
Abstract
Introduction:
Studies of the impact of hepatitis C virus (HCV), hepatitis B virus (HBV) and HIV mono and co-infections on the risk of cancer, particularly extra-hepatic cancer, have been limited and inconsistent in their findings.
Methods:
In the British Columbia Hepatitis Testers Cohort, we assessed the risk of colorectal, liver, and pancreatic cancers in association with HCV, HBV and HIV infection status. Using Fine and Gray adjusted proportional subdistribution hazards models, we assessed the impact of infection status on each cancer, accounting for competing mortality risk. Cancer occurrence was ascertained from the BC Cancer Registry.
Results:
Among 658,697 individuals tested for the occurrence of all three infections, 1407 colorectal, 1294 liver, and 489 pancreatic cancers were identified. Compared to uninfected individuals, the risk of colorectal cancer was significantly elevated among those with HCV (Hazard ration [HR] 2.99; 95% confidence interval [CI] 2.55–3.51), HBV (HR 2.47; 95% CI 1.85–3.28), and HIV mono-infection (HR 2.30; 95% CI 1.47–3.59), and HCV/HIV co-infection. The risk of liver cancer was significantly elevated among HCV and HBV mono-infected and all co-infected individuals. The risk of pancreatic cancer was significantly elevated among individuals with HCV (HR 2.79; 95% CI 2.01–3.70) and HIV mono-infection (HR 2.82; 95% CI 1.39–5.71), and HCV/HBV co-infection.
Discussion/Conclusion:
Compared to uninfected individuals, the risk of colorectal, pancreatic and liver cancers was elevated among those with HCV, HBV and/or HIV infection. These findings highlight the need for targeted cancer prevention and diligent clinical monitoring for hepatic and extrahepatic cancers in infected populations.
Introduction
Of the 14 million cancer cases occurring globally in 2012, 2.2 million were attributed to infectious agents. 1 Hepatitis C virus (HCV) and hepatitis B virus (HBV) account for approximately 25% and 50% of all hepatocellular carcinoma (HCC) cases, respectively. 2 HIV is also associated with an increased risk of AIDS-defining malignancies (ADM), namely non-Hodgkin lymphoma. 3 In addition to ADM, the incidence of non-AIDS-defining malignancies (NADMs) is also associated with excess mortality among individuals living with HIV compared to those who are HIV-negative.4,5 Despite the current evidence, there have been limited evaluations of the impact of HCV, HBV, or HIV mono-infections on the risk of other cancers, such as colorectal and pancreatic cancers. Although colorectal cancer is the second leading cause of cancer-related death worldwide, and pancreatic cancer carries an extremely low 5-year survival rate, risk factors for these cancers, including potential associations with oncogenic viruses, have not been fully identified, requiring further investigation.6,7
The impact of co-infection with these viruses on cancer risk is an important consideration given the large number of people around the world with co-infection (e.g. 2.7 and 2.3 million people worldwide have HIV/HBV and HIV/HCV co-infections, respectively). 8 Besides HCC and ADM, only a few studies have assessed the risk of colorectal and pancreatic cancers among individuals with HCV, HBV, and/or HIV co-infection.9–14 Furthermore, in most studies conducted to date, common underlying social and behavioral acquisition risks (e.g. injection drug use, problematic alcohol use) among infected individuals in the context of ‘disease syndemics’ have been inadequately addressed.15,16 In the context of syndemic theory, the co-occurrence of HIV and HCV could act as a surrogate for risk activities, consequently leading to increased cancer risks in infected populations. 15 Finally, these studies lacked a negative-for-all infections comparison group with similar acquisition risks to evaluate the risk of cancer. 16
To address these gaps in knowledge, we used the British Columbia Hepatitis Testers Cohort (BC-HTC) to assess the risk of colorectal, liver, and pancreatic cancers among HCV, HBV, and HIV mono and co/triple-infected individuals compared to individuals who tested negative for these infections.
Materials and methods
Study population
We utilized data from the BC-HTC, which includes all individuals tested for HCV or HIV at the British Columbia Centre for Disease Control Public Health Laboratory (BCCDC-PHL), or who have been reported to public health as confirmed cases of HCV, HBV, HIV, or active tuberculosis, since 1990 (Supplemental Table 1). The BCCDC-PHL performs more than 95% of HCV and HIV serology and confirmatory testing in British Columbia (BC). Using a unique personal health number, data are linked with provincial healthcare administrative databases covering medical visits, hospitalization records, prescription drugs, cancers, and deaths. Detailed descriptions of the BC-HTC cohort are provided elsewhere.17,18
For the current analysis, we included only individuals who were tested for all three infections (HCV, HBV, and HIV), by 31 December 2015. The non-infected group included individuals tested for HCV, HBV, and HIV with no record of these infections. We excluded individuals diagnosed with cancer before the date of the first infection, individuals who were less than 18 years of age at cancer diagnosis, and individuals of unknown sex.
Infection status
Individuals testing positive for HCV antibodies, HCV RNA or genotype, or who were reported as HCV cases to public health were classified as HCV cases. 17 HBV cases included individuals who were reported as HBV cases in the provincial registry or tested for HBV DNA or hepatitis B virus surface antigen (HBsAg), or individuals who received HBV treatment. 17 HIV diagnosis was based on serological testing, a record in the provincial HIV/AIDS reporting system or two medical visits or a hospitalization with an HIV-related diagnostic code. 17 Infection status was categorized as: (a) negative for all three infections; (b) HCV mono-infection; (c) HBV mono-infection; (d) HIV mono-infection; (e) HCV/HBV co-infection; (f) HCV/HIV co-infection; (g) HBV/HIV co-infection; (h) HCV/HBV/HIV triple infection. Negative controls were followed from the last negative test date, mono-infected from the first positive test date and co/triple infected from the last positive test date to end of study defined as the date of cancer diagnosis, death or 31 December 2016, respectively.
Cancer diagnosis
The outcomes of interest for this study were colorectal, pancreatic, and liver cancers. Cancer diagnoses for BC-HTC participants were ascertained by linking with the BC Cancer Registry (BCCR). This registry has been gold certified by the North American Association of Central Cancer Registries with the case-capture estimate from the 2016 cancer diagnosis data being 97.1%. 19 Colorectal, liver, and pancreatic cancers were identified by International Classification of Diseases for Oncology, version 3 (ICDO-3), topography codes C18-C20, C22.0, and C25, respectively.
Covariates
We identified the following as potential confounders to be included in our analyses: age, sex, ethnicity, problematic alcohol use, injection drug use (IDU), cirrhosis, diabetes, and material and social deprivation.16,20,21 Multiple comorbidities were also assessed using the Elixhauser comorbidity index. 22 Covariates were measured at the date of most recent infection diagnosis in the infected groups and the date of the last HCV, HBV, or HIV diagnostic test for the negative group.
IDU and problematic alcohol use were assessed based on diagnostic codes and fee item codes for medical visits and hospitalizations (Supplemental Table 2). The IDU validation algorithm has been described elsewhere. 23 Ethnicity was classified based on the validated name recognition software Onomap.24,25 Ethnicity was categorized as South Asian (Pakistani, Indian, Bangladeshi, Nepalese, and Sri Lankan), East Asian (Chinese, Filipino, Japanese, Korean, and South-East Asian), and other (other BC residents). Cirrhosis and diabetes were assessed from the British Columbia Chronic Disease Registry, which uses a combination of International Classification of Diseases (ICD) diagnostic or procedure codes, fee item codes from medical visits or hospital admissions, and a prescription medication database to identify chronic disease cases. Diagnostic codes and definitions are provided in Supplemental Table 2.
In order to account for the potential impact of HCV treatment on cancer risk, we further categorized individuals with HCV mono-infection to treated and untreated groups. Individuals who initiated HCV treatment between HCV positive test date and study end date (i.e. cancer, censor, or death), irrespective of treatment type, were categorized as: (a) patients who achieved a sustained virological response (SVR); or (b) individuals who failed the treatment or had unknown SVR status (TF/unknown). SVR was defined as undetectable serum HCV RNA at ⩾10 weeks’ post treatment.26,27 The untreated group was categorized as: (a) individuals who spontaneously cleared (SC) the virus; or (b) untreated individuals with chronic HCV (UCHC) infection. SC was defined as a negative HCV RNA by polymerase chain reaction (PCR) test after a positive anti-HCV test among untreated individuals. 27 UCHC was defined as a positive HCV RNA test with no negative HCV RNA and no history of HCV treatment during the follow-up. 27
Statistical analysis
We compared baseline characteristics between negative, mono-infected, co-infected and triple-infected individuals. The crude incidence rate of each cancer was calculated for each of the eight infection status categories by dividing the number of events by the at-risk person-years (PY) of follow-up.
We constructed a Fine and Gray adjusted proportional subdistribution hazards model to assess the impact of infection status on each cancer, accounting for competing mortality risk. 28 Models were stratified by sex. Hazard ratio estimates among infection categories with less than five events were deemed unreliable and therefore were not included. In a sensitivity analysis, HCV mono-infected individuals were characterized by their treatment status into four categories including SVR, TF/unknown, SC, and UCHC. 27 To assess the impact of each category on colorectal, liver, and pancreatic cancer, separate adjusted proportional subdistributional hazards models, with SC group as the reference, were constructed. All analyses were performed using SAS version 9.4 (Cary, NC, USA). Data linkage to establish the BC-HTC was performed under the auspices of the BCCDC public health mandate.
Results
Description of cohort
The final analytic cohort included 658,697 individuals who were tested for all three infections between 1990 and 2016 (Figure 1). Among this group, 596,072 (90.5%) were negative for all three infections; 34,807 (5.3%), 14,913 (2.6%), and 4846 (0.7%) were HCV, HBV, and HIV mono-infected, respectively; 3472 (0.5%), 2668 (0.4%), and 679 (0.1%) were co-infected with HCV/HBV, HCV/HIV, and HBV/HIV, respectively; and 1240 (0.2%) were triple infected. A greater proportion of infected individuals were men as compared to uninfected individuals (Table 1). The majority of individuals across the infection groups were among other ethnic categories, except for HBV mono-infected individuals who were mostly of East Asian descent. A higher proportion of people with co-infection and triple infection had problematic alcohol use, IDU and co-morbidities as compared to the uninfected group. HIV mono-infected and HBV/HIV co-infected individuals tended to be less materially deprived compared to the other groups (Table 1).

Flow diagram for primary analysis.
Characteristics of participants by infections status in BC Hepatitis Testers Cohort, 1990–2016.
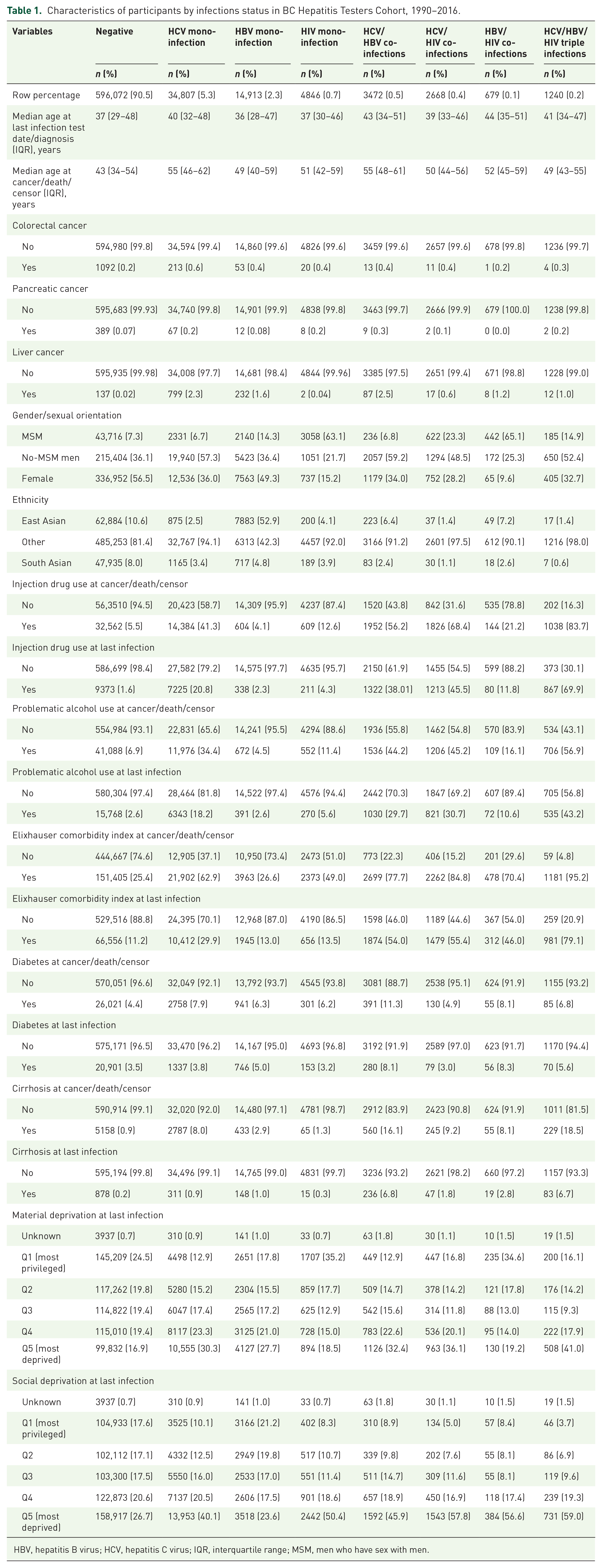
HBV, hepatitis B virus; HCV, hepatitis C virus; IQR, interquartile range; MSM, men who have sex with men.
Incidence rates
In total, 1407 (0.21%) individuals were diagnosed with colorectal cancer [median age 60.0 years, interquartile range (IQR) 52–69], 1294 (0.20%) with liver cancer (median age 60.0 years, IQR 54–66), and 489 (0.07%) with pancreatic cancer (median age 63.0 years, IQR 55–71), over 7,471,228.9 PY of follow-up (median follow-up time of 11.0 years; interquartile range 6.05, 16.46) (Figure 2).
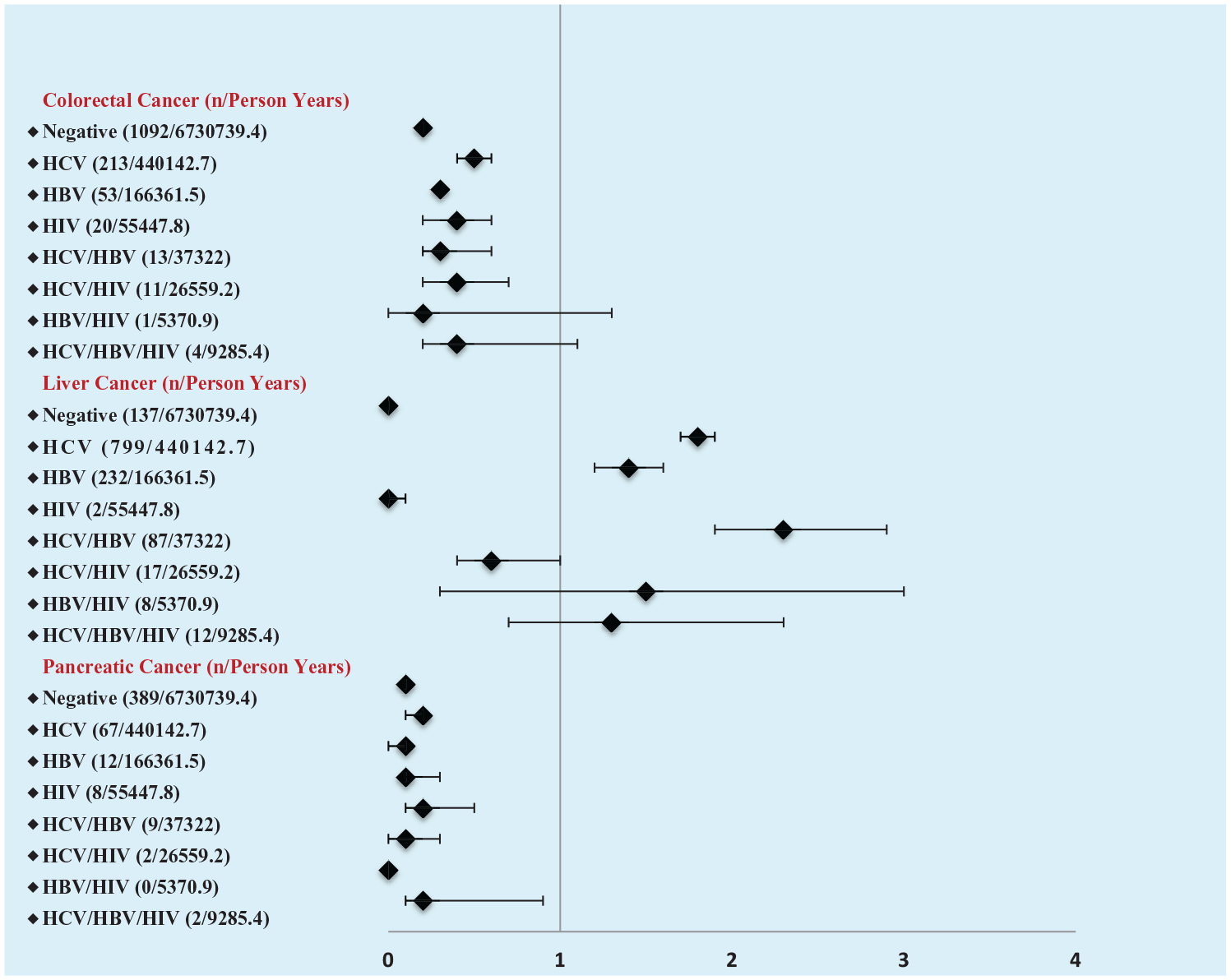
Crude incidence rate of cancer per 1000 person years by negative and infection groups, BC Hepatitis Testers Cohort.
The crude incidence of colorectal cancer was similar across the infection groups (Figure 2). For liver cancer, the incidence per 1000 PY, was highest among those with HCV mono-infection (1.8; 95% confidence interval [CI] 1.7–1.9; 799 cases per 440,142.7 PY follow-up), HBV mono-infection (1.4; 95% CI 1.2–1.6; 232 cases per 166,361.5 PY follow-up), and HCV/HBV co-infection (2.3; 95% CI 1.9–2.9; 87 cases per 37,322 PY follow-up) (Figure 2). The incidence of pancreatic cancer was similar across the infection groups (Figure 2).
Effect of infection status on cancer risk
In analyses adjusted for potential confounders, compared to uninfected individuals, HCV (hazard ratio [HR] 2.99; 95% CI 2.55–3.51), HBV (HR 2.47; 95% CI 1.85–3.28), and HIV (HR 2.30; 95% CI 1.47–3.59) mono-infections were associated with increased risks of colorectal cancer (Table 2). In addition, the risk of colorectal cancer was significantly higher among HCV/HIV co-infected (HR 2.38; 95% CI 1.31–4.34) individuals (Table 2). In sex-stratified analyses, similar associations were observed among men. Among women, HCV and HBV mono-infections were associated with an increased risk of colorectal cancer. There were no female cancer cases with HIV mono-infection and HCV/HIV co-infection (Table 3).
Risk of colorectal, pancreatic and liver cancers among HCV, HBV, and/or HIV-infected individuals at last infection diagnosis/test date, using adjusted subdistribution hazards ratio accounting for competing mortality risk.
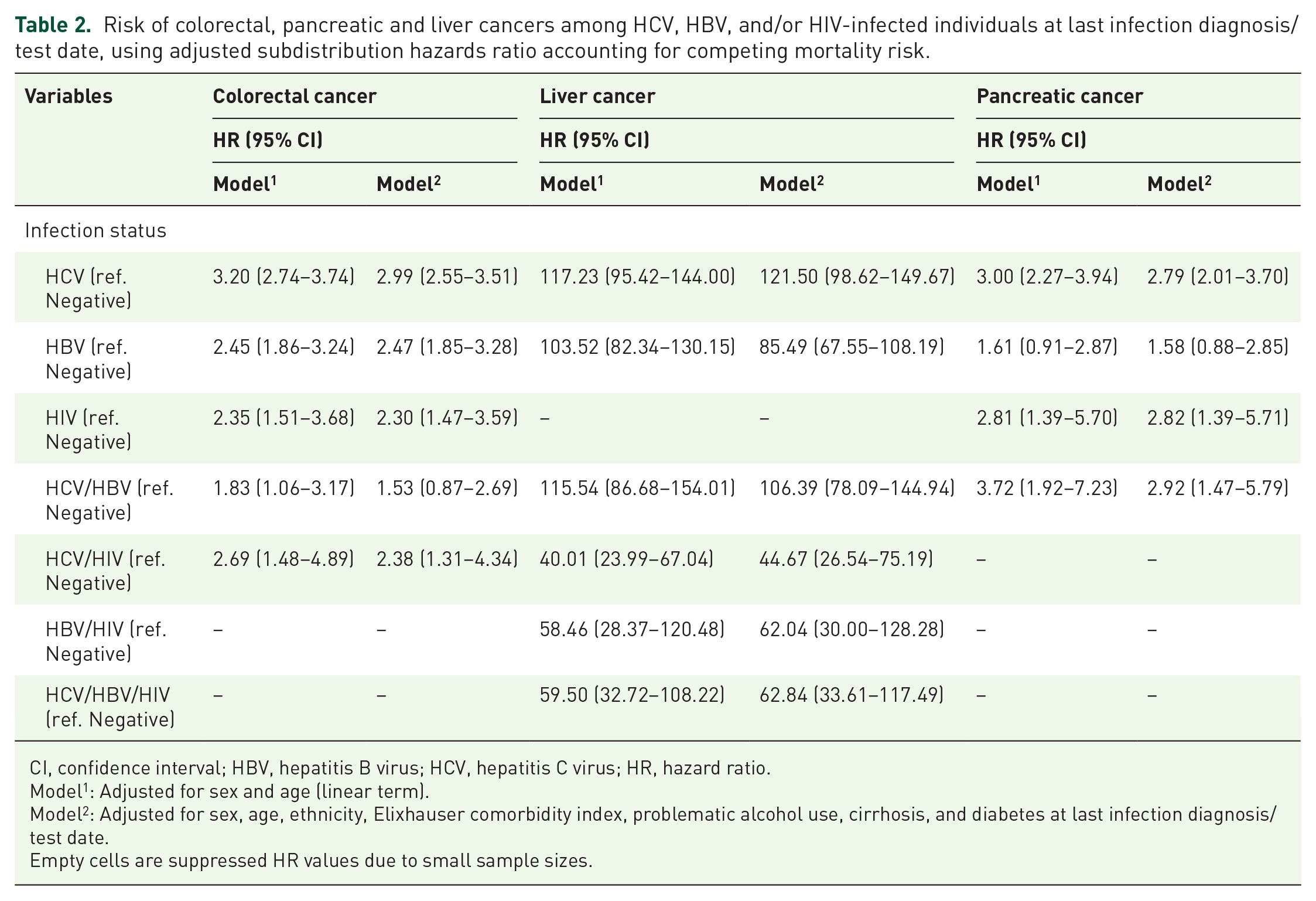
CI, confidence interval; HBV, hepatitis B virus; HCV, hepatitis C virus; HR, hazard ratio.
Model 1 : Adjusted for sex and age (linear term).
Model 2 : Adjusted for sex, age, ethnicity, Elixhauser comorbidity index, problematic alcohol use, cirrhosis, and diabetes at last infection diagnosis/test date.
Empty cells are suppressed HR values due to small sample sizes.
Risk of colorectal, pancreatic and liver cancers among HCV, HBV, and/or HIV-infected individuals stratified by sex, at last infection diagnosis/test date, using adjusted subdistribution hazards ratio accounting for competing mortality risk.
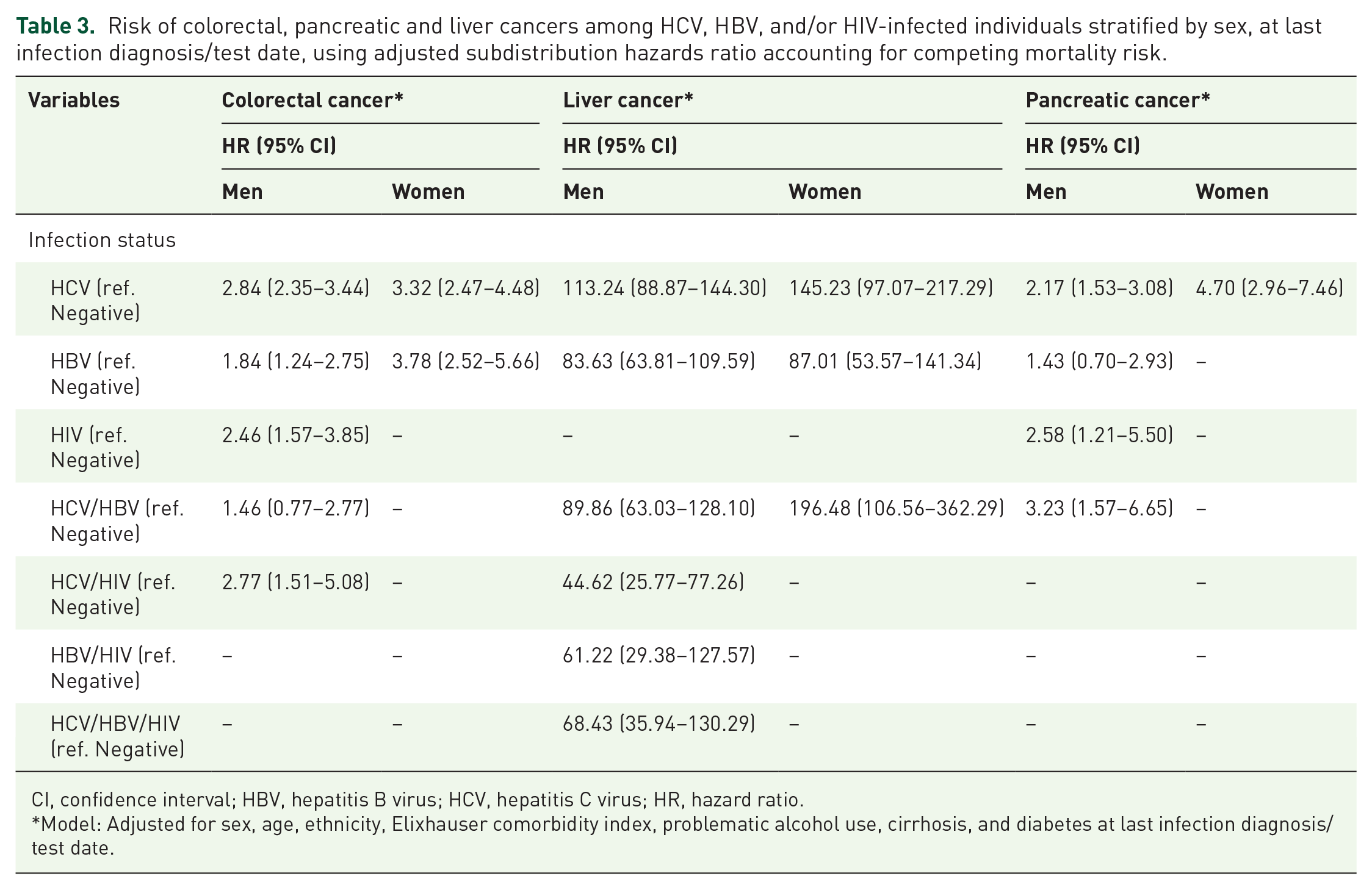
CI, confidence interval; HBV, hepatitis B virus; HCV, hepatitis C virus; HR, hazard ratio.
Model: Adjusted for sex, age, ethnicity, Elixhauser comorbidity index, problematic alcohol use, cirrhosis, and diabetes at last infection diagnosis/test date.
Compared to the uninfected group, HCV mono-infection (HR 121.50; 95% CI 98.62–149.67), HBV mono-infection (HR 85.49; 95% CI 67.55–108.19), and HCV/HBV co-infection (HR 106.39; 95% CI 78.09–144.94) were associated with increased risks of liver cancer. HCV/HIV and HBV/HIV co-infection, as well as triple infection, were also significantly associated with an elevated risk of liver cancer. In sex-stratified analyses, the risk of liver cancer was elevated among men with HCV/HIV and HBV/HIV co-infection and triple infection, while there were no female cancer cases within either of these infection categories (Figure 1, Table 3).
People with HCV mono-infection (HR 2.79; 95% CI 2.01–3.70), HIV mono-infection (HR 2.82; 95% CI 1.39–5.71), and HCV/HBV co-infection (HR 2.92; 95% CI 1.47–5.79) were at increased risk of pancreatic cancer compared to uninfected individuals (Table 2). In sex-stratified analysis, similar associations were observed among men, while except for HCV mono-infection, there were no female cancer cases within any other infection categories (Table 3).
Among 34,807 (5.3%) HCV mono-infected individuals, 7370 (21.2%) were SC, 18,926 were UCHC, and 8511 were treated, of whom 5695 (16.4%) achieved SVR, and 2816 (8.1%) were TF/unknown (Supplemental Table 3). In general, higher proportions of colorectal and liver cancers were observed among UCHC (0.8%) and TF/unknown (8.8%) groups, respectively (Supplemental Table 3). The TF group was slightly older, included more men, and had a higher proportion of individuals diagnosed with diabetes and/or cirrhosis (Supplemental Table 3). A greater proportion of individuals with UCHC had problematic alcohol use (Supplemental Table 3). No statistically significant associations of HCV clearance status with colorectal or pancreas cancers were observed (Table 4). Compared to the SC group, the risk of liver cancer was significantly higher among the TF/unknown group (HR 18.55; 95% CI 11.99–28.69), followed by the UCHC (HR 5.76; 95% CI 3.74–8.84), and SVR (HR 2.92; 95% CI 1.81–4.72) groups (Table 4).
Adjusted subdistribution hazards ratio accounting for competing mortality risk for association of HCV clearance status with colorectal, pancreatic and liver cancers among HCV-mono-infected individuals.
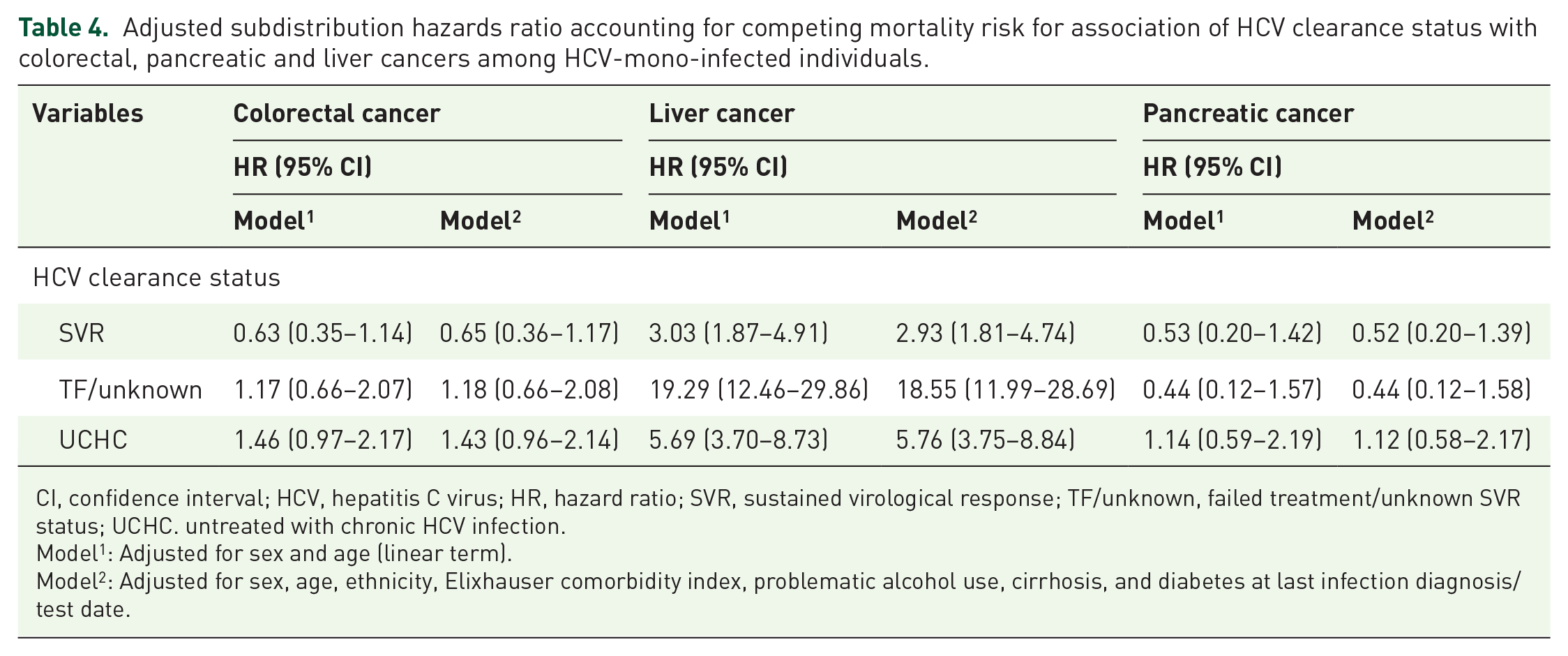
CI, confidence interval; HCV, hepatitis C virus; HR, hazard ratio; SVR, sustained virological response; TF/unknown, failed treatment/unknown SVR status; UCHC. untreated with chronic HCV infection.
Model 1 : Adjusted for sex and age (linear term).
Model 2 : Adjusted for sex, age, ethnicity, Elixhauser comorbidity index, problematic alcohol use, cirrhosis, and diabetes at last infection diagnosis/test date.
Discussion/conclusion
In this large population-based cohort study, we observed that HCV, HBV, and HIV mono-infections were, respectively, associated with an elevated risk of colorectal, pancreatic and liver cancers, colorectal and liver cancers, and colorectal and pancreatic cancers. We also observed elevated risks of colorectal cancer among individuals with HCV/HIV co-infection, liver cancer among all co-infected and triple-infected individuals, and pancreatic cancer among HCV/HBV co-infected individuals.
Findings from previous studies of the association between HCV and colorectal cancer have been mixed.12,29–32 In a US cohort study, the incidence of rectal cancer was significantly elevated among individuals with HCV infection. 29 Furthermore, in a case–control study, the odds of detecting advanced neoplasia during colonoscopy among individuals with HCV was significantly higher than uninfected individuals. 31 Other studies, however, observed no increased risk of colorectal cancers among HCV-infected individuals.12,32 In these latter studies, the use of standardized colorectal cancer incidence rates among HCV-infected individuals did not account for the potential impact of risk factors, such as the presence of comorbid conditions. In our study, after adjusting for potential risk factors, the risk of colorectal cancer remained elevated among HCV-infected individuals, thereby supporting the hypothesis that, in addition to social and behavioral acquisition risks, HCV core protein with the ability to limit the performance of tumor suppressor gene p53 may promote cancer occurrence.16,31,33
Among HCV-infected individuals in our cohort, the risk of pancreatic cancer was significantly elevated, irrespective of sex. As reported by previous studies, the observed association could potentially be related to smoking.9,34,35 In our study, information on smoking status was not available; however, compared to the non-infected group, a much greater proportion of HCV-infected individuals had a history of IDU (41.3% versus 5.5%). 36 The higher proportion of IDU among infected individuals could be an indicator of higher smoking exposure in this population, which is consistent with available evidence on the association between smoking and opioid use. 37
In the sensitivity analysis, HCV clearance was significantly associated with a reduced risk of liver cancer but not colorectal or pancreatic cancers. Our findings were consistent with data reported by the study of Huang et al. in which there was no significant association between SVR and colon (HR 0.74; 95% CI 0.40–1.34) or pancreatic (HR 1.41; 95% CI 0.46–4.35) cancers. 38 While we did not have data on the specific type of HCV treatment [i.e. interferon-based versus direct acting antiviral (DAA) therapy], the majority of SVR is expected to be due to interferon-based therapies as DAA therapy was only publicly funded in BC 1 year before the study end date. Furthermore, among HCV mono-infected individuals, the risk of liver cancer was higher among the TF category (HR 18.55) compared to the UCHC category (HR 5.76). This finding was consistent with our previously reported data assessing the impact of early HCV clearance on HCC risk, and highlights the poorer prognosis profile of TF at treatment initiation (i.e. higher pre-existing medical complications such as diabetes and/or cirrhosis (Supplemental Table 3).27,39
We observed an elevated risk of colorectal cancer among HBV-infected individuals, as has been reported in previous studies from China and Taiwan.30,40 In addition to local inflammation, it has been hypothesized that HBV X protein (HBx) could increase the risk of colorectal and other extrahepatic cancers by binding to p53 tumor suppressor and consequently inducing oncogenesis.30,40–43 Current evidence for the link between HBV and pancreatic cancer is inconsistent.30,35,40,44–46 Although the risk of pancreatic cancer was elevated in our cohort, it did not reach statistical significance, which may be due to the low number of observed cases (n = 12). Given reports of HBx being detected in pancreatic cancer cells, further investigation of this potential association is warranted. 40
Consistent with previous studies, the risk of pancreatic cancer was significantly elevated among HIV-infected individuals in our cohort.5,47,48 It has been suggested that a potential association between antiretroviral therapy (ART) and diabetes might contribute to an increased risk of pancreatic cancer among HIV-infected individuals.48–50 Although information on ART status was not available in our study, the risk of pancreatic cancer remained elevated among HIV-infected individuals even after adjusting for a history of diabetes.
It is well known that, compared to HCV or HBV mono-infections, HCV/HBV co-infection is associated with a higher risk of liver cancer. 13 Furthermore, it has been shown that, among HIV-infected individuals who are co-infected with HCV and/or HBV, the risk of liver cancer is increased. 51 However, elevated cancer risks observed among co-infected and triple-infected individuals in our study were generally consistent with risk estimates among HCV, HBV, or HIV mono-infected individuals. The consistent estimates in our study could be attributed to the fact that a higher proportions of individuals with co-infection and triple infection had a history of IDU, problematic alcohol use, and comorbid conditions (Table 1), and are therefore at higher risk of death. 36 In a recent study using BC-HTC data, individuals with triple infection were shown to be at highest risk of mortality, followed by co-infected and mono-infected individuals. 52 Hence, compared to mono-infection, individuals with multiple infections are more likely to acquire their infection through high-risk behaviors and are less likely to survive long enough to be diagnosed with cancer. Further research is needed to understand the interactive effects of multiple infections on cancer, particularly in settings where the risk of mortality related to the acquisition related factors is low.
Our findings were consistent with the higher incidence of colorectal adenoma among HCV/HIV-co-infected individuals reported in a previous US-based study. 11 It is well known that, compared to HCV or HBV mono-infections, HCV/HBV co-infections are associated with a higher risk of liver cancer. 13 Furthermore, it has been shown that, among HIV-infected individuals who are co-infected with HCV and/or HBV, the risk of liver cancer is increased. 51 In our cohort, compared to the uninfected group, the risk of liver cancer was elevated among co-infected and triple-infected individuals. The incidence of HCC is increasing worldwide, including in the USA and Canada. 53 According to American and Canadian guidelines, HCC screening with ultrasonography every 6 months is recommended among individuals with cirrhosis and chronic HBV infection.54,55 However, available data from the USA suggest a very low screening utilization rate, 56 and data on compliance with HCC screening guidelines in BC and/or in Canada are not available. Hence, as part of cancer prevention strategies, data on HCC screening and its impact on early detection, treatment, and survival among individuals with HBV infection and HCV-related cirrhosis is required. Furthermore, as early HCV treatment initiation could reduce the risk of HCC considerably, therapy with DAA regimens closer to infection acquisition should be considered as a prevention strategy among infected individuals. 27
To our knowledge, this is the first population-based cohort study in North America that has assessed the risk of multiple gastrointestinal cancers among individuals tested for and diagnosed with HCV, HBV, and HIV (co-)infections. In our study, the large number of individuals who tested negative for all three infections (n = 596,072) provided a comparable group for analyses of risk among the various infection categories. We were also able to assess the impact of many potential confounding factors, such as ethnicity, alcohol consumption, and chronic medical conditions that were not considered in previous studies.12,29
Despite these strengths, there are some limitations with our study. Firstly, although the impact of multiple covariates has been taken into account in this study, information on other factors, such as HIV ART, HBV treatment, and smoking status, was not available. In addition, the assessment of alcohol consumption was based on diagnostic codes that solely captured alcohol abuse and not more moderate levels of consumption, which may have an impact on cancer risk. Secondly, although we validated Onomap for use in the BC population, it is not able to identify all people, in particular: those who would describe themselves as having a mixed ethnicity; people whose surnames are not specific to ethnic groups; and people who adopt surnames of another ethnic group. 25 Onomap does not identify people with indigenous ethnicity. Due to legislated forced assimilation in Canada during the 18th–20th centuries, Indigenous peoples’ names were routinely changed to biblical or other European names. 57 Thus, there is a misclassification of various ethnic groups through this methodology. Moreover, despite the size of our cohort, several combinations of infection and cancer were quite rare in our data (less than five events), preventing us from properly estimating differences in risk or stratifying the estimates further by different malignancy subtypes. Furthermore, as including the sequence for eight infection categories would significantly increase the number of infection groups (e.g. for HCV: HCV mono, HCV/HBV, HBV/HCV, HCV/HIV, HIV/HCV, HCV/HBV/HIV, HCV/HIV/HBV, HBV/HCV/HIV, HIV/HCV/HBV, etc.) and would further decrease the sample size in each infection category, the potential impact of infection sequence on cancer risk was beyond the scope of current study. Besides, although other analytical approaches were considered to address the time-dependent nature of infection status and covariates, the Fine–Gray subdistribution hazards models were used in this study, as in the presence of competing risk (i.e. mortality), including time-varying variables may lead to unclear inferences and bias. 58 Finally, since the introduction of DAA therapy in BC is relatively new, the BC-HTC has not yet accrued enough follow-up time to assess the impact of DAA therapy on cancer development. However, it should be noted that the main objective of the current study was to assess the association between mono and co/triple-viral infections on cancer risk, irrespective of treatment status. Hence, assessing the impact of antiviral therapy on the risk of cancer was beyond the scope of this study and will be explored in the near future. Despite these limitations, as reported by Allaire et al., extra-hepatic cancers could remain the leading cause of death in patients who achieved SVR or with low viral replication, likely due to the presence of acquisition risks through high-risk behaviors. 59
In conclusion, we observed significant associations between HCV, HBV, HIV mono-infections, co-infection, and triple infection with an elevated risk of colorectal, liver and pancreatic cancers. The associations could be explained by the potential oncogenic effect of viruses and/or underlying risk factors (e.g. alcohol consumption) for which these infections are surrogates. Irrespective of underlying mechanisms, these results highlight the need for cancer prevention and diligent clinical monitoring for hepatic and extrahepatic cancers in infected populations.
Supplemental Material
sj-pdf-1-tam-10.1177_1758835921992987 – Supplemental material for Elevated risk of colorectal, liver, and pancreatic cancers among HCV, HBV and/or HIV (co)infected individuals in a population based cohort in Canada
Supplemental material, sj-pdf-1-tam-10.1177_1758835921992987 for Elevated risk of colorectal, liver, and pancreatic cancers among HCV, HBV and/or HIV (co)infected individuals in a population based cohort in Canada by Maryam Darvishian, Zahid A. Butt, Stanley Wong, Eric M. Yoshida, Jaskaran Khinda, Michael Otterstatter, Amanda Yu, Mawuena Binka, Carmine Rossi, Geoff McKee, Margo Pearce, Maria Alvarez, Jason Wong, Darrel Cook, Troy Grennan, Jane Buxton, Mark Tyndall, Ryan Woods, Mel Krajden, Parveen Bhatti and Naveed Z. Janjua in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors acknowledge the assistance of BCCDC, PHSA performance measurement and reporting, information analysts, Ministry of Health Data Access, Research and Stewardship, and medical services plan (MSP), discharge abstract database (DAD) and Medical Beneficiary and Pharmaceutical Services programme areas, BC Ministry of Health, and BC Cancer Agency and their staff involved in data access and procurement, and data management.
Author contributions
Conceived and designed the study: MD, NZJ. Analyzed the data: MD. This article was written by MD, taking into account the comments and suggestions of the co-authors. All co-authors had the opportunity to comment on the analysis and interpretation of the findings and approved the final version for publication.
Conflict of interest statement
D. Cook received speaker honoraria and travel expense reimbursement from Hologic, unrelated to the present study. M. Krajden received grants from Roche Molecular Systems, Boehringer Ingelheim, Merck, Siemens Healthcare Diagnostics, and Hologic. E.M. Yoshida participated in clinical trials sponsored by: Abbvie, Gilead Sciences, Merck, Janssen, Genfit, Intercept, Madrigal, Pfizer; he received honoraria for CME/Ad board lectures from Gilead, Merck, AbbVie, Intercept. Celgene.
Disclaimer
All inferences, opinions, and conclusions drawn in this publication are those of the author(s), and do not necessarily reflect the opinions or policies of the [British Columbia] Ministry of Health.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by BC Centre for Disease Control and Agencies contributing data to the study and the Canadian Institutes of Health Research (grant nos. NHC-348216, PHE-337680, and PJT-156066), Michael Smith Foundation for Health Research and Canadian Network on Hepatitis C.
Statement of ethics
The study was approved by the Behavioral Research Ethics Board at the University of British Columbia (study id: H15-01776).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.