
Abstract
Background:
Results from DESTINY-Breast04 trial revealed that trastuzumab deruxtecan (T-DXd) improved both progression-free survival and overall survival for patients with human epidermal growth factor receptor 2 (HER2)-low metastatic breast cancer (mBC). However, the economic impact of this practice remains unclear. The purpose of this study was to evaluate the cost-effectiveness of T-DXd on HER2-low mBC from the viewpoint of U.S. payers.
Methods:
Using the clinical data from the DESTINY-Breast04 trial, a three-state Markov model was created to assess the economic and health effects of T-DXd versus chemotherapy. The incremental cost-effectiveness ratio (ICER) and willingness-to-pay threshold were determined and compared. One-way and probabilistic sensitivity analysis were used to measure parameter uncertainty.
Results:
In the overall HER2-low population, T-DXd provided additional 0.47 quality-adjusted life-years (QALYs) at an increased cost of $149,222 compared with chemotherapy, yielding an ICER of $317,494/QALY. The ICER was $353,903/QALY in the hormone receptor (HR)-positive subgroup, which decreased to $259,825/QALY in the HR-negative subgroup. The sensitivity analysis found that T-DXd would not be cost-effective in the base-case. The expected cost of T-DXd will be less than $4,281/cycle ($11.33/mg) or $1,903/cycle ($5.03/mg) to achieve a 50 or 90% cost–benefit probability, respectively.
Conclusions:
T-DXd provides significant health benefit for patients with HER2-low mBC compared with chemotherapy but is unlikely to be cost-effective in the United States.
Keywords
Introduction
Breast cancer (BC) is the most diagnosed malignancy and the leading cause of cancer-related deaths among women both in the United States and across the globe, with 287,850 new cases and 43,250 deaths estimated in 2022. 1 Approximately 80–85% of those new cases were previously considered to be human epidermal growth factor receptor 2 (HER2)-negative subtype, including hormone receptor (HR)-positive and triple negative breast cancer (TNBC). 2 However, approximately 45–55% of tumors previously reported as HER2-negative subtype can now be considered as HER2-low expression, with an immunohistochemistry (IHC) 1+ or 2+ with negative in situ hybridization. 3 Due to the low level of HER2 protein on the cancer cell surface, conventional HER2-directed therapies have not improved clinical outcomes in patients with HER2-low.4–8 Therefore, HER2-low BC is treated as HER2-negative.
For HR-positive HER2-negative advanced or metastatic BC (mBC), endocrine therapy (ET) combined with cyclin-dependent kinase (CDK) 4/6 inhibitor is the preferred option.9,10 On progression, the treatment is usually selected based on the patient’s previous treatment, tumor load, and biomarkers. ET combined with targeted therapy or chemotherapy can be considered as the second- or later-line therapy. For advanced or metastatic TNBC, pembrolizumab combined with chemotherapy is recommended as first-line therapy for patients with programmed cell death-ligand 1 (PD-L1) combined positive score (CPS) ⩾ 10. 11 Patients with germline breast cancer susceptibility gene 1/2 (BRCA 1/2) mutation can be treated with platinum or polyadenosine diphosphate-ribose polymerase inhibitors. Sacituzumab govitecan (SG) is one of the recommended options in the second or later line in the metastatic setting according to the ASCENT trial. 9 In the case of PD-L1–negative, no germline BRCA 1/2 mutation TNBC, or in later-line settings, systemic chemotherapy is the standard of care, which has poor response rates and limited progression-free survival (PFS).12–14 Recent findings from randomized phase III DESTINY-Breast04 trial have challenged this paradigm, opening the door to a new therapeutic option for the large subset of patients with HER2-low disease. 15
Trastuzumab deruxtecan, also known as T-DXd or DS-8201a, is a new HER2-targeted antibody-drug conjugate (ADC) with a cytotoxic drug payload. 16 T-DXd was granted approval by the U.S. Food and Drug Administration for the treatment of patients with unresectable or metastatic HER2-low BC based on the data from the DESTINY-Breast04 (NCT03734029) trail. 17 In this randomized, multicenter clinical trial, T-DXd successfully prolonged both PFS and overall survival (OS) in patients with HER2-low unresectable and/or mBC who had been heavily pretreated, compared to the standard single-agent chemotherapy chosen by the physicians. 15 Based on 18.4 months of median follow-up, T-DXd reduced the risk of disease progression or death by approximately 50% (median PFS: 9.9 versus 5.1 months; hazard ratio [HR] 0.50, p < 0.0001), and the risk of death by 36% (median OS: 23.4 versus 16.8 months; HR 0.64, p = 0.001) among all patients, regardless of HR status. In addition, the chemotherapy group had a higher incidence of adverse events (AEs) of grade 3 or higher than the T-DXd group (67.4 versus 52.6%). In light of these results, T-DXd may become the standard therapy for HER2-low mBC with limited alternative options. Furthermore, T-DXd was recommended as the preferable therapy for patients with unresectable or metastatic HER2-low BC who have received a prior chemotherapy in metastatic setting, and if HR-positive are refractory to ET in updated guidelines.9,10,18
T-DXd has shown great efficacy and safety, but it is costly. Attention should be paid to the huge cost burden of patients and the healthcare system. Evaluating the cost-effectiveness of novel therapy has become crucial for providing policymakers, providers, and patients with reliable evidence regarding the value of implementing new therapeutic interventions. The current study was designed to investigate the economic outcomes of T-DXd compared with chemotherapy in previously treated HER2-low mBC from the U.S. payers’ perspective.
Materials and methods
Population and intervention
The population in our model was similar to those in the DESTINY-Breast04 clinical trial: patients had HER2-low, unresectable, or mBC (regardless of HR status); and had received 1–2 prior lines of chemotherapy (Supplemental Table 1). 15 Patients were randomly assigned in a 2:1 ratio to receive either T-DXd or single-agent chemotherapy (Figure 1), including eribulin (51.1%), capecitabine (20.1%), gemcitabine (10.3%), nab-paclitaxel (10.3%), or paclitaxel (8.2%). 15 Patients were followed up by whole blood count, liver and kidney function, SpO2, and alkaline phosphatase, chest computed tomography (CT), abdominal CT/magnetic resonance imaging (MRI), brain MRI, bone scan, and test for any additional newly suspected sites of progression every 6 weeks during the treatment and every 3 months from the date of follow-up visit until death.

Markov model simulating the results of the DESTINY-Breast04 clinical trial. The three health states are associated with transitional variables. During each 3-week cycle, patients either remained in their assigned health state or progressed to a new health state.
Model construction
TreeAge Pro 2018 software (TreeAge Software, Williamstown, MA) was used to build a comprehensive Markov model (Supplemental Figure 1). As shown in Figure 1, three health states were identified in the development of HER2-low mBC: PFS (initial state), progressive disease (PD state), and death (absorbing state). In the PFS state, all patients continued with their therapies until disease progression, intolerable AEs, or death. In the PD state, all patients were presumed to receive salvage chemotherapy and best supportive care (BSC) until death due to the lack of treatment data in the sequence line based on the DESTINY-Breast04 trial. We used a cycle duration of 21 days in our model, matching the cycle of T-DXd and chemotherapy in the trial. 15 During each cycle, patients were assigned to one of three health states depending on their transition probabilities. The model was run using a 10-year time horizon, after which all patients moved to the absorbing state.
The total mean costs, life-years (LYs), quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratios (ICERs) were the key outcomes of this study. For cost and survival estimations, a 3% annual discount rate was used.
19
The ICERs were compared to a willingness-to-pay (WTP) threshold of $150,000/QALY.20–22 Additionally, the incremental monetary benefit (INMB) and incremental net-health benefit (INHB) were calculated using the following formulas:
Model survival and transition probabilities
The survival data in the model came from the survival curves of the DESTINY-Breast04 trial. Due to the short follow-up intervals in clinical trials, it is commonly essential to conduct parameter distribution fitting on the survival curve to acquire the long-term survival data on patients beyond the follow-up period of clinical trials.
24
We used GetData Graph Digitizer software (version 2.26) to extract data points from the PFS and OS Kaplan-Meier curves of T-DXd and chemotherapy.
25
Then, these data were used to fit parametric survival models, including the log-logistic, exponential, log-normal, Gompertz, and Weibull models (Supplemental Figures 2–4).
26
Finally, log-logistic and Weibull distributions were found to be the most appropriate functions for extrapolating the OS and PFS curves because they provided the best fit for curves according to the clinical rationality, visual inspection, Akaike information criterion, and Bayesian’s information criterion (Supplemental Tables 2 and 3).
27
The time-dependent transition probabilities for each cycle were calculated using following formulas:
Model parameters for PFS and OS.

HER2, human epidermal growth factor receptor 2; HR, hormone receptor; OS, overall survival; PFS, progression-free survival; SE, standard error; T-DXd, trastuzumab deruxtecan.
Cost and utility
Only the direct medical expenditures were taken into consideration, including drug costs, treatment cost for serious AEs,29–31 regular follow-up and monitoring, 32 drug administration cost, 33 salvage chemotherapy, BSC, and the end-of-life care (Table 2). 20 The price of each drug was obtained from the July 2022 Average Sales Price Drug Pricing File provided by the Centers for Medicare and Medicaid Services. 34 The medication doses were calculated by using the mean body surface area 1.79 m2, weight 70.0 kg. 35 Supplemental Table 4 provides information on the drug doses and unit cost in detail. In additional, drug-related interstitial lung disease (ILD)/pneumonia is a recognized risk associated with T-DXd. The administration of T-DXd must be interrupted for ILD/pneumonitis events regardless of grade. Therefore, we included the cost of management of ILD/pneumonitis related to T-DXd. Besides, we included grade 3–4 AEs that affected more than 5% of patients (neutropenia, leukopenia, anemia, thrombocytopenia, fatigue, and increased aminotransferase levels), whereas we considered grade 1–2 AEs were to be manageable with routine patient-monitoring. The cost of AEs was estimated by multiplying the per-event costs of treating the AE by the incidence rates of each AE.29,30
Model parameters used in the sensitivity analysis.
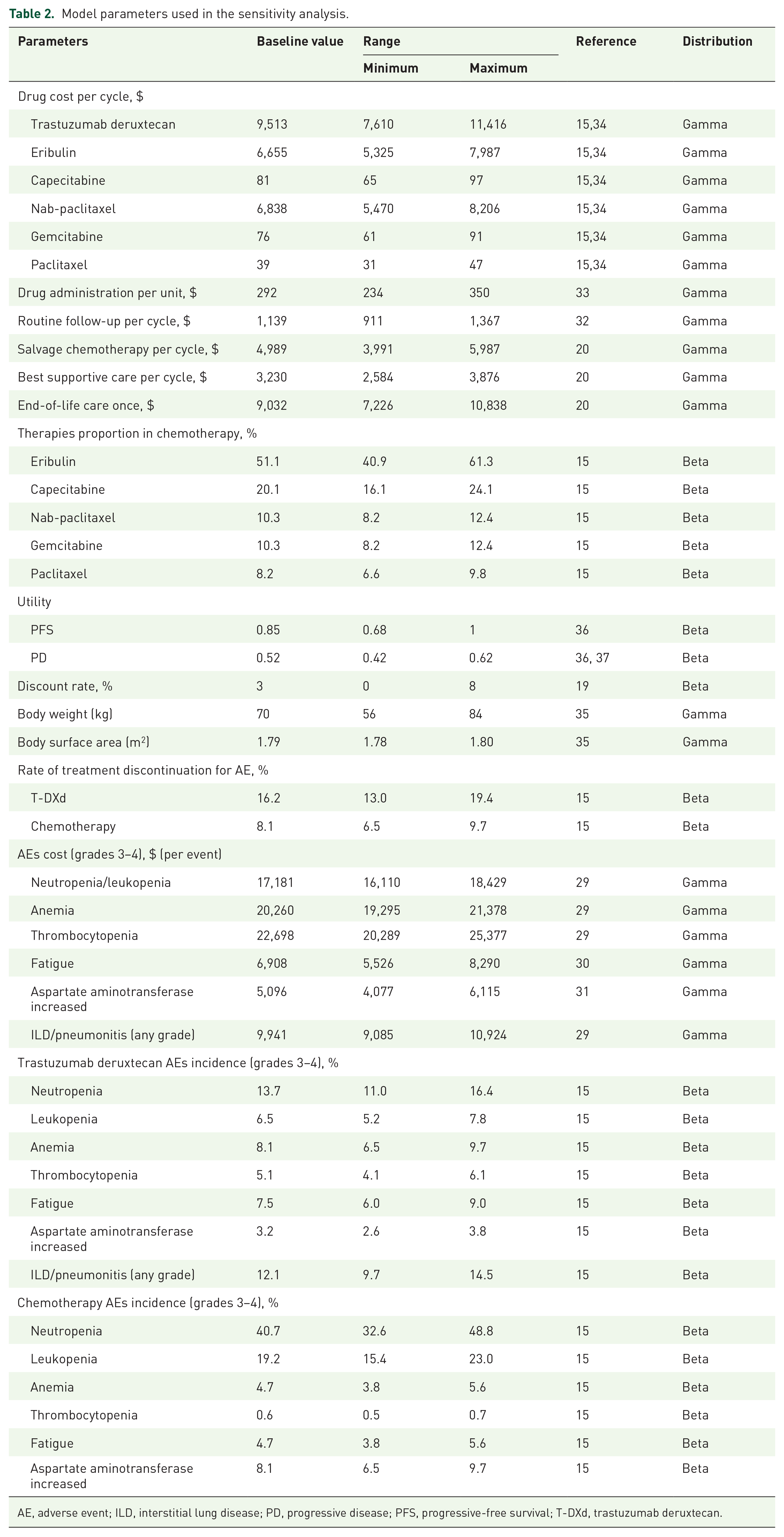
AE, adverse event; ILD, interstitial lung disease; PD, progressive disease; PFS, progressive-free survival; T-DXd, trastuzumab deruxtecan.
Each Markov health state was assigned a health utility preference between 0 and 1, where 0 represents death and 1 represents perfect health. Because the DESTINY-Breast04 trial did not disclose quality-of-life data, utility values were determined from previous research on advanced HER2-negative BC.20,36,37 For patients in the PFS state, we assigned a utility value of 0.85, whereas for those in the PD state, we assigned a value of 0.52.
Sensitivity analysis
The robustness of the model and the impact of variable uncertainty on the outcomes were assessed using sensitivity analysis. One-way sensitivity analysis was carried out for all parameters with changes within a ±20% range from their baseline values based on the recognized methods for estimating the impact of uncertainty on the ICER.22,35 Monte Carlo simulations were used for the probabilistic sensitivity analysis (PSA), which were performed to generate 10,000 repeated results based on a random selection of the key model parameters. 38 We adopted a gamma distribution for the costs and a beta distribution for the incidence of AEs and all utilities according to the recommendation, respectively. 39 Tornado diagrams, acceptability curves, and scatter plots were implied to show the findings of sensitivity analysis. This cost-effectiveness analysis was presented in accordance with the CHEERS 2022 report list. 40
Results
Base-case results
The results of the base-case analysis comparing the T-DXd with chemotherapy are presented in Table 3. In the overall patients with HER2-low mBC, T-DXd was associated with an additional 0.47 QALYs and 0.68 overall LYs (8.2 months) at a higher cost of $149,222, leading to an ICER of $317,494/QALY ($219,444/LY). The INMB and INHB were −$78,722 and −0.52 QALYs, respectively, at a WTP of $150,000/QALY.
Summary of base-case and sensitivity analysis.

HR, hormone receptor; ICER, incremental cost-effectiveness ratio; INHB, incremental net-health benefit; INMB, incremental net monetary benefit; PD, progressive disease; PFS, progression-free survival; QALY, quality-adjusted life-year; T-DXd, trastuzumab deruxtecan; WTP, willingness-to-pay.
In the HR-positive HER2-low subgroup, T-DXd was estimated to provide an additional 0.34 QALYs and 0.42 overall LYs relative to chemotherapy. The incremental cost of T-DXd was $120,327, resulting in an ICER of $353,903/QALY for T-DXd versus chemotherapy. In the HR-negative HER2-low subgroup, T-DXd provided additional 0.75 QALYs (1.19 LYs) with an additional cost of $194,869, resulting in an ICER of $259,825/QALY. Both ICERs were substantially higher than the WTP threshold. Also, T-DXd was associated with negative INMB and INHB in both HR-positive and HR-negative patients (Table 3).
Sensitivity analysis
As shown by the tornado diagram from the one-way sensitivity analysis (Figure 2), the cost of T-DXd and average body weight had significant influence on the results. Decreasing the cost of T-DXd per cycle to $7,610 decreased the ICER to $257,792/QALY while increasing it to $11,416 resulted in the ICER increasing to $378,295/QALY. As we varied the body weight of patients between its lower and upper bounds, the ICERs remained greater than the WTP threshold. In addition, the ICERs were also affected by the utility of PFS and PD, the cost of chemotherapy, and the cost of eribulin in the PFS state. However, regardless of how the parameters changed in our model based on practical situation, the results remained unchanged.

Tornado diagram of one-way sensitivity analysis. The light green bar represents the lower bound and dark green bar represents the upper bound for each variable.
A PSA-based cost-effectiveness acceptability curve demonstrated that chemotherapy was preferable to T-DXd for HER2-low patients at current drug price, independent of the HR status. Reducing the cost of T-DXd by 40, 55, and 80% would result in ICERs of $197,223/QALY, $150,421/QALY, and $76,955/QALY, with 24.9, 51.3, and 91.9% chance of T-DXd being the optimal strategy at a threshold of $150,000/QALY, respectively (Table 3 and Figure 3). Therefore, without a substantial decrease in the cost of T-DXd, the chemotherapy might be the optimal therapeutic option for patients with HER2-low mBC at present.

Probabilistic sensitivity analysis. (a) Cost-effectiveness acceptable curves show the cost-effective probabilities of T-DXd at different WTP thresholds. The dark dotted lines represent the WTP thresholds. (b) Scatterplot of 10,000 Monte Carlo simulations shows low probability of cost-effectiveness.
Discussion
Based on the result of the DESTINY-Breast04 clinical trial, T-DXd provides a new treatment option for HER2-low BC, and even challenges the traditional classification and treatment pattern of BC. In the United States, national healthcare expenditure for BC treatment was estimated at $16.50 billion in 2010, and it was projected to rise to $20.50–$25.64 billion in 2020. 41 The incidence of mBC in the United States now is 7.2 per 100,000 population at risk, and 45–55% of patients are characterized by low HER2 expression. 42 In light of the huge demand for treatment of HER2-low BC and a growing interest in the economic assessment of medicinal therapies, the requirement for precise economic evaluation of T-DXd usage in this clinical setting has prompted research.
This study compared the cost-effectiveness of T-DXd with the physician’s choice of chemotherapy in patients with HER2-low mBC. T-DXd was not considered to be cost-effective in comparison to chemotherapy, with an ICER of $317,494/QALY. The ICER values were $353,903/QALY and $259,825/QALY in HR-positive and HR-negative subgroups, respectively. The sensitivity analysis demonstrated that T-DXd might become a favorable therapeutic option for patients with HER2-low disease with a drop in the price.
The subgroup analysis suggested that treatment with T-DXd was more likely to be cost-effective for patients with the HR-negative HER2-low mBC, who have a poor prognosis due to a typically aggressive phenotype and the absence of targeted therapy and ET. In this subgroup, treatment with T-DXd was associated with an additional 1.19 LYs and 0.75 QALYs, respectively, which were higher than those in the overall HER2-low patients and HR-positive subgroup. The ICER decreased to $259,825/QALY relative to $317,494/QALY for the overall population, which suggested that T-DXd may bring a significant benefit to patients with HR-negative HER2-low. In the HR-positive subgroup, the increased cost of obtaining an additional QALY increased to $353,903, which is mainly due to the more obvious survival benefit in HR-positive patients receiving chemotherapy, thus, reducing the difference of overall LYs gained and QALYs gained. Therefore, screening more suitable patients would make T-DXd more likely to be cost-effective from a more prospective perspective.
One recent cost-effectiveness analysis has analyzed the cost-effectiveness of T-DXd in HER2-positive mBC, which reported an ICER of $220,533/QALY for patients treated with T-DXd relative to T-DM1 in the United States. 43 An analysis evaluated the cost-effectiveness of another novel ADC SG for metastastic TNBC. 44 In this study, patients treated with SG versus chemotherapy were associated with an ICER of $494,479/QALY in the United States. Another study by Le et al. 45 reported that the ICERs comparing T-DM1 to lapatinib plus capecitabine was $183,828/QALY and comparing T-DM1 to capecitabine was $126,001/QALY. Not only the ADCs, other drugs for advanced BC, such as CDK 4/6 and PD-1/L1 inhibitors, are also not cost-effective because of extremely high incremental costs and limited incremental QALYs. A previous study reported the ICERs of $634,000/QALY and $440,000/QALY for patients with HR-positive and HER2-negative BC treated with palbociclib and ribociclib, respectively. 36 Another study explored the cost-effectiveness of atezolizumab and nab-paclitaxel as first-line treatment for TNBC and reported ICERs of $106,339.26/QALY and $331,996.89/QALY in China and in the United States, respectively. 46 All the results showed that the new and expensive drugs led to uneconomical results, which was similar to our data. However, this does not imply that these patients should be given the less-effective treatment. Meaningful price negotiations and more evidence of cost-effective treatment options are warranted to make these highly effective drugs cost-effective and affordable.
Our model highlights the reality that in a non-curable disease, better PFS and OS mean more time to accrue costs for expensive therapies. Regardless of other direct costs, T-DXd every 21-day cycle costs $9,513, which already exceeded $150,000 a year. This may explain why T-DXd is not cost-effective even under the most optimistic assumptions. According to the sensitivity analysis, the economic outcome could be improved when the cost of T-DXd drops. Therefore, we investigated the most reasonable and affordable price of T-DXd using PSA. When the cost of T-DXd was less than $4,281/cycle ($11.33/mg) or $1,903/cycle ($5.03/mg), the probabilities of it being cost-effective were more than 50 and 90%, respectively. The results can help patients, government officials, and the medical financial structure make decisions. Moreover, the body weight also plays a significant role in the results as the dosage of T-DXd is weight-dependent. Patients with increased body weight needed higher doses of T-DXd, which increases the barriers for T-DXd to become affordable. Therefore, maintaining a normal body mass index might reduce the economic burden of patients with cancer.
This study has some limitations. First, our simulation model, like many others, was derived from clinical trial data and hence necessarily vulnerable to uncertainty. However, the log-logistic and Weibull models showed a good fit to the survival data and were validated in the sensitivity analysis. The long-term benefits of T-DXd for HER2-low mBC remain an open question. Further updated data reported from the DESTINY-Breast04 trial is needed to reduce these uncertainties in the future. Second, except for ILD/pneumonitis, costs of grade 1 or 2 AEs and grade 3–4 AEs with an incidence rate below 5% were excluded from the evaluation, which might influence the results. However, the sensitive analysis revealed that no matter how these parameters related with AEs varied within the predefined range, the results stayed unchanged. Third, the utility values play a pivotal role in the pharmacoeconomic analysis. We used published utility values for HER2-negative mBC as no quality-of-life data was reported in the DESTINY-Breast04 trial. One-way sensitivity analysis revealed that PFS and PD utility values affected the outcomes; however, tornado diagrams indicated that regardless of how these values varied within the allowed range, the ICERs kept greater than the threshold.
Conclusions
From the perspective of the United States, T-DXd would not be cost-effective compared with chemotherapy for HER2-low mBC given current drug prices. Considering that T-DXd can significantly extend PFS and OS of HER2-low patients, discussions and negotiations on the pricing of T-DXd are required to improve its cost-effectiveness.
Supplemental Material
sj-docx-1-tam-10.1177_17588359231169983 – Supplemental material for Cost-effectiveness of trastuzumab deruxtecan in previously treated human epidermal growth factor receptor 2-low metastatic breast cancer
Supplemental material, sj-docx-1-tam-10.1177_17588359231169983 for Cost-effectiveness of trastuzumab deruxtecan in previously treated human epidermal growth factor receptor 2-low metastatic breast cancer by Jiangping Yang, Jiaqi Han, Ni Zeng and Xi Yan in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.