
Abstract
Recently, immune checkpoint inhibitors (ICIs) have become the standard treatment option for patients with lung cancer, including small cell lung cancer (SCLC). ICI-induced neurological immune-related adverse events are rare and exhibit diverse clinical manifestations, often leading to missed or delayed diagnosis. Herein, we report the case of a patient with extensive-stage SCLC who received atezolizumab with etoposide/platinum and gradually developed neurological symptoms after three cycles of chemoimmunotherapy. Subsequently, the patient received a diagnosis of subacute immune-related cerebellar ataxia and was treated successfully with pulse steroid therapy. The patient exhibited almost complete remission of neurological symptoms and had progression-free survival for >24 months.
Keywords
Introduction
With the increasing popularity of immune checkpoint inhibitors (ICIs) as the first-line or adjuvant therapy for lung cancer, understanding immune-related adverse events (irAEs), including neurological irAEs (nirAEs), has become essential for clinicians. ICI-induced nirAEs are rare, and a precise diagnosis of nirAEs is challenging. A systemic approach (i.e. the categorization of the involved neuroanatomy and the baseline assessment of complete blood count, liver function, renal function, and thyroid function) and a thorough evaluation of neuronal antibodies may facilitate dignosis. 1 However, cerebellar magnetic resonance imaging (MRI) reveal no abnormalities in most patients. Seropositivity and seronegativity may vary across cancer types; the non-small cell lung cancer (SCLC) has the highest seronegativity rate, which means probably there was no any detectable neuronal antibodies in these patients with nirAEs. 2 The immediate discontinuation of ICI use and the use of patient management strategies specific to the type and severity of nirAEs are crucial for improving patient prognosis. Our knowledge regarding nirAE-associated cerebellar ataxia in patients with SCLC and its posttreatment prognosis remains limited. Herein, we report a case of cerebellar ataxia in a patient who received atezolizumab plus chemotherapy for SCLC. The patient was successfully treated with high doses of steroids. He remained disease-free after the improvement of nirAE symptoms.
Case presentation
A 46-year-old man had a diagnosis of SCLC of the upper lobe of the left lung with mediastinal lymphadenopathy; metastases to the right liver, left scapula, and sacrum were also noted. Clinical staging was determined to be T1bN3M1c and extensive stage based on Veterans Administration Lung Study Group staging. The patient received three cycles of chemoimmunotherapy with platinum, etoposide, and atezolizumab. Chest computed tomography (CT) indicated almost complete resolution of the previous lung tumor, mediastinal lymphadenopathy [Figure 1(b)]. However, 2 weeks after the latest chemoimmunotherapy, the patient reported progressive dysarthria and unsteady gait with clear consciousness. Neurological assessments revealed multidirectional nystagmus (video in Supplementary Material), saccadic pursuit, hypometric saccade, asymmetric dysmetria with left-side dominance, slight wide-based gait, and evident unsteadiness during tandem stance. Muscle power, sensory function, deep tendon reflex, and visual field were all intact. Bilateral flexion (normal) was noted for the plantar reflex. Emergent brain MRI revealed no intracranial lesions [Figure 1(c)]. Analysis of the patient’s cerebrospinal fluid (CSF) revealed no pleocytosis, and CSF glucose and protein levels were within the normal range. No antinuclear or extractable nuclear antigen antibodies were detected in his serum. The CSF contained no autoantibodies associated with paraneoplastic neurological syndrome (PNS) or limbic encephalitis (Table 1). The electrophysiological examination, which included motor and sensory nerve conduction studies to assess the function of the patient’s peripheral nerve system, revealed mostly normal results. There was a slight reduction observed in the sensory nerve action potential, which could potentially indicate an early sign of chemotherapy-related polyneuropathy. A multidisciplinary discussion with the neurologists led to a diagnosis of ICI-induced subacute cerebellar ataxia in our patient. The patient’s initial score on the Scale for the Assessment and Rating of Ataxia (SARA) was 19. After receiving dexamethasone at a dose of 30 mg/day for 5 days, the patient exhibited improved clinical symptoms with mild neurological deficit. Subsequently, pulse therapy was started with methylprednisolone at a dose of 1000 mg/day for 5 days, followed by oral prednisolone at a dose of 80 mg/day for 2 weeks, with gradual tapering [Figure 1(a)]. The patient’s neurological deficit improved gradually, and his SARA score was 6 after 1 month of steroid treatment. Chemoimmunotherapy was then terminated. After complete neurological recovery, the patient received thoracic radiotherapy. He exhibited progression-free survival for >24 months without any recurrence of nirAE.

(a) Clinical course of the neurological immune-related adverse event and steroid treatment. (b) Serial chest CT scan. (i) CT performed before chemoimmunotherapy administration revealed the presence of a tumor on the upper lobe of the left lung (arrow) and liver metastasis over right lobe of liver (black arrow). (ii) CT performed after three cycles of chemoimmunotherapy indicated almost complete remission without a residual tumor. (iii) Latest CT performed at follow-up, approximately 24 months after the neurological immune-related adverse event, indicated no disease progression. (c) Serial brain MRI. (i) Brain MRI performed before chemoimmunotherapy administration revealed no metastatic lesions. (ii) MRI performed few days after progressive ataxia. (iii and iv) MRI performed three and 24 months after the event showed slight cerebellum atrophy, as evident from the widened cerebrospinal fluid space (arrowhead).
The CSF finding and the results of autoantibodies.
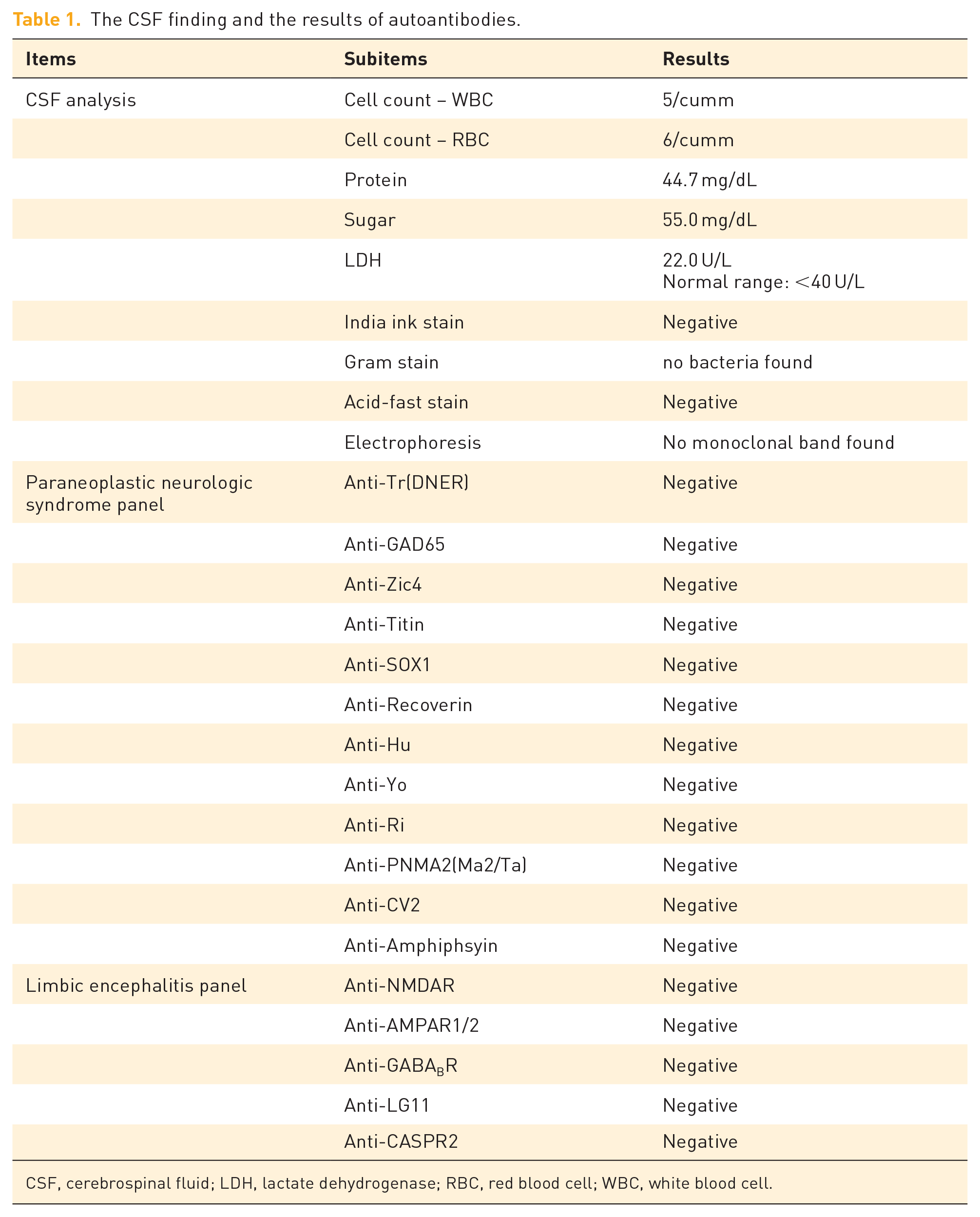
CSF, cerebrospinal fluid; LDH, lactate dehydrogenase; RBC, red blood cell; WBC, white blood cell.
Discussion
The symptoms of nirAEs are similar to those of paraneoplastic cerebellar degeneration (PCD) and fulfill the criteria for PNS. In our patient, neuronal autoantibodies were absent. PCD is usually associated with mild lymphocytic pleocytosis and the presence of Yo autoantibodies in the CSF. Patients with PCD often have an unfavorable outcome. Our patient was diagnosed as having atezolizumab-induced subacute cerebellar ataxia, rather than PCD, based on the absence of neuronal autoantibodies in the CSF and a temporal relationship with atezolizumab. A recent systemic review on cerebellar involvement associated with ICIs revealed that 38.1% of all studied patients had no detectable autoantibody, which indicates that seropositivity is not essential for diagnosis. 2 Notably, the excellent response of our patient to steroid therapy further supported this perspective. Recently, novel antibodies targeting neuronal antigens, such as tripartite motif-containing (TRIM) protein 9 (TRIM9) and protein 67 (TRIM67), have been detected in patients with PCD and lung cancer. 3 Sebbag et al. 4 reported a case of ICI-induced cerebellar ataxia in a 47-year-old patient with SCLC who received atezolizumab; subsequently, the patient was diagnosed as having TRIM9-antibody-positive ICI-induced cerebellar irAE. Unfortunately, no clinical improvement was noted after the administration of immunosuppressants. Another case of atezolizumab-induced cerebellar ataxia was reported by Tan et al. 5 In their study, a 66-year-old man was diagnosed as having lung adenocarcinoma; his condition was similar to that of our patient. He exhibited an initial improvement in cerebellar ataxia within 1 week of treatment initiation; however, ataxia recurrence was observed soon after the treatment. He died after 5 months due to progressive metastatic disease. We reviewed relevant case reports published within the last 5 years and identified two cases of ICI-induced cerebellar ataxia in patients with lung cancer.6,7 Clinical manifestations are similar between our case and the aforementioned four cases. However, our patient exhibited a more favorable response to immunosuppressive therapy than did the other patients (Table 2). To the best of our knowledge, this is the first case report on a patient with SCLC with atezolizumab-induced cerebellar ataxia who exhibited almost complete remission of neurological symptoms after receiving steroid treatment and who had progression-free survival for >24 months. The brain MRI image obtained 2 years after the occurrence of nirAE demonstrated slight cerebellar atrophy [Figure 1(c)], without any newly developed neurological symptoms being observed. We retrieved a cohort study on ICI-related encephalitis; this study included four patients with lung cancer and concurrent cerebellar syndrome. Of them, two exhibited a favorable response. 8 However, we cannot include these cases because of the lack of a detailed description and clinical manifestation data. In light of the aforementioned studies, we hypothesize that patients with ICI-induced nirAE-associated cerebellar ataxia would exhibit diverse treatment responses and prognoses. Patients with SCLC with neurological PNS may have better overall survival than those without neurological PNS. 9 However, whether this finding is valid in patients with ICI-induced nirAE that mimics PNS remains debatable. Furthermore, the detection of novel antibodies in patients with nirAE and better clinical description may help us categorize patients into specific subgroups; this, in turn, may facilitate improved prognosis and treatment outcomes. 1 Subacute cerebellar ataxia has various etiologies, including infection, stroke, degenerative disease, and viral infection (e.g. Epstein-Barr virus); these factors may be considered before subacute cerebellar ataxia is assessed as an nirAE. 10 In the era of ICIs, the early diagnosis of nirAEs and the prompt administration of systemic immunosuppressants may lead to favorable neurological outcomes and long-term progression-free survival in patients with ICI-induced nirAE.
Comparison of the case reports on cerebellar ataxia associated with ICIs.

123I-IMP SPECT,
Conclusions
We reported the case of a patient with SCLC who developed nirAE-associated cerebellar ataxia after receiving atezolizumab for SCLC. In contrast to the poor response to immunosuppressants noted in patients with ICIs-associated cerebellar ataxia described in the literature, our patient exhibited an excellent response to immunosuppressive therapy with no subsequent disease progression. This suggests a heterogeneity in nirAEs and the importance of early diagnosis and management. To our knowledge, this is the first detailed report on subacute cerebellar ataxia associated with ICI administration in which a favorable clinical outcome was noted. The complete remission of neurological symptoms was observed with progression-free survival for >24 months.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.