
Abstract
Background:
This study evaluated the cost-effectiveness of nivolumab plus chemotherapy (NC) or ipilimumab versus chemotherapy as a first-line treatment for advanced esophageal squamous cell carcinoma (ESCC) in the United States and China.
Methods:
A partitioned survival model was constructed from the perspective of the US third-party payers and Chinese healthcare system. Health states and transition probabilities were modeled based on the survival data from the CheckMate-648 clinical trial (NCT03143153). The time horizon for the model was 10 years. Only direct medical costs were considered. One-way and probabilistic sensitivity analyses were conducted to assess the robustness of the results.
Results:
In the United States, nivolumab plus ipilimumab (NI) led to an incremental cost-effectiveness ratio (ICER) of $155,159.82/quality-adjusted life year (QALY) and $104,297.07/QALY gained in the overall population and in patients with tumor cell programmed death-ligand 1 (PD-L1) expression of ⩾1% (subgroup), respectively. The ICER for the subgroup was between the willingness-to-pay (WTP) threshold values of $100,000/QALY and $150,000/QALY, and the other case was higher than $150,000/QALY. NC led to an ICER of $518,062.85/QALY and $193,169.49/QALY gained in the overall population and the subgroup, respectively. Both ICERs were significantly higher than the WTP threshold of $150,000/QALY. In China, the ICERs for patients treated with the addition of nivolumab were >$90,000/QALY in all cases, significantly exceeding the WTP threshold of $37,654/QALY.
Conclusions:
NI is more cost-effective than NC or chemotherapy alone for treating advanced ESCC with PD-L1 expression ⩾1% in the United States. Chemotherapy alone is the only cost-effective option in China.
Keywords
Introduction
Esophageal cancer (EC) is one of the leading causes of cancer-related deaths and the most common cancer worldwide. 1 EC mainly includes adenocarcinoma and squamous cell carcinoma. Squamous cell carcinoma has a much higher incidence than adenocarcinoma and is the most common EC subtype worldwide. 2 In 2018, there were approximately 572,000 new cases of EC worldwide, among which squamous carcinoma accounted for approximately 482,000 cases (84%).1,2 In addition, patients with EC were most likely diagnosed with unresectable, advanced, recurrent, or metastatic esophageal squamous cell carcinoma (ESCC). Compared to esophageal adenocarcinoma, patients with ESCC have a poor prognosis, with a 5-year relative survival rate of approximately 5.2%. 3 Currently, there are limited treatment options for patients with advanced ESCC. Guidelines recommend systemic chemotherapy with fluorouracil or paclitaxel plus platinum; however, the therapeutic effect of these treatments is not ideal. 4
Immune checkpoint inhibitors (ICIs) can amplify or eliminate immune system signals and control immune responses by blocking the binding of programmed death-ligand 1 (PD-L1) and programmed death 1 (PD-1) proteins to tumor cells and T cells, respectively.5,6 Currently, ICI-based antibody therapies are being used to treat a variety of solid tumors and have shown good efficacy. The potential benefits of therapies that combine ICIs with other drugs have been continuously explored in clinical practice.5–7
Nivolumab is a highly effective PD-1 inhibitor. In 2015, nivolumab was approved by the Food and Drug Administration for the treatment of previously treated advanced squamous non-small-cell lung cancer, and it has also shown efficacy against other advanced solid tumors.8–10 CheckMate-648 was a large, phase III, randomized, open-label clinical trial (NCT03143153) that had used a web-based interactive response technique for randomization and was conducted at 190 institutions in 24 countries worldwide. The trial explored the efficacy and safety of nivolumab plus chemotherapy (NC), nivolumab plus ipilimumab (NI), and chemotherapy (C). A total of 970 patients with advanced ESCC were randomly assigned to three arms: NC, NI, and C. The median overall survival (OS) was 13.2, 12.7, and 10.7 months in the overall population and 15.4, 13.7, and 9.1 months in the subgroup (patients with tumor cell PD-L1 expression of ⩾1%) in the NC, NI, and C arms, respectively. The median progression-free survival (PFS) was 5.8, 2.9, and 5.6 months in the overall population and 6.9, 4.0, and 4.4 months in the subgroup in the NC, NI, and C arms, respectively. 11 The results showed that NC and NI significantly improved OS and PFS in patients with advanced ESCC. Although there are significant clinical benefits of combined chemotherapy, the high cost of nivolumab and ipilimumab may impose a heavy burden on society, healthcare systems, and families. Therefore, cost-effectiveness data must be measured in terms of the economic impact of NC or NI versus chemotherapy.
The present study investigated the economic outcomes of implementing NC or NI regimens as a first-line treatment for patients with advanced ESCC from third-party payers in the United States and healthcare perspectives in China, representing high- and middle-income regions, respectively. We provided the following articles according to the request of the CHEERS 2022 report list. 12
Materials and methods
Population
Targeted population
This study utilized the sample characteristics of the CheckMate-648 clinical trial: participants were aged ⩾18 years (median age, 63–64 years); had unresectable, advanced, recurrent, or metastatic EC (regardless of PD-L1 expression status); and had not received prior systemic therapy for the disease. 11 The study was conducted in the overall population and subgroup population (patients with tumor cell PD-L1 expression ⩾1%). 11
Interventions
According to the design of the CheckMate-648 clinical trial, patients were randomly assigned to receive nivolumab (intravenous 240 mg every 2 weeks) plus chemotherapy (4 weeks as the treatment cycle; intravenous fluorouracil 800 mg/m2 on days 1–5 and intravenous cisplatin 80 mg/m2 on day 1 of each treatment cycle), nivolumab (intravenous 3 mg/kg every 2 weeks) plus ipilimumab (intravenous 1 mg/kg every 6 weeks), or chemotherapy alone. Treatment was continued until the progression of the disease, the occurrence of unacceptable toxic effects, the withdrawal of consent, or the end of the trial. Patients can be treated with NC or ipilimumab for up to 2 years. 11
Model
Model approach
The model of cost-effectiveness analysis (CEA) was based on a partitioned survival structure that determined the proportion of members in each status from the survival curves. 13 This is the method most commonly used by National Institute for Health and Clinical Excellence (NICE) to currently evaluate advanced or metastatic cancer interventions. 13 Survival data in each arm were digitally extracted from the survival curves of CheckMate-648 using GetData Graph Digitizer software (version 2.26; http://www.getdata-graph-digitizer.com/download.php). According to the method developed by Guyot et al. 14 , Kaplan–Meier survival curves were reconstructed using the R software (version 3.5.1) to obtain the new survival curves. Distribution functions included Weibull, log-logistic, log-normal, Gompertz, and gamma. 15 Akaike information criterion (AIC), Bayesian information criterion (BIC), and visual simulation methods were used to test the goodness of fit, and distribution functions with lower AIC and BIC and better visual simulation were selected as fitting curves to extrapolate to obtain long-term clinical survival outcomes. 16 The fitted results are shown in Supplemental Figures 1 and 2, and the selected fitting curves and data are shown in Table 1. The median OS, PFS, and tail of the selected curves were consistent with the results observed in CheckMate-648, which validated the model (Supplemental Figures 3–4).
Model parameters and ranges used in the sensitivity analyses in the United States.
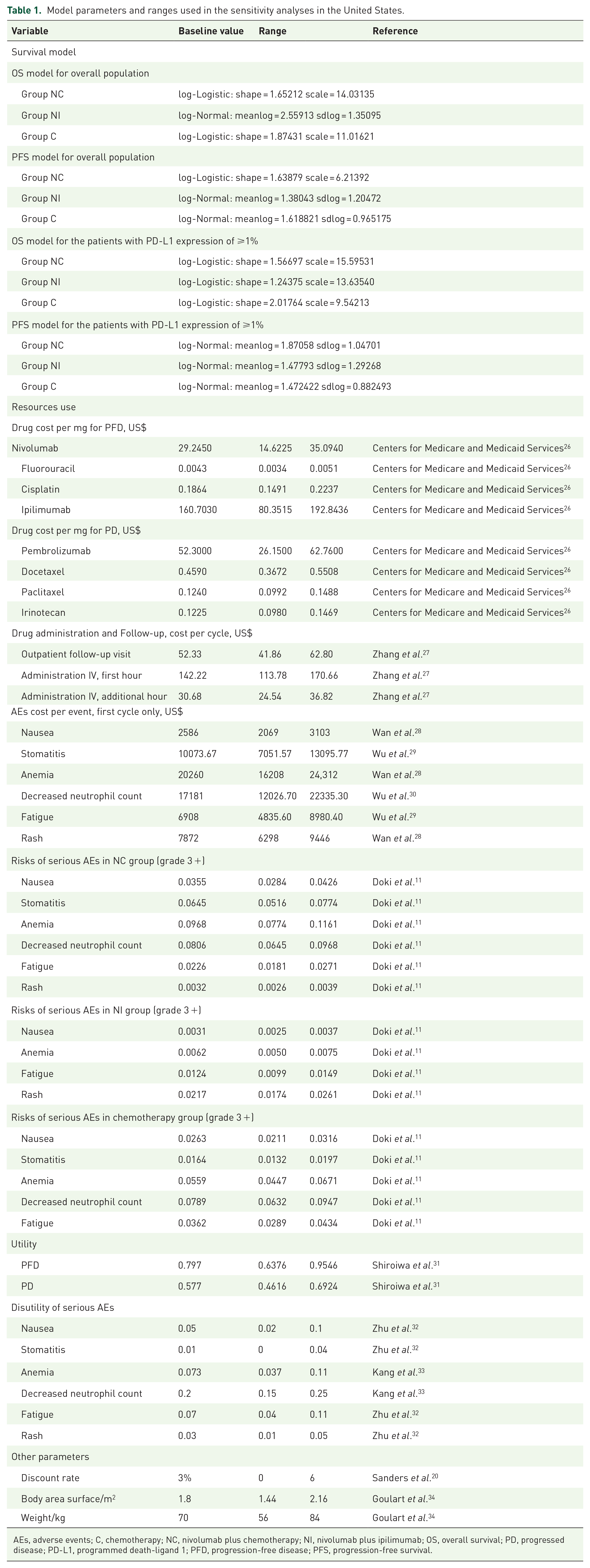
AEs, adverse events; C, chemotherapy; NC, nivolumab plus chemotherapy; NI, nivolumab plus ipilimumab; OS, overall survival; PD, progressed disease; PD-L1, programmed death-ligand 1; PFD, progression-free disease; PFS, progression-free survival.
Model structure
Based on the published literature and the recommendations of oncologists, the patients could be assigned to the three mutually exclusive health states: progression-free disease (PFD), progressive disease (PD), and death. The initial status of all patients was set as PFD. During each cycle, patients were redistributed among the three health states. The areas below the OS and PFS curves indicated the proportion of individuals who survived and patients with PFD, respectively. The area between the OS and PFS curves simulated the proportion of individuals with PD. The probability of the PFD state transition to the death state was assumed to be natural mortality.17–19 The TreeAge Pro 2020 software was used to build the model for the analysis (Figure 1). The model cycle was set at 1 month, in line with the cycle of chemotherapy. According to the survival curve of the CheckMate-648 clinical trial, the time horizon was set to 10 years, which was sufficient to model the OS of patients with advanced ESCC. Patients entered different states before death and received appropriate treatment, incurring certain treatment costs and health effects. The primary outcomes included total cost, quality-adjusted life years (QALYs), and incremental cost-effectiveness ratio (ICER), which is expressed as the cost per QALY. According to the China Guidelines for Pharmacoeconomic Evaluations and Sanders et al.’s20,21 recommendations, discount rates of 5% and 3% were used in China and the United States to discount costs and utilities. A deterministic analysis of the base case was performed.

Partitioned survival model simulating the results of the CheckMate-648 clinical trial. All patients started in the PFD and received appropriate treatment. Patients could enter the PFD state and subsequently move to the death state.
Model assumptions
According to CheckMate-648, the median treatment duration of the NC, NI, and C arms was 5.7, 2.8, and 3.4 months, respectively. Therefore, the duration of treatments for our model was assumed to be six, three, and four cycles in the NC, NI, and C arms, respectively. All patients received second-line chemotherapy after disease progression. Second-line chemotherapy regimens were formulated based on the recommendations of the NCCN Clinical Practice Guidelines in Oncology, information on systematic therapy provided by CheckMate-648, and recommendations of oncologists, which made our model assumptions more realistic and effective. 4 The regimens of arms NC and NI were assumed to be paclitaxel, docetaxel, or irinotecan monotherapy. Arm C included nivolumab or pembrolizumab monotherapy, in addition to taxane and irinotecan, and their proportions were set at 12% and 2%, respectively. According to the ATTRACTION-3 (NCT02569242) and KEYNOTE-181 (NCT02559687) clinical trials, the median treatment duration of nivolumab and pembrolizumab as a second-line treatment was 2.6 and 4 months, respectively, for patients with advanced ESCC.22,23 Therefore, the duration of nivolumab and pembrolizumab after progression was estimated to be three and four cycles, respectively, in the C arm.
Cost
All model inputs for the United States are listed in Table 1, and the model parameters of China are listed in Supplemental Table 1. Only direct medical costs were considered in our study, including drug, drug administration, management of adverse events (AEs), follow-up costs, relapse, and subsequent second-line treatments. Chinese drug costs were obtained from Yaozh.com, and the median prices in the last 5 years across the country were adopted. 24 These were converted into US dollars at an average exchange rate of the Renminbi in 2021 (6.4515 Renminbi per US dollar). 25 The US drug costs were obtained from the Medicare part B drug average sales price provided by the Centers for Medicare & Medicaid Services, and the administration costs were obtained from the Medicare Physician Fee Schedule.26,27 The infusion times for nivolumab, ipilimumab, and chemotherapy were 0.5, 0.5, and 8.5 h, respectively. Therefore, the duration of regimens of each cycle was 9, 1, and 8.5 h for arms NC, NI, and C, respectively. Second-line chemotherapy drugs were divided into irinotecan and taxane in arms NC and NI, with equal chances of using either of the two after progression. To exclude this assumption from the results, a one-way sensitivity analysis was performed on the proportion of different treatment options after progression. All other costs were derived from the available literature. Only grade 3 or 4 AEs with an incidence of >3% and a difference in the incidence of >2% between the arms were considered in our study. The management costs of AEs per cycle were calculated as the product of the probability of AEs and their management cost. The AE costs were only applied to the first cycle of the model and were assumed to occur only once a month.
Utility
All model inputs concerning utility are listed in Table 1. At present, there is no relevant literature on the health utility values of PFD and PD in patients with ESCC. Therefore, our study adopted the health utility value of gastric cancer, which is similar to ESCC. The utility value of the PFD state was 0.797, which was calculated using the Japanese scoring algorithm based on the EuroQoL (EQ-5D) responses of the ToGA trial. 31 The utility value of the PD state was 0.577, which was adopted based on the NICE technology appraisal 208. 31 The utilities of AEs were derived from the published literature. The utility of AEs per cycle was calculated as the product of the AE probability and utility.
Sensitivity analysis
A one-way sensitivity analysis was used to assess the influence of different parameters on the stability of results. The median price of nivolumab, ipilimumab, and pembrolizumab fluctuated 50% downward and 20% upward as the variation range of the cost. The variation ranges of administration cost, follow-up cost, AEs cost, utility, discount rate, body surface area, and body weight were obtained from the published literature. The remaining parameters were varied by 20% as the variation range for these parameters. The results were presented as tornado diagrams.
Second-order Monte Carlo simulations were used for probabilistic sensitivity analyses. According to the recommendations of the ISPOR-SMDM Modeling Good Research Practice Working Group, the costs, incidence of AEs and all utilities, as well as the body surface area and body weight were set to gamma, beta, and normal distributions, respectively. 35 Probabilistic sensitivity analyses were repeated 1000 times, and the results were presented as cost-effectiveness acceptability curves and incremental cost-effectiveness scatter plots. The willingness-to-pay (WTP) threshold of China was $37,654 (three times per capita gross domestic product of China in 2021) according to the China Guidelines for Pharmacoeconomic Evaluations, and the WTP of the United States was $100,000 and $150,000, as suggested by Neumann et al.21,36
Results
Base case results
The basic CEA results are shown in Table 2. In the United States, NI was increased by 0.44 and 0.64 QALY with an additional cost of $67,519.13 and $66,246.66, respectively, compared to the features of chemotherapy, which led to an ICER of $155,159.82/QALY and $104,297.07/QALY gained in the overall population and subgroup, respectively. The ICER for the subgroup was between the WTP thresholds of the US ($100,000/QALY and $150,000/QALY), and the other case was above the threshold of $150,000/QALY. NC increased by 0.02 and 0.08 QALY with the additional cost of $12,901.65 and $15,918.81 compared to chemotherapy, which led to an ICER of $518,062.85/QALY and $193,169.49/QALY gained in the overall population and subgroup, respectively. Both ICER values were significantly higher than the threshold value of $150,000/QALY.
The results of the base case analysis.
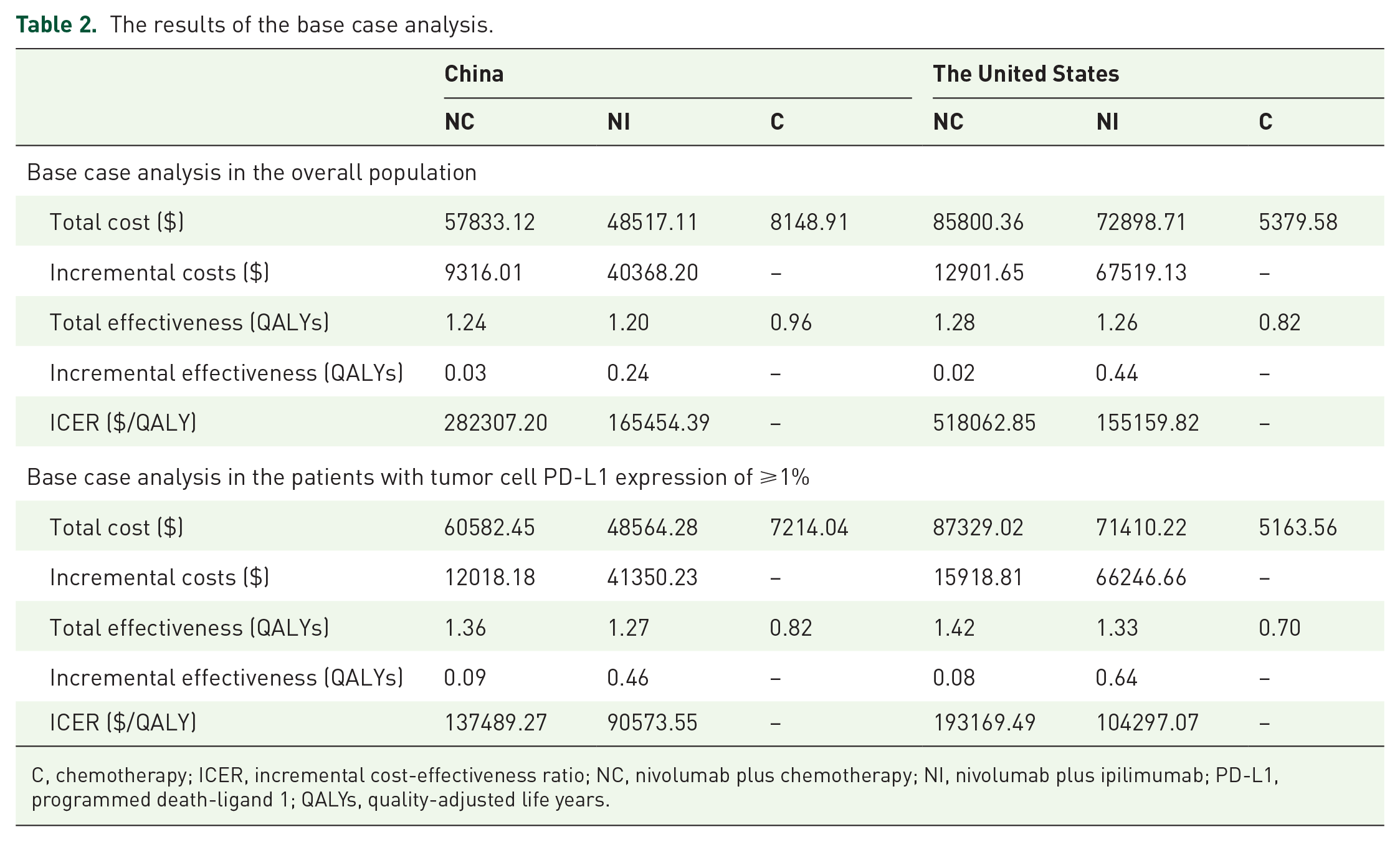
C, chemotherapy; ICER, incremental cost-effectiveness ratio; NC, nivolumab plus chemotherapy; NI, nivolumab plus ipilimumab; PD-L1, programmed death-ligand 1; QALYs, quality-adjusted life years.
For patients with advanced ESCC in the overall population and subgroup, the ICER values for NI (compared to chemotherapy) and NC (compared to NI) were higher than $90,000/QALY, significantly exceeding the WTP threshold of China ($37,654/QALY).
One-way sensitivity analysis
The results of the one-way sensitivity analysis are shown in Figure 2. In the United States, the main influencing factors included the cost of nivolumab, discount rate, and patients’ weight in the overall population. The subgroup analysis was most sensitive to the cost of nivolumab and ipilimumab and the patients’ weight. Some additional parameters, including the utility of PFS and PD, and the cost and probability of AEs, such as anemia in the NC group had also a slight impact on the ICER.

Tornado diagrams of one-way sensitivity analyses. a and b were the results for the overall population and the subgroup in China, respectively; c and d were the results for the overall population and the subgroup in the United States, respectively. The dotted line intersecting the blue and red bars represents the ICER of base case results.
In China, the cost of paclitaxel and fluorouracil and the discount rate were the main factors influencing the ICER in the overall population. Some additional factors, including the cost of nivolumab and docetaxel and the weight of patients, also had a slight effect on the ICER. For the subgroup, the cost of fluorouracil and nivolumab and patients’ weight were the main influencing factors, and additional parameters, including the utility of PFS and the cost of ipilimumab and paclitaxel, had a slight impact on ICER.
Probabilistic sensitivity analysis
All the results of the probabilistic sensitivity analysis are shown in Figure 3 and Supplemental Figures 5 and 6. For patients with advanced ESCC in the United States, the cost-effectiveness acceptability curve at a WTP threshold of $100,000/QALY showed nearly 0.9% and 9.1% probabilities of NC (compared to NI) and NI (compared to chemotherapy), respectively, as a cost-effective strategy in the overall population, and 15.4% and 41.9% probabilities of being a cost-effective strategy in the subgroup, respectively.
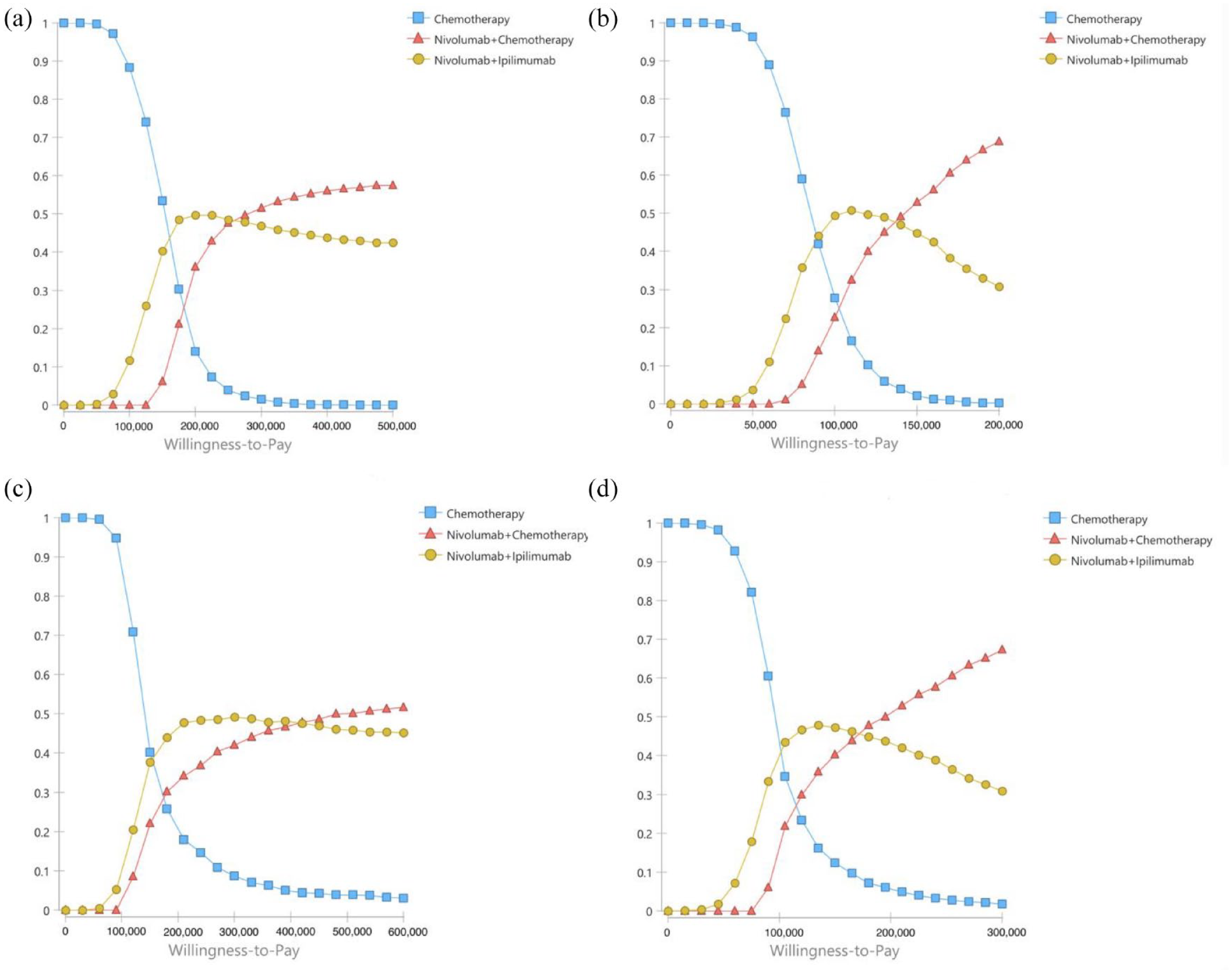
Cost-effectiveness acceptability curves. a and b were the results for the overall population and the subgroup in China, respectively; c and d were the results for the overall population and subgroup in the United States, respectively.
The cost-effectiveness acceptability curve at a WTP threshold of $150,000/QALY showed nearly 23.2% and 37.9% probabilities of NC (compared to NI) and NI (compared to chemotherapy) as a cost-effective strategy in the overall population, respectively, and 40.9% and 46.6% probabilities of being a cost-effective strategy in the subgroup, respectively.
For patients with advanced ESCC in China, the cost-effectiveness acceptability curve showed a <1% probability of NC (compared to NI) and NI (compared to chemotherapy), which is a cost-effective strategy at the threshold of $37,654/QALY in either the overall population or subgroup.
Discussion
According to the CheckMate-648 clinical trial, NC or NI significantly improved the OS and PFS of patients with advanced ESCC. However, nivolumab and ipilimumab are relatively expensive to administer. In the United States, our base case results showed that NI was a favorable option compared to chemotherapy in the subgroup with a WTP threshold of $150,000/QALY, and there was no such advantage at the WTP threshold of $100,000/QALY. The ICER values of NC and NI were $518,062.85/QALY and $193,169.49/QALY in the overall population and subgroup, respectively, both of which were higher than the WTP threshold of $150,000/QALY. Therefore, NC may not be a cost-effective option in the United States. In China, combination therapy with nivolumab is not a cost-effective option because the ICER of all treatments was higher than $90,000/QALY, regardless of the overall population and subgroup, which significantly exceeded the WTP threshold of $37,654/QALY.
Our findings are similar to those of the two recent economic analyses of ICIs for the treatment of advanced ESCC. Both studies were conducted from the Chinese perspective. A study of camrelizumab plus chemotherapy as a first-line treatment showed that this combination produced an ICER of $46,671.10/QALY compared to chemotherapy, which was higher than the WTP threshold of China. 37 Another economic analysis of nivolumab alone as a second-line treatment showed that the ICER generated by nivolumab versus chemotherapy was $136,709.35/QALY, which was also higher than the WTP threshold in China. 38 The results of these studies suggest that the addition of nivolumab to chemotherapy may not be a cost-effective option in Chinese patients with advanced or metastatic ESCC, which is consistent with our findings.
The Chinese model results were most sensitive to the cost of paclitaxel. The potential reasons are that all patients entering the PD state were administered second-line chemotherapy (except for pembrolizumab and nivolumab) until death, and the variation range of the cost of paclitaxel included the price of relatively expensive dosage forms such as liposomes. The second reason is the cost of fluorouracil because of the large variation range of cost and the high dosage of fluorouracil (800 mg/m2, days 1–5 per cycle).
The US model was more sensitive to the cost of nivolumab. The baseline cost and range of variation of paclitaxel and fluorouracil were small, whereas nivolumab was expensive and had a large range of variation. Ipilimumab is the most expensive drug, but all sensitivity analyses showed that the cost of ipilimumab had a slight impact on our study results. In addition, the total cost and total effectiveness of NI were lower than those of NC. The potential reason may be that the median PFS and OS of the NI arm were 2.9 and 12.7 months, respectively, in the overall population and 4.0 and 13.7 months in the subgroup, respectively, which were lower than those in the NC arm (the median PFS was 6.9 and 5.8 months and the median OS was 13.2 and 15.4 months in the overall population and subgroup, respectively). 11 Therefore, patients treated with NI progressed faster and received the drugs for a shorter time than those treated with NC.
This is the first analysis to evaluate the economics of NC or NI as the first-line treatment for patients with advanced ESCC through economic modeling approaches and provides latest evidence that may provide a reference for the formulation of related medical insurance policies and clinical decision-making. Our study analyzed the economic results for the United States and China, which are representatives of developed and developing countries, respectively; hence, our results can be applied to other developed and developing countries and regions. However, our study has some limitations. First, there is uncertainty in the estimation of the utility values of PFD and PD. Currently, there were limited studies on the economic evaluation of the treatments applied in patients with advanced ESCC. Only eight references were retrieved from PubMed, of which seven and eight focused on second- and first-line treatments, respectively, for patients with advanced ESCC. However, the utility of PFD and PD as a first-line treatment was not reported in the literature. 35 In addition, the utility of PFD and PD as a second-line treatment differed significantly from that as a first-line treatment. Therefore, we used the utility of PFD and PD for advanced gastric cancer as a first-line treatment, which is similar to advanced EC, as model parameters. 31 Second, the costs of managing grade 1 and 2 AEs were not included in this study, and some AEs were adopted from other types of cancer, which might have influenced the results; however, sensitivity analysis showed that these AEs had a slight effect. Third, the second-line treatments and proportion of patients receiving corresponding drugs were formulated for patients entering the PD state according to the systematic therapy information provided by the CheckMate-648 clinical trial and NCCN Clinical Practice Guidelines in Oncology, which may not be consistent with actual clinical practice. Finally, the majority of patients in our study were from Asian countries [680/970 (70%)], which might have led to bias in the model results.
Although the above-mentioned factors may have restricted the application in our study, the utility of PFD, PD, and AEs had a slight impact on the results according to the sensitivity analysis. Therefore, our study may serve as a valuable reference for doctors and policymakers, reflecting the general clinical treatment of patients with advanced ESCC.
Conclusion
Under a WTP threshold of $150,000, NI is more cost-effective than NC or C alone for treating advanced ESCC with PD-L1 expression of ⩾1% in the United States. In addition, NC or NI is not a cost-effective option in either the United States or China.
Supplemental Material
sj-docx-1-tam-10.1177_17588359221122733 – Supplemental material for First-line nivolumab plus ipilimumab or chemotherapy versus chemotherapy alone for advanced esophageal cancer: a cost-effectiveness analysis
Supplemental material, sj-docx-1-tam-10.1177_17588359221122733 for First-line nivolumab plus ipilimumab or chemotherapy versus chemotherapy alone for advanced esophageal cancer: a cost-effectiveness analysis by Xueqiong Cao, Hongfu Cai, Na Li, Bin Zheng, Zhiwei Zheng and Maobai Liu in Therapeutic Advances in Medical Oncology
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.