
Abstract
Gastroesophageal cancers (GEC) have a poor survival rate of 20–30% at 5 years, often due to delayed presentations. Neoadjuvant chemoradiotherapy (CRT) followed by surgery or peri-operative chemotherapy and surgery are widely used as the standard of care for patients with resectable GEC. Immune checkpoint inhibitors (ICIs) have improved survival in metastatic and recurrent GEC which led to their application in resectable GEC. Based on the pivotal CheckMate 577 study results, the Food and Drug Administration (FDA) approved nivolumab for patients with completely resected high-risk esophageal or gastroesophageal junction cancer (GEJC). Several ongoing trials with many ICIs could potentially improve resectable GEC outcomes. This review explores the rationale for using ICIs in resectable GEC and discusses the significance of reported clinical trials. Finally, we will examine some ongoing clinical trials and the challenges as well as prospects of ICIs in resectable GEC.
Keywords
Introduction
Esophageal cancer is a global health problem. As per the 2020 global cancer statistics, 604,100 new esophageal cancer cases were diagnosed globally with 544,076 deaths. 4 Most of the esophageal cancers in the United States are adenocarcinoma, whereas, worldwide, squamous cell carcinoma (SCC) is the most common histologic type. 4 Since the publication of the CROSS trial, most localized esophageal cancers are treated with trimodality treatment: chemoradiation (CRT) followed by planned esophagectomy with consideration for definitive chemoradiation in squamous cell cancer patients. 4
On the other hand, gastric cancer (GC) is one of the most common cancers worldwide and the third leading cause of cancer-related death. 4 Surgery is the only curative option, and peri-operative chemotherapy has been used in GC for several years. Compared to surgery alone, the MAGIC and FNCLCC/FFCD ACCORD study demonstrated improved overall survival (OS) with peri-operative chemotherapy.4,5 More recently, the FLOT4 study compared a docetaxel-based triplet FLOT (fluorouracil plus leucovorin, oxaliplatin, and docetaxel) as peri-operative therapy for patients with locally advanced, resectable gastric or gastroesophageal junction (GEJ) to epirubicin, cisplatin, fluorouracil/epirubicin, cisplatin, capecitabine, the chemotherapy backbone used in the MAGIC study. 5 As OS was better in the FLOT arm, since then the FLOT regimen has become the new standard of peri-operative chemotherapy for resectable GC. Despite multimodality treatment, only about half of the non-Asian patients are ultimately cured, highlighting the unmet need for developing better treatment options for these patients. In Asia, an upfront D2 gastrectomy followed by adjuvant chemotherapy is the standard of care for resectable gastric or GEJ cancer. 6
Recently, immune checkpoint inhibitors (ICIs) are routinely used in the frontline setting in combination with chemotherapy to treat metastatic gastroesophageal cancer (GEC) patients based on the OS advantage seen in the following landmark trials: KEYNOTE 590, CheckMate 648, and CheckMate 649.5,7,8 Based on these results, there is increasing enthusiasm for ICI in the resectable GEC. Several clinical trials have looked at the efficacy of ICIs in combination with the existing treatments to improve outcomes in this difficult to treat population. Of these trials, CheckMate 577 had practice changing implications. CheckMate 577 study recruited resected (R0) stage II or III esophageal or gastroesophageal junction cancer (GEJC) patients who had received neoadjuvant CRT and had residual pathological disease. Patients were randomized to receive nivolumab versus placebo postoperatively. 9 The median disease-free survival (DFS) was 22.4 months in the nivolumab group as compared with 11.0 months in the placebo group (HR 0.69; p < 0.001). 9 This study led to the Food and Drug Administration (FDA) approval of nivolumab in the adjuvant setting and sparked interest among investigators to use ICIs in the neo-adjuvant or peri-operative setting. In this review, we will discuss the data from some of the recent studies that used ICIs peri-operatively in GEC, highlight the challenges and discuss future directions.
Rationale for using ICI in the peri-operative setting
Peri-operative therapy aims to treat micrometastatic disease early on to prevent local and distal relapse. There are several advantages of using ICIs pre-operatively. Firstly, patients with resectable GEC often tolerate systemic treatment much better before surgery. Secondly, a larger tumor before surgery may also generate higher number of neoantigens to produce more polyclonal T-cells, which could make ICIs more effective in the neoadjuvant setting. 9 Finally, there are ongoing hypotheses that ICIs could be more effective in the preoperative setting to overcome the immunosuppressive effects of surgery, like systemic glucocorticoid secretion. 10 Therefore, the early use of immunotherapy could help downstaging and improves pathological responses. Most used checkpoint inhibitors in this setting are anti-PD-1/PD-L1 drugs, which reinvigorate exhausted T-cells, and the anti-CTLA-4 drugs that decrease the activation threshold for naïve T-cells. 11 In the clinical arena, the randomized phase III, CheckMate 816 study showed that neoadjuvant nivolumab, when combined with chemotherapy, improved event-free survival (EFS) and pathologic response rate in resectable non-small cell lung cancer, compared to chemotherapy alone. 12 Similarly, the KEYNOTE-522 study, a phase 3 randomized trial, showed that neoadjuvant pembrolizumab combined with chemotherapy followed by adjuvant pembrolizumab improved both pathologic complete response (pCR) as well as EFS in early-stage triple-negative breast cancer compared to neoadjuvant chemotherapy alone.13,14 Another small, randomized study in resectable glioblastoma showed that the neoadjuvant use of pembrolizumab was associated with improved progression-free survival (PFS) and OS compared to those who received adjuvant pembrolizumab alone. 15 Based on this data and the proven activity of ICIs in advanced/metastatic GEC and resected esophageal cancer, there is a clear rationale for using these agents in the neoadjuvant/peri-operative setting. On the other hand, there are certain advantages of using ICIs in the adjuvant setting as well, like less concern about delaying surgery and surgical complications. Figure 1 depicts the advantages and disadvantages of using ICIs in the neoadjuvant versus adjuvant setting.

Advantages and disadvantages of using ICIs in the neoadjuvant versus adjuvant setting.
Esophageal cancer
GECs can originate at the esophagus, GEJ, or stomach. Esophageal adenocarcinoma (EAC) presents as a loco-regional disease in approximately 50% of the cases. 16 Typically, most of these patients are treated with neoadjuvant chemoradiation followed by surgery. However, despite multimodality treatment, OS at 5 years is less than 50%. 17 It has been shown that achieving pathologic complete response (pCR) improves OS. 18 Therefore, several neoadjuvant clinical trials have used pCR as a surrogate endpoint. In the CROSS trial, a pCR was observed in 23% of patients with adenocarcinoma versus 49% with squamous-cell carcinoma (p = 0.008). Given the high pCR rate with chemoradiation, sometimes, surgery is omitted in ESCC patients, and this approach is known as definitive chemoradiation.
There are several proposed mechanisms why radiation may render a tumor immunosensitive. Some of these mechanisms include the release of pro-inflammatory mediators, increasing tumor-infiltrating cytotoxic cells and modulating neo-antigen expression. 18 Herrera et al. showed that radiotherapy could directly induce the DNA damage in tumor cells, stimulate the release of tumor-associated antigens, and increase the infiltration of T lymphocytes in the tumor. However, radiotherapy can also upregulate the PD-L1 expression on the tumor cells and inhibit the anti-tumor activity of effector T cells, leading to radiotherapy resistance. Therefore, radiotherapy combined with ICIs can not only improve the sensitivity of radiotherapy but also harness the immune system to improve cancer therapy. 19
In the adjuvant setting, CheckMate 577 study showed that adjuvant nivolumab was associated with an improvement in the DFS. Notably, esophageal squamous cell cancer (ESCC) patients achieved more benefit from nivolumab [29.7 versus 11.0 months, HR 0.61 (95% CI, 0.42–0.88)] compared to EAC patients [19.4 versus 11.1 months, HR 0.75 (95% CI, 0.59–0.96)] (Table 1). 9 Like the CheckMate 577 study, a phase II study included 24 patients with EAC or GEJ adenocarcinoma who did not achieve a pCR after the trimodality therapy. Patients received durvalumab, an anti-PD-L1 drug, for up to a year after the surgery. Adjuvant durvalumab improved the 1-year recurrence-free survival to 78.6% compared to the historical rate of 50%. 20
Reported clinical trials with ICI in neoadjuvant/adjuvant setting in esophageal cancer.

pCR, pathologic complete response; CRT, chemoradiation; RFS, relapse-free survival; DFS, disease-free survival; FOLFOX, Oxaliplatin + Leucovorin + Fluorouracil; OS, overall survival; PFS, progression-free survival; MPR, major pathologic response.
Encouraged by the positive data in the adjuvant setting, investigators have designed clinical trials to use ICIs pre-operatively. Shah et al. conducted a single-arm phase 2 study in EAC/GEJ adenocarcinoma patients, where they showed that a combination of pembrolizumab with preoperative chemoradiation was not only well-tolerated but also produced a major pathologic response (MPR) in 50% patients, which was significantly higher compared to the historical data 29 On the other hand, two other neoadjuvant trials used atezolizumab 24 and pembrolizumab, 25 respectively, combined with chemoradiation per CROSS trial, did not show an improvement in the path CR rate. Table 1 summarizes some of the neoadjuvant studies.
Given that many patients are not eligible for surgery, the KEYNOTE-975 study is evaluating the role of pembrolizumab in combination with definitive chemoradiation in locally advanced esophageal or GEJ cancer. 29 On the other hand, SKYSCRAPER-07 study is a randomized phase 3 study that will assess the efficacy of a combination of atezolizumab, an anti-PD-L1 antibody, and tiragolumab, an anti-TIGIT antibody against atezolizumab monotherapy or placebo in patients with unresectable ESCC whose cancers have not progressed following definitive chemoradiation. 30 Similarly, KUNLUN (NCT04550260) is a global, randomized, multicenter, placebo-controlled, phase 3 study which is assessing the efficacy of durvalumab along with and after definitive chemoradiation in locally advanced, unresectable ESCC patients. 31 Of note, unlike the KEYNOTE-975 study, the later two studies are only enrolling patients with ESCC, where chemoradiation and ICIs generally produce better outcomes, and these effects may be enhanced by further blocking the TIGIT pathway in the SKYSCRAPER-07 study. Nevertheless, if the above studies successfully produce a significant clinical response in ESCC, we can potentially move towards a more organ-sparing approach in this patient population.
In Asia, pre-operative chemotherapy without radiation is often used prior to surgical resection of stage II or stage II esophageal cancer. 32 Like radiation, chemotherapy drugs have an immunomodulatory effect, which explains their synergistic activity with the ICIs. 31 Several studies have combined chemotherapy with immunotherapy in resectable esophageal cancer. In a recent study from China, investigators combined chemotherapy with camrelizumab, an anti-PD-1 antibody, to treat patients with ESCC before their surgery. It produced a path CR rate of 39%. Notably, the combination was well tolerated. 30 Similarly, another study used a combination of pembrolizumab, cisplatin, and paclitaxel in resectable stage III ESCC patients, and MPR was observed in 72% of patients, including a path CR of 41%. Objective Response Rate (ORR) was 97%. The combination did not have any new safety signals and did not result in a delay in surgery. 33 These results suggest that with the increasing use of ICIs in the future, some patients may be spared from radiation, at least in ESCC. 34 Table 2 lists some ongoing clinical trials with ICI in resectable esophageal cancers.
Ongoing clinical trials (accessed March 2022) with ICIs in resectable esophageal cancer.
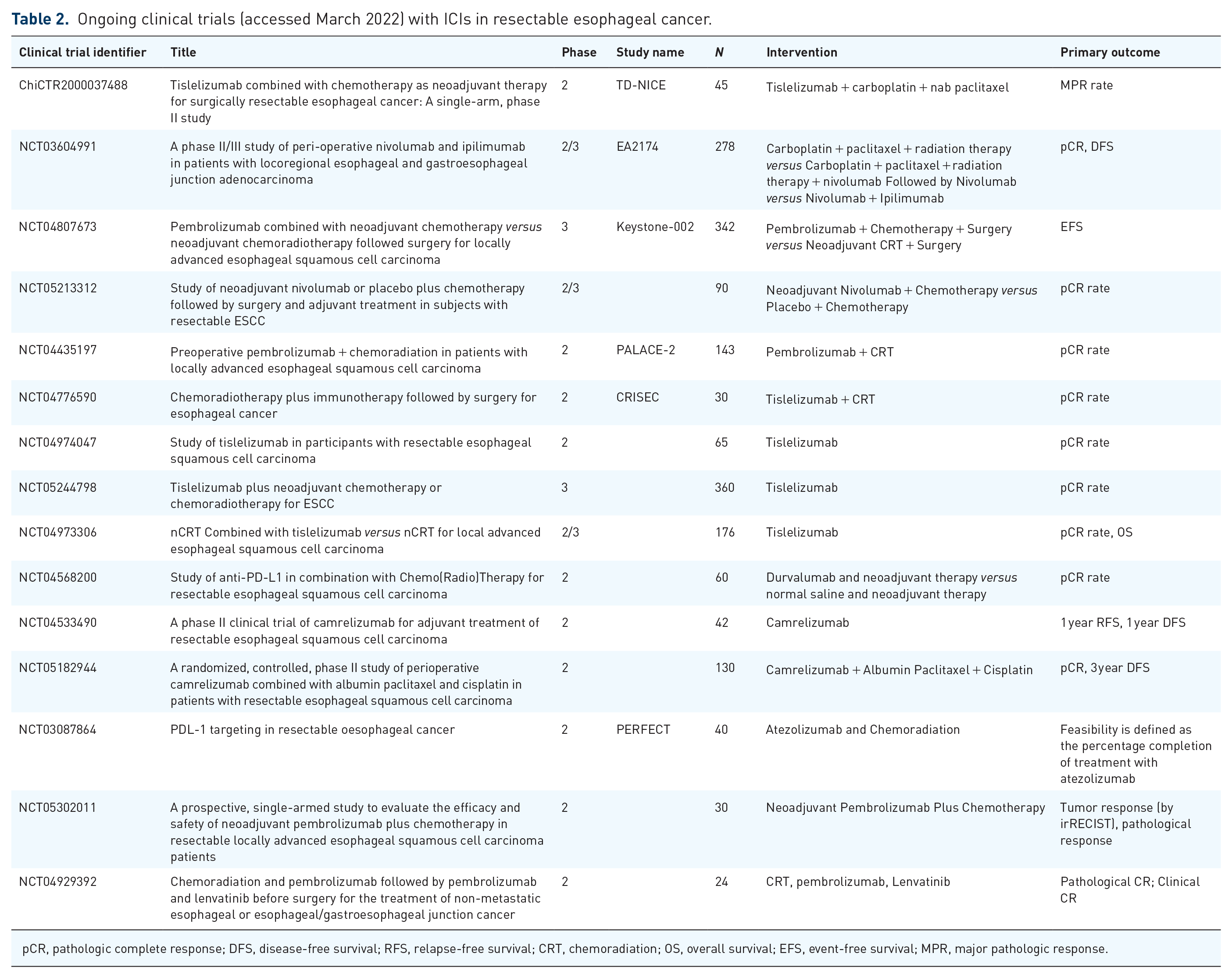
pCR, pathologic complete response; DFS, disease-free survival; RFS, relapse-free survival; CRT, chemoradiation; OS, overall survival; EFS, event-free survival; MPR, major pathologic response.
Gastric/GEJ cancer
Comprehensive molecular characterization of gastric adenocarcinoma has revealed four distinct subtypes: Epstein–Barr virus (EBV) positive, microsatellite unstable (MSI-H), genomically stable, and chromosomal unstable. 35 Further characterization of esophageal cancers has shown that ESCC and adenocarcinoma show distinct molecular characteristics. EAC mirrors the chromosomally unstable variant of gastric adenocarcinoma, suggesting that these cancers could be thought of as a single disease. Apart from EBV positive and MSI-H disease, which are infrequent, gastroesophageal adenocarcinoma (GEAC) is not usually very sensitive to anti-PD-1/PD-L1 ICIs. 36
It is, therefore, reasonable to consider a combination of chemotherapy and an ICI in resectable GEAC. Until recently, it was not known whether chemotherapy helps or hinders the effect of ICIs. Kim et al. performed a study to examine the effect of chemotherapy on the immune microenvironment of GC. Using paired pretreatment and on-treatment tissue biopsy during standard first-line chemotherapy, they showed that among the chemotherapy non-responders, there was a lack of effector T-cells, decreased dendritic cells, along with an increase in LAG 3-positive exhausted T-cells, thereby arguing that sometimes tumor microenvironment (TME) directed immunomodulatory agents may need to be combined with chemotherapy to achieve the desired response. 37 On the other hand, in a responder, CD8 + T-cell infiltration and PD-L1 upregulation were noted, highlighting that PD-L1 is a dynamic biomarker. In some instances, chemoimmunotherapy combination can favorably modulate the TME, regardless of the baseline TME composition.
Based on these premises and the remarkable clinical success of chemoimmunotherapy combinations in metastatic GEAC, such combinations have been tested in resectable GEAC. Several single-arm studies have shown a path CR rate ranging between 4% and 33% in resectable GEAC (Table 3). We must be cautious in interpreting these data since these studies did neither have a comparator arm nor a robust sample size.
Reported ICI trials in resectable GEC.

FOLFOX, Oxaliplatin + Leucovorin + Fluorouracil, CAPOX, Oxaliplatin + Capecitabine; DFS, disease-free survival; OS, overall survival; MPR, major pathologic response.
However, all the studies mentioned above used a combination of 5-FU-platinum doublet with an ICI. Since FLOT is the most commonly used peri-operative regimen in GEAC, it is interesting to see the safety and efficacy of a FLOT and ICI combination. ICONIC is a single-arm phase II trial investigating the safety and efficacy of peri-operative FLOT with an anti-PD-L1 agent avelumab in resectable GEAC. Interim results from the study showed that the combination was safe and achieved a 100% R0 resection rate. 45 Similarly, the randomized phase II DANTE study evaluated the safety and efficacy of atezolizumab in combination with peri-operative FLOT. The preliminary data suggest that the combination is both feasible and safe. The addition of Atezolizumab increased complete path CR from 15% to 24% in all patients, regardless of the PD-L1 Combined Positive Score (CPS) score. However, the difference was much higher in higher PD-L1 CPS groups as well as the MSI-H subgroup. 44
Currently, several phase III trials are assessing the efficacy of chemoimmunotherapy in resectable GEAC. KEYNOTE-585 is a global, multicenter, double-blind, placebo-controlled, randomized, phase III study randomizing gastric/GEJ adenocarcinoma patients to chemotherapy plus pembrolizumab versus Placebo. 46 However, the majority of the patients will have received platinum doublet chemotherapy. On the other hand, the phase III MATTERHORN study randomizes patients to peri-operative FLOT with or without durvalumab, an anti-PD-L1 antibody. 47 EORTC VESTIGE study is an ongoing open-label randomized phase II study comparing the efficacy of adjuvant nivolumab plus ipilimumab versus standard post-operative chemotherapy in high risk (pathologic node-positive or margin positive) post-resection GEAC patients who received neoadjuvant chemotherapy. 48 VESTIGE is similar to CheckMate-577 in its risk-adaptive design but it remains to be seen whether it produces a similar magnitude of benefit given patients will not be exposed to radiation unlike CheckMate-577 and compares to an active chemotherapy control arm. Finally, the ATTRACTION-05 study is an ongoing double-blind, multicenter, randomized, phase III, Asian study comparing the efficacy of nivolumab and chemotherapy to chemotherapy alone in the adjuvant setting in gastric/GEJ adenocarcinoma patients undergoing upfront D2 or more extensive lymph node dissection. 49 Table 4 lists some other ongoing clinical trials with ICI in gastric/GEJC.
Ongoing clinical trials (accessed March 2022) with ICIs in resectable gastric/GEJ cancer.

ORR, Objective Response Rate; AE, Adverse Events; DFS, Disease free survival; XELOX, Oxaliplatin + Capecitabine; GEJ, Gastroesophageal Junction; PDL-1, programmed death-ligand 1; AGOC, Advanced Gastro-Oesophageal Cancer; no, number; pCR, Pathologic complete response; NCT, Neoadjuvant chemootherapy; MPR, major pathological response; FLOT, Fluorouracil, Leucovorin, Oxaliplatin and Docetaxel; GE, Gastroesophageal; ctDNA, circulating tumor DNA; OS; overall survival; EFS; event-free survival.
Unique subpopulations in GEAC
HER-2 positive GEAC is a unique population that seems sensitive to both HER-2 directed and a combination of HER-2 and anti-PD-1 therapy. It has been shown that trastuzumab, an anti-HER-2 antibody commonly used in HER-2 positive GEAC, upregulates PD-1 and PD-L1 expression, increases tumor-infiltrating lymphocytes, and modulates the expression of MHC class II. 50 Besides, it also synergizes with anti-PD-1 therapy. 51 This led to the KEYNOTE-811 trial, a multicenter, global, double-blind, phase III study assessing the efficacy of pembrolizumab combined with trastuzumab and chemotherapy against placebo combined with trastuzumab and chemotherapy in advanced HER-2 positive gastric or GEJ adenocarcinoma. The pembrolizumab arm produced an unprecedented response rate of 74% compared to 52% in the standard arm, leading to the FDA approval of pembrolizumab in this setting. Given this success, it is worth investigating this regimen in the peri-operative setting. Of note, a randomized phase II study in Her 2 positive, resectable esophagogastric adenocarcinoma showed that a combination of two Her-2 targeted antibodies, trastuzumab and pertuzumab to the FLOT chemotherapy backbone improved pCR from 12% to 35%. 52 Unlike when combined with chemotherapy, addition of Her-2 targeted therapy does not appear to benefit patients undergoing chemoradiation. The randomized phase III RTOG 1010 study evaluated the efficacy of trastuzumab in Her-2 overexpressing, resectable, esophageal cancer patients undergoing chemoradiation. Patients were randomized to chemoradiation (with carboplatin and paclitaxel) versus chemoradiation and peri-operative trastuzumab. The addition of trastuzumab failed to improve DFS in the total population. Therefore, it seems that peri-operative chemotherapy combined with Her-2 targeted therapy and ICIs could be promising for Her-2 overexpressing, resectable esophagogastric adenocarcinoma. 53
The incidence of MSI-H in resectable GC can be as high as 15%. 54 Advanced GC patients often respond well to single-agent immunotherapy. 55 Further subgroup analysis of the KEYNOTE-062 study showed that the addition of chemotherapy to pembrolizumab neither improved the response rate compared to pembrolizumab alone (64.7% versus 57.1%) nor did it add any survival advantage. On the other hand, a post hoc analysis of the MAGIC trial by Smyth et al. showed that MSI-H patients did not have any survival benefit from peri-operative chemotherapy. These results suggest that immunotherapy alone may be used as a peri-operative treatment in MSI-H GC. 56 Accordingly, the phase II NEONIPIGIA trial enrolled 32 treatment-naïve, resectable, MSI-H gastric/GEJ adenocarcinoma patients to treat them with a combination of nivolumab and ipilimumab for a total of 12 weeks of neoadjuvant treatment. It was followed by surgery and adjuvant nivolumab for 9 months. The study showed an unprecedented path CR rate of 58.6%. The regimen was well tolerated, with rare relapses within the short-term follow-up period. 57 This trial raised several questions. Firstly, the path CR rate is so high in the MSI-H population that some patients may be cured by immunotherapy alone and may never require surgery. This approach is being evaluated in the phase II INFINITY trial. 58 Secondly, some patients still do not respond to immunotherapy despite the high response rate. Therefore, it is crucial to identify those MSI-H patients upfront who would not benefit from the immunotherapy-only approach. A recently published study showed that AXIN1 and PTCH1, related to WNT/b-signaling, can confer resistance to pembrolizumab monotherapy in MSI-H GC patients. 59 The same study showed that a higher tumor mutational burden (TMB) was associated with a better outcome. Similarly, another study by Chida et al. showed that low TMB and PTEN mutations are negative predictors of response from PD-1 blockade in MSI-H gastrointestinal cancers. 60 These studies suggest that TMB and the TME composition should be taken into consideration for designing future immunotherapy trials in the MSI-H patient population. Patients with a low probability of response should be treated with combination therapy rather than immunotherapy alone.
Challenges and future directions
Despite great promise, there are several unanswered questions regarding the design of future immunotherapy clinical trials in resectable GEC. Perhaps, the most important among those is whether immunotherapy should be used for all patients or a biomarker selected group of patients. Subgroup analysis of the CheckMate 649 study showed no survival advantage of using nivolumab in patients with a PD-L1 CPS score of less than 5; however, the ORR was improved with the addition of nivolumab, regardless of the CPS score. Besides, PD-L1 is a biomarker that shows both spatial and temporal heterogeneity. In a study, Zhou et al. showed that the concordance between PD-L1-status of paired baseline primary and metastatic tumors was only 61%. Also, PD-L1 is a dynamic biomarker whose expression may change over time, especially after chemotherapy. In the study mentioned above, Zhou et al. showed that the concordance between pre and post PD-L1 status is only 63%. 61 Finally, it is also unclear if the PD-L1 CPS score is used as a biomarker in the neoadjuvant setting, what would the optimal cut-off be. Based on these data, it is reasonable to say that the PD-L1 CPS score alone may not be a sufficient selection criterion for neoadjuvant trials.
This brings up another important question regarding the use of novel biomarkers in the peri-operative setting. Although not specific to immunotherapy, several clinical trials show that circulating tumor DNA (CtDNA) can be a useful biomarker in monitoring disease response/recurrence in resectable cancers. 62 In a study that looked at adjuvant atezolizumab in urothelial cancers, atezolizumab improved DFS and OS only in those patients who were CtDNA positive but not in CtDNA negative patients. Interestingly, atezolizumab also increased CtDNA clearance compared to observation. Using a similar approach in patient selection may avoid unnecessary toxicity and the cost of long-term immunotherapy in several GEC patients after surgery.
Historically, peri-operative immunotherapy trials have used anti-PD-1/PD-L1 or anti-CTLA-4 antibodies in GEC. However, several other checkpoints are showing promise in advanced GEC. In a study by Wainberg et al., a combination of atezoliumab and tiragolumab, an anti-TIGIT antibody, was well tolerated and produced a response rate of 28% in a heavily pre-treated population in esophageal cancer. 63 In another study, Wainberg et al. showed that a combination of TTX-030 (anti CD39 antibody) with chemoimmunotherapy has promising activity in advanced GEC. 64 Similarly, a phase IB trial is assessing the efficacy of an anti-LAG3 antibody, relaltimab, in combination with nivolumab, prior to concurrent chemoradiation in resectable esophageal/GEJ cancer (NCT03044613). Soon, we are likely to see more trials using a combination of novel checkpoint inhibitors with PD-1/PD-L1 drugs in resectable GEC. Also, recent data suggest that claudin 18.2 and fibroblast growth factor receptor 2b (FGFR2b) are important targets in GEC.65–67 There are ongoing trials evaluating a combination of these agents with ICIs. For example, the FORTITUDE-102 (NCT05111626) study is evaluating the safety and efficacy of a combination of Bemarituzumab, an anti FGFR2b antibody with chemotherapy and Nivolumab in metastatic, FGFR2b overexpressed untreated advanced gastric and GEJ cancer. If the above studies are successful, they may be used in the treatment of resectable GEC adenocarcinoma as well (Table 2).
Despite the high response rate with the use of chemoimmunotherapy, some GEC patients, unfortunately, do not respond. An exploratory biomarker analysis of the CheckMate 649 study showed that a higher angiogenetic gene expression signature was associated with less benefit from the addition of nivolumab. 68 This may bring up the rationale for using anti-VEGF combination with chemoimmunotherapy to improve the ORR in resectable GEC. However, it should be kept in mind that bevacizumab was associated with increased surgical complications without improving survival in resectable GEC. 69 Therefore, anti-VEGF combinations should be considered cautiously in this patient population.
There are also several studies associating immune checkpoints with prognosis in GE cancers. For example, lymphocyte activation gene-3 (LAG-3), which is expressed by immune cells, is often associated with good prognosis in ESCC 70 ). On the other hand, overexpression of CD-39, which is the rate-limiting enzyme in the production of adenosine, was shown to be associated with poor outcomes after resection in GC 71 ). A combination of anti PD-1/PD-L1 checkpoints with these novel targets should be explored in GEC.
Finally, as we move towards using more combination immunotherapy upfront, we are likely to see an increase in the response rate, which, in turn, may lead to organ preservation or a non-surgical approach in a certain subgroup of patients like MSI-H, HER-2, or ESCC. As already discussed, the path CR rate was nearly 59% in the NEONIPIGIA study, with some durable responses. These patients can probably be observed without surgery. Similarly, definitive chemoradiation is already practiced for some patients with esophageal SCC. If the ongoing trials like KEYNOTE-975 are successful, more patients with esophageal cancer will likely undergo non-operative management (NOM).
Conclusion
We have established adjuvant nivolumab as a standard of care in high-risk esophageal cancer patients after trimodality therapy. Specific subgroups of resectable GEC patients, like MSI-H or ESCC, are susceptible to immunotherapy and may be treated non-operatively, pending larger, confirmatory studies. Unfortunately, most resectable GEC patients have microsatellite stable adenocarcinoma, and they do not respond to ICIs very well. We believe that we will see more use of peri-operative chemoimmunotherapy, or immunotherapy combined with radiation, in this population. Finally, the combination of chemotherapy, targeted therapy, anti-PD-1/PD-L1/CTLA-4 ICIs, novel ICIs, and proper biomarker-designed trials probably holds the key to the cure of GECs.
Footnotes
Acknowledgements
None.