of 1144 eligible cases were included in the analysis.

Flow chart of patient inclusion and exclusion criteria in the analytic cohort.
All patient details have been de-identified in the study. The following factors were collected for each patient: age, year of diagnosis, sex, ethnicity, marital status, primary site, grade, tumor size, TNM, and AJCC stage (Sixth Edition of the AJCC Cancer Staging Manual), primary surgical type, number of lymph nodes removed, POAT, cause-specific death classification, and survival months. The endpoint of the present study was defined as cancer-specific survival (CSS). The reporting of this study conforms to Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD) guidelines. 11
Ethics approval
The study was approved by the Nanfang Hospital Medical Science Research Ethics Committee. All procedures were performed in accordance with the Declaration of Helsinki. Informed consent was waived for this study because patient data from the SEER database were de-identified and openly available.
Statistical analysis
Patients were randomly divided into training (70%) and validation groups (30%). The demographic characteristics of the two groups were compared. Continuous variables conforming to a normal distribution were reported as mean ± standard deviation and compared using the Student t-test; otherwise, variables were reported as median (interquartile range, IQR) and compared using the Mann–Whitney U test. Categorical variables were reported as n (%) and compared using the chi-square test.
Univariate and multivariate Cox regression models were used to analyze risk factors associated with CSS in the training group. We developed a nomogram according to the independent risk factors. The accuracy of the predictions was evaluated using discrimination and calibration. The discrimination of the nomogram was measured using the concordance index (C-index) and time-dependent receiver operating characteristic (ROC) curves. 12 A C-index of 0.5 means agreement only by chance and 1 indicates perfect discrimination. The predictive accuracy was compared between the nomogram and conventional AJCC stage. Calibration was measured using a calibration plot with 1000 bootstrap resamples. Good agreement between the nomogram prediction and actual observation indicates good calibration. We tested the discrimination and calibration of the nomogram in both the training and validation groups.
Total points were calculated according to the nomogram and stratified as low-risk, intermediate-risk, and high-risk groups according to tertiles in the training group. Kaplan–Meier curves and the log-rank test were used to illustrate the CSS of patients according to risk stratification and conventional AJCC stage. Decision curve analysis was performed to illustrate the accuracy of the model by calculating the net benefit over a spectrum of probability thresholds. Nomogram development and calibration were conducted with R software version 4.0.3 using the “rms” package (The R Project for Statistical Computing, Vienna, Austria), and other statistical analyses were performed with IBM SPSS version 26 (IBM Corp., Armonk, NY, USA). All P-values were two-sided and P < 0.05 indicated statistical significance.
Results
Patient characteristics
The data of 1144 patients were included in the analysis. The mean age of the entire cohort was 64.81 ± 10.31 years, and 914 (79.9%) patients were men. More than half of patients (n = 661, 57.8%) were diagnosed with stage IV disease. Of these, 468 (40.9%), 167 (14.6%), and 509 (44.5%) patients received local tumor resection, pharyngectomy, and pharyngectomy with laryngectomy, respectively. The median follow-up time of the analytic cohort was 30.5 (IQR: 12–62) months, with 556 (48.6%) cancer-specific deaths. The 3-year, 5-year, and 8-year CSS of the cohort was 58.1%, 49.9%, and 42.4%, respectively. The cohort was then randomly divided into training (n = 688, 60%) and validation groups (n = 456, 40%). As shown in Table 1, the baseline characteristics between the two groups were similar.
Baseline characteristics of patients in the training and validation groups.

POAT, postoperative adjuvant therapy; CT, chemotherapy; RT, radiotherapy; CRT, chemoradiotherapy; AJCC, American Joint Committee on Cancer.
Prognostic analysis and nomogram development
The results of univariable and multivariable Cox regression analysis are shown in Table 2. In univariate analysis, age, marital status, tumor size, surgical type, POAT, T stage, N stage, M stage, and AJCC stage were associated with CSS in the training group. In multivariate analysis, age, marital status, T stage, N stage, M stage, and POAT were independent prognostic factors linked to CSS.
Univariate and multivariate Cox proportional regression for risk factors in predicting cancer-specific survival.

* To avoid collinearity, AJCC stage was not included in the multivariate model.
HR, hazard ratio; CI, confidence interval; POAT, postoperative adjuvant therapy; CT, chemotherapy; RT, radiotherapy; CRT, chemoradiotherapy; AJCC, American Joint Committee on Cancer.
The nomogram was established by incorporating age, marital status, T stage, N stage, M stage, and POAT (Figure 2). Then, the nomogram was validated in both the training and validation groups. As shown in Figure 3, time-dependent ROC curves indicated that the discrimination of the nomogram for 3-year, 5-year, and 8-year C-index was 0.705, 0.706, and 0.723, respectively, in the training group, which was superior to those of AJCC staging (3-year: 0.613, 5-year: 0.597, 8-year: 0.563, P < 0.001). In the validation group, the 3-year, 5-year, and 8-year C-index was 0.736, 0.713, and 0.681, respectively, which was also significantly higher than those of AJCC staging (3-year: 0.624, 5-year: 0.587, 8-year: 0.577, P < 0.001). The calibration plot showed good agreement with the predicted and actual probabilities in both groups (Figure 4).

Nomogram to predict cancer-specific survival with six independent prognostic factors.
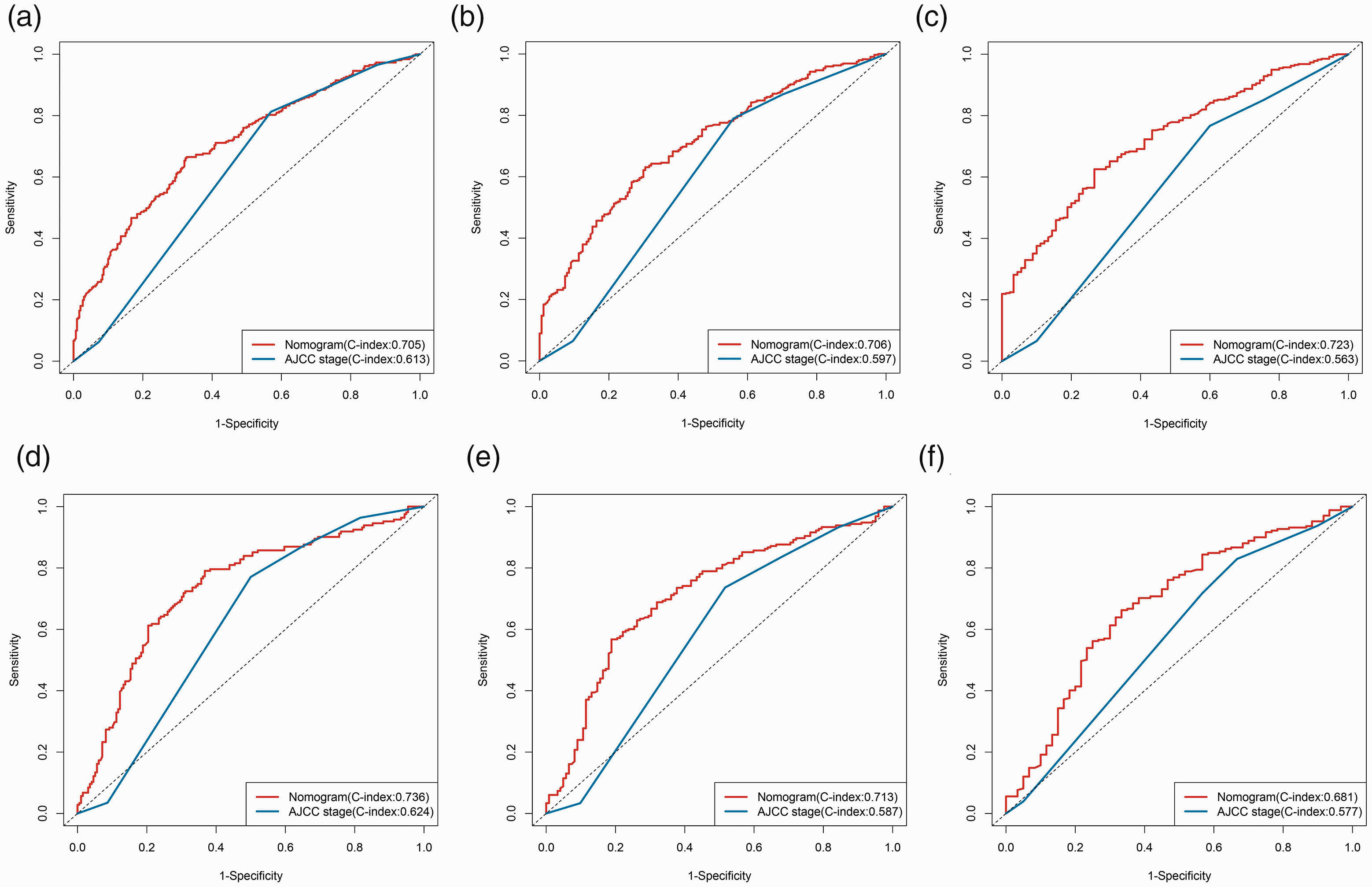
Time-dependent ROC curves and AUCs were used to assess prognostic accuracy of the nomogram compared with conventional AJCC staging at different timepoints.
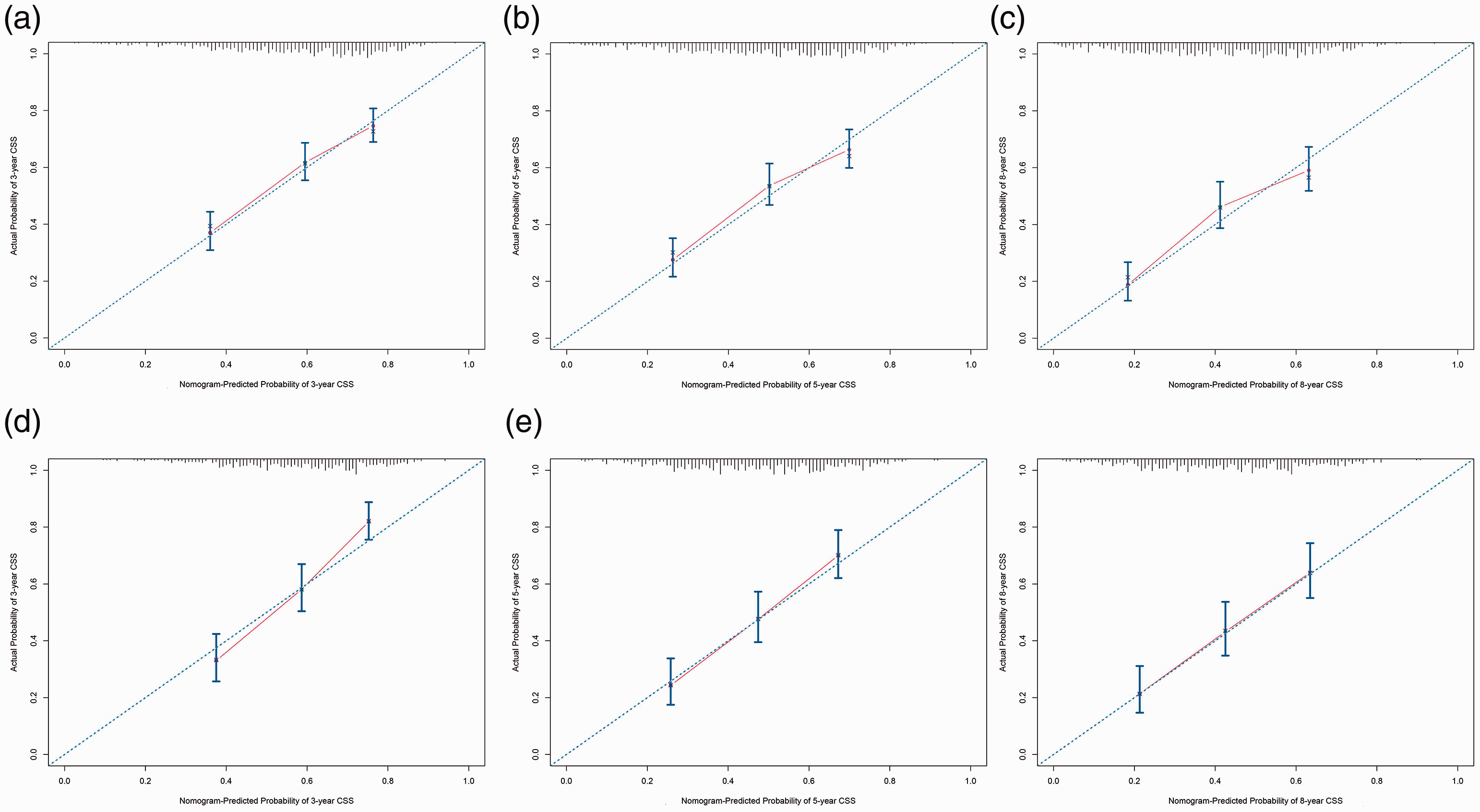
Calibration plot for predicting patient cancer-specific survival at different timepoints.
Prognostic risk stratification
We conducted prognostic risk stratification for CSS according to the total points calculated using the nomogram. Patients were divided into low-risk, intermediate-risk, and high-risk groups according to tertiles in the training cohort. As is shown in Figure 5, the 5-year CSS for high-risk patients was 27.6% and 24.7% in the training and validation groups, respectively; these were significantly lower than those of the intermediate-risk (55.4% and 50.7%, P < 0.001) and low-risk (67% and 70.8%, P < 0.001) groups, respectively. The Kaplan–Meier curves demonstrated that AJCC stage could be used to stratify patients between stage IV and stage I–III; however, use of the AJCC stage was unsatisfactory in stratifying patients among stage I–III. Decision curve analysis showed that the net benefits of the nomogram were greater than those of AJCC staging, suggesting that the established nomogram had better risk stratification than using the conventional AJCC stage (Figure 6).

Kaplan–Meier survival curves in the training group (a: nomogram, b: AJCC stage) and validation group (c: nomogram; d: AJCC stage).

Decision curve analysis indicating net benefit for use of the nomogram and AJCC stage in predicting cancer-specific survival at 36 months, 60 months, and 96 months in the (a) training and (b) validation groups.
Discussion
HSCC is a rare type of cancer, accounting for less than 5% of all neck and head cancers.1,2 Considering the rarity and special anatomy of HSCC, treatment strategies for HSCC have long been a challenge. With the concept of laryngeal preservation, use of non-surgical methods has become a trend in treatment of this disease. 2 However, recent evidence confirms that patients who undergo primary surgery have better survival outcomes than those treated with non-surgical strategies, which indicates that surgery remains the primary option for this disease.13–16 Because of the rich lymphatic network in the neck and the submucosal invasive behavior of tumor cells, the recurrence rates for patients with HSCC who are treated with surgery are relatively high. 5 Thus, POAT including RT, chemotherapy, and immunotherapy could also be useful to eliminate residual cancer cells and reduce disease recurrence. 6 However, POAT can also cause severe damage to normal cells and tissue. Thus, it is essential for clinicians to perform accurate risk stratification for patients with HSCC to guide POAT.
AJCC stage is a widely used risk stratification system in clinical practice. However, recent evidence suggests that the current AJCC stage classification has many limitations in terms of accurately revealing patients’ risk.7–9,17–19 First, AJCC staging does not include factors like age, ethnicity, marital status, and preoperative blood parameters, which have been associated with prognosis in previous studies.7–9 Second, some pathologic characteristics like histologic features, tumor size, number of positive lymph nodes, and positive lymph node ratio are also associated with prognosis but cannot be completely revealed using conventional AJCC staging.17–19 Thus, a more comprehensive model is urgently needed for risk stratification in patients with HSCC.
Regarding prognostic models of HSCC, Arends et al. 20 retrospectively analyzed patients from a single center and developed a nomogram incorporating TNM classification, Adult Comorbidity Evaluation-27 score, body mass index, hemoglobin, and albumin. However, the discrimination of the model was unsatisfactory (C-index: 0.620) and it was therefore not superior to conventional AJCC staging. Tang et al. 8 and Lin et al. 7 established nomograms to predict CSS using the SEER database. Both nomograms included similar factors like age, ethnicity, TNM stage, and treatment strategies. However, these models were mainly developed using data of patients treated with non-surgical methods and thus lack pathological information like tumor size and extension, lymph nodes status, and tumor grade. Therefore, these models cannot accurately reflect the prognosis for patients treated with surgery. Heng et al. 21 retrospectively analyzed 385 patients with HSCC treated with surgery and developed a nomogram based on tumor size, esophageal invasion, extracapsular spread or internal jugular vein adhesion, thyroid gland invasion, and number of lymph node metastases (≤3 or >3). However, that study was conducted at a single center in a Chinese population only. Additionally, the model was not externally validated, which may limit its application. Therefore, we developed and validated a nomogram to predict CSS using the SEER database. Notably, we found that age, marital status, T stage, N stage, M stage, and POAT were independent risk factors that could predict CSS in patients with HSCC. Older age and unmarried status have been reported as adverse prognostic factors.7,8,22 In our study, we incorporated the above five factors into the nomogram, which was found to be superior to conventional AJCC stage. Therefore, the nomogram is not only user friendly (includes only six factors that are easily accessible), it can help clinicians to perform better risk stratification.
Our study has several limitations. First, the SEER database lacked information on patients’ comorbidities, blood parameters, and complications, which could affect the prognosis of patients with HSCC.7–10 Other factors, including the use of tobacco and alcohol, are also closely related to prognosis in head and neck cancers, and data for these factors were lacking in the SEER database.23,24 Second, the predictive accuracy of the nomogram was moderate (C-index: 0.705–0.723 in the training group and 0.681–0.736 in the validation group), which suggests that many potential risk factors have not been included. Recently, studies have shown that gene patterns, PD-L1, and the immune microenvironment can also reflect the prognosis of HSCC.25–27 Thus, a multi-omics model should be developed in the future to improve the predictive accuracy of prognosis in these patients. Third, the present nomogram was developed based on a retrospective population-based analysis, which was not externally validated. Owing to small size of these patient populations, future studies are needed to externally validate the proposed nomogram in a multicenter prospective cohort.
Conclusion
We found that older age, unmarried status, advanced T stage, N stage, M stage, and not receiving POAT were independently associated with shorter CSS in patients with HSCC. We established a nomogram using these six factors, which was superior to AJCC staging. The established nomogram may offer better risk stratification for patients with HSCC who are treated with primary surgery.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605211067414 - Supplemental material for Development and validation of a nomogram to predict cancer-specific survival in patients with hypopharyngeal squamous cell carcinoma treated with primary surgery
Supplemental material, sj-pdf-1-imr-10.1177_03000605211067414 for Development and validation of a nomogram to predict cancer-specific survival in patients with hypopharyngeal squamous cell carcinoma treated with primary surgery by Ke Wang, Xia Xu, Ruotao Xiao, Danyi Du, Luqi Wang, Hanqing Zhang, Zehong Lv, Xiangping Li and Gang Li in Journal of International Medical Research
Footnotes
Author contributions
KW, XX, GL: conceived the study, analyzed the data, and drafted the manuscript. RX, DD: conducted data collection and reference collection, and revised the manuscript. LW, HZ, ZL: analyzed the data, drafted the manuscript. XL: helped to critically revise the manuscript for important intellectual content.
Availability of data and material
Declaration of conflicting interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by Clinical Research Program of Nanfang Hospital, Southern Medical University (grant number: 2018CR043).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.