
Abstract
Pancreatic cancer has an extremely poor prognosis, only a small minority of patients undergo a resection with curative intent. Chemotherapy and/or radiochemotherapy may improve this by prolonging survival or disease-free interval and improving resectability and the proportion of microscopically complete (R0) resections. With regard to prolonging survival, both in the postoperative adjuvant setting and in locally advanced disease, chemotherapy has a positive but limited effect on survival and may be considered standard. The role of postoperative adjuvant radiochemotherapy remains debatable. For improving resectability/proportion of R0 resections, many studies suggest that the proportion of patients undergoing a resection during exploration and the proportion of R0 resections increase after neoadjuvant radiochemotherapy. This may improve the prognosis of patients with a resectable or borderline resectable pancreatic carcinoma. The effect of neoadjuvant radiochemotherapy, if any, is modest. The search for better combinations, including targeted therapy, must continue. The interpretation of single-arm studies is hampered by (selection) biases. The reporting of pathology and study endpoints should be internationally standardized. To avoid biases in studies of patients with (borderline) resectable tumours, prospective parallel registration of all patients referred for surgery would help. Ultimately, randomized controlled phase III trials should establish the role of neoadjuvant radiochemotherapy. Thus, neoadjuvant radiochemotherapy has a potential benefit in resectable and borderline resectable pancreatic cancer, but better combinations are warranted.
Introduction
Pancreatic cancer has an extremely poor prognosis. With a crude incidence of 11 in 100,000 inhabitants, it is the ninth common form of cancer in The Netherlands. It is the fifth leading cause of cancer death, and currently, the overall 2-year survival rate in The Netherlands has hardly improved over the last two decades and is less than 10% [Dutch Comprehensive Cancer Centres, 2010]. Similarly, in the USA, pancreatic cancer is the fourth leading cause of cancer death [Jemal et al. 2009]. Many papers claim that surgery is the only treatment option with curative intent, but less than 10% of all patients present with resectable disease. Even after radical surgery the median survival is about 20 months and 5-year survival rate is 15–25% [Hidalgo, 2010; Schnelldorfer et al. 2008; Sener et al. 1999]. This warrants a coordinated multidisciplinary approach to try and improve results.
Interpretation of the literature concerning the treatment of pancreatic cancer is difficult for several reasons. One methodological problem is that all studies consist of highly selected patient cohorts, and in a disease such as pancreatic cancer that has so many recurrences and deaths, even a limited selection bias may lead to relatively large and misleading differences in outcome. Surgeons currently use different criteria for resectability. Radiochemotherapy studies for locally advanced disease use a variety of selection criteria. Surgical series may or may not include peri-operative mortality in survival figures. Reporting by intent to treat (including peri-operative mortality, or even including all patients undergoing an exploratory laparotomy) might change outcome figures in some papers dramatically. Definitions currently used for borderline resectable and locally advanced disease have substantial variations between centres. Palliative chemotherapy series may or may not include nonmetastasized patients with locally advanced disease, who have a better outcome than those metastasized from the onset. One should therefore be cautious when comparing results from different studies. On the other hand, randomized data are not available for some situations and we have to rely on data from single-arm studies.
Given the fact that the only possibility for surviving pancreatic cancer is to have undergone a radical resection, and that the chance of long-term survival is substantially improved if this resection is microscopically complete (R0) [Chang et al. 2009; Neoptolemos et al. 2001], there are principally two ways in which combined modality therapy may play a role: improve survival and/or progression-free survival; increase resectability and the proportion of R0 resections. In this paper, relevant recent literature is reviewed, and suggestions for how these goals can be best pursued by performing well-designed randomized phase II trials of neoadjuvant multimodality treatment are discussed.
Improve survival or progression-free survival
Postoperative adjuvant setting
A number of studies have addressed improved survival or progression-free survival for the subset of patients with a resectable pancreatic cancer. In the adjuvant setting, a number of randomized trials have been performed over the years. Both 5-fluorouracil (5-FU) plus folinic acid and gemcitabine chemotherapy have shown a modest survival benefit in randomized clinical trials from the European Society of PAncreatic Cancer (ESPAC) [Neoptolemos et al. 2004] and the German Charité ONKOlogie (CONKO) groups [Oettle et al. 2007], respectively. In the ESPAC-1 trial, 3-year survival significantly improved from 14% to 30%. In the CONKO trial, disease-free survival improved significantly and overall survival showed a trend (3 years from 21% to 34%). In Europe, postoperative adjuvant chemotherapy is therefore widely accepted as the standard of care. ESPAC has performed another trial comparing 5-FU with gemcitabine in over a 1000 patients, that appears to show no difference, but this trial has only been presented and not yet published [Neoptolemos et al. 2005].
Chemoradiation, based on 5-FU, is widely used in the USA based on large, single-institute series from the Johns Hopkins University and the Mayo Clinic, and a Gastro-Intestinal Tumour Study Group (GITSG) trial, performed in the early 1980s [Corsini et al. 2008; Herman et al. 2008; Kaiser and Ellenberg, 1985] However, neither the small GITSG trial [Kaiser and Ellenberg, 1985], nor the randomized studies from the European Organization on Research in Treatment of Cancer (EORTC) [Smeenk et al. 2007; Klinkenbijl et al. 1999], and the ESPAC-01 trial [Neoptolemos et al. 2004], showed a significant survival benefit. On the other hand, all of these three trials used a split-course radiotherapy scheme (40 Gy in 6 weeks), that is nowadays considered obsolete and, since the early 1980s, radiochemotherapy has evolved. The EORTC has recently conducted a randomized phase II study that showed the feasibility of modern gemcitabine-based radiochemotherapy [Van Laethem et al. 2010]. In a recent surveillance, epidemiology, and end results (SEER) data analysis and a study in which the Johns Hopkins University and Mayo Clinic tried to overcome the biases of comparison with historic controls by performing a matched-pair analysis, modern radiochemotherapy is suggested to be better than observation [Hsu et al. 2010; Stessin et al. 2008] In 2010, the Radiation Therapy Oncology Group (RTOG), in close collaboration with the EORTC, opened a phase III trial to investigate the efficacy of adding erlotinib to gemcitabine chemotherapy as well as adding gemcitabine-based chemoradiation to this treatment in the postoperative adjuvant setting (RTOG 0848, EORTC 40084–22084).
Locally advanced and advanced disease
Chemotherapy is used as a palliative measure in patients with metastasized and locally advanced pancreatic cancer. A Cochrane Systematic Review of 50 randomized trials revealed a clear benefit of chemotherapy over best supportive care (odds ratio for 1-year mortality 0.37, p < 0.00001), no clear benefit of gemcitabine over 5-FU and no clear benefit of combinations over single-agent chemotherapy [Yip et al. 2006]. Later studies have sought further improvement by adding 5-FU, capecitabine, cisplatin, oxaliplatin or other drugs, such as cyclooxygenase II inhibitors, to gemcitabine but so far have failed [Hidalgo, 2010; Morak et al. 2010; Bernhard et al. 2008; Heinemann et al. 2006]. Only one trial showed a statistically significant but clinically hardly relevant benefit of adding erlotinib to gemcitabine [Moore et al. 2007].
Since local tumour growth is often a factor of importance, causing severe pain that is extremely hard to conquer, it is logical to consider radiotherapy or radiochemotherapy as a treatment option, particularly for locally advanced disease. Indeed, long-lasting palliation of pain can be achieved. In a single-arm phase II study of 44 patients with locally advanced pancreatic cancer (LAPC), 68% of the patients suffering pain experienced pain relief with a median duration of 6 months [Ceha et al. 2000]. In a retrospective analysis of pain management of 98 patients with unresectable pancreatic cancer at exploratory laparoscopy, we found the group of patients receiving radiotherapy to have a significant longer pain medication-free interval than those undergoing bypass surgery alone or those undergoing bypass surgery plus coeliac plexus blockade (9 versus 3 versus 3 months, respectively) [Van Geenen et al. 2002]. Azria and colleagues reported a series of 26 patients in which 20 patients experienced improvement of pain, 11 of whom experienced complete relief and complete cessation of analgesic consumption [Azria et al. 2002].
The qualitative systematic review of Huguet and colleagues focused on the prognostic benefit of radiochemotherapy for locally advanced nonmetastatic pancreatic cancer [Huguet et al. 2009]. They included 2 systematic reviews, 13 randomized trials and 6 nonrandomized studies. As in the previously mentioned Cochrane Systematic Review [Yip et al. 2006], they concluded that radiochemotherapy improves survival compared with the best supportive care (median survival 6 versus 13 months, p < 0.01). Also, radiochemotherapy appears to be better than radiotherapy alone (median survival 5 versus 9 months, p < 0.01). Radiochemotherapy is not superior to chemotherapy alone and is more toxic [Huguet et al. 2009].
Hence, for unresectable LAPC and advanced pancreatic cancer chemotherapy alone can be considered the standard of care unless severe pain from the local tumour is the main symptom. In that case, radiochemotherapy should be considered.
Increase resectability and R0 resections
It is difficult to assess the proportion of patients with a resectable tumour. Some centres showed that even a nonradical (R1 or R2) resection is better than bypass surgery only in a selected group of patients [Sasson et al. 2002]. Others only want to perform a R0 resection. Thus, the selection criteria for pancreatoduodenectomy, and hence the proportion of patients undergoing resection, vary in different studies. Moreover, the pathology methods to assess microscopic margins and lymph node involvement show a wide variation and there is no standardization, which may largely influence results [Westgaard et al. 2009]. These factors make comparison of surgical series extremely difficult. Resectability of tumours is difficult to assess. Although criteria have been developed for assessment by preoperative modern imaging techniques, such as computed tomograpy scan or magnetic resonance imaging [Phoa et al. 2000, 2005], many still decide during exploratory laparotomy whether or not to continue with a resection. This is mainly dependent on attitudes towards performing a resection of the portal and mesenteric veins and the mesenteric artery. It is generally believed that increasing the proportion of resectable tumours improves survival and this is why many aim to ‘make unresectable tumours resectable’ by chemotherapy or radiochemotherapy. In addition, it is important to analyse if preoperative radiochemotherapy increases the proportion of R0 resections. Large studies showed that R0 resection leads to a better prognosis [Chang et al. 2009; Neoptolemos et al. 2001].
Recent studies of neoadjuvant radiochemotherapy.
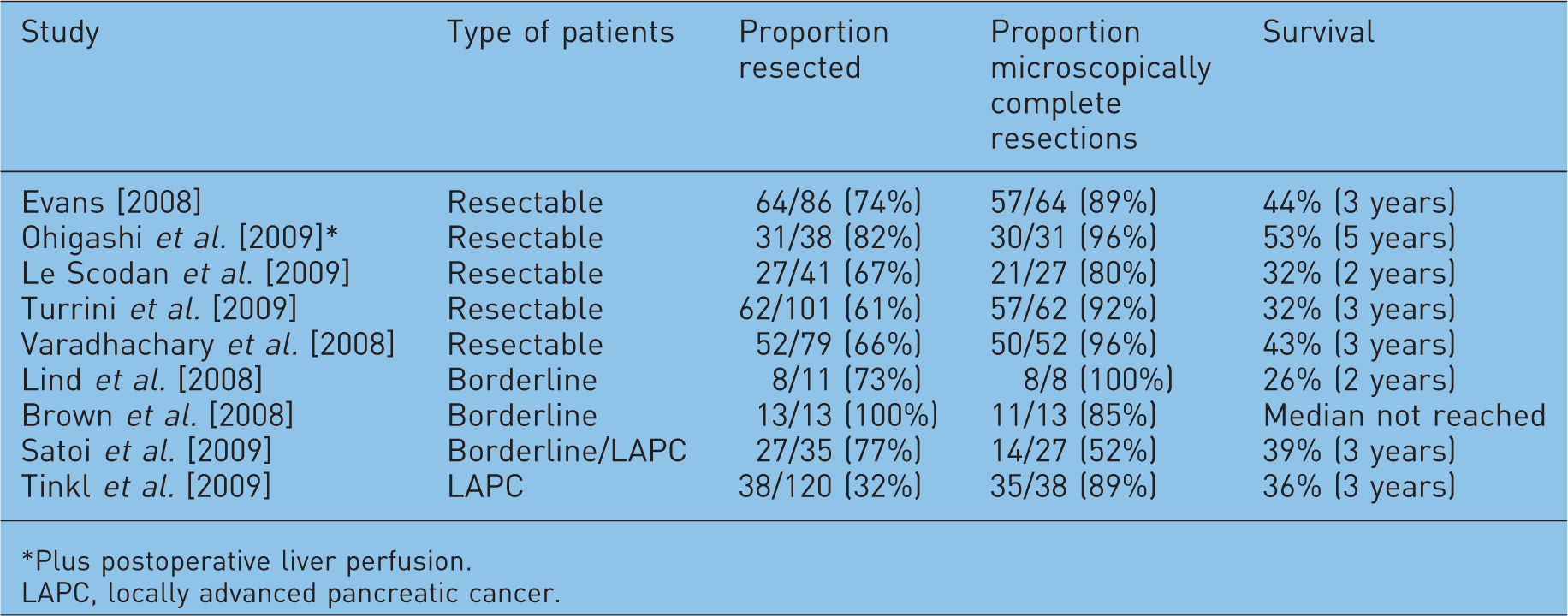
Plus postoperative liver perfusion.
LAPC, locally advanced pancreatic cancer.
Discussion
The role of radiochemotherapy in pancreatic cancer is still under discussion. In the postoperative adjuvant setting chemotherapy alone is nowadays generally accepted. A new phase III trial is underway to establish the value of modern radiochemotherapy (RTOG 0848, EORTC 40084–22084). For LAPC or advanced pancreatic cancer, radiochemotherapy may play a role in pain management but it does not appear to be better than chemotherapy alone in terms of survival [Huguet et al. 2009]. Both in the adjuvant setting and for (locally) advanced disease, 5-FU or gemcitabine-based chemotherapy may be considered standard, but their effects are limited.
Studies of ‘neoadjuvant radiochemotherapy’ for patients with resectable or borderline resectable pancreatic cancers seem to offer hope [Le Scodan et al. 2009; Ohigashi et al. 2009; Satoi et al. 2009; Tinkl et al. 2009; Turrini et al. 2009; Brown et al. 2008; Evans et al. 2008; Lind et al. 2008; Varadhachary et al. 2008]. The neoadjuvant approach has the theoretical advantage of allowing a higher proportion of patients to undergo a resection. Furthermore, results of the available studies show a relatively high percentage of R0 resections [Gillen et al. 2010]. Some studies even suggest a better survival in this group of patients initially considered prognostically worse than the primarily operable patients [Satoi et al. 2009; Brown et al. 2008; Lind et al. 2008]. A SEER database report concerning a total of 3885 operated patients, showed the overall survival of patients treated with preoperative radiochemotherapy to be better than that of patients treated with postoperative radiochemotherapy or surgery alone [Stessin et al. 2008]. This is in line with recent developments in other forms of cancer such as rectal and oesophageal cancer where the preoperative application of radiochemotherapy has been shown to be superior to postoperative use of the same treatment or surgery alone [Jin et al. 2009; Wong et al. 2007].
However, the advantages of neoadjuvant treatment are still limited and the search for optimal schedules should continue. Targeted therapies may specifically enhance the effects of both radiation and chemotherapy to pancreatic cancer cells. Perhaps even combinations of new compounds will have to be added to radiochemotherapy to optimize the effect. Therefore, new phase I/II studies remain necessary in the near future. Furthermore, the available information should be interpreted with caution. Study populations are by definition selected, and in diseases with a poor prognosis such as pancreatic cancer, differences in selection may strongly influence the number of events and hence the outcome. Comparison of different studies is impossible if criteria for selection remain poorly defined. Endpoints and definitions of endpoints may differ per study. Analysis of the proportion of patients that have actually undergone a resection is not by intention to treat. To overcome some of these methodological flaws, we suggest the following policies. There should be international appointments on uniform reporting of endpoints in clinical trials. Recently, the EORTC, in collaboration with a number of international research groups, has started a formal consensus project to achieve this, that is, the DATECAN project. There should be international appointments and standardization of reporting pathology data, in particular resection margins and lymph node status [Westgaard et al. 2009]. Studies for neoadjuvant radiochemotherapy of borderline or unresectable pancreatic cancer should clearly and uniformly state the inclusion criteria. Prospective registration of patients considered to have a resectable tumour in parallel would be interesting to obtain a ‘historical’ control group and an indication of the total cohort of resectable and potentially resectable patients, and hence, potential biases. Moreover, performing analyses by intent to treat would be necessary to analyse overall outcome and obtain an estimation of numbers needed to treat.
Conclusion
Neoadjuvant radiochemotherapy appears to have a potential benefit in resectable and borderline resectable pancreatic cancer. Studies to investigate this further should try to overcome selection biases by recording all patients referred for resection. Uniform standards for reporting pathology and study endpoints must be developed.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Conflict of interest statement
The authors state no conflict of interest.