
Abstract
Background:
Validated predictors of sensitivity or resistance to Bevacizumab (Bev) are not available, and Inflammatory Indexes (IIs) has been reported to be useful prognostic factors in various malignant solid tumours, including metastatic colorectal cancer (mCRC).
Objectives:
To explore the prognostic value of IIs in mCRC patients treated with first-line chemotherapy plus Bev.
Design:
One hundred and eighty-two patients diagnosed with mCRC and treated with first line chemotherapy plus Bev were considered for this prospective non-pharmacological study. Neutrophil, lymphocyte, platelet, aspartate transaminase (AST) and lactate dehydrogenase (LDH) tests were carried out at baseline and before each treatment cycle, according to clinical practice.
Methods:
Pre-treatment Systemic Immune-inflammation Index (SII), Colon Inflammatory Index (CII) and Aspartate aminotransferase-Lymphocyte Ratio Index (ALRI) were evaluated to assess a correlation with progression-free survival (PFS) and overall survival (OS).
Results:
In the overall population, PFS and OS were lower in patients with high SII (HR 1.64, p = 0.006 and HR 1.75, p = 0.004, respectively) and high ALRI (HR 2.13, p = 0.001 and HR 1.76, p = 0.02, respectively), but no difference was detected according to CII value. The multivariate analysis confirmed both SII and ALRI as independent prognostic factors for PFS (HR 1.64 and 2.82, respectively) and OS (HR 1.65 and 2.12, respectively).
Conclusion:
Our results demonstrate and confirm that IIs, and in particular SII and ALRI, are easy to measure prognostic markers for patient candidates to first line chemotherapy plus Bev for mCRC.
Plain language summary
Bevacizumab (Bev) is a humanized monoclonal antibody with antiangiogenic activity, used in combination with chemotherapy as a standard first line treatment for many metastatic colorectal cancer patients. Validated predictors of sensitivity or resistance to Bevacizumab are not available, although several studies have investigated this issue in recent years.
In this study, we investigated whether some selected baseline inflammatory indexes levels, namely Systemic Immune-inflammation Index (SII) and Aspartate aminotransferase-Lymphocyte Ratio Index (ALRI) could predict the survival in patients with metastatic colorectal cancer treated with Bevacizumab plus chemotherapy.
We enrolled 182 patients diagnosed with mCRC and treated with first line chemotherapy plus Bev. For each patient we tested blood neutrophils, lymphocytes, platelets, aspartate transaminase (AST) and lactate dehydrogenase (LDH) before each treatment cycle, according to clinical practice. We calculated the SII value as platelet count × neutrophil count/lymphocyte count, and ALRI as AST/lymphocyte count. We found that patients with high SII and high ALRI values had lower survival as compared to those with low values.
These parameters represent reproducible, inexpensive and easy to measure biomarkers to be used in both clinical practice and clinical trials, for patient selection.

Introduction
Bevacizumab (Bev) is a humanized monoclonal antibody with antiangiogenic activity, which acts by binding to the vascular endothelial growth factor (VEGF). 1 The use of Bev in combination with chemotherapy (CT) is considered a standard first and second-line treatment for several patients with metastatic colorectal cancer (mCRC).
Validated predictors of sensitivity or resistance to Bev are not available, although several studies have investigated this issue in recent years. 2 In particular, studies focusing on VEGF pathway have generally failed, and more attention is being paid to the tumour microenvironment and the inflammatory response.3–9 In this field, Inflammatory Indexes (IIs), such as Systemic Immune-inflammation Index (SII), Colon Inflammatory Index (CII) and Aspartate aminotransferase-Lymphocyte Ratio Index (ALRI) have been reported to be useful prognostic factors in various malignant solid tumour, including colorectal cancer (CRC).10–23
The prognostic and predictive role of endothelial nitric oxide synthase (eNOS) and VEGF polymorphisms, as well as of baseline II was investigated in patients with mCRC treated with first-line CT with or without Bev in the phase III prospective multicenter randomized ITACa (Italian Trial in Advanced Colorectal Cancer) trial (EudraCT no. 2007-004539-44 and on ClinicalTrials.gov (NCT01878422).24–29 The aim of this study was to investigate the prognostic role of IIs in an independent cohort of patients.
Patient and methods
Patient population and treatment regimens
One hundred and eighty-two patients were enrolled onto this prospective non-pharmacological trial to validate eNOS and VEGF polymorphisms as predictors of Bev efficacy. All patients provided written informed consent and the studies were carried out in accordance with the Declaration of Helsinki under good clinical practice conditions and after approval by the local Ethics Committee (IRST and Wide Area Romagna Ethics Committee).
The study design and key eligibility and exclusion criteria, together with data about the prognostic role of eNOS and VEGF polymorphisms have been shown in detail. 30 The present paper shows the results about the prognostic role of the IIs. All patients were treated with chemotherapy doublet (FOLFIRI, FOLFOX4, CAPIRI, CAPOX) plus Bev. Patients were treated until disease progression or unacceptable toxicity occurred. Tumour response was radiologically evaluated every 8 weeks according to the Response Evaluation Criteria in Solid Tumors (RECIST).
Neutrophil, lymphocyte, platelet, aspartate transaminase (AST) and lactate dehydrogenase (LDH) tests were carried out at baseline and before each treatment cycle, according to clinical practice. As in the ITACA trial, IIs obtained with different combination of these factors were investigated. The SII was calculated as platelet count × neutrophil count/lymphocyte count, and the same cutoff (730) used in the ITACA trial was considered for this analysis. 26 ALRI was calculated as AST/lymphocyte count, with the same cut off used in the ITACA trial (14). 28 CII was obtained combining neutrophil-to-lymphocyte ratio (NLR) and LDH. In particular, patients were divided into three risk groups depending on their CII: good [NLR < 3 and LDH ⩽upper limit of normal (ULN)], intermediate (NLR ⩾3 or LDH >ULN) and poor (NLR ⩾3 and LDH >ULN). 29 The cutoff for NLR had been previously determined 26 and the ULN for LDH was provided by the local analysis laboratory.
Statistical analyses
The aim of this analysis was to examine the association between the selected baseline II levels and patient’s outcomes in terms of PFS and OS. PFS was defined as the time-interval between diagnosis of metastatic disease and disease progression or last follow-up visit if not progressed. OS was defined as the time-interval between diagnosis of metastatic disease and death or last follow-up visit.
PFS, OS and their two-sided 95% confidence intervals (95% CI) were estimated by the Kaplan–Meier method and curves were compared by the log-rank test. Hazard ratios (HRs) and their two-sided 95% CI were calculated using the Cox proportional-hazard model. Multivariate analyses were performed after univariate analyses revealed a significant effect of the II. Models were adjusted for chemotherapy regimen (FOLFOX/CAPOX versus FOLFIRI/CAPIRI versus other), gender, age, KRAS status, NRAS status, BRAF status, tumour location (rectum versus right colon versus left colon) and ECOG Performance Status (PS), as suspected confounders derived from the ITACa trial. 24
All p-values were based on two-sided testing and p < 0.05 were considered statistically significant. Analyses were performed using R (version 4.1.0).
Results
Patient characteristics
From January 2016 to October 2019, one hundred eighty-two patients were enrolled onto the present trial at the IRCCS Istituto Romagnolo per lo Studio dei Tumori (IRST) ‘Dino Amadori’ in Meldola. The data cut-off for analysis was October 2019, when the median duration of follow-up was 52.6 months [95% CI: 49.9-Not Reached (NR)]. Information on baseline SII, ALRI and CII levels was available for 132, 86 and 76 patients, respectively; 70 and 62 had low and high SII values, 53 and 33 had low and high ALRI values, and 30, 29 and 17 had good, intermediate and poor CII values, respectively.
Baseline characteristics of patients are shown in Table 1. Patients with high SII had a higher probability of having a poor PS (PS 1-2: 45% versus 20%, p = 0.003) and had a lower chance of bearing a eNOS VNTR 4bb genotype (eNOS VNTR 4bb: 61% versus 77%, p = 0.05), whereas the other characteristics were balanced in patients with low and high SII. We found no significant difference in baseline characteristics of patients with high and low ALRI. A higher proportion of patients with poor CII value had PS 1-2 and carried a NRAS mutation (PS 1-2: 41% versus 35% and 7%, p = 0.006; NRAS mutated: 29% versus 4% and 3%, p = 0.03).
Patients’ characteristics according to inflammatory indexes.

ALRI, Aspartate Aminotransferase-Lymphocyte Ratio Index; CII, Colon Inflammatory Index; ECOG, Eastern Cooperative Oncology Group; SII, Systemic Immune-Inflammation Index.
Progression-free survival as a function of IIs
Results on the impact of treatment on PFS according to the analyzed IIs are summarized in Table 2. Median PFS for patients with low and high SII was 13.2 months (95% CI: 11.8–16.2) and 9.4 months (95% CI: 7.7–12.2), respectively [log-rank p = 0.006, HR 1.64, 95% CI: 1.15–2.34 Figure 1(a)]. Patients with high and low ALRI had a median PFS of 12.4 months (95% CI: 11.6–14.9) and 9.3 months (95% CI: 7.6–11.2), respectively. The difference was statistically significant [log-rank p = 0.001, HR 2.13, 95% CI: 1.34–3.37; Figure 1(b)]. In patients with good, intermediate and poor CII values median PFS was 12.9 months (95% CI: 9.8–16.2), 11.3 months (95% CI: 10.0–15.4) and 8.9 months (95% CI: 6.0–19.1), respectively, but there was no evidence of difference [log-rank p = 0.2, HR intermediate versus good 1.11, 95% CI: 0.66–1.88, HR poor versus good 1.72, 95% CI: 0.92–3.20, Figure 1(c)].
Prognostic value of the Inflammatory Indexes in the cohort in terms of progression-free survival.

Adjusted for CT (FOLFOX/CAPOX versus FOLFIRI/CAPIRI versus Other), gender, age, ECOG PS, KRAS status, NRAS status, BRAF status, tumour localization (rectum versus right colon versus left colon).
95% CI, 95% Confidence Interval; ALRI, Aspartate Aminotransferase-Lymphocyte Ratio Index; HR, Hazard Ratio; SII, Systemic Immune-Inflammation Index; CII, Colon Inflammatory Index; PFS, Progression-Free Survival.

Kaplan–Meier curves of progression-free survival (PFS) for inflammatory indexes. (a) systemic Immune-Inflammation Index, (b) Aspartate Aminotransferase-Lymphocyte Ratio Index and (c) Colon Inflammatory Index.
Overall survival as a function of IIs
Data on the prognostic value of the II in terms of OS are shown in Table 3. Median OS was 29.1 months (95% CI: 20.8–37.1) and 15.0 months (95% CI: 10.9–21.8) in patients with low and high SII, respectively [log-rank p = 0.004, HR 1.75, 95% CI: 1.19–2.57, Figure 2(a)], whereas in patients with low and high ALRI it was 24.6 months (95% CI: 18.5–38.6) and 14.8 months (95% CI: 10.3–22.6), respectively [log-rank p = 0.02, HR 1.76, 95% CI: 1.1–2.82, Figure 2(b)]. Patients with good, intermediate and poor CII values had a median OS of 21.4 months (95% CI: 17.02–35.7), 22.6 months (95% CI: 13.80–44.4) and 14.4 months (95% CI: 8.77–30), respectively [Figure 2(c)]. There was no evidence of association between OS and CII value (log-rank p = 0.1, HR intermediate versus good 0.94, 95% CI: 0.54–1.64, HR poor versus good 1.82, 95% CI: 0.94–3.55).
Prognostic value of the Inflammatory Indexes in the cohort in terms of overall survival.
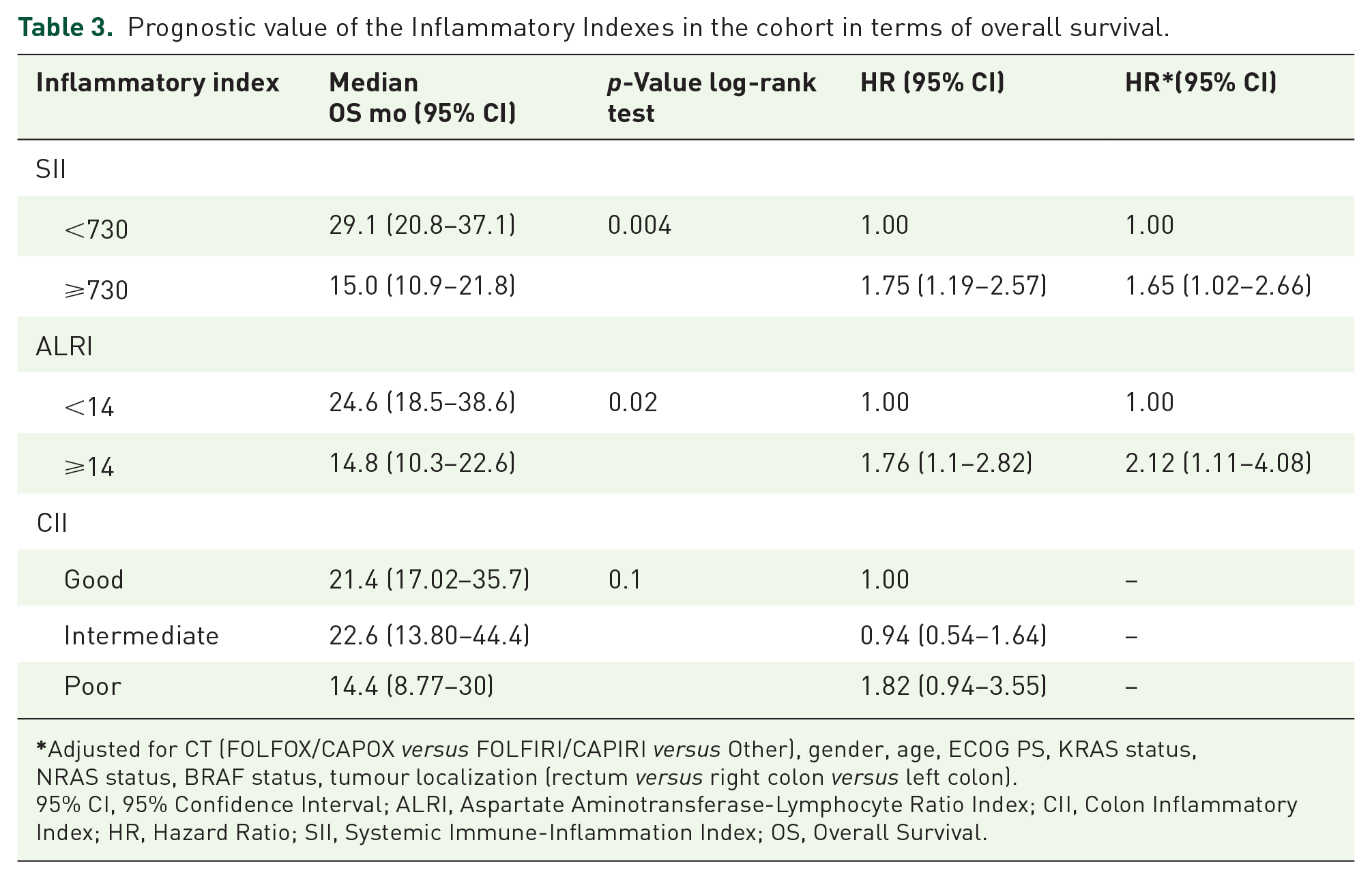
Adjusted for CT (FOLFOX/CAPOX versus FOLFIRI/CAPIRI versus Other), gender, age, ECOG PS, KRAS status, NRAS status, BRAF status, tumour localization (rectum versus right colon versus left colon).
95% CI, 95% Confidence Interval; ALRI, Aspartate Aminotransferase-Lymphocyte Ratio Index; CII, Colon Inflammatory Index; HR, Hazard Ratio; SII, Systemic Immune-Inflammation Index; OS, Overall Survival.
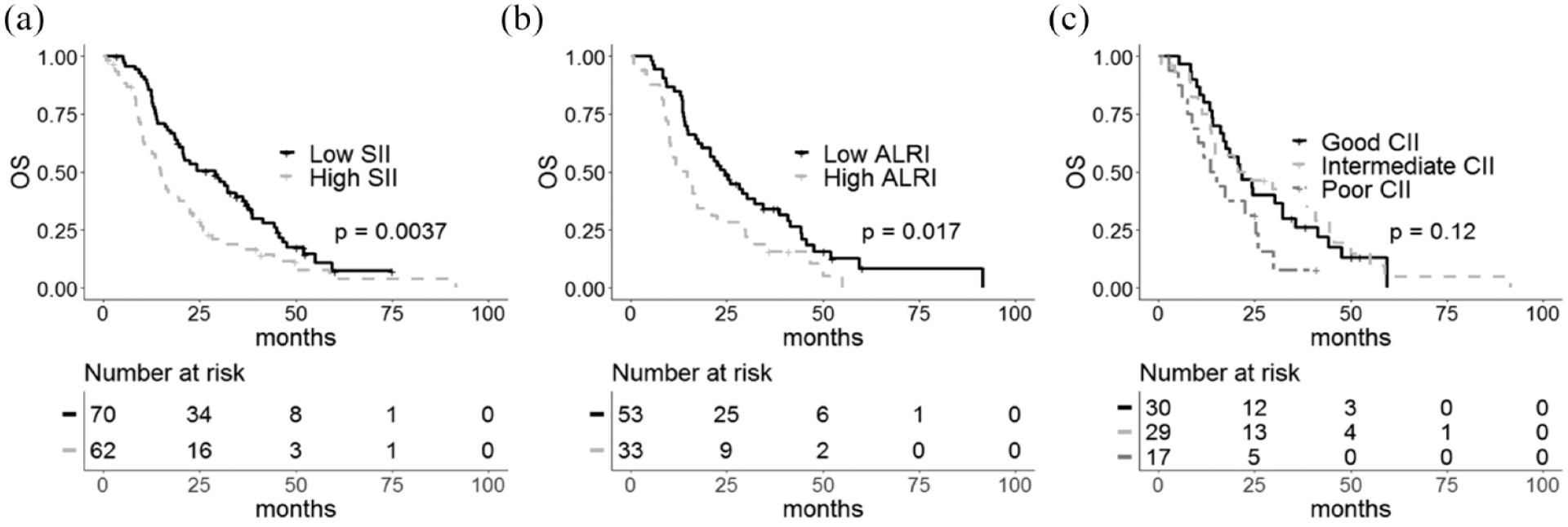
Kaplan–Meier curves of overall survival (OS) for inflammatory indexes. (a) Systemic Immune-Inflammation Index, (b) Aspartate Aminotransferase-Lymphocyte Ratio Index and (c) Colon Inflammatory Index.
Multivariate analysis
Following adjustment for potential confounders (chemotherapy regimen, gender, age, KRAS status, NRAS status, BRAF status, tumour location and ECOG PS), multivariate analysis confirmed both SII and ALRI as independent prognostic factor for PFS (HR adjusted (HR-adj) 1.64, 95% CI: 1.04–2.57; HR-adj 2.82, 95% CI: 1.5–5.18, respectively) and OS (HR-adj 1.65, 95% CI: 1.02–2. 6; HR-adj 2.12, 95% CI: 1.11–4.08, respectively).
Discussion
Cancer-associated inflammation has been identified as a key determinant of disease progression in cancer. Several IIs have been evaluated as predictors of outcome in mCRC patients treated with chemotherapy, while limited data are available about their prognostic role in patients treated with Bev. Our study confirmed the role of SII and ALRI as prognostic indicators for PFS and OS in patients with metastatic mCRC treated with chemotherapy plus Bev.
SII combines neutrophils, platelets and lymphocytes in a single score and has been already associated with prognosis in different malignancies including hepatocellular carcinoma, renal cancer and pancreatic cancer.19,22,32 The role of SII in mCRC setting was assessed in different studies with conflicting results. In a retrospective study on a cohort of patients treated with chemotherapy plus cetuximab 32 three different IIs were studied, neutrophil-lymphocyte ratio (NLR), platelet-lymphocyte ratio (PLR) and SII. An elevated baseline SII was significantly associated with a poor PFS, but not with OS at univariate analysis. Moreover, the prognostic value was not maintained at multivariate analysis, where only NLR remained significantly related to patients’ outcome. A similar study on 102 metastatic KRAS wild type CRC patients treated with chemotherapy plus cetuximab showed comparable results, with NLR significantly associated with PFS and OS, and no prognostic value for SII. 33 On the other hand, in a previous analysis on patients included in ITACa Trial, SII levels were associated with PFS (11.5 versus 8.6 months, in low and high SII patients respectively, p = 0.01) and OS (27.4 versus.15.1 months, p = 0.002) in the sub-group of patients treated with chemotherapy plus bevacizumab but not in chemotherapy only arm. 26 These results, confirmed in this study, suggested a prognostic effect of SII in mCRC patients treated with Bev. Interestingly, several studies reported that platelets were related to angiogenesis and tumour invasion through increasing the production of VEGF in cancer microenvironment, 34 suggesting a possible explanation for this observation.
CII is a novel inflammatory index composed by NLR, an inflammatory index, and LDH serum levels, which are an indirect marker of tumour hypoxia, neo-angiogenesis, metastasis development and poor prognosis in many cancers. 35 The role of this score was investigated in ITACA trial, in a cohort of 276 patients with metastatic CRC treated with chemotherapy plus or minus Bev. 29 In multivariate analysis, CII showed an independent prognostic value in terms of PFS and OS. Considering the sub-group of patients who received treatment with Bev, median PFS was 12.1, 10.0 and 8.6 months for patients with good, intermediate and poor CII, respectively (p ⩽ 0.001). High LDH values may partially explain the poor outcome of patients with high CII on Bev treatment due to a lower efficacy of the drug in hypoxic conditions. Indeed, in hypoxic microenvironment, activation of Hypoxia Inducible Factors-1 (HIF-1) induce transcription of several target genes implicated in angiogenesis, including LDH which may represent an indirect indicator of activated tumour angiogenesis. 36 More recently, CII has been evaluated as a prognostic marker also in patients with resected CRC liver metastases. 37 The study included 90 patients who underwent RO resection for liver metastases with or without perioperative chemotherapy. Multivariate analysis showed CII score as an independent predictor of OS in this setting. Unfortunately, our study did not confirm the prognostic value of CII in patients treated with chemotherapy plus Bev, perhaps due to the small sample size.
Our analysis also confirmed the prognostic role of ALRI, a score combining the inflammatory state with a liver injury index, in terms of both PFS and OS. Increased serum AST is related with hepatic cells injury and may be associated with progression of liver disease, while lymphocytes play a crucial role in antitumour immune response, inducing cytotoxic cell death and inhibiting tumour cell proliferation and migration. 38 The prognostic role of ALRI was evaluated in hepatocellular carcinoma (HCC) in several retrospective studies, showing that high ALRI predicted poor survival. 39 Only few data are available about the prognostic role of ALRI in mCRC. In particular, we investigated the role of ALRI in the ITACA trial 28 in 284 metastatic CRC patients treated with chemotherapy with or without Bev and showed that high levels of ALRI at baseline were associated with shorter PFS and OS. Similar results were observed in a cohort of 44 CRC patients undergoing trans arterial radio embolization for CRC liver metastasis, where a low pre-treatment ALRI score was associated with longer OS. 40
The main drawback of our study is the limited number of patients. The trial, in fact, was not designed to validate IIs, thus no power calculation had been performed to properly determine the sample size. Missing data, moreover, further reduce the sample size, having a huge impact in multivariate analysis. The lack of statistical significance, therefore, should not be interpreted as absence of effect and future studies should be correctly developed to validate IIs.
Conclusion
In conclusion, SII and ALRI were confirmed as powerful predictive indicators of poor outcome in mCRC patients treated with chemotherapy plus Bev. These parameters represent reproducible, inexpensive and easy to measure biomarkers to consider for patients’ selection.