
Abstract
Aim:
To explore clinical features and prognosis of hepatocellular carcinoma (HCC) in hepatitis B virus surface antigen (HBsAg)-serocleared patients and identify risk factors associated with postoperative recurrence after curative hepatectomy.
Methods:
Patients who had undergone initial hepatectomy for HCC from January 2010 through December 2022. Clinicopathological data were compared between HBsAg-seropositive and HBsAg-serocleared patients. Furthermore, risk factors associated with early and late postoperative HCC recurrence (early and late recurrences (ER and LR), respectively) were analyzed for HBsAg-serocleared HCC patients treated by curative hepatectomy.
Results:
A total of 2184 consecutive patients undergoing initial hepatectomy for HCC were enrolled, including 339 (15.5%) HBsAg-serocleared and 1845 (84.5%) HBsAg-seropositive cases. Tumor characteristics were comparable between the two groups. After curative hepatectomy, the ER rate was lower in the HBsAg-serocleared group than in the HBsAg-seropositive group (16.2% vs 26.3%; p = 0.000). LR rates in the HBsAg-seropositive and HBsAg-serocleared groups were similar (8.3% vs 6.9%, respectively, p = 0.418). Multivariate analysis showed that among HBsAg-serocleared patients, Hong Kong Liver Cancer stage and microvascular invasion were risk factors associated with postoperative ER, while γ-glutamyl transferase level and neutrophil-to-lymphocyte ratio were associated with LR.
Conclusion:
HBsAg-serocleared and HBsAg-seropositive HCC patients exhibited similar tumor characteristics. Curative hepatectomy-treated HBsAg-serocleared HCC patients experienced a lower ER rate and better short-term (⩽3 years) overall survival (OS) rates than their HBsAg-seropositive counterparts. LR, very late recurrence, and long-term (4-, and 5-year) OS rates were similar between the two groups.
Keywords
Introduction
Hepatitis B virus (HBV)-related hepatocellular carcinoma (HCC) continues to jeopardize global health, comprising 75%–85% of primary liver cancers and constituting the sixth most prevalent malignancy and the third leading etiology of cancer mortality.1,2 The attributable morbidity and mortality of HCC are expected to escalate over the next two decades due to global population growth. 3 Chronic HBV infection is the leading etiologic risk factor for HCC in China.4,5
Liver resection is the primary treatment for HCC; however, the notable recurrence rate following liver resection significantly affects patient prognosis. At present, hepatectomy is a common and safe treatment option for patients with early-stage HCC. Unfortunately, the 5-year recurrence rate after resection is as high as 50%–70%. The recurrence of HCC after hepatic resection remains a major obstacle, with recurrence rates as high as 70% at 5 years.6,7 The development of effective systemic therapies has substantially improved the outcomes of patients with advanced-stage HCC, with the aim of increasing overall survival (OS) and disease-free survival (DFS). However, this remarkable progress in systemic therapy has not been paralleled by the improvements in the treatment of resectable HCC, which typically involves the administration of therapies with curative intent, such as resection, liver transplantation, or local ablation.8–10
HBV elimination through vaccination constitutes the central strategy for primary prevention of HCC. 11 The aim of anti-HBV therapy has changed from viral suppression to the seroclearance of HBV surface antigen (HBsAg) (functional cure),12,13 defined as the loss of HBs antigenemia (with or without seroconversion to anti-HBs antibody positivity) and undetectable HBV DNA on two tests taken at least 6 months apart, either spontaneously or following antiviral therapy. 13 HBsAg seroclearance is unusual during the course of chronic HBV infection and is unrelated to receipt of antiviral therapy, therapeutic regimen, study design, geographic location, or regional prevalence.14–16 HBsAg seroclearance mitigates the risk of liver-related adverse clinical outcomes such as HCC, cirrhosis, and liver failure.17–19 However, studies of clinical outcomes following HBsAg loss have yielded inconsistent results, 15 thereby precluding definitive conclusions regarding the potential benefits of HBsAg loss on HCC oncogenesis.
Yoo et al. 20 reported that HBsAg seroclearance lowered the incidence of post-hepatectomy late recurrence (LR) of HBV-related HCC. However, whether HBsAg seroclearance improves prognosis remains controversial.21–23 In this study, we aimed to explore whether tumor characteristics differ between HBsAg-serocleared and HBsAg-seropositive HCC patients, to identify risk factors associated with postoperative recurrence after curative hepatectomy in HBsAg-serocleared HCC patients, and to determine whether this special entity cohort experiences better clinical outcomes, including less frequent recurrence and improved post-recurrence survival (PRS) and OS.
Materials and methods
Study design and population
The source population included 2184 consecutive patients undergoing initial hepatectomy indicated for HCC in the First Hospital Affiliated with Hunan Normal University, Hunan Provincial People’s Hospital from January 2010 through December 2022. HBsAg-serocleared HCC patients were identified from our prospectively constructed HCC database. Clinicopathologic characteristics and clinical outcomes were compared with those of HBsAg-seropositive HCC patients during the same study period. This study is a segment of our series studies on HCC.24,25
Exclusion criteria were: (a) histopathologic diagnosis other than HCC; (b) hepatectomy indicated for recurrent HCC; (c) incomplete clinicopathologic or follow-up data. The criteria for curative hepatectomy of HCC used in our center were complete excision of all tumor nodules and no involvement of any major branch of the hepatic or portal veins, no gross hepatic vein or bile duct tumor thrombi, extrahepatic spread, and/or metastases; and negative surgical margins.24,25
This study was conducted in compliance with the 1964 Helsinki Declaration and its subsequent amendments or comparable ethical standards. The study protocol was authorized by the Institutional Review Board of The First Hospital Affiliated with Hunan Normal University, Hunan Provincial People’s Hospital (approval no. [2024]-131). Patient privacy was safeguarded, and all data were anonymized or stored to maintain confidentiality. The reporting of this study conforms to the STORE statement (see Supplemental File).
Preoperative evaluation
Demographic and clinicopathological data were obtained after hospitalization. The most recent preoperative imaging and laboratory findings were utilized for the preoperative evaluation. HBsAg seroclearance was defined as the loss of HBs antigenemia documented by multiple tests over a duration of at least 6 months and throughout ensuing follow-up until final analysis, irrespective of anti-HBs antibody status and whether the loss of HBs antigenemia occurred spontaneously or followed anti-HBV therapy. 13
Surgical therapies
Details of surgical therapy have been reported previously.24,25 HCCs were excised by open or laparoscopic hepatectomy conducted by senior hepatic surgeons.
Tumor characteristics, staging, and pathological examination
Resected tumors were staged by the Barcelona Clinic Liver Cancer 26 and the Hong Kong Liver Cancer (HKLC) systems. 27 Tumor characteristics (size and number, encapsulation, differentiation, microvascular invasion (MVI), 28 and immunohistochemical markers) and surgical margin status were obtained from pathology reports. Tumor differentiation was assessed using the Edmondson–Steiner classification. 29 Noncancerous hepatic parenchymal specimens obtained far from the tumor were graded for inflammation (G0–G4) and fibrosis (S0–S4) according to the Scheuer scoring system. 30 Fibrosis was scored as either S0–1 (absent or mild), S2 (significant), S3 (severe), or S4 (early cirrhosis). Inflammation was appraised as either G0 (absent), G1 (mild without necrosis), or G2–4 (mild-moderate to severe). Two experienced pathologists who were blinded to clinical data evaluated tissue specimens independently. Discordant results were adjudicated by consensus.
Postoperative recurrence and treatment
Postoperative recurrence of HCC was diagnosed as described previously.24,25 The date, site (intrahepatic and/or extrahepatic), size, and number of lesions were documented. Recurrences at ⩽2 or >2 years post-hepatectomy were labeled as early or late recurrences (ER and LR), respectively. Recurrent HCC was treated with sole or combined therapeutic modalities that included re-resection or metastasectomy, radiation, microwave ablation, transcatheter arterial chemoembolization (TACE), targeted drug + immunotherapy, etc.
Follow-up
All enrollees underwent telephone follow-up or clinical re-examinations. Follow-up investigations comprised liver function tests; quantitative HBsAg, HBV-DNA, and serum alpha fetoprotein levels; and imaging (ultrasonography, enhanced computed tomography (CT), or magnetic resonance imaging (MRI)) conducted at 3-month intervals during the first 2 years and at 6-month intervals thereafter. Follow-up was continued until HCC recurrence or death from any cause. Results were censored on March 31, 2023. DFS was characterized as the timespan between the dates of surgery and the diagnosis of recurrence. PRS was determined as the timespan between tumor recurrence and either death or last follow-up. OS was the interval between surgery and either death or last follow-up. Information regarding deaths was acquired from the families of the decedents.
Statistical analyses
Continuous variables were displayed as median and range and compared by using the Mann–Whitney test. Categorical variables were recorded as frequencies and percentages and compared by either the Wilcoxon rank sum test, Chi-square test, or Fisher exact test as appropriate. Kaplan–Meier and Nelson–Aalen cumulative risk curves were used to compare DFS, PRS, and OS between HBsAg-seropositive and HBsAg-serocleared group (log-rank test). The primary endpoints—centrally assessed DFS, post-operative recurrence time, PRS, and OS—were used to compare the prognosis between the two groups based on Landmark analysis at 12, 24, 36, 48, and 60 months after curative liver resection. Time-dependent covariate Cox proportional-hazard regression analysis was utilized to distinguish factors linked to ER and LR in HBsAg-serocleared patients post-curative hepatectomy. Significant (p < 0.05) predictors identified by univariate analysis underwent multivariate analysis utilizing the backward stepwise method (threshold p < 0.05). Respective 95% confidence intervals (CIs) and hazard ratios were determined. All statistical analyses (which yielded two-tailed values) were conducted using SPSS software (version 23.0; IBM Corporation, Armonk, NY, USA). A value of p < 0.05 indicated significance.
Results
Demographic and clinicopathologic features
Patient characteristics are presented in Table 1. Of the 2184 participants, 339 (15.5%) were HBsAg serocleared, while 1845 (84.5%) were HBsAg-seropositive. Male predominance was similar between both groups (HBsAg-seropositive group: 87.1%; HBsAg-serocleared group: 84.1%). HBsAg-serocleared participants were older than HBsAg-seropositive patients (median ages 62.0 and 53.0 years, respectively). After setting the age cutoff point at 65 years, the prevalence of ⩾65 year-old individuals in the HBsAg-serocleared group (38.6%) still exceeds that of the HBsAg-positive patients (17.0%) (Table 1). In the HBsAg-serocleared group, among patients aged ⩾65 years, 87.0% (114/131) were men and 13.0% (17/131) were women; in patients aged <65 years, 82.2% (171/208) were men and 17.8% (37/208) were women.
Clinicopathological characteristics of the entire cohort (n = 2184).

Pearson χ2.
Wilcoxon rank sum.
Fisher’s exact.
Mann–Whitney U test.
AFP, alpha fetoprotein; BCLC, Barcelona Clinic Liver Cancer; BDTT, bile duct tumor thrombosis; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HCV, hepatitis C virus; HKLC, Hong Kong Liver Cancer; HVTT, hepatic vein tumor thrombosis; IVCTT, inferior vena cava tumor thrombosis; LT, liver transplantation; MD, maximum diameter; MVI, microvascular invasion; PVTT, portal vein tumor thrombosis; SR, spontaneous rupture.
A total of 75.7% (1396/1845) HBsAg-seropositive and 92.3% (313/339) HBsAg-serocleared patients had documented histories of past HBV infection. About 24.3% (449/1845) patients in the HBsAg-seropositive group and 7.7% (26/339) in the HBsAg-serocleared group received first diagnosis of HBV infection on this admission. About 14.1% (260/1845) cases in the HBsAg-seropositive group received prior antiviral therapy, in contrast to only 4.7% (16/339) in the HBsAg-serocleared group, indicating that 95.3% had not received antiviral treatment and that the rate of spontaneous clearance was high. Entecavir was the most frequently used antiviral agent in both groups. Other drugs were used sporadically, including adefovir, lamivudine, tenofovir disoproxil fumarate, and interferon. Antiviral regimens and treatment durations of the two groups were similar. Highly variable antiviral treatment regimens, durations, and treatment endpoints were observed in both groups, reflecting arbitrary practices and insufficient emphasis on standardized HBV treatment protocols in real-life Chinese clinical practice. Antiviral treatment time cutoffs were similar between the two groups, suggesting that either patients were unaware of the hazards of HBV and treatment noncompliance, or that individual physicians had widely varying understandings of the management of HBV infection.
About 93.5% of HBsAg-serocleared patients exhibited undetectable HBV-DNA levels (HBV-DNA <100 IU/mL, lower limit of detection in our center) and 6.5% featured detectable levels (HBV-DNA ⩾ 100 IU/mL). In contrast, in HBsAg-seropositive group, 601 (32.6%) patients exhibited undetectable HBV-DNA levels and only 43.3% (260/601) of them had received prior antiviral treatment.
A higher HBsAb (+) rate was observed in the HBsAg-serocleared than in the HBsAg-seropositive group (49.3% vs 4.2%, respectively). The HBsAg-seropositive group displayed a higher HBeAb (+) and HBcAb (+) (78.3%, 94.4%, respectively) than the HBsAg-serocleared group (60.5%, 89.7%, respectively). One HBeAg (+) case was identified in the HBsAg-serocleared group. HCV coinfection was more prevalent in the HBsAg-serocleared group than in the HBsAg-seropositive group (10.6% vs 3.3%, respectively).
Tumor characteristics were comparable between two groups, with the only difference being tumor Edmondson–Steiner grade (p = 0.000). Background liver parenchyma inflammation grades G1 and G2, and liver fibrosis stages S1 and S2 were significantly more prevalent in the HBsAg-serocleared group. Most surgery-related factors were comparable between the two groups, except for hepatectomy approach due to more laparoscopic hepatectomy adopted in recent years.
Notably, 0.6% (2/339) in the HBsAg-serocleared group experienced HBsAg reactivation during postoperative follow-up (Table 2), and 0.3% (5/1845) HBsAg-seropositive patients exhibited HBsAg seroclearance during postoperative follow-up (Table 3). In this study, we observed a significantly lower rate of postoperative HBsAg seroclearance than that reported in a previous study (6.8%, 172/2520). 20
HBsAg seroconversion in HBsAg-serocleared patients.

DFS, disease-free survival; ER, early recurrence; HBsAg, hepatitis B surface antigen; HBV, hepatitis B; HKLC, Hong Kong Liver Cancer; LR, late recurrence; LT, liver transplantation; MVI, microvascular invasion; TACE, transcatheter arterial chemoembolization.
HBsAg seroclearance in HBsAg-seropositive patients.

DFS, disease-free survival; ER, early recurrence; HBsAg, hepatitis B surface antigen; HBV, hepatitis B; HKLC, Hong Kong Liver Cancer; LR, late recurrence; LT, liver transplantation; MVI, microvascular invasion; TACE, transcatheter arterial chemoembolization.
Prognoses of HCC in curative hepatectomy-treated HBsAg-seropositive and HBsAg-serocleared patients
According to our curative hepatectomy criteria,24,25 we excluded patients with: (a) liver transplantation (HBsAg-seropositive: n = 4, HBsAg-serocleared: n = 1); (b) portal vein tumoral thrombosis and/or bile duct tumoral thrombosis and/or hepatic vein tumoral thrombosis and/or inferior vena cava tumoral thrombosis (HBsAg-seropositive: n = 222, HBsAg-serocleared: n = 38); (c) positive resection margin (HBsAg-seropositive: n = 21, HBsAg-serocleared: n = 5); (d) postoperative 90-day mortality (HBsAg-seropositive: n = 16, HBsAg-serocleared: n = 4). Ultimately, 1582 HBsAg-seropositive cases and 291 HBsAg-serocleared cases were included in further analysis of clinical outcomes following curative hepatectomy.
At the conclusion of the follow-up, HCC recurred in 67 (23.0%) HBsAg-serocleared patients and 547 (34.6%) HBsAg-seropositive patients (p = 0.000, Figure 1(a), Table 4). ER rate in the HBsAg-serocleared group was 16.2% lower than that of the HBsAg-seropositive participants (26.3%; p = 0.000, Table 4). The two groups exhibited comparable LR rates of 8.3% in the HBsAg-seropositive group versus 6.9% in the HBsAg-serocleared group (p = 0.418, Table 4) (Figure 1(b)–(f)). Recurrence rates after 5 postoperative years (very LR) were similar; 1.4% (22/1582) in HBsAg-seropositive group versus 1.7% (5/291) in the HBsAg-serocleared group (p = 0.667, Table 4).

Nelson–Aalen cumulative hazard estimates of postoperative recurrence. (a) Summary of the risk of recurrence. (b) Landmark at 12 months of postoperative recurrence. (c) Landmark at 24 months of postoperative recurrence. (d) Landmark at 36 months of postoperative recurrence. (e) Landmark at 48 months of postoperative recurrence. (f) Landmark at 60 months of postoperative recurrence.
Postoperative prognosis after curative hepatectomy between HBsAg-seropositive and HBsAg-serocleared groups.

Pearson χ2.
Median (min–max).
Log-rank test.
Fisher’s exact.
Wilcoxon rank sum.
DFS, disease-free survival; ER, early recurrence; HBsAg, hepatitis B surface antigen; LR, late recurrence; OS, overall survival; PRS, post-recurrence survival; TACE, transcatheter arterial chemoembolization.
Median DFS was similar (12.3 months in the HBsAg-seropositive group vs 12.8 months in the HBsAg-serocleared group) (log-rank test, χ2 = 0.999, p = 0.318, Table 4, Figure 2(a)). Cumulative DFS rates at 1, 2, 3, 4, and 5 years were 48.6%, 30.9%, 37.1%, 19.4%, 11.5%, and 6.9% in HBsAg-seropositive participants and 45.4%, 28.5%, 16.5%, 11.7%, and 6.5% in the HBsAg-serocleared group, respectively (p = 0.308, 0.416, 0.244, 0.930, 0.823) (Figure 2(b)–(f)). The median PRS was 17.4 months in the HBsAg-seropositive group and 13.0 months in HBsAg seroclearance group (log-rank test, χ2 = 1.995, p = 0.158, Table 4, Figure 3(a)). The landmark analysis of PRS at different time intervals is shown in Figure 3(b)–(f). There were no intergroup differences in recurrence site or post-recurrence treatment modalities (Table 4).
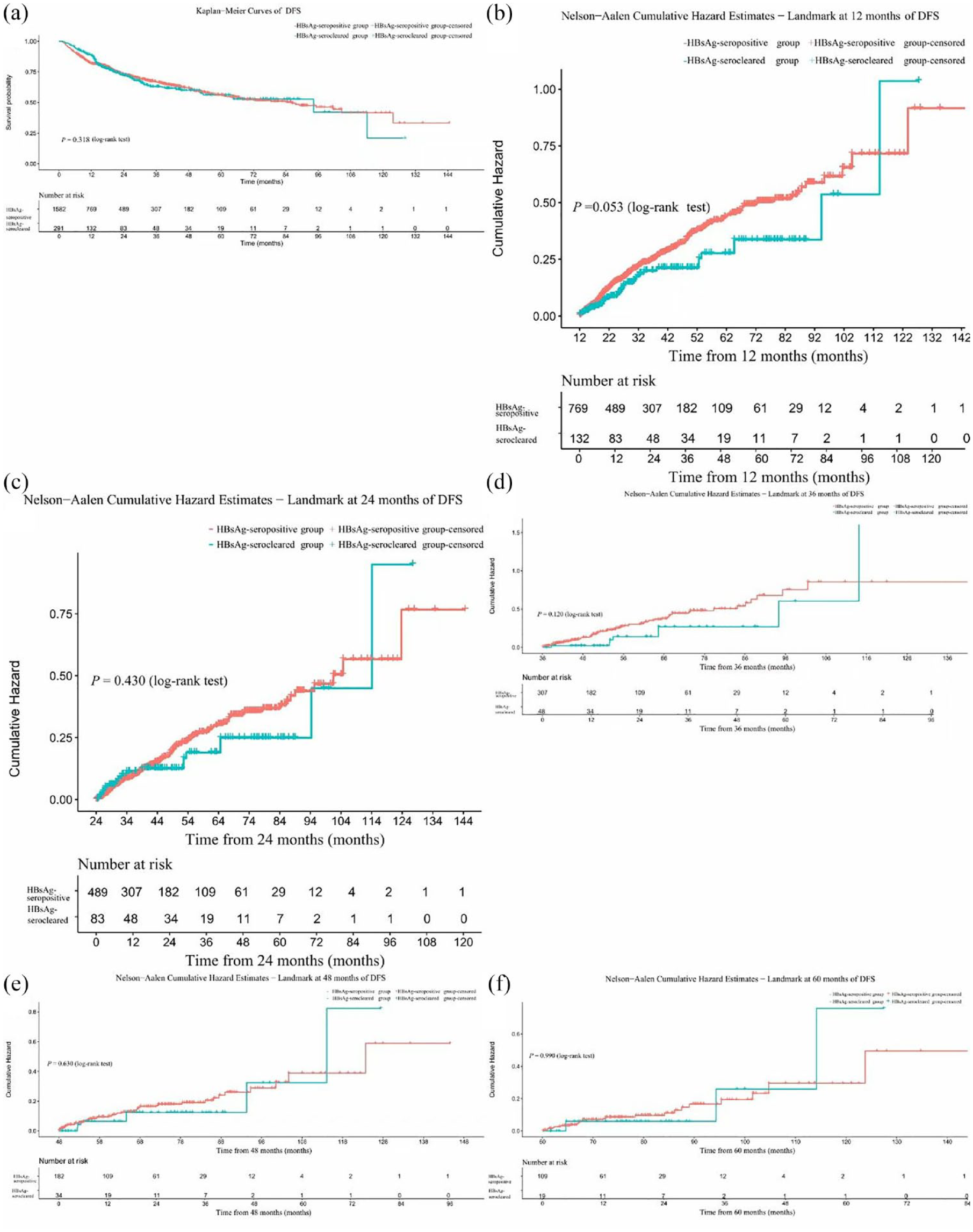
Kaplan–Meier analysis of DFS in HBsAg-seropositive and HBsAg-serocleared groups after curative hepatectomy. (a) Summary of DFS. (b) Landmark at 12 months of DFS. (c) Landmark at 24 months of DFS. (d) Landmark at 36 months of DFS. (e) Landmark at 48 months of DFS. (f) Landmark at 60 months of DFS.

Kaplan–Meier analysis of PRS in HBsAg-seropositive and HBsAg-serocleared groups after curative hepatectomy. (a) Summary of PRS. (b) Landmark at 12 months of PRS. (c) Landmark at 24 months of PRS. (d) Landmark at 36 months of PRS. (e) Landmark at 48 months of PRS. (f) Landmark at 60 months of PRS.
The median OS was 28.7 months in the HBsAg-seropositive group and 26.0 months in the HBsAg-serocleared group (log-rank test, χ2 = 0.031, p = 0.860, Table 4, Figure 4(a)). Cumulative OS rates at 1, 2, and 3 years were 61.9%, 43.4%, and 27.9% in HBsAg-serocleared group and 53.3%, 36.1%, and 21.6% in the HBsAg-seropositive group, respectively (p = 0.007, 0.019, 0.020, Table 4). The landmark analysis of OS at different time intervals is shown in Figure 4(b)–(d). Cumulative OS rates at 4 and 5 years were 16.6% and 10.6% in HBsAg-seropositive patients and 14.8% and 9.3% in the HBsAg-serocleared group, respectively (p = 0.433, 0.511, Table 4, Figure 4(e) and (f)).

Kaplan–Meier analysis of OS in HBsAg-seropositive and HBsAg-serocleared groups after curative hepatectomy. (a) Summary of OS. (b) Landmark at 12 months of OS. (c) Landmark at 24 months of OS. (d) Landmark at 36 months of OS. (e) Landmark at 48 months of OS. (f) Landmark at 60 months of OS.
Risk factors for recurrence in curative hepatectomy-treated HBsAg-serocleared HCC patients
ER and LR were associated with five and four factors, respectively, by univariate analysis (Table 5). Multivariate analysis showed the association of HKLC stage and MVI with ER (Table 6), and the association of γ-glutamyl transpeptidase and neutrophil to lymphocyte ratio (NLR) with LR (Table 7).
Univariate analysis of postoperative recurrence in HBsAg-serocleared patients.

AFP, alpha fetoprotein; ALBI, albumin–bilirubin; ALT, glutamic pyruvic transaminase; AST, aspartate aminotransferase; BCLC, Barcelona Clinic Liver Cancer; CI, confidence interval; ER, early recurrence; γ-GGT, γ-glutamyl transpeptidase; Hb, hemoglobin; HBsAg, hepatitis B surface antigen; HBV, hepatitis B virus; HKLC, Hong Kong Liver Cancer; HR, hazard ratio; LR, late recurrence; MD, maximum diameter; MVI, microvascular invasion; NLR, neutrophil/lymphocyte ratio; 5′-NT, 5′-nucleotidase; PLR, platelet/lymphocyte ratio; PLT, platelet; RBC, red blood cell; TACE, transcatheter arterial chemoembolization; WBC, white blood cell.
Multivariate analysis of ER after curative hepatectomy in HBsAg-serocleared HCC patients.

Beta: standardized coefficient.
CI, confidence interval; ER, early recurrence; HBsAg, hepatitis B surface antigen; HCC, hepatocellular carcinoma; HKLC, Hong Kong Liver Cancer; HR, hazard ratio; MVI, microvascular invasion; SE, standard error.
Multivariate analysis of LR after curative hepatectomy in HBsAg-serocleared HCC patients.

Beta: standardized coefficient.
CI, confidence interval; γ-GGT, γ-glutamyl transpeptidase; HBsAg, hepatitis B surface antigen; HCC, hepatocellular carcinoma; HR, hazard ratio; LR, late recurrence; NLR, neutrophil/lymphocyte ratio; SE, standard error.
Discussion
Up to now, few studies have addressed HCC characteristics in HBsAg-serocleared patients and the potential clinical benefits of HBsAg loss on prognosis after curative hepatectomy. Our current study evaluated complex HCC characteristics and was representative of real-life situations compared to previous study focused on early-stage (BCLC stage 0 or A) HCC. 20 Our study revealed the relationships of HBsAg seroclearance with ER and LR. Our novel findings differed from those of Yoo’s report, which associated HBsAg seroclearance with a lower incidence of LR after curative hepatectomy. 20 Our previous reports verified that HBsAg seroclearance and variables related to HBV infection (HBsAg quantity, HBV-related markers, HBV-DNA level, prior antiviral therapy, treatment duration, postoperative antiviral treatment) were unrelated to postoperative ER or LR among HCC patients treated by curative hepatectomy.24,25 The current study associated similar risk factors with postoperative ER or LR, consistent with our previous report.24,25 In this study, 50.7% of HBsAg-serocleared patients did not experience HBsAb seroconversion, suggesting that anti-HBs seropositivity may be unnecessary for HBsAg seroclearance. Moreover, high rates of HBcAb positivity were observed in both the HBsAg-seropositive and HBsAg-serocleared groups. HBcAb seropositivity is a key biomarker of humoral immune response and indicates an elevated probability of liver-related complications. 31 Consequently, it is understandable that HBsAg seroclearance may not inevitably improve the clinical course of HCC.
This study disclosed a lower ER rate among HBsAg-serocleared patients, which may be attributed to better background liver fibrosis stage and older age, consistent with our previous association of the severity of fibrosis and younger age with an increased risk of postoperative ER. 24 Lower ER rates can reasonably explain better 1, 2, and 3-year OS in the HBsAg-serocleared group. Comparable LR rates may explain similar 4-, 5-year OS, as our previous study confirmed that postoperative ER influenced 3-year OS and that LR affected 5-year OS. 25 In this study, the two groups exhibited comparable LR and very LR rates; postoperative recurrence sites; post-recurrence treatment modalities; and median DFS, PRS, and 4- and 5-year OS. These findings suggest that HBsAg seroclearance may not confer clinical benefits that might be anticipated on theoretical grounds and should not be considered as a precondition of better clinical outcomes. Comparable tumor characteristics between the HBsAg-serocleared and HBsAg-seropositive groups suggest similar tumor behavior and clinical outcomes in both groups.
The median DFS and OS of patients enrolled in this study were not satisfied, perhaps because this population is quite heterogeneous and includes patients with more advanced cancer than BCLC 0–A. As shown in Table 5, BCLC B and BCLC C were 16.2% (47/291) and 7.9% (23/291), respectively, which were excluded from receiving curative intent surgery based on BCLC guidelines (including the latest 2022 updated edition 32 ). BCLC staging system and its later updated editions are still restrictive against surgery, limiting the indication of surgery to early stage only.32,33 However, surgical resection is still performed by surgeons worldwide, particularly in Asian countries where the incidence of HCC is the highest. In real-world practice, the use of LR for HCCs beyond the BCLC guideline recommendations for LR has been noted worldwide, including Western centers.34–37 We propose that it is important to sub-classify BCLC B and C stages since these categories are very broad and sub-classifications can help in selecting patients for surgical resections.
In our study population, HBV is still the main cause of HCC and the difference may contribute to the differences in DFS and OS. HCC surveillance is advised for HBsAg-serocleared patients, especially for men with antecedent cirrhosis, and for those who experience HBsAg seroclearance after 50 years of age. 38 However, our study revealed that HCC incidence in the HBsAg-serocleared group was distributed across all age levels (minimum age of 24 years in the HBsAg-serocleared group) and was not restricted to men. Thus, ongoing HCC surveillance and clinical management should continue even after HBsAg seroclearance in patients. Because most asymptomatic HBV carriers do not seek medical attention, especially after HBsAg seroclearance, we strongly suggest that HBsAg-serocleared patients should still be monitored by using the surveillance strategy adopted for HBsAg-seropositive patients.
Clinical benefits of HBsAg seroclearance have been studied extensively and may include reversal of HBs antigenemia-driven exhaustion of HBV-specific cell-mediated and humoral responses. 39 Serum HBsAg level may function as a biomarker for covalently closed circular DNA (cccDNA) transcription. 13 HBsAg seroclearance may indicate elimination or silencing of the HBV genome including cccDNA and integrated HBV DNA. However, because host-integrated HBV genome and cccDNA may be detected in both HCC and non-tumorous tissues in most functionally cured patients,40,41 the sequelae of HBV genomic integration could be similar between HBsAg-seropositive and HBsAg-serocleared HCC patients. 42 From this aspect, HCCs presenting after HBsAg seroclearance would be expected to exhibit similar tumor characteristics and behaviors as those of HBsAg-seropositive patients, as demonstrated in this study.
It remains unclear whether restoring HBV-specific immune responses will improve clinical outcomes for HCC after HBsAg seroclearance. An abnormal NLR could be regarded as a crude indicator of immunopathy. High NLRs suggest relatively increased neutrophil and/or depleted lymphocyte counts in circulating blood and tumor-associated leukocytes and are associated with low cancer-specific survival due to compromised anti-tumor immune responses.43,44 Circulating lymphocyte subsets of patients with HBV-related HCC disclose immune exhaustion, with fewer T cells and upregulated expression of inhibitory receptors, as well as altered Bcell populations. 45 HBV-DNA integration also occurs in peripheral lymphoid cells. 46 T subset phenotypes of functionally cured individuals differ from those of HBsAg-seropositive patients. For example, circulating PD-1+CD4+ T cells and PD-1+CD4+ Tregs were significantly lower than those of HBsAg-seropositive patients. 47 Tumor-infiltrating immune cell populations may be altered by the immunosuppressive HCC microenvironment and may be related to progression. 48
HBsAg recurrence, defined by HBs antigenemia and/or HBV DNA positivity, 16 has been considered infrequent after HBsAg seroclearance, because HBsAg seroclearance is generally deemed to be of long duration, regardless of HBsAb status.13,16 In this study, only two HBsAg-serocleared patients developed HBs antigenemia during postoperative follow-up, suggesting that HBsAg recurrence, as a rare postoperative event, maybe not necessarily increase the risk of HCC recurrence or portend a poor prognosis. Although patients adhered to strict postoperative surveillance, a temporal relationship between recurrent HBs antigenemia or tumor recurrence could not be determined.
Among HBsAg-serocleared patients, 6.5% exhibited detectable serum HBV-DNA, a status known as occult hepatitis B infection (OBI). 49 Currently available HBV DNA assay in our center has a lower limit of quantitation of <100 IU/mL, and the quantitative HBsAg assay has a lower limit of detection of 0.05 IU/mL. Restricted by objective conditions, differentiating HBV functional or complete cure from OBI would be difficult and beyond current clinical capabilities. Consequently, the inability to differentiate functional cure from OBI did not weaken the reliability of our conclusions, although we must admit it as a minor flaw of our study.
The strengths of this study include large sample size, judicious definitions of study variables, and an extended follow-up duration. Our study evaluated this specific cohort extensively and identified factors associated with prognosis, thereby filling an important knowledge gap.
Some limitations of this work must be addressed. First, retrospective study design may have introduced unavoidable biases and confounding factors. Second, our study population was Chinese patients. The results should be validated in other heterogeneous populations. Third, serum HBcrAg and quantitative intrahepatic cccDNA and HBV DNA assays were not routinely conducted. We must acknowledge that the accumulation of such data will add knowledge regarding this topic. Fourth, our study has limited power to detect a difference in LR between groups and this may be why the difference was not statistically significant. Fifth, the decisions about postoperative systematic therapy and/or postrecurrence management strategies adopted were based primarily on existing guidelines and may have been affected by patients’ preference for less-invasive treatment and a lesser financial burden, which may have introduced bias. In addition, we considered only primary postoperative recurrence treatment modalities although some patients received sequential treatments. The use of multiple and or sequential treatment modalities may provide additional benefits and deserve further studies.
Conclusion
HCCs in HBsAg-serocleared and HBsAg-seropositive patients shared similar tumor characteristics. HBsAg-serocleared HCC patients treated by curative hepatectomy had better ER and short-term (⩽3-year) cumulative OS rates compared with HBsAg-seropositive counterparts, while the two groups had similar LR, very LR, and long-term (4- and 5-year) cumulative OS rates.
Supplemental Material
sj-docx-1-tam-10.1177_17588359241289202 – Supplemental material for Hepatocellular carcinoma in HBsAg seroclearance: clinical features, recurrence, and prognosis following curative hepatectomy
Supplemental material, sj-docx-1-tam-10.1177_17588359241289202 for Hepatocellular carcinoma in HBsAg seroclearance: clinical features, recurrence, and prognosis following curative hepatectomy by Wei Xu, Huai Gong, Bolun Li and Xinmin Yin in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.