
Abstract
By 2030, pancreatic cancer will become the second leading cause of cancer-related deaths in the United States and in Europe. The management of patients with advanced pancreatic cancer relies on chemotherapy and poly (ADP-ribose) polymerase inhibitors for patients who carry BRCA1/2 inactivating alterations. Some variants, such as large insertion/deletions (Indels), inactivating BRCA1/2 and therefore of clinical relevance can be hard to detect by next-generation sequencing techniques. Here we report a 47-year-old patient presenting with pancreatic cancer whose tumour harbours a large somatic intra-exonic deletion of BRCA2 of 141 bp. This BRCA2 deletion, located in the C-terminal domain, can be considered as pathogenic and consequently affect tumorigenesis because it is involved in the interaction between the DSS1 protein and DNA. Thanks to the optimized bioinformatics algorithm, this intermediate size deletion in BRCA2 was identified, enabling personalized patient management via the inclusion of the patients in a clinical trial.
Introduction
Pancreatic ductal adenocarcinoma (PDAC) will become the second leading cause of cancer-related deaths in the United States and in Europe by 2030. Despite progress in the management of PDAC, the 5-year overall survival rate remains only 10%. 1 Most patients are diagnosed at an advanced stage and are not eligible for surgery. However, thanks to more efficient chemotherapies, an increasing proportion of patients achieves tumour molecular profiling, enabling targeted maintenance therapy to then be discussed.
BRCA1/2 genes are involved in the maintenance of genome stability, specifically the homologous recombination pathway ensuring double-strand DNA break repair. Most BRCA1/2 pathogenic variants (PVs) in pancreatic cancer are frameshift insertion/deletions (Indels), stop-gains and splice-site variants.2–5 Up to 15–17% of pancreatic cancer patients harbour somatic PVs of homologous recombination-related (HRR) genes (including BRCA1/2). Genetic testing of germline BRCA1/2 (gBRCA1/2), in particular with next-generation sequencing (NGS), is now widely recommended for patients with pancreatic adenocarcinoma. Indeed, patients with gBRCA1/2 PV and disease controlled with platinum chemotherapy are eligible for maintenance therapy with poly (ADP-ribose) polymerase (PARP) inhibitors based on the results of the POLO phase III trial. 2 This recent trial demonstrated that the administration of the olaparib PARP inhibitor as maintenance therapy significantly prolonged the median progression-free survival of gBRCA1/2 PV PDAC patients. In this context, the MAZEPPA PRODIGE 72 clinical trial (NCT04348045) evaluates the efficiency of PARP inhibitors in patients whose tumours harbour somatic HRR alterations and have been controlled by platinum-based chemotherapy.
The identification of (germline or somatic) BRCA1/2 PVs thus has a significant impact on PDAC patient management. Some variants, such as indels larger than 10 bp, inactivating BRCA1/2 and therefore of clinical relevance, can be hard to detect or missed by NGS. Indeed, routine NGS short-read analyses still lack accuracy since the information of these large indels can be lost in unmatched fragments of partially mapped reads. 6
Here we report a 47-year-old patient presenting with PDAC whose tumour harbours a large somatic intra-exonic deletion of 141 bp of BRCA2 exon 18, which was difficult to detect with ‘conventional’ bioinformatics strategies. This patient was included in the MAZEPPA PRODIGE 72 trial.
Results
NGS analysis of the tumour sample concluded to a PV of TP53, KRAS and SMARCA4 and to a 141bp in-frame deletion in exon 18 of BRCA2 (c.8065_8205del/p.(Cys2689_Pro2735del) (Table S1). This large deletion of BRCA2 was found at an allelic ratio of 6%, probably underestimated because of the difficulty of NGS analysis to align the sequence (Figure 1(a)). 7 This deletion was confirmed by Sanger sequencing (Figure 1(b)).
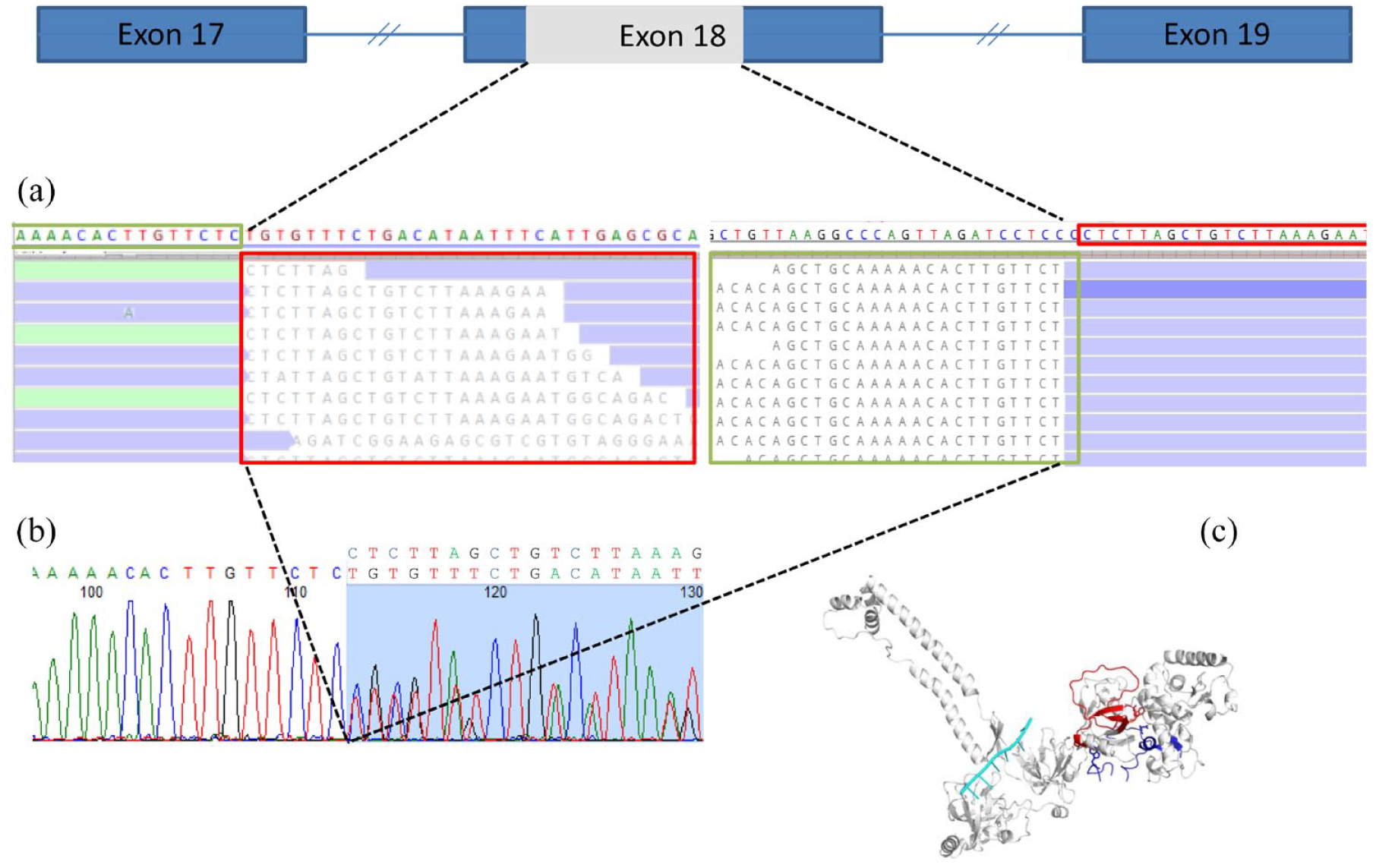
Sequencing analysis: (a) NGS reads in position 8065 and 8205 and (b) Sanger analysis with upper primer, (c) protein modelling of the 8065–8205 nucleotides (2689–2735 aa in human protein sequence) of BRCA2 bound to DSS1 and ssDNA. BRCA2 is in white/grey, DSS1 in dark blue and DNA poly-dT in cyan. The deletion of nucleotides 8065 at 8205 (2689–2735 aa in human sequence) is in red.
Both tumour and germline DNA samples were analysed (Supplemental Figure S1). The deletion was observed only on the tumour sample, suggesting that this intra-exonic deletion of BRCA2 is strictly somatic.
Genetic testing of BRCA2 revealed that some variants of uncertain clinical significance affect normal splicing patterns and disrupt gene function for exon 18.8,9 Variants of uncertain significance can induce abnormal splicing with aberrant transcripts where exon skipping was the most preponderant event. Aberrant splicing is especially common in BRCA2 exons 17 and 18 due to the presence of active exon splicing enhancers involved in exon recognition.9,10 To test the hypothesis of aberrant splicing, the BRCA2 transcript was analysed using Sanger sequencing. The data clearly indicate that the in-frame intra-exonic deletion of the BRCA2 exon 18 does not cause an aberrant skipping of exon 18. In fact, only the wild-type and the 141bp deleted forms were observed at the RNA level with the absence of pathological splicing of the entire exon 18 of 355pb (data not shown).
A 3D model was created to evaluate the potential functional impact of this deletion on the BRCA2 protein. It showed that the deletion, located in the C-terminal domain (CTD) that is also the DNA-binding domain, probably has a deleterious effect on protein function (Figure 1(c)).
Discussion
Here we report a 47-year-old woman with PDAC (tail of the pancreas, with liver metastases) whose tumour harboured a large somatic intra-exonic deletion of BRCA2 identified by NGS and confirmed using Sanger sequencing. Multiplex ligation-probe amplification analysis was unable to identify this large deletion of 141pb of exon 18. Using the transIndel bioinformatic algorithm, this deletion of clinical relevance was identified following NGS analysis. In fact, transIndel is highly sensitive for large indels usually missed by standard bioinformatics tools. 11 TransIndel can directly infer indels from the initial alignment given by the short-read aligner, offering competitive performance with the tools using realignment strategies, even though tumour cell content is low.
The CTD of BRCA2 is the DNA-binding domain and harbours a DSS1 binding site (Figure 1(c)). DSS1 and BRCA2 play a direct role in homologous recombination. 12 Indeed, the importance of the interaction of DSS1 with BRCA2 in HR is further supported by the fact that deletion of DSS1 phenocopies BRCA2 deficiency. The stability of the BRCA2 protein in mammalian cells depends on the presence and interaction with DSS1. In addition, DSS1, a component of the TRanscription-EXport-2 complex involved in transcription and mRNA nuclear export that stabilizes BRCA2 expression, may be required for the BRCA2–RAD51 complex to be associated with sites of DNA damage to promote repair.13–17 This intra-exonic deletion was further modelled to evaluate its potential functional impact. Data showed that the deletion is located in the CTD that is also the DNA-binding domain, further suggesting that this somatic BRCA2 deletion is pathogenic and could impact tumorigenesis via the loss of interaction with DDS1 in particular.
Finally, microhomology of five nucleotides found at the breakpoint junction (Supplemental Figure S2) suggests that the mechanism triggering this deletion may be Fork Stalling and Template Switching. 18 Actually, according to this model, during DNA replication, the DNA replication fork stalls at one position, the lagging strand disengages from the original template, transfers and then anneals by virtue of microhomology at the 3′ end to another replication fork in physical proximity and resumes DNA synthesis.
In conclusion, we identified a large somatic intra-exonic deletion of 141bp of BRCA2 exon 18.
Thanks to optimized bioinformatics algorithms such as transIndel, this intermediate size deletion in BRCA2 was identified, allowing personalized patient management via the inclusion of the patients in a clinical trial.
Methods
Patient
This patient was a 47-year-old woman included in the MAZEPPA PRODIGE 72 trial (NCT04348045). The trial evaluates the efficacy of a molecular-driven maintenance therapy with olaparib in PDAC patients with disease controlled after 4 months of mFOLFIRINOX chemotherapy whose tumour harbours a somatic ‘BRCAness’ profile.
Her mother had breast cancer at 46 years. Other relatives were cancer free. The patient had a well-differentiated PDAC immunopositive for CK19 and CK7 but negative for P63 and synaptophysin. The proliferation index based on Ki67 immunostaining was 50% and the tumour did not harbour a loss of MMR protein (MLH1, MSH2, MSH6 and PMS2).
Patients provided written consent to take part in the study.
NGS analysis
Sequencing was carried out using an in-house NGS panel of 571 genes, called DRAGON (detection of relevant alterations in genes involved in oncogenetics). Indexed paired-end libraries of tumour DNA from a formalin-fixed paraffin-embedded sample were generated using the Agilent SureSelect XT2 library prep kit (Agilent Technologies, Santa Clara, CA, USA). The kit allows the sequencing of targeted regions of the genome spanning 2.7 Mb. 100 ng of input DNA was used to build the libraries according to the manufacturer’s protocol. The pool was finally sequenced on a NovaSeq 6000 (Illumina) Sp 2 × 100 bp flow cell (Illumina Inc., San Diago, CA, USA) to reach an average depth of 2000× and a minimum depth of 30×.
Variant calling for intermediate-size copy number variants
A dedicated strategy using transIndel 10 was applied to call large-sized indels, with the following parameters: minimum mapping quality of 0, read depth above 10×, length between 10 bp and 1000 bp, covered by at least 30× and presenting an allelic ratio above 1%. Annotations from several databases (RefSeq, dbsnp v150, COSMIC v86, 1000 g project 08/2015 version, ESP6500, gnomAD (all and ethnicities), ICGC v21 and dbnsfp v35 predictions) were provided by Annovar 13 to annotate small variants. Only the RefSeq database was used for intermediate indels. During this step, all variants present in −10/+10 bp of each exon junction were defined as splicing.
Finally, in-house python scripts were used to add supplementary annotations (correct HGVS nomenclature (python hgvs package v1.2.5 and 2018 UTA database), MaxEntScan, Grantham and ESR scores).
PCR, RT-PCR and Sanger sequencing
A PCR was performed on tumour and constitutional DNAs to confirm the existence of the identified alteration. The pair of primers used was 5′-GAATTCTAGAGTCACACTTCC-3′ (intron 17) and 5′AATTGAGCATCCTTAGTAAGC-3′ (intron 18). Amplified sequences of DNA migrated through an agarose gel (2%) to evaluate their presence and the length. Finally, the presence of the BRCA2 deletion was validated by Sanger sequencing on the tumour sample.
RT-PCR was performed on tumour RNA using the following couple of primers: 5′-CCAGAAAGGGTGCTTCTTCAACT-3′ (exon 17) and 5′-GCGAGCAGGCCGAGTACTGT-3′ (exon 19). Then, amplified sequences of cDNA from the tumoral sample and from a wild-type sample migrated through an agarose gel (2%) and the result was confirmed by Sanger analysis.
Modelling
Modelling used the 1mje (BRCA2 CTD 2399-3011 mouse/DSS1/DNA poly-dT) and 1miu (BRCA2 CTD 2399-3102 mouse-DSS1) structure of the BRCA2 protein CTD resolved by X-ray (Yang et al. 11 ). Models of the selected mutants were visualized with PYMOL software (DeLano Scientific LLC, Palo Alto, CA, USA).
Supplemental Material
sj-docx-1-tam-10.1177_17588359221146132 – Supplemental material for Identification of a large intra-exonic deletion in BRCA2 exon 18 in a pancreatic ductal adenocarcinoma
Supplemental material, sj-docx-1-tam-10.1177_17588359221146132 for Identification of a large intra-exonic deletion in BRCA2 exon 18 in a pancreatic ductal adenocarcinoma by Inès Debbabi, Sophie Vacher, Cindy Neuzillet, Jérome Cros, Françoise Revillon, Ambre Petitalot, Anthony Turpin, Samantha Antonio, Elodie Girard, Célia Dupain, Maud Kamal, Pascal Hammel, Ivan Bièche, Julien Masliah-Planchon and Sandrine M. Caputo in Therapeutic Advances in Medical Oncology
Supplemental Material
sj-pptx-2-tam-10.1177_17588359221146132 – Supplemental material for Identification of a large intra-exonic deletion in BRCA2 exon 18 in a pancreatic ductal adenocarcinoma
Supplemental material, sj-pptx-2-tam-10.1177_17588359221146132 for Identification of a large intra-exonic deletion in BRCA2 exon 18 in a pancreatic ductal adenocarcinoma by Inès Debbabi, Sophie Vacher, Cindy Neuzillet, Jérome Cros, Françoise Revillon, Ambre Petitalot, Anthony Turpin, Samantha Antonio, Elodie Girard, Célia Dupain, Maud Kamal, Pascal Hammel, Ivan Bièche, Julien Masliah-Planchon and Sandrine M. Caputo in Therapeutic Advances in Medical Oncology