
Abstract
Antibody–drug conjugates (ADCs) are a class of antineoplastic agents whose structure is composed of three main components: a monoclonal antibody (mAB) targeting a specific target antigen, a cytotoxic payload, and a linker binding the antibody to the payload. By combining the specificity of mABs with the high potency of the payloads, ADCs constitute a smart drug delivery system with improved therapeutic index. After recognition and binding of the mAB to its target surface antigen, ADCs are internalized by endocytosis by the tumor cell, releasing the payloads into the cytoplasm, where they exert their cytotoxic activity, eventually leading to cell death. The composition of some of the new ADCs confers additional functional properties that allow expanding their activity to neighboring cells not expressing the target antigen, constituting a valuable strategy to overcome tumor heterogeneity. Some of these ‘off-target effects’, such as the bystander effect, are possibly the mechanism underlying the antitumor activity demonstrated in patients with low expression of the target antigens, which represents an important paradigm shift in anticancer targeted therapy. Three ADCs are currently approved for the treatment of breast cancer (BC); two anti-HER2 (human epidermal growth factor receptor 2) ADCs (trastuzumab emtansine and trastuzumab deruxtecan); and one Trop-2-targeted ADC (sacituzumab govitecan). Based on the unprecedented efficacy data demonstrated by these agents, ADCs have been incorporated as part of standard regimens for all subtypes of advanced BC, as well as for high-risk early HER2-positive BC. Despite the remarkable advances, several hurdles still remain to overcome, including the development of reliable biomarkers for patient selection, prevention, and management of potentially severe toxicities, ADC resistance mechanisms, post-ADC resistance patterns, and optimal treatment sequencing and combinations. In this review, we will summarize the currently available evidence related to the use of these agents, as well as explore the current landscape of ADC development for BC treatment.
Background
High rates of adverse events and a narrow therapeutic index 1 were hallmarks of the first chemotherapeutic agents to demonstrate antitumor activity in the early 20th century. Since then, a major drug development ambition in oncology has been the development of compounds that could act on specific tumor targets with minimal or no effect on normal cells, with the promise of improved efficacy and reduced toxicities. 2 This aspiration was largely facilitated by improvements in nuclear acid sequencing technologies that allowed the characterization of malignancies according to molecular alterations, thus examining these aberrations as potential therapeutic targets. Breast cancer (BC) is perhaps one of the best examples of solid malignancies that had their natural history modified by targeted therapies whose development were only made possible by the accumulation of knowledge about tumor biology. 3 However, even in the successful case of anti-HER2 agents for BC therapy, the use of concomitant chemotherapy is often required to optimize antitumor effects. 4 Antibody–drug conjugates (ADC) are a class of anticancer agents developed as an attempt to overcome the major limitations of monoclonal antibodies and cytotoxic compounds through a smart strategy of tumor-specific drug delivery. 5 In this narrative review, we will explore the main characteristics, efficacy data, and safety profile of approved and investigational ADC for the treatment of BC.
Molecular structure and mechanism of action of ADCs
The structure of ADCs is characterized by three core components: a monoclonal antibody (mAB) bound by a molecular linker to a cytotoxic agent (payload). 5 All three elements are important determinants of ADC efficacy and toxicity. Conjugation is the methodology used for the linker fixation on the mAB backbone in which the linker is attached on a stochastic or site-specific manner to one of the mAB’s available amino acids. The average number of drug molecules conjugated per antibody is defined as Drug-Antibody Ratio or ‘DAR’. The conjugation methods used impact the DAR and the homogeneity of the payloads on the mAb, being partially responsible for improvements on ADCs’ therapeutic indexes. 6
The chemical characteristics of the mAB of each ADC are major determinants of its immunogenicity and of the circulating half-life of the drug. 7 The binding of the mAB to its target surface antigen through the fragment antigen-binding (Fab) portion leads to the formation of a mAB-antigen complex, which is then internalized. 8 Internalization of the mAB-antigen complex may occur by several mechanisms, including antigen-dependent caveolin-mediated endocytosis, clathrin-mediated endocytosis, or antigen-independent pinocytosis. 9 In the endosome, acidification or proteolysis triggers the release of the payload in the cell cytoplasm, finally reaching its intracellular target. 5 This mechanism of releasing the payload directly into cells that express the target antigen, in a ‘Trojan horse’ fashion, is responsible for a significant reduction in systemic side effects.
Linkers can be classified as ‘cleavable’ and ‘non-cleavable’, and they are a key component of the structure of any ADC, since they are responsible for reducing potential side effects related to the premature payload release by stabilizing the drug in the circulation. Non-cleavable linkers, such as the thioether linker present in T-DM1, provide a high stability to the compounds and allow a relatively delayed payload release, as this process relies on the lysosomal enzyme degradation of the ADC. 6 Cleavable linkers can be subcategorized as chemically or enzyme-cleavable, and cleavage mechanisms may involve (1) internalization of the ADC-antigen complex by endocytosis, lysosomal processing, and intracellular payload release (‘traditional’ cleavage mechanism) or (2) non-internalizing mechanisms, in which the payload is released extracellularly (e.g. tumor microenvironment or circulation). 10 Non-internalizing mechanisms of payload release are hypothesized to be associated with potentially greater efficacy due to lower dependence on intracellular trafficking process and on high cell-surface antigen expression, but also lower cell selectivity. 10 Thus, a significant part of off-target toxicity of newer generation ADCs has been associated to the premature payload release by cleavable linkers, which are subdivided into four main subclasses (hydrazone, cathepsin B-cleavable, disulfide, and pyrophosphate diester). 6
Payloads are the cytotoxic agents conjugated to the mAB, which are usually highly potent agents associated with excessive toxicity that precludes their use in the unconjugated form. 11 Such a high potency, on the contrary, becomes a major advantage in the ADC context, considering that only a small amount of ADC administrated intravenously will reach tumor cells (as low as 0.001–0.01%) and that the payloads delivered need to be active at nanomolar or even picomolar concentrations.12,13
Although the ‘on-target’ effect (i.e. cytotoxic effect after ADC internalization in cancer cells that express the target antigen) is hypothesized to be the main mechanism of action of ADCs, several features of the components of the ADC structure play a crucial role in other aspects that also contribute to their antitumor activity. 8 In ADCs with cleavable linkers, membrane-permeable hydrophobic payloads may diffuse from the interior of dying cells that endocytosed the ADC to the neighboring cells, on which they can elicit a cytotoxic effect regardless of target antigen expression. 14 This phenomenon known as ‘bystander effect’ is believed to have paramount importance in cases of heterogeneous or low-level expression of the target antigens. In some cases, mABs present in the ADC structure retain Fab-mediated antitumor activity by interfering with pathways initiated by antigens expressed on the cell surface by blocking ligand binding, dimerization, and/or inducing degradation of the target protein.5,14,15 These mechanisms, which are typical of ‘classical’ targeted therapies, may also occur with some ADCs, although they are not their main mechanism of action. Finally, ADCs may elicit immune-mediated antitumor responses by several mechanisms, including (1) antibody-dependent cell-mediated cytotoxicity by the recognition of mAB Fc component by immune cells such as natural killers, (2) antibody-dependent cell-mediated phagocytosis by the interaction with tumor-associated macrophages, and (3) complement-mediated cytotoxicity through C1q binding. 5
ADCs currently approved for BC treatment
Two anti-HER2 ADCs (ado-trastuzumab emtansine and fam-trastuzumab deruxtecan-nxki) and one Trop-2-targeted ADC (sacituzumab govitecan) are currently approved by the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of BC (Figure 1, Table 1).

ADCs currently approved by the US FDA and EMA for the treatment of breast cancer.
Key efficacy results of ADCs currently approved by the US FDA and EMA.

aBC, advanced breast cancer; AC/EC, doxorubicin or epirubicin plus cyclophosphamide; ADCs, Antibody–drug conjugates; CI, confidence interval; eBC, early breast cancer; EFS, event-free survival; EMA, European Medicines Agency; HR, hazard ratio; IDFS, invasive disease-free survival; ITT, intention-to-treat; mOS, median overall survival; mPFS, median progression-free survival; NR, not reported; ORR, objective response rate; OS, overall survival; SG, sacituzumab govitecan; TC-HP, docetaxel, carboplatin, and trastuzumab plus pertuzumab; T-DM1 + P, T-DM1 plus pertuzumab; TH, trastuzumab plus paclitaxel; THP, taxane plus trastuzumab plus pertuzumab; TNBC, triple negative breast cancer; TPC, treatment of physician’s choice.
Ado-trastuzumab emtansine
T-DM1 (ado-trastuzumab emtansine) was the first HER2-targeted ADC to be granted approval for the treatment of solid malignancies. This agent combines the anti-HER2 activity of trastuzumab, a humanized anti-HER2 IgG1 mAb, withthe cytotoxic properties of DM1, and a microtubule inhibitor derived from maytansine.Trastuzumab is binded to DM1 through a non-reducible thioether linker(N-succinimidyl-4-(N-maleimidomethyl) cyclohexane-1-carboxylate).31,32
In the metastatic setting, the EMILIA trial was the pivotal study demonstrating the efficacy of T-DM1 in the second-line setting. In this study, 991 patients with HER2-positive advanced BC (aBC) previously treated with taxane-based chemotherapy and trastuzumab, were randomized to receive T-DM1 or capecitabine plus lapatinib. T-DM1-based therapy led to significant improvements in all the primary endpoints: median progression-free survival (mPFS) was 9.6 versus 6.4 months (HR 0.65, 95% CI 0.55–0.77, p < 0.001), and in the final descriptive analysis, at a median follow-up of 41.9 months in the control group and 47.8 months in the T-DM1 group, median overall survival (mOS) was 29.9 months versus 25.9 months (HR 0.75, 95% CI 0.64–0.88). 16 These results were confirmed in a more heavily pretreated population by the results of TH3RESA trial, since mPFS (6.2 versus 3.3 months, HR 0.52, 95% CI 0.422–0.661 p = 0.0001) and mOS (22.7 versus 15.8 months, HR 0.68, 95% CI 0.54–0.85, p = 0.0007) were also improved by T-DM1 as compared to the treatment of physician’s choice (TPC) group comprising of chemotherapy (any single agent), hormonal therapy for hormone-receptor-positive disease (single-agent or dual therapy), or HER2-directed therapy (single-agent, dual HER2-targeted therapy, or combination with either single-agent chemotherapy or single-agent hormonal therapy). 17 Hence, until late 2021, T-DM1 was considered the preferred second-line therapy for the treatment of HER2-positive metastatic patients.
In the early setting, the KATHERINE trial led to the approval of T-DM1 as post-neoadjuvant treatment for patients with residual disease after a neoadjuvant treatment. In this phase III trial, 1486 patients who had not achieved a pathological complete response (pCR) after neoadjuvant taxane-based chemotherapy combined with anti-HER2 treatment (with or without anthracyclines) were randomized to receive adjuvant T-DM1 or trastuzumab, both for 14 cycles. At a median follow-up of 41.4 months, the estimated invasive disease-free survival (iDFS) was 88.3% for the T-DM1 arm, compared to 77% for the standard arm (HR 0.50, 95% CI 0.39–0.64, p < 0.001). T-DM1 showed its benefit in every subgroup of patients, notwithstanding pathological nodal status, hormonal expression, age, and type of anti-HER2 therapy used. 18 While the KATHERINE trial has used T-DM1 as an escalation strategy in patients at high risk of relapse, the ATEMPT trial aimed to test if this drug could be used to ‘de-escalate’ adjuvant treatment in patients with stage I HER2-positive disease. In this study, 497 patients were randomized to receive T-DM1 for 17 cycles or paclitaxel and trastuzumab with standard schedule in the adjuvant setting. The objective of the study was to evaluate if T-DM1 was less toxic than standard adjuvant treatment and yielded clinically acceptable iDFS. At a median follow-up of 3.9 years, iDFS were 97.8% and 93.4% for T-DM1 and paclitaxel-trastuzumab, respectively. The incidence of clinically relevant toxicities was similar in both arms (46% versus 47%, p = 0.83) and a higher number of patients (17%) had early T-DM1 discontinuation due to adverse events (AE) as compared to the paclitaxel-trastuzumab arm (6%). 19 The ongoing ATEMPT 2.0 trial is comparing adjuvant paclitaxel and trastuzumab with T-DM1 for six cycles (18 weeks) followed by trastuzumab for 11 cycles (NCT04893109).
T-DM1 activity was also tested in combination with other HER2-targeted agents in the early setting. The phase III KAITLIN trial randomized patients with HER2-positive BC with tumor size >2 cm or node positive to receive adjuvant chemotherapy with anthracyclines followed by pertuzumab and T-DM1 or taxane plus pertuzumab and trastuzumab. No significant difference was seen in terms of iDFS rate at a median follow-up of 57 months, 93.1% (95% CI 91.4–94.7) versus 94.2% (95% CI 92.7–95.8). 20 In the neoadjuvant setting, the phase III KRISTINE trial randomly assigned 444 patients with locally advanced HER2-positive BC to receive neoadjuvant chemotherapy with T-DM1 plus pertuzumab or docetaxel, carboplatin, and trastuzumab plus pertuzumab. Higher pCR rates were seen in patients treated with the standard treatment, as compared to T-DM1 plus pertuzumab (55.7% versus 44.4%; p = 0.016). At a median follow-up of 37 months, the 3-year event-free survival was 85.3% in the T-DM1 and pertuzumab arm, compared to 94.2% in the other arm (HR 2.61, 95% CI 1.36–4.98). No significant differences in iDFS (HR 1.11, 95% CI 0.52–2.40) and OS (HR 1.21, 95% CI 0.37–3.96) were found.18,21
A recent review assessing the combined incidence of AE in patients treated with anti-HER2 agents included data from 20 studies reporting T-DM1- related AE. Among these patients, the most common side effect were decreased platelet count (incidence of 84.6%, with more than 20% of grade ⩾3), hepatotoxicity (53.6%), diarrhea (19.6%), vomiting (19.2%), hypokalemia (10–15%), and cutaneous reactions (7.7%). 33 A pooled analysis of individual data from over 1900 patients treated with T-DM1 in seven clinical trials demonstrated a rate of adverse cardiac events of 3.4%, most of which were characterized by asymptomatic left ventricular ejection fraction (LVEF) drops. 34 Notably, in the TH3RESA trial 7% of patients treated with T-DM1 experienced AE leading to treatment discontinuation, while in the KATHERINE trial, in adjuvant setting, the rate of T-DM1 discontinuation was 28.5%.17,18 Figure 2 summarizes the toxicity profile of ADCs currently approved for BC treatment, as reported in the main registration trials.23,28

Incidence of adverse events associated with T-DXd, T-DM1, and SG in DESTINY-Breast03 and ASCENT trials.
Trastuzumab Deruxtecan (T-DXd)
Fam-trastuzumab deruxtecan-nxki (T-DXd or DS-8201) is an ADC consisting of humanized anti-HER2 immunoglobulin G1 antibody linked to deruxtecan, a topoisomerase I inhibitor payload derived from exatecan through a tetrapeptide-based cleavable linker. It is characterized by a relevant bystander effect and a high DAR of 8:1 (compared to a DAR of 3.5:1 in T-DM1). 35 In the open-label, single-group DESTINY-Breast01 trial, heavily pretreated patients (median of six previous treatments received) who received T-DXd at the recommended dose (5.4 mg/kg) experienced an ORR of 60.9% (95% CI 53.4–68.0) and a mPFS of 16.4 months (95% CI 12.7 to not reached). 36 The activity of this ADC was further tested in a larger phase III trial (DESTINY-Breast02) comparing T-DXd with TPC in similar later-line patient population (>99% with prior treatment with T-DM1). Primary results of this study confirmed the clinical benefit and superiority of T-DXd over conventional chemotherapy-based regimens in this setting with prolonged PFS (HR, 0.36; 95% CI 0.28–0.45; p < 0.000001) and OS (HR, 0.66; 95% CI 0.50–0.86; p = 0.0021). 37
In the phase III DESTINY-Breast03 trial, 524 patients with HER2-positive aBC pretreated with trastuzumab and a taxane were randomly assigned to receive T-DXd or T-DM1. Patients with newly diagnosed or progressing brain metastases were not eligible. At 12 months, 75.8% of patients treated with T-DXd were alive and without disease progression, compared to 34.1% of those treated with T-DM1 (HR 0.28, 95% CI 0.22–0.37; p < 0.001). Overall response rate (ORR) was 79.7% in the T-DXd arm and 34.2% in the T-DM1 arm. The benefit in terms of PFS was seen in all the subgroups, irrespective of hormone-receptor status, previous treatment with pertuzumab, presence of visceral disease, number of previous lines, or presence of stable brain metastases. 23 Based on the results of this trial, T-DXd has become the preferred second-line regimen for HER2-positive aBC. The updated survival results of this trial were presented in SABCS 2022, confirming the superiority of T-DXd. With a median follow-up of 28.4 months, the risk of death was reduced by 36% (HR, 0.64, 95% CI 0.47–0.87; p = 0.0037) with the median OS not reached in any of the arms. The landmark of 12 months OS rate remained superior in T-DXd (94.1% versus 86.0%) and 24 months OS rate was 77.4% for T-DXd compared to 69.9% for T-DM1. 24
Interestingly, approximately 60% of HER2-negative aBCs express low levels of HER2 (HER2-low), defined as a score of 1+ on immunohistochemistry (IHC) or an IHC score of 2+ and negative results on in situ hybridization (ISH) 38 These tumors were traditionally treated as HER2-negative malignancies due to the inefficacy of previously available HER2-directed therapies to improve their outcomes.39–41 Under the hypothesis that T-DXd could potentially be active in this population particularly through the bystander effect to neighboring tumor cells heterogeneously expressing HER2, 35 T-DXd efficacy was also evaluated in patients with HER2-low aBC in the DESTINY-Breast04 trial. 15 In this phase III trial, patients pretreated for HER2-low aBC were randomized 2:1 to receive T-DXd or TPC (eribulin, capecitabine, gemcitabine, paclitaxel, or nab-paclitaxel). Among 557 randomized patients, median PFS was 9.9 months in the T-DXd arm and 5.1 months in the control arm (HR 0.50, 95% CI 0.40–0.63, p < 0.001), while mOS was increased from 16.8 months to 23.4 months in patients treated with T-DXd (HR 0.64; 95% CI 0.49–0.84, p = 0.001). In the hormone receptor-positive subgroup (88.7%, 494 patients) the mPFS was 10.1 months in the T-DXd arm and 5.4 months in the control arm (HR 0.51, 95% CI, 0.40–0.64, p < 0.001), and mOS was 23.9 versus 17.5 months (HR 0.64, 95% CI, 0.48–0.86, p = 0.003), consistent with the data of overall population. In the hormone-negative subgroup (11.3%, 63 patients), the median mPFS was 8.5 months for patients treated with T-DXd and 2.9 months for patients who have undergone TPC treatment (HR 0.46, 95% CI, 0.24–0.89), mOS was 18.2 and 8.3 months, respectively (HR 0.48, 95% CI 0.24–0.95). 25 However, the number of patients with hormone receptor-negative disease was limited and this data should be seen with caution. Further data of patients with hormone receptor-negative, HER2-low aBC treated with T-DXd were presented in SABCS 2022 with the updated results of the cohort treated with T-DXd in combination with durvalumab from the BEGONIA phase Ib/II trial. In this study, patients treated with the combination in the first-line setting achieved an ORR of 57% and a median PFS of 12.6 months, with a manageable safety profile. 42
The unprecedented results of the DESTINY-Breast04 trial demonstrating the efficacy of T-DXd in patients with HER2-low BC represent a paradigm shift by demonstrating the activity of this agent in a population traditionally considered HER2-negative, which expand its indication for patients with HER2-low tumors traditionally classified as hormone receptor-positive/HER2-negative and triple negative breast cancer (TNBC). Interestingly, new data were presented in SABCS 2022 in the early setting with the presentation of the TRIO-US B-12 TALENT neoadjuvant study. This trial randomized patients with previously untreated, operable invasive early stage, hormone receptor-positive, HER2-low BC measuring >2 cm to receive T-DXd alone (Arm A) or in combination with anastrozole (with gonadotropin-releasing hormone (GnRH) agonist in men and pre/perimenopausal women) (Arm B). The ORR was 68% in arm A and 58% in arm B. At the time of this presentation, some patients were still receiving therapy and data were not fully mature for the primary endpoint (pCR rate at surgery) or for long-term outcomes. 43 In addition to providing efficacy and safety data, window trials such as TRIO-US B-12 TALENT trial provide valuable opportunities for translational research in this setting.
The most common any-grade AEs associated with T-DXd are gastrointestinal (nausea, vomiting, constipation), hematological (anemia, neutropenia, thrombocytopenia), fatigue, and alopecia. 44 Hematological AEs, particularly neutropenia and anemia, and fatigue are also among the most frequent high-grade (grade ⩾3) events and leading causes of dose interruptions due to AEs, which were required in approximately 32% of patients treated with T-DXd. 44 Left ventricular dysfunction was reported in 2.7% (7 of 257) of the patients treated with T-DXd in DESTINY-Breast03; all cases were asymptomatic and low grade (grade 1–2).24,45 Thus, LVEF assessment should be performed before beginning treatment with T-DXd and at regular intervals during treatment. 45 Considering T-DXd’s safety profile, a particular concern relates to interstitial lung disease (ILD) due to reports of high-grade and fatal events. 25 ILD is the most common type of drug-induced lung toxicity and is associated with inflammation and fibrosis of the pulmonary interstitium that may ultimately lead to loss of functional gas exchange. 46 It has been hypothesized that the mechanisms of T-DXd-related ILD may involve target-dependent or target-independent uptake of ADC by normal cells; or direct damage caused by the free payload, either released by premature deconjugation into the circulation or from cells following ADC catabolism.47,48 Preclinical evidence demonstrate that, although T-DXd induces ILD in animal models, those receiving deconjugated DXd did not experience lung toxicity, failing to corroborate the hypothesis of direct lung damage caused by the free payload. 48 Furthermore, the low levels of HER2 expression in alveoli 48 and the occurrence of ILD in patients exposed to non-HER2-targeted ADCs (e.g. HER3-targeted patritumab deruxtecan) 49 undermine the hypothesis that this toxicity is caused by target-dependent ADC uptake. Thus, the accumulated evidence suggests that the development of ILD is predominantly associated with target-independent ADC uptake by normal cells (e.g. immune cells), which is supported by the finding of ADC accumulation in alveolar macrophages (and not in pulmonary epithelial cells) in animal models of T-DXd-induced ILD. 48 In a pooled analysis of nine phase I/II trials with T-DXd including data from 1150 patients (44.3% with BC), the incidence of any-grade ILD was 15.4% (177 patients), of which 77.4% (137/177) were grade 1–2, 8.5% (15/177) were grade 3–4, and 14% (22/177) were grade 5. 50 Importantly, the median time to ILD onset was 5.4 months (range <0.1–46.8 months), with 87% of ILD events occurring within 12 months after starting T-DXd. 50 Table 2 summarizes the incidence and median time to onset of ILD in patients treated with T-DXd in DESTINY-Breast01, DESTINY-Breast02, DESTINY-Breast03, and DESTINY-Breast04 trials. Although ILD most commonly develops in the first 6–12 months of treatment with T-DXd, cases of late onset have been reported up to 2 years from the start of T-DXd, emphasizing the importance of permanent surveillance in patients on treatment with this agent. 25 In this pooled analysis, some characteristics were associated with potentially higher risk of ILD, namely age <65 years, enrollment in Japan, higher doses of T-DXd (>6.4 mg/kg), lower oxygen saturation (<95%), renal impairment (moderate/severe), lung comorbidities, and longer time since initial diagnosis (>4 years). 50 Patients should be closely monitored for signs/symptoms and radiographic changes potentially consistent with this AE as T-DXd administration must be interrupted as soon as a diagnosis of ILD (grade ⩾1) is made. 45 Guidelines recommendations for the management of ILD vary with the AE grade and include dose reductions, administration of corticosteroids, and T-DXd interruption (grade 1/asymptomatic events) or permanent discontinuation in patients who are diagnosed with symptomatic (Grade 2 or greater) ILD/pneumonitis. 45
Incidence and time to onset of interstitial lung disease in patients treated with trastuzumab deruxtecan.

ILD, interstitial lung disease.
Sacituzumab govitecan
Sacituzumab govitecan (SG) is an ADC composed of an IgG1 kappa mAb anti-trophoblast cell-surface antigen (Trop-2) bound to SN-38, the active metabolite of irinotecan (topoisomerase I inhibitor), through a hydrolyzable linker.28,51 Trop-2 is a transmembrane calcium signal transducer that is overexpressed in BC, with particularly higher expression in TNBC.52,53 In the phase III ASCENT trial, SG was compared with TPC (eribulin, vinorelbine, capecitabine, or gemcitabine) in patients with metastatic TNBC previously treated with two or more prior standard chemotherapy regimens. 28 When compared with TPC, SG improved mPFS (5.6 versus 1.7 months; HR 0.41, 95% CI 0.32–0.52) among patients without brain metastases, mOS (12.1 versus 6.7 months; HR 0.48, 95% CI 0.38–0.59), and ORR (35% versus 5%). 28
Considering the expression of Trop-2 in other BC subtypes, the activity of SG was evaluated beyond the TNBC population. In the phase III TROPiCS-02 trial, 543 patients with advanced hormone receptor-positive BC pretreated with 2–4 prior systemic therapy regimens (including one prior taxane, one CDK4/6 inhibitor, and one endocrine therapy in any setting) were randomly assigned to SG or TPC (capecitabine, eribulin, vinorelbine, or gemcitabine). Patients with active brain metastases were excluded. 29 SG improved mPFS when compared to TPC (5.5 versus 4.0 months; HR 0.66; 95% CI 0.53–0.83). 29 In the planned second interim analysis, SG also demonstrated a significant improvement in OS (14.4 versus 11.2 months, HR 0.65–0.96). 30 In SABCS 2022 the authors presented an interesting post hoc analysis showing that these improvement were observed regardless of Trop-2 expression. 54
In the ASCENT study, serious treatment-related AE were reported in 15% in the SG arm and in 8% in the TPC arm, although the rate of AE leading to drug discontinuation was similar in both arms. 28 Importantly, SG is associated with a risk of severe neutropenia and diarrhea (and possibly neutropenic colitis). The rates of grade ⩾3 treatment-related AE were the following: neutropenia (51% with SG and 33% with TPC), leukopenia (10% and 5%), diarrhea (10% and <1%), anemia (8% and 5%), and febrile neutropenia (6% and 2%). 28 In the TROPiCS-02 trial, the safety profile of SG was consistent with previous trials with the drug. 30
Incorporation of ADCs into BC clinical practice guidelines
Different ADCs have been endorsed as standard therapy for the treatment of all BC subtypes by regulatory authorities around the world. However, the positioning of these agents in treatment algorithms remains an important challenge, especially considering differences in the registration trials and the absence of data on the use of new ADCs after prior ADC exposure. Based on the available data, we propose a simplified algorithm for incorporating these agents into the management of metastatic breast cancer (Figure 3).

Incorporation of ADCs into the management of metastatic breast cancer.
For HER2-positive BC, T-DXd has become the preferred second-line therapy based on DESTINY-Breast03 data.27 T-DXd is currently approved by the FDA and EMA for patients with advanced HER2-positive BC who have received one or more prior anti-HER2-based regimens.44,56 Based on data from the TH3RESA study, T-DM1 remains a valid FDA- and EMA-approved later-line treatment option, although there are no data demonstrating its efficacy after prior T-DXd treatment. 17
For TNBC, SG is a standard clinical option for patients with pretreated disease based on the results of the ASCENT trial. 28 SG is approved by the FDA and the EMA for the treatment of patients with advanced TNBC who have received two or more prior systemic therapies, at least one of them for metastatic disease.57,58 Patients with TNBC and HER2-low disease who have been previously treated with chemotherapy for metastatic disease (or have had disease recurrence during or within 6 months after completing adjuvant chemotherapy) might also be considered for T-DXd based on DESTINY-Breast04 data.36 T-DXd is approved by the FDA and the EMA for the treatment of patients with HER2-low (TNBC or hormone receptor-positive) advanced BC who have received prior chemotherapy in the metastatic setting or developed disease recurrence during or within 6 months of completing adjuvant chemotherapy.44,59
Finally, patients with hormone receptor-positive disease who have previously received 2–4 lines of systemic therapy (including one prior taxane, one CDK4/6 inhibitor, and one endocrine therapy in any setting) should be considered for SG based on the results of the TROPiCS-02 trial. 30 SG is approved by the FDA for the treatment of patients with advanced hormone receptor-positive (HER2-zero or HER2-low) BC who have received endocrine-based therapy and at least two additional systemic therapies in the metastatic setting. 60 T-DXd might also be considered as a treatment option for patients with hormone receptor-positive and HER2-low BC, who have previously received at least one line of endocrine therapy and one line of chemotherapy based on the results of DESTINY-Breast04. 25 There are no head-to-head comparative data in these two agents in patients with HER2-low disease. Therefore, toxicity profile and patients’ preferences should be considered in the decision-making process.
For patients with brain metastases (BM), the subgroup analysis of patients with stable BM at baseline in DESTINY-Breast03, confirms benefit in PFS of T-DXd (HR 0.38, 95% CI 0.23–0.64), 23 position this drug as a second-line therapies option after THP also in case of stable central nervous system (CNS) involvement. 27 Of particular interest, the activity of T-DXd in patients with active BM was not evaluated in DESTINY-Breast03 trial because only patients with stable BM were included in the study. 23 The TUXEDO trial was a phase II, single-arm study assessing the activity of T-DXd in patients with HER2-positive aBC after exposure to trastuzumab and pertuzumab and with BM that were previously untreated or progressing after previous local therapy. 27 In this trial, the intracranial ORR was 73.3% (95% CI 48.1–89.1). 27 Although limited by the small sample size (15 patients) and absence of comparator arm, these data demonstrate the CNS activity of T-DXd and suggest a potential role of T-DXd also in patients with active central nervous system metastases.
HER2-targeted ADCs in clinical development for the treatment of BC
Building on the success achieved with T-DM1 and T-DXd, HER2 is currently the most intensively studied ADC target in BC, setting an extremely dynamic drug development environment. In this highly competitive field, several strategies are being explored, including innovations in the structure and components of ADCs, often with the aim of achieving tumor responses not only in HER2-positive tumors, but also in the highly prevalent HER2-low population, in which T-DXd has demonstrated unprecedented benefits. Table 3 summarizes the characteristics, efficacy, and safety profile of HER2-targeted ADCs in clinical development for the treatment of BC (non-exhaustive list).
HER2-targeted ADCs in clinical development for the treatment of breast cancer (non-exhaustive list).

aBC, advanced breast cancer; ADC, antibody–drug conjugate; AE, adverse event; ALT, alanine aminotransferase; AST: aspartate aminotransferase; CI, confidence interval; DAR, drug-to-antibody ratio; DCR, disease control rate; F; HR, hazard ratio; ILD, interstitial lung disease; mAB, monoclonal antibody; mPFS, median progression-free survival; mOS, median overall survival; NR, not reported; MMAE, Monomethyl auristatin E; MMAF, Monomethyl auristatin; ORR, objective response rate.
Trastuzumab duocarmazine is a novel HER2-targeted ADC that, although not yet approved, is in a more advanced stage of development. This agent, also known as SYD985 is an anti-HER2 ADC consisting of trastuzumab, a cleavable linker, and a duocarmycin (vc-seco-DUBA) payload. 61 In the phase I trial, 39 patients with different tumor types (including 26 with BC, among which 17 were HER2-positive) with at least 1 + HER2 expression assessed by immunohistochemistry were enrolled in the dose-escalation phase and 146 patients (50 with HER2-positive and 49 with HER2-low BC) were enrolled in the dose-expansion phase. ORR was 33% (95% CI 20.4–48.4) in patients with HER2-positive BC, 28% (13.8–46.8) in HER2-low, hormone-receptor positive, and 40% (16.3–67.6) in HER2-low hormone-receptor negative BC. 61 In the phase III TULIP study, 437 patients with advanced HER2-positive disease, pretreated with two or more lines of therapy were randomly assigned in a 2:1 ratio to receive SYD985 or TPC. 62 Median PFS was 7.0 months in the SYD985 arm and 4.9 months in the TPC arm (HR 0.64, 95% CI 0.49–0.84, p = 0.002). At the first interim analysis, no significant difference was seen between the two arms in terms of mOS (20.4 versus 16.3 months, HR 0.83, 95% CI 0.62–1.09, p = 0.153). 62 The most common AE of any-grade reported in the TULIP trial were conjunctivitis (38.2%), keratitis (38.2%), and fatigue (33.3%), with 52.8% of patients treated with SYD985, experiencing grade ⩾3 AE. 62 Notably, to mitigate the eye toxicity risk, patients with prior keratitis were excluded, lubricating eye drops were administered prophylactically, eye examinations were regularly performed by an ophthalmologist. Nevertheless, eye toxicity remains the most common AE in this trial, reported by 78.1% of patients with 21.2% of grade ⩾3, requiring dose reductions in 22.9% and drug discontinuation in 20.8% of cases. The incidence of ILD was 7.6% (22 patients), with 2.4% (7 patients) being of grade ⩾3 and 0.7% (2 patients) of grade 5. This AE led to treatment discontinuation in 5.2% of cases, despite the exclusion of patients with history of pneumonitis and the implementation of a full diagnostic workup for new or worsening respiratory symptoms. 62 SYD985 license application is currently under review by regulatory authorities.
In terms of their structure (Table 3), most anti-HER2 ADCs in earlier stages of development for BC treatment are composed of: (1) a HER2-targeted mAB, which can be either trastuzumab (or a variation) or a novel mAB targeting one or more HER2 subdomains (e.g. bispecific mABs targeting subdomains 2 and 4 of HER2); (2) a cleavable linker (with the exception of ARX788), 67 (3) a payload more commonly belonging to the class of microtubule inhibitors, with DAR ranging from 2 to 12 molecules of payload per mAB. Among the innovations explored in these new compounds we can mention the wide incorporation of cleavable linkers and innovative bispecific mABs targeting two epitopes in subdomains 2 and 4 of the HER2 receptor, which results in crosslinking followed by internalization of the complex and release of the payload after the cleavage of the linker. 75
Although cross-trial comparisons are not possible considering the heterogeneity of study designs and the different populations included in each study, ORR ranging from 13% to as high as 75% were observed with these agents. In terms of their safety profiles, hematological AEs (including low- and high-grade events) are among the most common incident toxicities observed with several of these agents, which is probably related to the payloads’ mechanisms of action.65,68,76 Importantly, the safety profiles of each of these agents should be closely monitored as some patients might experience high grade (or fatal AEs) and also because the toxicity of these agents is not easily predictable based on the ADC’s structure. For instance, some important toxicities of the new ADCs were not commonly observed either with T-DM1 or other HER2-targeted agents, namely ocular toxicities, an important class of AEs observed with trastuzumab duocarmazine, A166, ARX788, and other agents.62,63,68
Beyond HER2: investigational ADCs exploring other targets for the treatment of BC
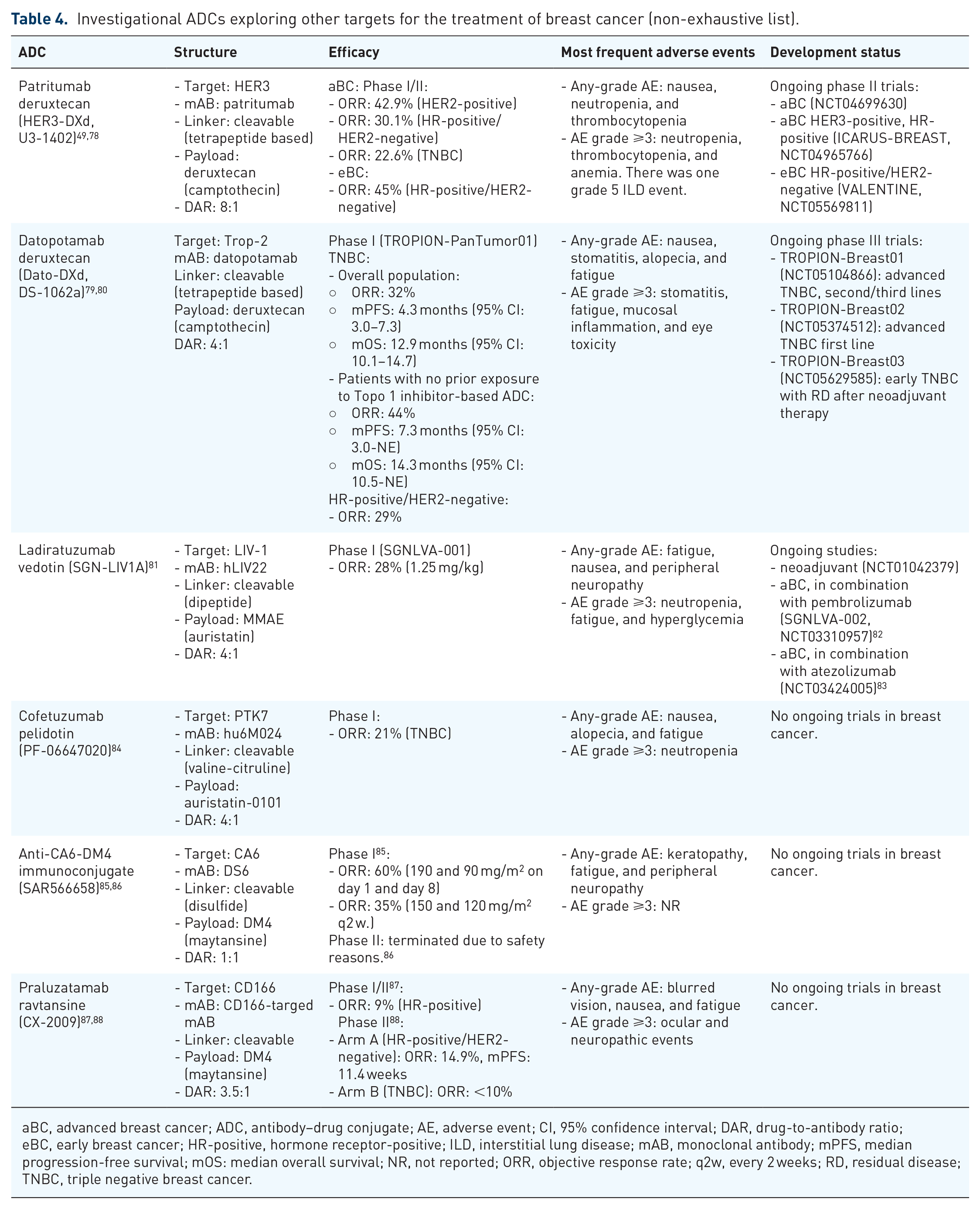
Although considerable research efforts have been employed in the search for new therapeutic targets in the last decades, it was only with the approval of SG for the treatment of TNBC in 2021 that an ADC targeting a non-HER2 target was incorporated into clinical practice. 28 The benefit demonstrated with this anti-Trop-2 agent proved the concepts that a new generation of ADC could effectively target proteins that are highly expressed in tumors, even if they are not part of hyperactivated oncogenic driver pathways. These findings further boosted the development of ADC targeting new targets, many of which with promising initial results in all BC subtypes. Table 4 summarizes data from ADCs exploring other (non-HER2) targets for the treatment of BC, several of which use antimicrotubule payloads and cleavable linkers with variable DAR.
Investigational ADCs exploring other targets for the treatment of breast cancer (non-exhaustive list).
aBC, advanced breast cancer; ADC, antibody–drug conjugate; AE, adverse event; CI, 95% confidence interval; DAR, drug-to-antibody ratio; eBC, early breast cancer; HR-positive, hormone receptor-positive; ILD, interstitial lung disease; mAB, monoclonal antibody; mPFS, median progression-free survival; mOS: median overall survival; NR, not reported; ORR, objective response rate; q2w, every 2 weeks; RD, residual disease; TNBC, triple negative breast cancer.
Datopotamab deruxtecan (Dato-DXd, DS-1062a) is another Trop-2 targeted ADC composed of a human IgG1 mAb that is enzymatically conjugated by a cleavable tetrapeptide-based linker with a topoisomerase I inhibitor (DXd) payload. 89 Relying on the high expression of Trop-2 in epithelial carcinomas and in the high potency of the payload (DXd), the activity of Dato-DXd was evaluated in patients with BC. In the BC cohort of the phase I TROPION-PanTumor01 study, including 43 patients with pretreated advanced TNBC the ORR was 39% (and 52% among those not previously treated with SG, another topoisomerase 1 inhibitor-based ADC). 90 The rates of AE of any grade and grade ⩾3 were 95% and 35%, respectively. The most commonly reported AE were nausea (58%), stomatitis (53%), alopecia (35%), vomiting (35%), and fatigue (33%). 90 The ongoing phase III TROPION-Breast01 (NCT05104866) and TROPION-Breast02 (NCT05374512) will assess the activity of this agent in patients with pretreated and treatment-naïve metastatic TNBC, respectively.
In addition to HER2, other members of the human epidermal growth factor (EGFR/HER) family have been explored as novel ADC targets. HER3 is a membrane receptor with little intrinsic tyrosine kinase activity, that commonly participates in the activation of oncogenic signaling via PI3K/Akt pathway and Src kinase by the formation of heterodimers with other receptor tyrosine kinases, including HER2.91,92 Patritumab deruxtecan (HER3-DXd, U3-1402) is a HER3-directed ADC comprising a fully human anti-HER3 immunoglobulin G1 (IgG1) mAb linked to a topoisomerase I inhibitor payload (deruxtecan) via a tetrapeptide-based cleavable linker. 91 U31402-A-J101 was a phase I/II, first-in-human study of HER3-DXd in patients with HER3-expressing aBC. The ORR in the HER2-positive (n = 14) and hormone receptor-positive (n = 113) disease and TNBC (n = 53) were 42.9%, 30.1%, and 22.6%, respectively. 49 The rate of grade ⩾3 AEs was 71.4%, with the most common being neutropenia (39.6%), thrombocytopenia (30.8%), anemia (18.7%), and leukopenia (18.1%). Importantly, the rate of treatment-related ILD was 6.6%, including one grade 5 event. 49 The activity of HER3-DXd was also evaluated in the early setting. SOLTI TOT-HER3 study enrolled patients with untreated hormone receptor-positive/HER2-negative operable (⩾1 cm) BC (divided in four cohorts with different levels of ERBB3 mRNA expression) to receive a single dose of HER3-DXd. The ORR was 45% among the 77 evaluable patients. 78 Ongoing studies (NCT04965766, NCT04699630) will provide additional data about the efficacy and safety of this agent.
Interestingly, updated results from the phase Ib/II BEGONIA trial presented at SABCS 2022 showed that patients with advanced TNBC treated with the combination of Dato-DXd with durvalumab (anti-PD-L1) as first-line therapy had an ORR of 79% (95% CI: 61–91) with 2/33 patients (6%) having a complete response and 24/33 (73%), a partial response. 93 Although preliminary, these data suggest the potential benefit of combining ADCs with immune checkpoint inhibitors, a strategy also being tested with other agents. Ladiratuzumab vedotin (SGN-LIV1A) is an LIV-1 directed ADC composed of mAb targeting LIV-1, a protease-cleavable dipeptide linker, and a microtubule polymerization inhibitor payload (MMAE). 94 LIV-1 is a transmembrane protein with metalloproteinase activity and downstream target of STAT3 that is expressed in a moderate/high level in the majority of BCs.95,96 Ongoing studies are investigating the combination of this agent with other pembrolizumab (NCT03310957) and atezolizumab (NCT03424005).
Predictive biomarkers for ADCs
With an increasing number of agents demonstrating clinical efficacy, predictive biomarkers will be an essential part of the incorporation of these new agents into clinical practice. As of now, HER2 expression is the only biomarker available for patient selection, although the demonstration of the activity of some ADCs in patients with low HER2 expression represented a complete paradigm shift which will require further and in-depth exploration.
T-DM1 antitumor activity is closely related with HER2 expression. The efficacy of this agent was evaluated in patients who did not fulfill traditional HER2 positivity criteria (IHC +3 or ISH positive) in a centralized reanalysis of HER2 status in patients enrolled in a phase II trial with T-DM1. In this population, the activity associated with T-DM1 was significantly limited (ORR of 4.8% and median PFS of 2.6 months). 41 Evidence suggesting a correlation between the levels (and homogeneity) of HER2 expression and the response to T-DM1 is also available in the early setting. In the neoadjuvant KRISTINE study, locoregional progression was more frequent in the T-DM1 than in the trastuzumab, pertuzumab, and chemotherapy arm (7% versus <1%, respectively), and the majority (66%) of patients progressing under T-DM1 were IHC + 2 with ISH amplified. 97 Additionally, in a neoadjuvant study including patients with HER2-positive disease receiving T-DM1 plus pertuzumab, no pathologically complete response occurred in patients with heterogeneous HER2 expression. Notably, 75% of these cases were IHC2+ with ISH amplified. 98
Although T-DXd improved clinical outcomes of patients with HER2-positive and HER2-low disease, the activity of this agent also correlates with HER2 expression levels.23,25,26 The relationship between different levels of HER2 expression and the efficacy of T-DXd was prospectively explored in DAISY trial. In this phase II study, patients with aBC pretreated with at least one chemotherapy regimen in the advanced setting were divided in three cohorts: (1) IHC 3+ or IHC 2+ with ISH amplified, (2) IHC 2 + and ISH not amplified or IHC1+, and (3) IHC 0. The ORR to T-DXd according to HER2 expression were 71, 37.5, and 30%, respectively (p < 0.0001) and the median PFS were 11.1, 6.7, and 4.2 months, respectively (p < 0.0001), suggesting a correlation between HER2 expression and response to this agent. 26 Moreover, nonresponse to T-DXd was correlated with a high percentage of HER2-zero cells and their spatial distribution (wide areas of HER2-zero cells distant to HER2 3+ cells). 26 In this study, no driver alterations in baseline biopsies were associated with primary resistance to T-DXd. A higher frequency of mutations in the DNA repair gene SLX4 were identified in biopsies performed at resistance (20%, 4/20 patients) than at baseline (2%, 2/88 patients), suggesting that this gene may be implicated in secondary resistance to T-DXd. Interestingly, 13 out of 20 (65%, 95% CI: 40.8–84.6) patients had a decrease in the baseline HER2 expression at the time of progression on T-DXd. Similarly, trastuzumab duocarmazine not only showed activity in HER2-positive BC, but also in HER2-low disease, with an ORR of 32% and a median PFS of 4 months in the metastatic setting. 61 Among 48 patients with HER2-low BC treated with RC48, ORR was 40% and median PFS was 5.7 months. 65 Based on these results, an ongoing phase III study is currently testing RC48 in patients with metastatic HER2-low BC (NCT04400695). The ongoing DESTINY-Breast06 (NCT04494425) will assess the efficacy of T-DXd compared with TPC in patients with HER2-low aBC, including those with ultralow expression (IHC 0+). A particularly important challenge in this setting is the limitation of current immunohistochemistry assays to differentiate HER2-low from HER2-zero, as they were not designed for this purpose. 99
Considering the variety of agents with activity demonstrated for the treatment of HER2-positive aBC,100,101 the identification of predictive biomarkers will be a key factor to guide optimal treatment sequencing. Importantly, under the pressure of HER2-targeted agents, HER2 expression levels may vary during the disease course, with some primary HER2-positive tumors relapsing as HER2-negative or HER2-low, and conversely.102,103 Thus, it can be hypothesized that the levels of HER2 expression and its distribution among different metastatic foci may be significantly modified by the prior treatment with HER2-targeted ADCs, which could possibly impact the efficacy of subsequent therapies. Molecular imaging has been successfully used to explore intra-/interpatient heterogeneity in HER2 mapping of metastatic disease and to identify patients unlikely to benefit from HER2-targeted agents. In the ZEPHIR trial, the patterns of HER2 radio-labeled tracer uptake assessed by HER2-positron emission tomography (PET-CT) with 82 Zr-trastuzumab have been shown to be a promising strategy for understanding tumor heterogeneity in aBC and for selecting patients who will/will not benefit from T-DM1-based therapy. 104
Beyond the levels of HER2 expression, the presence of HER2-mutations appears to be a relevant predictor of ADC efficacy. Interestingly, preclinical data suggest that, regardless of the presence of HER2 overexpression, ubiquitination, and internalization of the receptor are the main mechanisms driving endocytosis and subsequent antitumor activity of anti-HER2 ADCs. 105 Thus, HER2 mutations that increase the rate of receptor internalization and trafficking may induce responses upon exposure to ADCs, regardless of their intrinsic dependence on HER2 signaling for cell growth and/or survival. 105 These findings are supported by clinical data demonstrating high ORR from T-DM1 and T-DXd in HER2-mutated metastatic NSCLC (ORR 44% and 55%, respectively).106,107 Interestingly, in hormone receptor-positive disease (but not in TNBC), ERBB2 and luminal-related genes are more expressed in HER2-low than HER2 IHC 0. 38 Ongoing studies are assessing the efficacy of T-DXd in patients with HER2-mutated solid tumors, including BC (NCT04639219).
Finally, the accumulated evidence suggest that the benefit derived from SG is observed regardless of the levels of Trop-2 expression in hormone receptor-positive and TNBC and the assessment of this biomarker is currently not recommended for patient selection.54,108 Thus, the clinically significant activity of T-DXd and SG in patients with low expressions of HER2 and Trop-2 demonstrate that IHC should not be the only biomarker for treatment selection.
Conclusions and future perspectives
BC is a markedly heterogeneous disease, a characteristic intrinsically related to resistance to cytotoxic agents and traditional targeted therapy. ADCs are a class of potent anticancer agents characterized by a smart form of targeted drug delivery that have demonstrated unprecedented efficacy in the treatment of early and advanced BC and have challenged paradigms by demonstrating efficacy in populations with low expression of target antigens. 25
Despite all the progress achieved, several challenges still remain to be overcome. There is still a long way to improve efficacy, better prevention, and management AEs, and increase understanding of biomarkers and resistance mechanisms (payload- vs target-driven). Some of these hurdles may be overcome by ongoing studies exploring (1) new therapeutic targets (e.g. EGFR, RON, EpCAM); (2) bispecific ADCs, inhibiting multiple pathways or modulating the interface between tumor and immune cells; (3) dual-payload ADCs; and (4) potential synergistic interactions between ADCs and other agents such as immune checkpoint inhibitors.82,83,109–112 If future research in this field continues properly addressing these important questions, ADCs could potentially replace cytotoxic and traditional targeted agents as the preferred therapeutic strategy for treatment of BC.