
Abstract
Objective:
This study aimed to determine the prevalence and identify associated factors of hepatitis B virus infection among pregnant women attending antenatal care (ANC) follow-up.
Methods:
An institution-based cross-sectional study was conducted from March 04 to April 03, 2020. A total of 381 women were selected using systematic random sampling after every two consecutive women. Structured and interviewer administered questionnaire was used to collect the data. A 2 ml of venous blood sample was drawn from each participant. The plasma was separated from the collected blood samples and was analyzed using a rapid hepatitis B surface antigen (HBsAg) kit to determine hepatitis sero status. Data were entered into the EPI-Data version 3.1, then exported to the statistical package for social sciences version 25 software and analyzed. Multivariable logistic regression was performed to identify independent predictors of HBsAg B seroprevalence at a p-value <0.05.
Results:
The prevalence of HBsAg sero-positivity among pregnant women was 6.6%, 95% CI (4.2, 8.9). History of hosptal admission (adjusted odds ratio (AOR) = 4.11; 95% CI = 1.33–12.71), surgical history (AOR = 6.8; 95% CI = 1.93–23.93), history dental procedures (AOR = 4.93; 95% CI = 1.31–18.53), and body tatoo practices (AOR = 6.822; 95% CI = 1.89–24.69) were found to be associated with HBsAg sero-positivity.
Conclusion:
This study found that HBsAg sero positivity among pregnant women in the study area was in intermediate edemicity. Factors such as history of hospital admission, history of surgery, history of dental procedures, and body tattoo practices were found to be associated with HBsAg sero-positivity. The government of Ethiopia should strengthen screening of all pregnant women for HBV as a part of routine ANC in ANC clinics and treating if they are positive to prevent mother to child transmission.
Introduction
Hepatitis is an inflammation of the liver that can be self-limiting or may progress to fibrosis (scarring), cirrhosis or liver cancer. Hepatitis is mostly caused by hepatitis viruses. There are five main hepatitis viruses, namely A, B, C, D, and E. Types B and C lead to chronic diseases such as liver cirrhosis and cancer in hundreds of millions of people. 1 HBV is primarily found in the liver but is also present in the blood and certain body fluids.2,3 Serologic markers for hepatitis B virus (HBV) are used to diagnose hepatitis B viral infection; the screening should include testing for HBV sero-markers in the blood namely hepatitis B surface antigen (HBsAg), antibody to HBsAg (anti-HBs), and antibody to hepatitis B core antigen (anti-HBc).4–6
HBV is a major cause of acute and chronic hepatitis, cirrhosis or liver cancer. According to the WHO 2017 report an estimation of 257 million peoples (3.5% of the population) were living with chronic HBV infection worldwide in 2015. Among these the African and Western Pacific regions accounted for 68% of the infection. In 2015, viral hepatitis was responsible for 1.34 million deaths (0.884 million deaths due to HBV alone). 7 Hepatitis B is caused to account for 87,890 deaths annually in sub-Saharan Africa. 8 However, the risk of developing chronic HBV infection after acute exposure is dependent on age of the patient; it ranges from 90% in newborns of hepatitis B e core antigen (HBeAg) positive mothers to 25%–50% in infants and children aged <5 years to less than 10% in adults.4,5
Immunologic changes during pregnancy may induce a state of increased susceptibility to certain intracellular pathogens, including viruses, intracellular bacteria and parasites. More than 90% of HBV-infected infants through vertical transmission become chronically infected with HBV, and approximately 25% of them will die prematurely because of liver cirrhosis or hepatocellular carcinoma. 5 Approximately 65 million females of childbearing age worldwide are infected with HBV. 7 A systematic review and meta- analysis conducted in Europe revealed that the prevalence of chronic HBV infection varies widely between European countries generally ranging from 0.1% to 4.4% among pregnant women and from 0.1% to 5.6% in the general population. 9
The prevalence of HBV highest in sub-Saharan Africa and East Asia (5%–10% of the adult population) is chronically infected in this area. 10 According to different studies, HBV infection among pregnant women in Central and East African countries was 3.2% in Eritrea,9.3% in Kenya, 3.1% in Kigali, and 7.5% in Sudan.11–14 Prevalence of hepatitis B is high in Africa, which may be due to low timely birth dose vaccine coverage. The first birth dose vaccine coverage was estimated to be only 3% in low-income countries.15,16 A meta-analysis conducted in Ethiopia reported that the prevalence of HBV infection was 4.7% and 7.4% among pregnant women and the general population, respectively.17,18
Chronic HBV infection among pregnant mothers is associated with gestational diabetes mellitus, ante partum hemorrhage, threatened premature labor and lower Appearance, Pulse, Grimace, Activity and Respiration (APGAR) score. Mothers with serious abnormal liver function complications are also at risk of postpartum hemorrhage, puerperal infection, low body weight infants, fetal distress, premature birth, fetal death, and neonatal asphyxia.19,20
Prevention of neonatal and early childhood infection through birth dose vaccination of the HBV vaccine is crucial to prevent chronic infection and subsequent complications of chronic liver disease. Even though viral hepatitis is an international public health challenge, and it has a significant burden on communities across the world, hepatitis has been largely ignored as a health and development priority until recently. 10 Previous studies on seroprevalence of HBsAg among pregnant women were conducted in different parts of the world including Ethiopia. Studies in Ethiopia indicated that the seroprevalence of HBsAg among pregnant women ranged from 2.3% to 8.3%.21,22 However, studies on the prevalence and associated factors among pregnant women particularly in the study area are limited. Therefore, this study aimed to assess the prevalence and factors associated with HBV infection among pregnant mothers who attended ANC at Hawassa city public hospitals.
Methods
Study area, study design, and study period
A health facility-based cross-sectional study design was employed at Hawassa city public hospitals from March 04 to April 03, 2020. Hawassa is a city in Ethiopia, on the shores of Lake Hawassa in the Great Rift Valley. It is the capital city of the Southern Nations Nationalities and Peoples Region and is located 273 km from Addis Ababa, the capital of Ethiopia, and covers an area of 50 km2. There are 1 comprehensive specialized hospital, 1 general hospital, 1 primary hospital, 6 private hospitals, 7 health centers, 15 health post, and 47 private clinics. The Hawassa University Comprehensive Specialized Hospital (HUCSH) provides antenatal care (ANC) services to over 2880 pregnant women annually. The Adare General Hospital serves more than 5184 pregnant women annually. The Tula Primary Hospital serves more than 1224 pregnant mothers annually. 23 All three hospitals were well equipped and provided a full range of ANC and delivery services including cesarean delivery.
Population
All pregnant mothers who visit the ANC clinic at the Hawassa city public hospitals were the source population, while all randomly selected pregnant mothers who visit the ANC clinic during the study period were the study population.
Inclusion and exclusion criteria
All pregnant women with confirmed pregnancy and attending the ANC clinic for follow up during the study period were included, while pregnant women who were critically ill and needed urgent intervention and mothers who revisited the ANC clinic during study period were excluded.
Sample size determination
The sample size was calculated using Epi-Info version 7.2 STAC CALC with the assumptions of 95% confidence level, 80% power, adjusted odds ratio (AOR) = 2.28, exposed to nonexposed ratio of 1:1, and proportion of outcome among non-exposed (6.2%). 24 Considering a non-response rate of 10%, the final sample size of 381 was reached.
Sampling technique and sampling procedure
In Hawassa city, there are three public hospitals namely the HUCSH, the Adare General Hospital, and the Tula Primary Hospital. All these hospitals were included in the study. Then, proportional allocation to the calculated sample size was made based on the number of client flows in the previous quarter total case flow counted in the ANC registration book of these three hospitals . The average 1 month case load of each hospital was then calculated. After a quarter average of all facilities calculated 1 month case load of the three health facilities became 774. By considering 1 month data collection period the kth value became 774/381 = 2. The first participant was selected by lottery method. Finally, individual study participants were selected by using a systematic sampling technique every two women until the required sample size was achieved .
Data collection tools and procedure
Data were collected using pretested interviewer administered structured questionnaire and chart review. The questionnaire included socio-demographic and socioeconomic variables, hospital-associated factors, and risky sociocultural and behavioral practices. It was prepared after reviewing different literatures which are similar to the current study and modified.17, 18 , 21 , 24 – 30 A HBsAg kit was used to determine the sero-positivity of the women. A brief explanation about the aim of the study was given to participants by the data collector; then they were requested to take part in the study voluntarily and 2 ml of blood was drawn by a laboratory technologist to determine their HBsAg status. After the data collector finished the interview they gave the code and sent the client with a laboratory request form to the blood collector laboratory technologist. Blood samples were collected aseptically by a laboratory technologist according to the standard hospital procedures. Once the participants participated in the study, specific marks were placed on the chart to prevent duplication (reparticipation) in the study.
Test procedure
The HBsAg status of the participants was determined by using an advanced quality one step HBsAg test kit (InTec PRODUCTS, INC.). The advanced quality one step HBsAg test is a rapid immunogromatographic assay for the qualitative detection of HBsAg in the human whole blood serum or plasma. The advanced quality one step HBsAg test kit had two lines namely control and test lines. Blood samples were added on the kit according to the manufacturer’s instructions and the results were interpreted after waiting for 20 min.The appearance of one red or pink line in the control line and the absence of a line in the test region were indicative of negative results for HBsAg. The appearance of a distinct red or pink band in both the test region and control line was indicative of positive result for HBsAg. The appearance of one red or pink line in the test region and absence of this line in the control line or absence of these lines in both the control and test regions interpreted as an invalid result. Positive and negative control samples within the test kits were used to assess the performance of the test kits by obtaining known positive and negative blood samples confirmed by Enzyme-Linked Immunosorbent Assay (ELISA).
Data quality assurance
The questionnaire was initially prepared in English, and then translated into Amharic for fieldwork purpose by a language expert. The translated version was again translated back to English to maintain its consistency in the meaning of words or concepts of the data collection tool. The tool was pretested among 5% 16 of the total sample size subjects at the family guidance association of Ethiopian Hawassa branch. Data collectors and supervisors were trained for 1 day before data collection. The collected data were checked for completeness on the daily bases by the supervisor and principal investigator.
Statistical analysis
After the collected data were checked for completeness, they were entered into Epi-Data version 3.1. Then the data were exported to SPSS version 25.0 for analysis. Bi-variable logistic regression analysis was used to determine the significance of the association between the dependent variables and each independent variable. A p-value of less than 0.25 in bivariate analysis was considered as a candidate for multivariable logistic regression. A multivariable logistic regression model was used to control for possible confounding variables and to identify independent predictors of HBsAg seroprevalence at a p-value of <0.05 with their respective adjusted odd ratios and confidence intervals (95% CI). The fitness of the logistic regression models was assessed using the Hosmer-Lemeshow test and the model was fit with a p-value of 0.42. A multicollinearity test was carried out to determine the correlation between each independent variable, using the Variance Inflation Factor. Finally, the findings were presented in the form of text, graph and tables as appropriate.
Ethical consideration
Ethical approval for this study was obtained from the Institutional Review Board of the Hawassa University College of Medicine and Health Sciences (CMHS/IRB 06-012) and an official letter permission was taken from the Hawassa city health department. Furthermore, after a thorough explanation of the purpose, benefit, and possible risks of the study, written informed consent was secured from each study participant before being enrolled into the study. For study participants aged <18 years, written informed consent was obtained from their parents. The confidentiality and the privacy of the respondents were maintained. All study participants were informed that their participation in this research project had no incentives or direct benefits. Their participation in the study was voluntary.
Results
Socio-demographic and socio economic characteristics
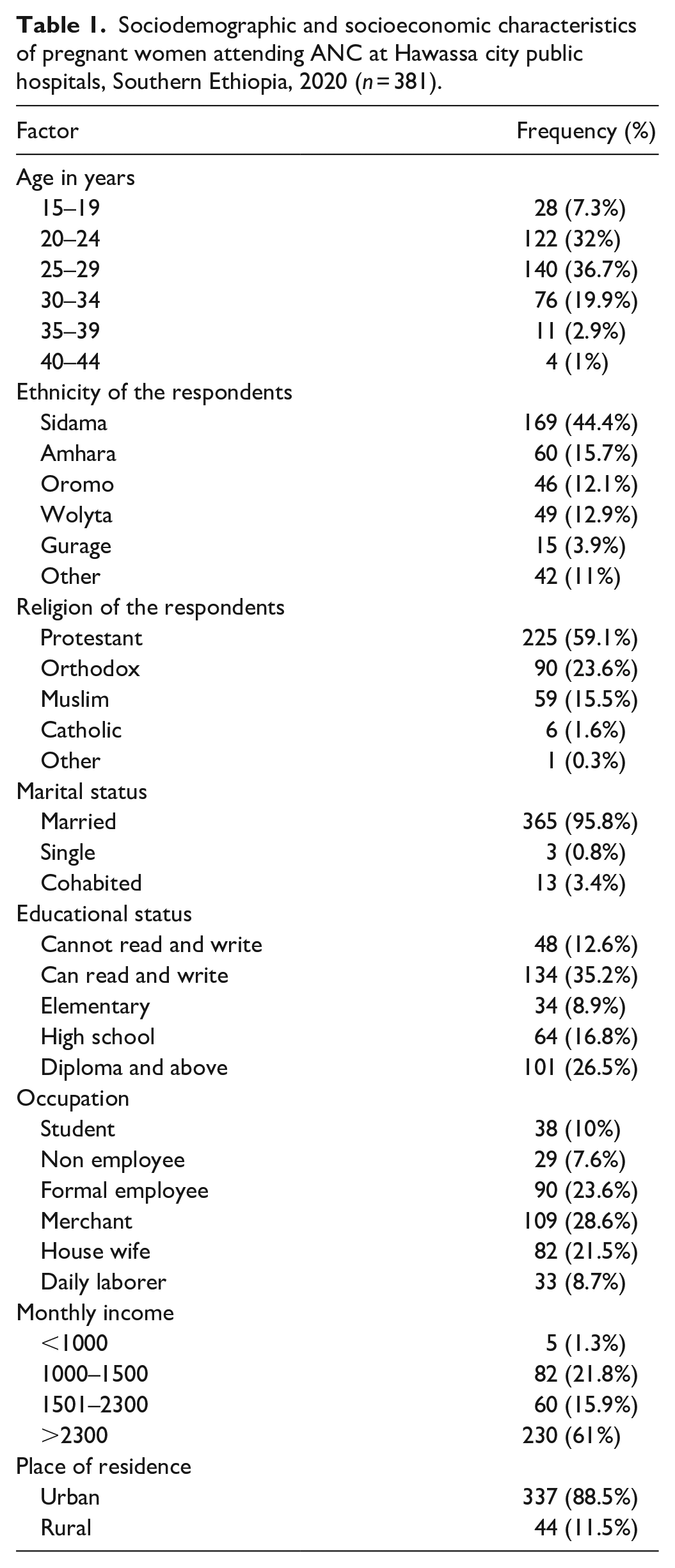
A total of 381 pregnant women participated in the study with a response rate of 100%. The median age of the respondents was 25 years with a minimum of 15 years and a maximum of 40 years. Almost all, 365 (95.8%) were currently married. Majority of respondents, that is, 169 (44.4%) respondents were Sidama followed by 60 (15.7%) Amhara respondents by ethnicity. Regarding educational level, 134 (35.2%) women can read and write and 34 (8.9%) attended until elementary school. The majority of the respondents, that is, 337(88.5%) respondents resided in urban areas and the remaining 44 (11.5%) respondents lived in rural areas (Table 1).
Sociodemographic and socioeconomic characteristics of pregnant women attending ANC at Hawassa city public hospitals, Southern Ethiopia, 2020 (n = 381).
Seroprevalence of HBV among pregnant women
Among 381 pregnant women who participated in the study 25 were positive for HBsAg which makes the overall prevalence of 25 (6.6%), 95% CI (4.2, 8.9).
Gynecological, obstetric, and risky cultural behavior-related factors
Of the respondents, 269 (70.6%) were multigravidas and 112 (29.4%) were primigravidas. Regarding parity, 172 (63.9%) respondents were multipara, and the remaining 2 (0.7%) were grand multipara. One hundred ninety (49.9%) respondents were in their third trimester of pregnancy and 17 (4.5%) were in their first trimester of pregnancy. Forty-eight (7.6%) respondents had a history of hospitalization and 46 (12.1%) had a history of surgery in their life. Regarding blood transfusion, 6 (1.6%) pregnant women had a history of blood transfusion in their life. And 24 (6.3%) pregnant women had a history of dental procedures.
Regarding risky sociocultural and behavioral practices 91 (23.9%) women had experienced abortion (44 induced and 47 spontaneous abortions). Concerning body tattoos, 30 (7.9%) pregnant women had a history of tattooing their bodies. Regarding ear piercing, 358 (94%) pregnant women had a history of ear piercing. And 22 (5.8%) pregnant women had a history of nose piercing. Of the 381 pregnant women, 16 reported that their husbands had other wife/ves and 6 pregnant women had boyfriends other than their husbands (Table 2).
Gynecological, obstetric, and risky cultural behavior-related characteristics of pregnant women attending ANC at Hawassa city public hospitals, 2020.

Predictors of HBsAg sero-positivity
Pregnant women with a history of admission were four times more likely to be reactive (positive) for HBsAg than those who had no history of hospitalization (AOR = 4.11; 95% CI = 1.33–12.71 with p-value = 0.014). Pregnant women with surgical history were 6.8 times more likely to be reactive (positive) for HBsAg than those who had no surgical history (AOR = 6.80; 95% CI = 1.93–23.93 with p-value = 0.003). Pregnant women with a history of dental procedure were 4.9 times more likely to be reactive (positive) for HBsAg than those who had no history of dental procedures (AOR = 4.93; 95% CI = 1.31–18.53 with p-value = 0.018), and those pregnant women who had a history of body tattoo were 6.8 times more likely to be reactive (positive) for HBsAg than those who had not (AOR = 6.822; 95% CI = 1.885–24.686 with p-value = 0.003) (Table 3).
Multiple logistic regression analysis results of factors associated with HBsAG sero-positivity of pregnant women attending ANC in Hawassa city public hospitals, Southern Ethiopia, 2020.

Discussion
In this study an attempt was made to determine the prevalence of HBsAg and its associated factors among pregnant women who were attending ANC follow-up at Hawassa city public hospitals. The study revealed that the prevalence of HBsAg was 6.6%, 95% CI (4.2, 8.9), which was consistent with the studies conducted in Addis Ababa 6%, 31 Yirgalem Hospital 7.2%, 32 Felege Hiwot Referral Hospital Bahir Dar 4.7%, 27 Dessie Referral Hospital 4.9%, 28 Debre Tabor District Hospital 5.8%, 33 Northwest Region of Cameroon 7.7%, 34 Hong Kong Special Administrative Region of China 7.5%, 35 Shenyang, China 3.1%, 36 India 3.8%, 37 Vientiane Mahosot Hospital 5.44%, 38 and Sokoto Metropolis 6.51%. 39 The agreement with studies conducted in Bahir Dar and Dessie and Sokoto Metropolis could be due to the relatively similar number of participants in the present study and method similarity and the agreement with Yirgalem Hospital may be due to relative similarities of socio cultural practices of the participants.
However, it is relatively higher than that in studies conducted in Haiti 2.5%, 40 Gandhi Memorial Hospital 2.3%, 21 Wollega Zone 2.4%, 41 St. Paul’s Hospital Millennium Medical College and Selam Health Center 3%, 42 Dawro Zone 3.5%, 24 and Bahir Dar City 3.8%. 43 The observed discrepancies with studies conducted in Gandhi Memorial Hospital and St. Paul’s Hospital Millennium Medical College and Selam Health Center could be due to the fact that participants in these studies had knowledge about the risk factors and mode of transmission of HBV infection, and the discrepancies with studies in Daworo and Wollega may be due to relatively higher number of participants in the present study.
In contrast it is lower than in studies conducted among rural women in China 9.51%, 44 Yemen 10.8%, 45 Kenya 9.3%, 12 and Gambia 9.2%. 26 However, a slightly lower prevalence was reported in other studies, 3.8% in Tanzania, 25 3.1% in Kigali, 13 and 3.2% in Eritrea. 11 Lower HBsAg prevalence was reported in Japan and Kashan, Isfaha which were 0.5% and 1.56%, respectively.46,47 The discrepancies in HBV prevalence across studies might be attributed to variations in the sociodemographic characteristics of the study population such as sociocultural environment, traditional practices, sexual practices and medical exposure, and differences in hepatitis epidemiology. The other reason may be the early vaccination of people with HBV in developed countries.
Pregnant women with a history of hospital admission had four times risk of developing HBV infection than those without a history of hospital admission. This was consistent with a previous report by the Shashemene General Hospital. 48 The association of hospital admissions with HBV infection might be due to the lack of proper bed hygiene between discharge of HBsAg positive patient and admission of new patients. In addition, pregnant women with a history of surgery had a 6.8 times chance of developing HBV infection than their counterparts. Similar finding was reported in different studies conducted in Tirunesh Beijing Hospital, Addis Ababa, 31 Khartoum Teaching Hospital, Sudan 14 and Cameroon. 34 The reason for association between surgical history and HBV infection might be due to lack of HBsAg screening test before surgery and re-usage of contaminated surgical instruments without proper sterilization of these instruments. Hence, in health-care settings, promotion of hygiene and infection prevention practices is recommended in order to avoid nosocomial infections. As well as we recommend a rigorous screening of blood before transfusion.
Moreover pregnant women with a history of dental procedure had about fivefold greater chances to be infected with HBV than women who had no history of dental procedure. Similar finding was reported in Shashemene General Hospital 48 and Debre Markos blood bank. 49 This might be due to most of the dental practices done out of health facility that lack standard precaution measures to prevent infection before using dental procedure instruments.
In this study pregnant women who had a history of body tattoo had more chance to be infected with HBV than their counterparts. Similar finding was also reported in different previous studies conducted in Bahir Dar City, 44 Tirunesh Beijing Hospital, 32 Debre Markos blood bank, 49 and Cameroon. 34 This might be due to lack of hygienic condition and proper sterilization of instruments used to perform body tattoo.
Limitation of the study
The limitation of this study was that it only focused on women attending government ANC clinics. Beside majority of the women in Hawassa attend ANC clinic in public health facilities, the results might not be generalizable to all pregnant women in Hawassa as more women are now seeking ANC services in the upcoming private health facility facilities. In this study we used the rapid diagnostic kit for detection of HBV, rather than the gold standard ELISA. In addition, incapability to check for HBeAG and viral load was a limitation as it could have pointed to the most likely efficient type of intervention needed to prevent vertical transmission.
Conclusion
This study has found that the prevalence of HBsAg sero-positivity among pregnant women in the study area was in intermediate endemicity according to Center for Disease Control 2012. Concerning factors associated, history of hospital admission, history of surgery, history of dental procedure, and history of body tattooing were found to be associated with HBsAg sero-positivity. Strengthen screening of all pregnant women for HBV as a part of routine ANC in ANC clinics and treating if they are positive to prevent MTCT of HBV. Health education on mode of transmission of HBV, to restrain from high-risk cultural behaviors like body tattooing, and prevention methods should be incorporated for pregnant women at ANC clinics as recommended.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221140778 – Supplemental material for Sero-prevalence and associated factors of hepatitis B virus among pregnant women in Hawassa city public hospitals, Southern Ethiopia: Cross-sectional study design
Supplemental material, sj-docx-1-smo-10.1177_20503121221140778 for Sero-prevalence and associated factors of hepatitis B virus among pregnant women in Hawassa city public hospitals, Southern Ethiopia: Cross-sectional study design by Birku Kassaw, Netsanet Abera, Tegene Legesse, Alemu Workineh and Gizachew Ambaw in SAGE Open Medicine
Footnotes
Acknowledgements
First of all, I would like to thank Hawassa university medicine and health sciences college school of public health for assigning advisors. I would like to show my appreciation for each hospital for their cooperation in providing the requested data preliminary to sampling. Finally, my pleasure also goes to data collectors, study participants, and all those who in one or other way have contributed to the success of this research.
Availability of data and material
All the minimal data sets used to reach the conclusions drawn in the manuscript are included within the manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
Ethical approval for this study was obtained from Institutional Review Board of Hawassa University College of Medicine and Health Sciences (CMHS/IRB 06-012) and official letter of permission was taken from Hawassa city health department. Furthermore, after a thorough discussion and explanations of the purpose, benefit, and possible risks of the study, written informed consent was secured from each study participant before enrolled to study.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from all subjects before the study. For study participants aged <18 years old, written informed consent was obtained from their parents.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.