
Abstract
Background:
Classic Kaposi’s sarcoma (CKS) is a rare, multifocal, endothelial cell neoplasm that typically occurs in elderly people with previous infection by human herpes virus-8. Prospective trials are rare, and the choice of drugs relies on prospective trials performed on HIV-associated Kaposi’s sarcoma (KS). Pegylated liposomal anthracyclines and taxanes are considered the standard first- and second-line chemotherapy, respectively. Despite the indolent biologic behavior, the natural history is characterized by recurrent disease. This condition of chronic administration of cytotoxic drugs is often associated with immediate/long-term adverse events.
Methods:
This was an observational, retrospective study to evaluate the effectiveness and safety of gemcitabine in patients with CKS. From January 2016 to September 2021, the patients were treated with gemcitabine 1000 mg/m2 on days 1 and 8, with cycles repeated every 21 days. The treatment was administered as first or second line.
Results:
Twenty-seven (27) patients were included in the study. Twenty-one (21) out 27 patients (77.8%) achieved a partial response (PR), including 8 patients with major response (MR) (29.6%) and 13 patients with minor response (mR) (48.2%); 2 (7.4%) showed a complete response (CR), 3 (11.1%) a stable disease (SD), and 1 (3.7%) a progressive disease (PD). Tumor responses were generally rapid, with a median time to first response of 4 weeks (range, 3–12 weeks). Patients who responded had disease improvement with flattening of the skin lesions, decrease in the number of lesions, and substantial reduction in tumor-associated complications. Median duration of response was 19.2 months. Common adverse events were grades 1/2 thrombocytopenia, and grade 1 noninfectious fever. No patient discontinued treatment as a result of adverse events.
Conclusion:
Our study showed that gemcitabine is effective and well tolerated, acts rapidly on cutaneous lesions, and allows substantial symptom palliation, without dose-limiting toxicity. Gemcitabine represents a safe and effective option for the treatment of CKS.
Keywords
Highlights
Classic Kaposi’s sarcoma (CKS) is featured by several unmet clinical needs.
Prospective trials are rare, and the choice of drugs relies on prospective trials performed on HIV-associated Kaposi’s sarcoma (KS).
Pegylated liposomal anthracyclines and taxanes are considered the standard first- and second-line chemotherapy.
Most patients need treatment, at least intermittently, for years, often with associated immediate/long-term adverse events.
Gemcitabine is effective and well tolerated, acts rapidly on cutaneous lesions, and allows substantial symptom palliation.
Introduction
Kaposi’s sarcoma (KS) is a rare, multifocal, endothelial cell neoplasm with an inflammatory component and highly heterogeneous clinical behavior. 1 Previous infection by human herpes virus-8 (HHV), also called KS herpesvirus (KSHV), is mandatory to the neoplasm development. 2 Viral infection is necessary, but not sufficient, in the multistep pathogenesis of KS. 3
Four clinical subtypes are known: classic, endemic, epidemic, and iatrogenic. Treatment of KS depends on the KS variant and the extent of the disease. 4 The epidemic subtype, observed in patients infected with the HIV, is the most studied.4,5 The HIV-associated subtype may follow an aggressive course, and visceral involvement is not uncommon. 6 The treatment with antiretroviral therapy (ART), reducing the immunosuppression, may cause regression of the early-stage tumors and represents often the first-line therapeutic approach.6 –8 In patients with HIV-associated KS, who had advanced disease and incomplete response to ART, several chemotherapeutic agents have been shown to have activity. 9 The recommended options are pegylated liposomal anthracyclines (PLD) and paclitaxel, showing response rates ranging from 46% to 76%.10 –12
Classic Kaposi’s sarcoma (CKS) typically occurs in elderly people of specific areas, such as the Mediterranean; it is usually featured by skin lesions, often at lower limbs, without visceral involvement, and has a chronic course that requires systemic chemotherapy for locally aggressive extensive disease. 13 In HIV-negative patients, prospective trials are rare, and published data include mostly retrospective series.14 –16 Thus, systemic treatment is less established, and the choice of drugs relies on prospective trials performed on HIV-associated KS. 17 In these patients, chemotherapy remains a mainstay of treatment. Several unmet clinical needs exist. Incidence of the classic KS exponentially increases with age; 18 despite the indolent biologic behavior and the frequent slow evolution, the natural history is characterized by recurrent disease. Most patients with CKS need treatment, at least intermittently, for years, often with the same chemotherapeutic agents. This condition of chronic administration of cytotoxic drugs is often associated with immediate and long-term adverse events. 19 Cytopenia is frequent toxicity; cumulative doses of liposomal doxorubicin increase potential anthracycline-induced cardiotoxicity, 20 and the hand-foot syndrome could worsen the evolution of the disease, mainly cutaneous and localized at the extremities in the classic subtype. Therefore, a key goal of KS treatment is to induce sustained remission using drugs that have a good safety profile. Gemcitabine is a cytotoxic agent characterized by a favorable toxicity profile and used for the treatment of a broad spectrum of tumors. 21 Interestingly, in the context of sarcomas, gemcitabine showed activity in the treatment of advanced vascular sarcomas, including angiosarcoma, epithelioid hemangioendothelioma, and intimal sarcoma.22 –25 Based on this background, gemcitabine could represent a rational therapeutic approach in classic Kaposi sarcoma.
Methods
Patient selection
Patients included in the study were adults with a pathologically confirmed diagnosis of KS, at least five evaluable skin lesions, absence of visceral involvement, symptomatic disease, and indication for systemic therapy. The study participants were HIV-negative, with age less than 90 years, Eastern Cooperative Oncology Group (ECOG) performance status of 0–2, a life expectancy ⩾6 months, an adequate bone marrow reserve with absolute neutrophil count (ANC) >1000 cells/ml, platelet count >100,000 cells/ml, hemoglobin >9 g/dl, and no renal or hepatic failure. The stages eligible for the study were stage II A (infiltrating) slow variant with complications, stage II B rapid variant, stage III (florid), and stage IV (disseminated), according to criteria by Brambilla et al. 26 Complications included lymphedema, lymphorrhea, pain, functional impairment, ulceration, and hemorrhage.
The evolution of disease, slow or rapid, was detected. Rapid progression was defined as an increase in the number or total surface area of KS lesions (nodules/plaques) over 3 months.
Patients may have received none or one prior systemic therapy.
Study design
This was an observational retrospective, single-institution study conducted from January 2016 to September 2021 in an Italian referral center for diagnosis and treatment of Soft Tissue Sarcoma: the ‘Sicilian Regional Center for the Prevention, Diagnosis and Treatment of Rare and Heredo-Familial Tumors’ of the University Hospital Policlinico ‘Paolo Giaccone’ of Palermo.
Patients received gemcitabine 1000 mg/m2 as 30 min intravenous infusion, on days 1 and 8, with cycles repeated every 21 days. Gemcitabine was administered for a maximum of 6 months; the early discontinuation occurred for progressive disease (PD), complete response (CR), life-threatening events, or patient preference. Patients with recurrent disease after previous discontinuation for objective response to gemcitabine could continue the treatment with the same schedule for up to six cycles.
Protocols were approved by the ethical committee of the University-affiliated Hospital A.O.U.P. ‘Paolo Giaccone’ (approval number 21-15092021), and the study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines.
Response assessment
There is no universally accepted staging classification for classic KS, and the only validated system was elaborated from the AIDS Clinical Trials Group (ACTG) Oncology Committee.27,28 These criteria are certainly useful for AIDS-associated KS, but are not established for the classic subtype. Therefore, the revised World Health Organization (WHO) criteria were used.28,29 This response assessment system was based on the number of skin lesions and reductions in tumor-associated complications, which are often present when there is an objective reduction of cutaneous lesions. Objective response was assessed every two cycles. Tumor-associated complications were evaluated every cycle. Evaluations included clinical observation accompanied by photographic documentation, with cutaneous lesion counts, assessment of the number of nodular lesions, measurement of the diameters of five indicator skin lesions, and measurement of limb circumference to evaluate the tumor-associated lymphedema. KS responses were categorized as complete response (CR), major response (MR), minor response (mR), stable disease (SD), or progression disease (PD).
CR required the clinical resolution of all lesions and tumor-associated phenomenon. CR had to be sustained for 8 weeks. MR was defined as a ⩾50% to <100% decrease in the number of measurable lesions and absence of new skin lesions lasting for at least 8 weeks. mR was defined as >25% to <50% decrease in the number of lesions and absence of new lesions lasting for at least 8 weeks. SD was defined as <25% decrease to <25% increase. PD required >25% increase in the number of lesions or worsening of tumor-associated complications, or the appearance of new lesions.
AE assessment
Treatment-related toxicity was monitored during each cycle and 4 weeks after completing therapy, or until resolution, using the National Cancer Institute Common Toxicity Criteria (version 4.0).
Statistical considerations
The main objective of this study was to determine the overall response rate (ORR), the duration of response, and the safety profile of gemcitabine, to predict the clinical benefits experienced by the patients with CKS. ORR included CRs plus MRs and mRs. Time to treatment failure (TTF), defined as time from day 1 of gemcitabine therapy until disease progression requiring a change in therapy, was estimated using the Kaplan–Meier method. Duration of response was calculated among responder patients and defined as time from response on gemcitabine therapy until progression of cutaneous lesions over treatment or follow-up. 30
Results
Patients
Between January 2016 and September 2021, 27 consecutive KS patients with classic variant, HIV-negative, were included in the study (Figure 1). All patients were Caucasians, from Mediterranean countries. The median age was 74 (range, 54–88 years). Twenty-two (22) out of 27 (81.5%) were male, 5 were female (18.5%). Florid cutaneous stage (III) was the most common (13 patients, 48.1%), followed in frequency by infiltrative stage (II) (12 patients, 44.5%), and disseminated (IV) (2 patients, 7.4%). Eight (8) patients (29.6%) showed a rapid evolution of disease: 1 patient in infiltrative stage, 4 patients in florid stage, and 2 patients in disseminated stage. Cutaneous distribution of macules, plaques, and nodules were frequent in limbs (15 patients, 55.6%) or lower limbs (8 patients, 29.6%). An involvement of limbs and trunk was seen in three patients (11.1%), while only one patient (3.7%) showed the most widespread skin lesions in limbs, trunk, and head. Lymph node metastatic disease was for two patients in disseminated stage; all other patients did not show visceral metastasis. Eleven (11) patients (40.7%) were treated with gemcitabine as first line of systemic chemotherapy; 16 (16) patients (59.3%) were previously treated for KS with liposomal doxorubicin (Table 1). All patients were evaluable for response.
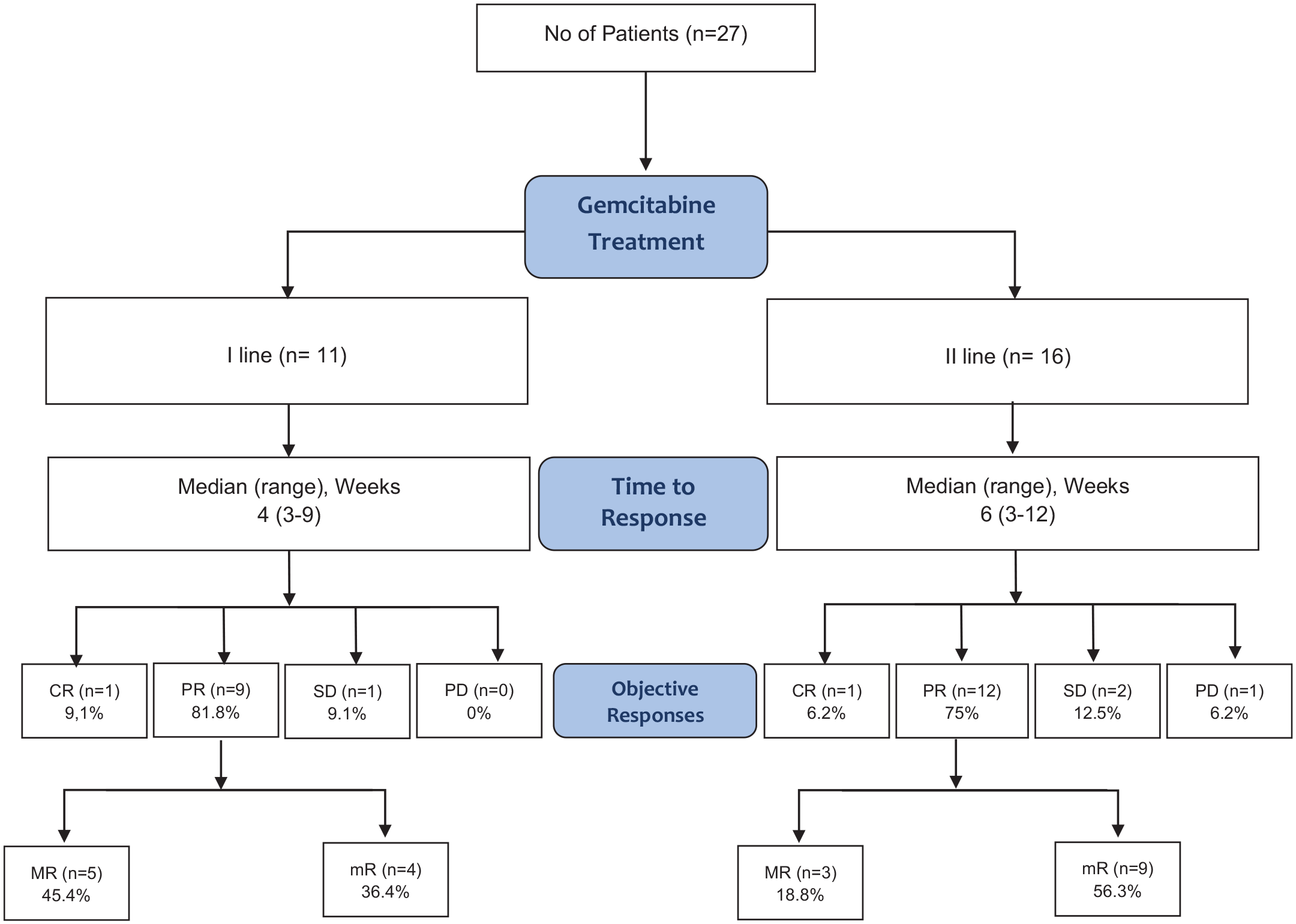
Consort flow diagram.
Patient and disease characteristics.

KS, Kaposi’s sarcoma.
Cutaneous staging system based on objective criteria by Brambilla et al.: 26 I. Maculonodular: Nodules or macules or both; II. Infiltrative: Plaques; III. Florid: Angiomatous nodules and plaques; IV. Disseminated angiomatous nodules and plaques.
Rapid evolution is defined as an increase in number of nodules/plaques or in total surface area of KS skin lesions over 3 months.
Effectiveness
Twenty-three (23) out 27 patients with CKS achieved objective tumor responses, for an ORR of 85.2% [95% confidence interval (CI), 64% to 96%], including two patients (7.4%) who achieved CRs. Ten (10) out of 11 patients who were treated with gemcitabine as first-line therapy achieved objective responses (ORR, 90.9%; 95% CI, 69% to 100%); 13 out of 16 patients previously treated achieved objective tumor responses during gemcitabine treatment as second-line therapy (ORR, 81.2%; 95% CI, 64% to 96%) (Table 2).
Objective responses and timing of responses.

CR, complete response; KS, Kaposi’s sarcoma; PD, progressive disease; PR, partial response; SD, stable disease; WHO, World Health Organization.
CR and PR are objective tumor responses by WHO Criteria, modified and adapted for classic KS form.
Several patients (21 patients, 77.8%) showed a partial response (PR), including 8 patients with MR (29.6%) and 13 (48.2%) with mR. Patients who responded had a substantial disease improvement with flattening of the skin lesions and a decrease in the number of lesions (Figure 2).

Waterfall plots showing individual responses to gemcitabine therapy. The horizontal axis across the plot shows the baseline number of cutaneous tumor lesions; vertical bars are drawn for each patient, either above or below the baseline, according to maximum percent change of the tumor growth or reduction from baseline. Vertical bars above the baseline represent the progressive disease; vertical bars below the line represent the tumor reduction degree in the number of skin lesions (minor response, major response, or complete response).
Patients showing an objective tumor response after gemcitabine treatment also had a reduction in tumor-associated complications: 17 of 25 patients with lymphedema (68%) had a decrease in limb circumference; 14 of 22 patients (63.6%) showed an evident lymphorrhea reduction; 10 of 15 patients (66.7%) had an improvement of pain, and 12 of 15 patients (80%) had an improvement of tumor-associated functional impairment (Table 3).
Most frequent tumor-associated complications and decrease after gemcitabine treatment, assessed at the best response achievement.

At least a 2-cm reduction of limb circumference.
Tumor responses were generally rapid, with a median time to first response of 4 weeks (range, 3–12 weeks); considering the group of patients according to the previous systemic chemotherapy, the same time of 4 weeks (range, 3–9 weeks) was in the first-line group of patients, while a time to response of 6 weeks (range, 3–12 weeks) was in the second-line subgroup.
The median duration of response was 19.2 months; 21.6 months was in the first line group of patients, and 17.8 months in the second line group.
After achievement of best objective response, 17 patients (62.9%) [I line: 6 patients (54.5%), II line: 11 patients (68.7%)], were retreated with further cycles of gemcitabine (median 6 cycles) due to PD (increased number of measurable skin lesions) or worsening in tumor-associated complications. During this second course of therapy, 11 out 17 patients (64.7%) had a new PR as assessed from the initiation of the second course [I line: 4 patients (66.7%), II line: 7 patients (63.6%)], 3 had SD (17.65%) [I line: 1 patient (16.7%), II line: 2 patients (18.2%)], and 3 had PD (17.65%) [I line: 1 patient (16.7%), II line: 2 patients (18.2%)].
Overall median TTF was 27 months (95% CI: 18.8–35.1). Median TTF was 28 months (95% CI: 26.5–29.5) for the first line group of patients, and 19 months (95% CI: 8.4–29.6) for the second line group of patients (Figure 3).

TTF curves according to first or second line of gemcitabine treatment.
Adverse events
Gemcitabine was well tolerated and the safety profile was consistent with previous clinical studies in other cancer populations (Table 4). Common adverse events were grades 1 to 2 thrombocytopenia (G1, 12 patients, 44.4%; G2, 5 patients, 18.5%), and grade 1 noninfectious fever, not attributable to neutropenia (10 patients, 37%), mainly in the first two cycles of therapy. Other mild and self-limited adverse events were fatigue (G1, 8 patients, 29.6%; G2, 4 patients, 14.8%), anemia not requiring transfusion (G1, 5 patients, 18.5%; G2, 3 patients, 11.1%), and neutropenia (G1, 3 patients, 11.1%). The infections developed included one patient with soft tissue infection, and one patient with upper respiratory tract infection requiring oral antibiotics. There were no episodes of febrile neutropenia. No secondary malignancies were found. No patient discontinued treatment as a result of adverse events.
Adverse events by CTCAE (version 4.0).

CTCAE, Common Terminology Criteria for Adverse Events; AST, Aspartate Aminotransferase; ALT, Alanine Aminotransferase.
CTCAE Grade 2 adverse events or higher, and Grade 1 occurred in >10% of cycles, possibly, probably, or definitely related to treatment with gemcitabine.
Discussion
The sporadic or classic KS subtype is a rare tumor. 31 Its incidence is affected by factors such as sex, immunosuppression, and geographic origin, and it is higher in Mediterranean countries, characterized by medium/high HHV8 seroprevalence. 18 The incidence exponentially increases with age, thus, classic KS is mainly a tumor of the elderly population. 32
Visceral, lymph node, and mucosal involvement are more frequent in AIDS-associated and post-transplant KS, resulting in widespread and life-threatening clinical variants. Whereas multiple bilateral cutaneous macules, plaques, and nodules of the lower limbs, without extensive visceral/nodal involvement, are the typical clinical presentation of classic subtype. 4 Despite the frequent indolent course and the slow evolution of classic KS, these patients present a long-time compromised quality of life due to the presence of many tumor-associated complications such as pain, functional impairment, ulceration, and hemorrhage, in addition to frequent lymphedema and lymphorrhea. 33 Therefore, an important objective of systemic treatment is not only to achieve disease control but also a substantial symptoms reduction, preserving the quality of life. 34 Considering the advanced age of the classic KS population, chronic administration of cytotoxic agents is often poorly tolerated.
The treatment options in classic KS are less codified than the HIV-related variant. High-quality evidence from prospectively designed clinical trials is lacking, and generally based on small retrospective studies.14 –16 The current systemic therapies are similar to those used for AIDS-related KS.
Pegylated liposomal anthracyclines and weekly taxanes are considered the standard first- and second-line chemotherapy, respectively. 33 The adverse events of liposomal doxorubicin include around 5% of grade IV neutropenia and 5% of hand-foot syndrome; the latter could further aggravate the skin lesions of the extremities of the limbs, becoming dose-limiting toxicity for PLD.14,15,35 Despite PLD is associated with a significantly reduced incidence of cardiotoxicity compared with the conventional doxorubicin, chronic infusion in elderly patients, who often are carriers of cardiovascular risk factors and comorbidities, could impact long-term cardiac safety.35,36 Paclitaxel shows greater neurotoxicity and alopecia, and more grade III and IV toxicity than PLD, particularly grade IV neutropenia.11,16 Therefore, a drug with limited side effects, such as gemcitabine, is a rational candidate for the classic KS treatment.
Gemcitabine is a fluorinated pyrimidine nucleoside analog with antitumor activity against a broad spectrum of solid tumors, 21 characterized by a favorable toxicity profile. Notably, gemcitabine is particularly active in sarcomas of vascular origin, representing a therapeutic option for the histology-driven treatment of angiosarcoma, epithelioid hemangioendothelioma, and intimal sarcoma.22 –25,37 Furthermore, we knew that gemcitabine does not have dose-limiting toxicity. Thus, in a neoplasm with an indolent course, with a long life expectancy, this element represents a great advantage.
To our knowledge, this research represents the largest study of gemcitabine in classic KS. Our data demonstrate that gemcitabine at a dosage of 1000 mg/m2 on days 1 and 8, with cycles repeated every 21 days, is effective and tolerable in patients with classic KS, both in the first and second line of treatment.
The overall ORR was 85.2%, including two patients who achieved CRs. Responses were particularly evident in patients treated with gemcitabine as the first systemic cytotoxic therapy, showing in this population an ORR of 90.9%. The clinical response was generally rapid and occurred with a median time to first response of 4 weeks. The complete and partial responses were characterized by flattening and clearing of cutaneous nodular lesions; purple color disappeared with residual pigmented macular lesions. The median duration of response in all population was 19.2 and 21.6 months in the first-line subgroup. Beneficial effects of gemcitabine treatment included reductions in tumor-associated complications, such as frequent lymphedema and lymphorrhea, and the improvement of pain and functional impairment. These elements contributed to a substantial quality of life preservation.
Response rates and improvement in tumor-associated symptoms are difficult to compare across published studies; often, they involve different study populations in terms of ethnicity and immune status, characterized by a highly variable clinical evolution, and used different response assessment criteria. 33 Nevertheless, the response rate observed here is substantially similar to that reported with PLD as first-line chemotherapy in a retrospective study on classic KS, 14 suggesting that gemcitabine can be a valid therapeutic approach in this setting of patients.
A further important consideration is the gemcitabine toxicity, acceptable and easily manageable than PLD or paclitaxel, also in patients who had received a previous first-line systemic chemotherapy with PLD. Treatment was well tolerated; there were no grade 3 or 4 adverse events, no episodes of febrile neutropenia, and only mild and self-limited side effects.
Conclusion
CKS is a chronic neoplasm that affects an elderly population. The current therapies for KS are not curative and are often administered for long periods. Therefore, the safety profile of systemic drugs should be a major objective of the treatment. Prospective trials are rare, and very few data are available on the benefit and tolerance of KS-specific treatment beyond PLD and paclitaxel. Our study showed that gemcitabine is effective and well tolerated, acts rapidly on cutaneous lesions, and allows substantial symptom palliation and improvement in tumor-associated complications. Therefore, it represents a safe and effective option for the treatment of classic KS.
Footnotes
Author contributions
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.