
Abstract
Background:
The level of evidence for palliative second-line therapy in advanced esophageal squamous cell carcinoma (aESCC) is limited. This is the first study that reports efficacy data comparing second-line therapy + active symptom control (ASC) versus ASC alone in aESCC.
Methods:
We conducted a tri-center retrospective cohort study (n = 166) including patients with aESCC who had experienced disease progression on palliative first-line therapy. A propensity score model using inverse probability of treatment weighting (IPTW) was implemented for comparative efficacy analysis of overall survival (OS) in patients with second-line + ASC (n = 92, 55%) versus ASC alone (n = 74, 45%).
Results:
The most frequent second-line regimens used were docetaxel (36%) and paclitaxel (18%). In unadjusted primary endpoint analysis, second-line + ASC was associated with significantly longer OS compared with ASC alone [hazard ratio (HR) = 0.49, 95% confidence interval (CI): 0.35–0.69, p < 0.0001]. However, patients in the second-line + ASC group were characterized by more favorable baseline features including a better Eastern Cooperative Oncology Group (ECOG) performance status, a longer first-line treatment duration and lower C-reactive protein levels. After rigorous adjusting for baseline confounders by re-weighting the data with the IPTW the favorable association between second-line and longer OS weakened but prevailed. The median OS was 6.1 months in the second-line + ASC group and 3.2 months in the ASC group, respectively (IPTW-adjusted HR = 0.40, 95% CI: 0.24–0.69, p = 0.001). Importantly, the benefit of second-line was consistent across several clinical subgroups, including patients with ECOG performance status ⩾1 and age ⩾65 years. The most common grade 3 or 4 adverse events associated with palliative second-line therapy were hematological toxicities.
Conclusion:
This real-world study supports the concept that systemic second-line therapy prolongs survival in patients with aESCC.
Keywords
Background
With over 570,000 newly diagnosed cases per year, esophageal cancer (EC) is the ninth most common cancer in the world and accounts for 5.3% of cancer case mortality. 1 The two main histological subtypes, esophageal squamous cell carcinoma (ESCC) and esophageal adenocarcinoma (EAC) have a distinct pathogenesis and show strong regional differences. 2 While in western countries the incidence of EAC has risen over the past two decades, numbers of ESCC have declined. Still globally ESCC accounts for almost 90% of newly diagnosed EC and thus represents a major public health burden especially in lower income countries.3,4 Until recently, treatment options for metastatic or locally advanced inoperable ESCC have been very limited and the level of evidence for established treatment strategies remains poor. Based on results from phase II trials current guidelines recommend a platin and fluoropyrimidine containing doublet chemotherapy as palliative first-line treatment for patients with advanced esophageal squamous cell carcinoma (aESCC) and a good Eastern Cooperative Oncology Group (ECOG) performance status.5–8 Most recently, preliminary results of the KEYNOTE-590 demonstrated superiority of frontline chemotherapy in combination with the programmed death-1 (PD-1) inhibitor pembrolizumab compared with chemotherapy alone in patients with locally advanced unresectable or metastatic EC, which might become the new standard of care in this setting. 9
While cytotoxic first-line treatment for advanced ESCC is a widely accepted treatment strategy, the treatment benefit for later lines of systemic therapy is even less clear. For patients who retain a good ECOG performance status after progression on first-line treatment, systemic second-line therapy might be considered according to current National Comprehensive Cancer Network (NCCN) and EC practice guidelines from Japan.10,11 In this case, mono-chemotherapy with paclitaxel, docetaxel, vinorelbin or irinotecan ± fluoropyrimidine (e.g. FOLFIRI) are commonly used regimens. However, the administration of these treatments is solely based on outcome data of small single-arm phase II trials or retrospective cohort studies from a primarily Asian population. Further reported outcome data have been modest, while toxicity rates were high.12–18 In 2019 the ATTRACTION-3 trial has proved superiority of the PD-1 inhibitor nivolumab over investigator choice of chemotherapy (paclitaxel or docetaxel) as second-line treatment in patients with aESCC. 19 Based on these findings nivolumab has recently received approval from the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for patients with unresectable advanced, recurrent or metastatic ESCC after prior fluoropyrimidine and platinum-based chemotherapy. However, globally immune checkpoint inhibitors have limited availability and given the promising findings from KEYNOTE-590 might soon move to the first-line treatment setting. 9 Considering the poor level of evidence and modest efficacy of second-line chemotherapy in aESCC, best supportive care only is a feasible treatment option after progression on first-line treatment especially for patients with reduced performance status. Importantly, to date no randomized controlled clinical trial or systemic meta-analysis has proved superiority of cytotoxic second-line therapy over a purely symptomatic treatment in aESCC.
To the best of our knowledge this is the first study reporting propensity score adjusted efficacy data comparing second-line therapy with active symptom control (ASC) in a multicenter real-world cohort of patients with first-line refractory aESCC.
Methods
Study design and patient cohort
This retrospective cohort study was performed at three academic centers in Austria (Medical University of Graz, Paracelsus Medical University Salzburg and Medical University of Innsbruck). All patients with histologically and radiologically confirmed metastatic or locally advanced inoperable ESCC who were 18 years or older and who had experienced disease progression on or after receiving palliative first-line therapy at one of the respective centers between 1 January 2006 and 30 April 2020 were considered for this study (n = 191). Of this cohort, patients who had ongoing palliative first-line at the date of data acquisition (n = 4) and patients who died during first-line therapy (n = 21) were excluded, resulting in an analysis population of n = 166 patients.
Data acquisition and outcome
Baseline and outcome data were retrospectively collected from the respective in-house electronic healthcare databases as well as from the central registry of the Austrian Social Security Providers Association for all-cause death as reported previously.20,21 To assess the survival time uniformly for both study groups, the baseline date was defined as the termination date of palliative first-line treatment, in detail the date when the last cycle of first-line treatment was administered. The primary endpoint of the study was overall survival (OS) defined as the time from baseline until death from any cause or censoring alive. The co-secondary endpoints in the subgroup of patients who received second-line treatment, were the investigator-assessed objective response rate (ORR); that is, the composite of complete or partial remission, the OS measured from the date of start of second-line therapy until death from any cause or censoring alive as well as the progression-free survival (PFS) measured from the date of start of second-line treatment until radiographically assessed disease progression, death from any cause or censoring alive. Adverse events were classified according to common terminology criteria for adverse events version 5.0 (CTCAE 5.0). This study was approved by the institutional review board of the leading center (Ethics Committee of the Medical University of Graz, Austria; document number 32-660 ex 19/20). All methods and analyses were performed in accordance with the relevant local and national guidelines and regulations.
Statistical methods
All statistical analyses were performed with Stata 15.0 (Stata Corp., Houston, TX, USA). Continuous variables were summarized as medians (25th–75th percentile), whereas count data were reported as absolute frequencies (column %). The distribution of baseline variables between the two treatment groups was analyzed with rank-sum tests, χ2 tests, and Fisher’s exact tests, as appropriate. Standardized mean differences (SMDs) were implemented to gauge the magnitude of difference in the distribution of baseline variables between the two treatment groups. 22 The propensity score was predicted from a multivariable logistic regression model with treatment assignment as the dependent variable and by including all baseline variables as explanatory variables that had a p-value for difference between the two treatment groups of ⩽0.10 or an SMD ⩾0.15. This multivariable propensity score model was fitted on multiply-imputed data to account for missingness in selected variables. Multiple imputation was performed with a chained equations algorithm with 10 imputation datasets, predictive mean matching for missing categorical variables, and linear regression for missing continuous variables without including the outcome in the imputation model. 23 Based on the propensity score, we then obtained the inverse probability of treatment weight (IPTW) according to the average treatment effect (ATE) principle. 24 Following best practice recommendations, we then re-calculated SMDs with IPTW-weighted data in order to gauge whether the propensity score modelling process achieved adequate balance. 22 Median follow-up was estimated with the reverse Kaplan–Meier method, 25 and follow-up was truncated at 24 months. The primary outcome of the study, OS, was computed with Kaplan–Meier estimators. The proportionality of hazards (PH) assumption according to treatment group was tested with a PH test on the Schoenfeld residuals of a univariable Cox model, and because this test revealed very strong evidence for a departure from the PH assumption, all subsequent analyses were performed with Royston–Parmar models that specifically accounted for non-proportionality [Stata routine stpm2 with 3 degrees of freedom for the time-dependent ‘effect’ of treatment and 2 degrees of freedom for the time-invariant ‘effect’ of treatment, directly modelling on the log(cumulative hazard) scale]. 26 In sensitivity analyses, we (a) estimated the progression-free survival (PFS) in patients who had received second-line therapy, (b) compared crude OS estimates for taxane versus non-taxane based second-line therapy, (c) quantified non-proportionality of the association between second-line therapy and OS outcomes, and (d) performed IPTW-weighted multivariable analysis by additionally adjusting for the two covariates with the strongest association with OS [ECOG performance status, C-reactive protein (CRP) levels]. Finally, we performed exploratory hypothesis generating subgroup analyses of the relative efficacy of the two treatment strategies according to eight pre-specified clinical covariables: ECOG performance status, age, gender, Charlson comorbidity index (CCI), primary metastatic disease, objective response to first-line therapy, surgery of the primary tumor, and modality of first-line therapy (monotherapy versus doublet). Here, interaction p-values <0.10 were considered to indicate a potentially relevant interaction. The analysis code is available on reasonable request from FP.
Results
Cohort description, first-line therapy data, and crude outcome rates
One hundred and sixty-six patients with a median age of 63 years (25th–75th percentile: 57–70) were included in the analysis (Table 1). The median CCI, excluding 6 points for advanced malignancy was 3 (2–4), and most patients (75%) had an ECOG performance status <2. Nearly half (n = 70) of the cohort had a primary palliative treatment intent, while 38 patients (23%) underwent prior resection of their primary tumor and 38 patients (23%) underwent prior definitive chemoradiation. The majority of patients were treated with a platinum agent and a fluoropyrimidine in first-line therapy, with only 44 patients (24%) being treated with a monotherapy. For computation of first-line treatment outcomes, we also included the n = 21 patients who died during first-line therapy (n = 187). Overall, first-line treatment duration was relatively short (median: 2.2 months), and the investigator-assessed ORR was 25% while the median OS from start of first-line therapy was 7.1 months (Supplemental Figure 1).
Baseline characteristics of the study population (n = 166).

Distribution overall and by treatment group. Data are medians (25th–75th percentile) for continuous data, and absolute frequencies (column %) for count data. n (%miss.) reports the number of patients with fully observed records for the respective variable (% missing).
IPTW-weighted p-values were obtained from linear, logistic, ordinal logistic, and multinomial logistic regression models.
2L, second-line therapy; ASC, active symptom control; ECOG, Eastern Cooperative Oncology Group; EGFRi, epidermal growth factor receptor inhibitor (e.g. cetuximab); IPTW, inverse probability of treatment weight; LDH, lactate dehydrogenase; N/A, not applicable; p, p-value; pIPTW, p-value after IPTW weighting; SMD, standardized mean difference; SMDIPTW, standardized mean difference after IPTW weighting.
Second-line therapy of advanced ESCC: unadjusted analysis
After progression on first-line therapy, 74 (45%) patients were treated with ASC while 92 patients (55%) received additional second-line therapy. The most frequent second-line regimens were monotherapies (82%), including docetaxel (36%) and paclitaxel (18%). A subset of patients received immune checkpoint inhibitors (7%, n = 6) and epidermal growth factor receptor (EGFR) (4%, n = 4) inhibitors, respectively (Table 2). The ORR of secpnd-line therapy was 13%, while median PFS and OS estimates after initiation of second line therapy were 2.2 and 4.7 months, respectively (Supplemental Figure 2). In terms of safety, the most common adverse events during second line therapy were hematological toxicities (Table 3). The most common grade 3 or 4 toxicities were anemia (15%), neutropenia (14%) and febrile neutropenia (4%). Fourteen patients (16%) were hospitalized because of serious adverse events and in 5% of the patients second line therapy had to be stopped due to toxicity.
Tabulation of second-line therapy characteristics.

95% CI, 95% confidence interval; DCR, disease control rate; EGFR, epidermal growth factor receptor; ORR, objective response rate; OS, overall survival; p25–p75, 1st to 3rd quartile of the distribution of the respective variable; PFS, progression-free survival.
Toxicity profile of second-line therapy.
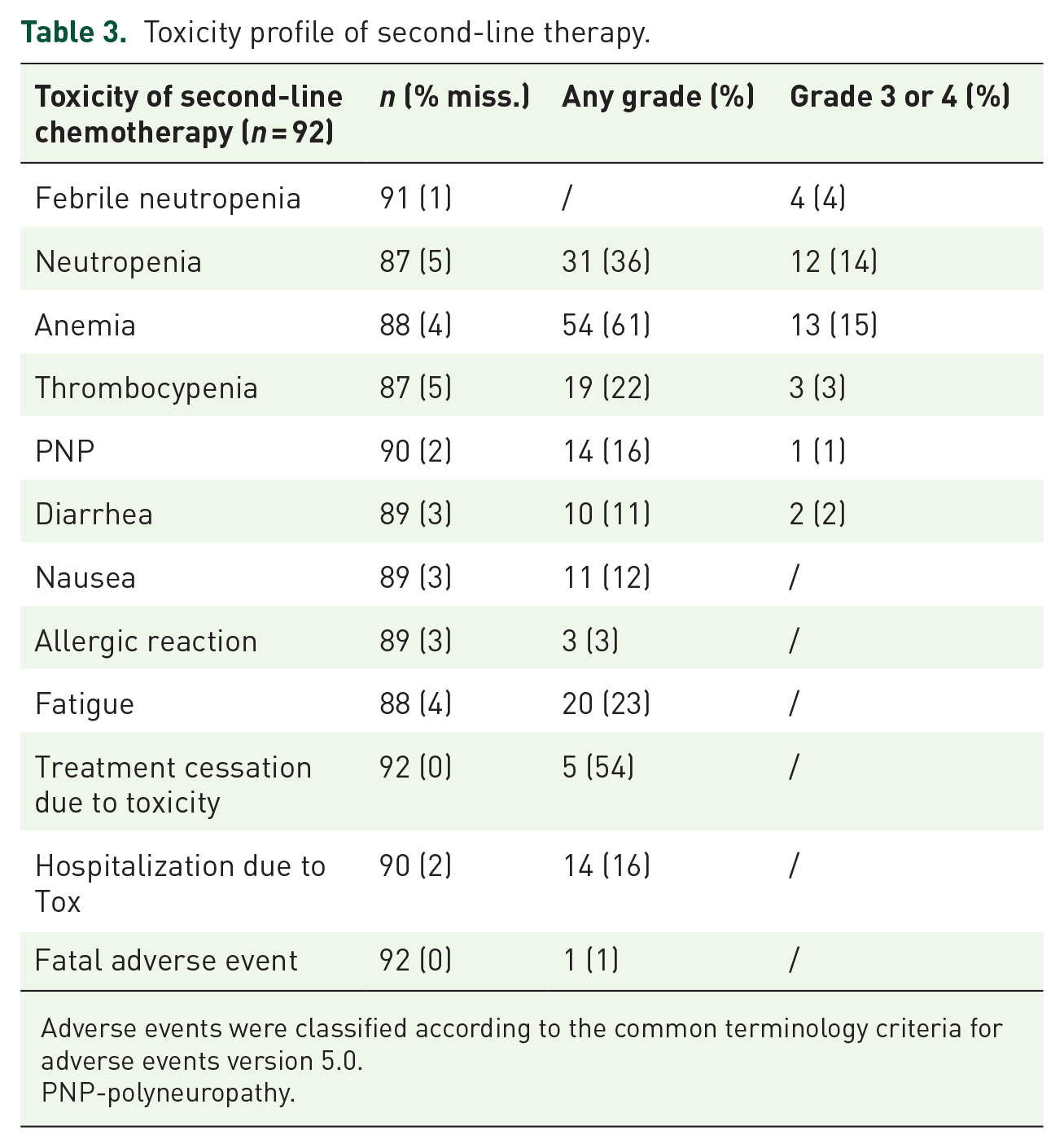
Adverse events were classified according to the common terminology criteria for adverse events version 5.0.
PNP-polyneuropathy.
In crude analysis of OS, patients who went on to receive second-line therapy had a significantly more favorable OS than patients who were treated with ASC alone. In detail, median OS estimates were 2.9 months in the ASC group, and 7.2 months in the 2nd-line + ASC group, respectively [Figure 1(a), log-rank p < 0.0001, Hazard ratio (HR) from a univariable Cox model = 0.49, 95% confidence interval (CI): 0.35–0.69, p < 0.0001]. As strong evidence for a violation of the proportional hazards assumption [Schoenfeld test p = 0.005, ‘converging curves’ in Figure 1(a)] was observed, we further analyzed the data with a Royston–Parmar model, yielding a HR of 0.29 (95% CI: 0.17–0.48, p < 0.0001) and a median predicted OS estimate of 2.7 months and 7.2 months in the ASC and 2L + ASC group, respectively [Figure 2(a)].
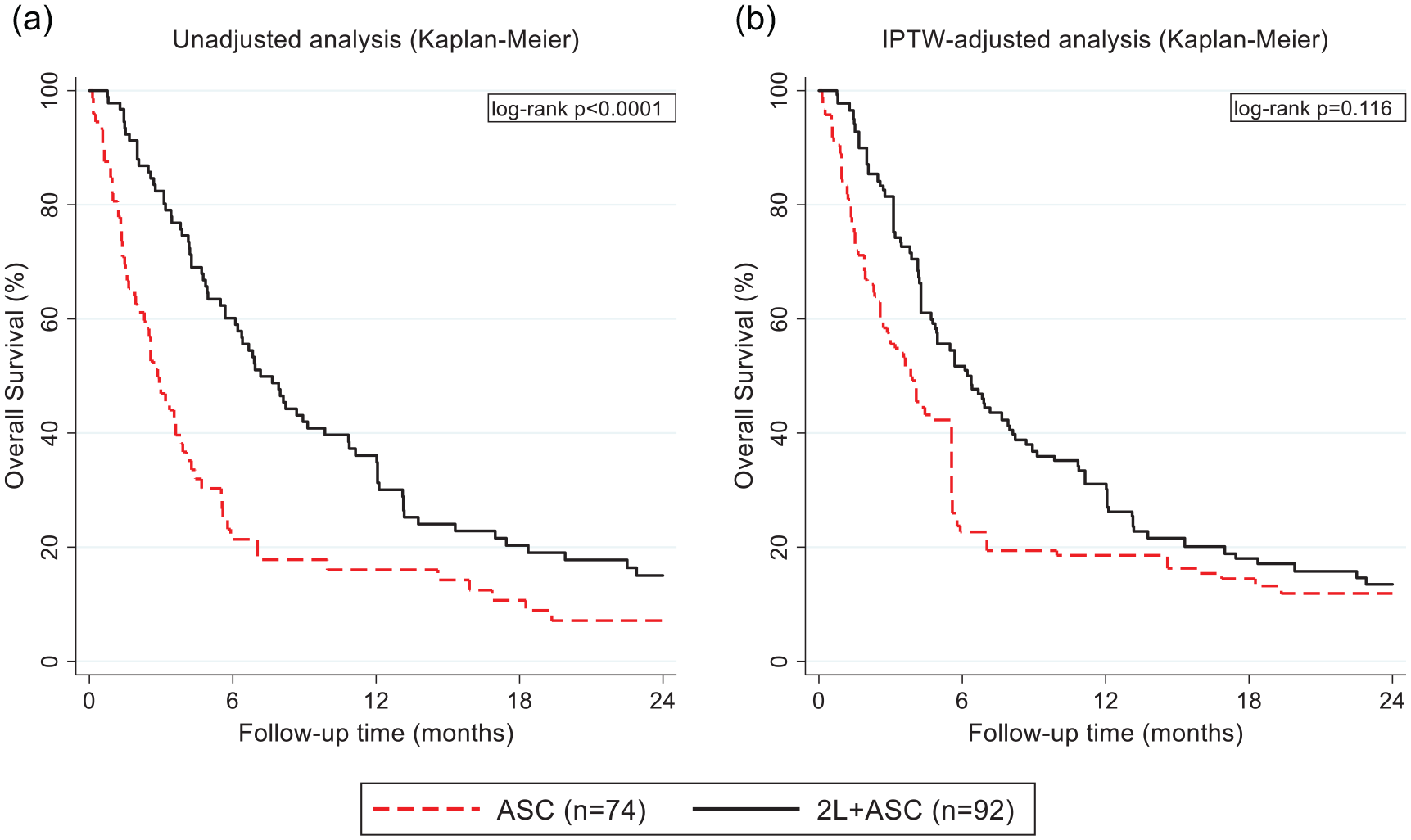
Kaplan–Meier analysis of overall survival by treatment group. (a) Unadjusted analysis. (b) IPTW-adjusted analysis.

Royston–Parmar analysis of overall survival by treatment group. (a) Unadjusted analysis. (b) IPTW-adjusted analysis.
Development of a propensity score
However, consistent with selection bias, patients in the second-line + ASC had a significantly higher prevalence of favorable prognostic factors (Table 1). Considering standardized mean differences (SMDs) ⩾0.3 to indicate a potentially large magnitude of difference in the distribution of a variable between the two treatment groups, patients in the second-line + ASC group had, among others, better ECOG performance status (SMD for ECOG 0 = 0.88), a longer first-line treatment duration (SMD = 0.36), and lower CRP levels (SMD = 0.54) than patients who were treated with ASC alone. Given the association of these and other unevenly distributed variables with OS (Supplemental Table 1), we obtained a propensity score (PS) from a multivariable logistic regression model (Supplemental Table 2). This propensity score covered the whole probability range [Supplemental Figure 3(a)], and was transformed into an IPTW [Supplemental Figure 3(b)]. Re-weighting the data with this IPTW strongly reduced imbalances between the two treatment groups (Table 1). In detail, none of the differences in baseline variables were statistically significant anymore, and SMDs were reduced (e.g. for age from 0.34 to 0.09). These balance diagnostics findings were considered to be indicative of adequate balance between the two treatment groups upon IPTW weighting.
Second-line therapy for aESCC: IPTW-adjusted analysis
On IPTW and thus controlling for selection bias, the favorable association between second-line therapy and longer OS weakened but prevailed. We again observed very strong evidence for a violation of the PH assumption (Schoenfeld test after Cox model: p < 0.0001, ‘converging curves’), and thus primarily analyzed the data with the Royston–Parmar model [Figure 2(b)], but also provide Kaplan–Meier estimators for reference [Figure 1(b)]. In detail, median predicted OS estimates were 3.3 months in the ASC group and 6.1 months in the second-line + ASC group, with corresponding 12-month OS estimates of 18% and 28%, respectively (IPTW-adjusted HR = 0.40, 95% CI: 0.24–0.69, p = 0.001).
Sensitivity analyses
This association prevailed on multivariable adjustment for the two strongest prognostic variables for OS, namely ECOG performance status and CRP levels (IPTW and multivariably adjusted HR for second-line + ASC within the Royston–Parmar model = 0.45, 95% CI: 0.25–0.83, p = 0.011, Supplemental Table 3). In terms of the violation of the proportional hazards assumption, our findings were consistent with a decreasing ‘effect’ of second-line therapy over time, with hazards of death between the two treatment groups approaching equality at around 10 months of follow-up (Figure 4). In crude analysis of OS of the 92 patients receiving second-line + ASC, we observed a weak, ‘borderline’ statistically significant association between taxane-based second-line therapy and worse OS outcomes [HR for taxane-based (n = 52) versus non-taxane-based (n = 40) second-line therapy = 1.54, 95% CI: 0.98–2.44, p = 0.062, Supplemental Figure 4], which prevailed after adjusting for ECOG performance status (adjusted HR = 1.58, 95% CI: 0.98–2.53, p = 0.060).
Exploratory subgroup analysis
The benefit of second-line therapy appeared to be consistent across several clinical subgroups, including ECOG performance status (interaction p = 0.950), age (p = 0.929), gender (p = 0.192), comorbidity (p = 0.744), tumor node metastasis (TNM) clinical metastasis status at diagnosis of disease (p = 0.702), objective response to first-line therapy (p = 0.260), surgery of the primary tumor (p = 0.380), and aggressivity of first-line therapy (monotherapy versus doublet, p = 0.704, Figure 3).

Hypothesis-generating, exploratory subgroup analysis of potential second-line therapy benefit. Black diamonds represent the hazard ratio for 2L + ASC within the respective subgroup, and black lines the associated 95% confidence intervals. The size of the grey boxes is proportional to the subgroups’ weight (i.e. proportional to the subgroup sample size).

Time-dependent ‘effect’ of second-line therapy. Data represent the difference (with 95% confidence bands) in the hazards of death (per 1000 person-years) between the 2L + ASC and ASC groups, as predicted from a Royston–Parmar model allowing for non-proportionality of hazards.
Discussion
Limited real-world outcome data especially from western countries have been reported for aESCC. In our study, a median OS of only 7.1 months after the start of palliative first-line therapy was observed, which underlines the aggressiveness of aESCC and the desperate need for new treatment options. After progression on palliative first-line treating physicians face the uncertainty whether to offer further anti-neoplastic therapy or to focus on a purely symptomatic treatment. Several small phase II trials have investigated different agents in this setting reporting response rates ranging from 6% for vinorelbine 12 to 45% for weekly paclitaxel.13–16 These findings, albeit accompanied by high toxicity rates, have prompted physicians to consider systemic second-line chemotherapy as an effective treatment strategy. However, all of these were single-arm trials and were therefore not designed to prove superiority of systemic second-line chemotherapy over best supportive care. Consistent with previous reports, approximately 50% of all patients who underwent first-line treatment were considered suitable for systemic second-line therapy in our study. 16 The unadjusted primary outcome analysis revealed a significantly improved OS for second-line therapy (7.2 months) compared with ASC only (2.9 months). Due to the non-random treatment assignment, these data should, however, be interpreted with caution as patients in the second-line therapy group were likely to have been selected under consideration of favorable prognostic features that could have led to a significant overestimation of the true treatment effect and thus, pose a major risk of selection bias. Consistently, patients treated with second-line therapy were younger, had a significantly better ECOG performance status, had a longer duration of previous first-line therapy as well as lower CRP and higher albumin levels. These factors are all known as good prognostic features in patients with advanced cancer.27–31 To adjust for baseline imbalances, we performed a propensity score analysis using IPTW. Propensity score (PS) models have been developed as a comparative effectiveness research method that can mimic randomization by reducing the effect of baseline confounding in observational studies. 24 This sophisticated statistical method harbors great potential for retrospective data analysis.32,33 For instance, by incorporating a propensity score analysis our study group could demonstrate a survival benefit for second-line chemotherapy over best supportive care in biliary tract cancer, which was recently supported by a preliminary outcome report of the prospective randomized phase III ABC-06 trial.23,34 In the present study, similar findings were observed. After rigorously adjusting for baseline confounders the survival benefit for second line therapy weakened, however, remained statistically significant. Aligning well with our data a retrospective Japanese study has shown a survival benefit for salvage chemotherapy in patients with fluoropyrimidine, platin and taxane refractory aESCC over best supportive care. 35 Importantly, we observed that the beneficial effect of second-line therapy weakened over time as indicated by a crossing of survival curves after one year. As discussed previously, these findings support the concept that later lines of palliative chemotherapy treatment can only delay death but usually do not lead to a higher proportion of long-term survivors. 23 Furthermore, the overall low treatment response rate of 13% and the considerable risk of toxicity should appropriately be taken into consideration, when discussing the option of second-line therapy with patients. The median OS of 4.7 months after treatment start of second-line therapy in our cohort was comparable with other real-world studies that have reported slightly better OS estimates of 5.5 months, 36 6.1 months 17 and 6.7 months 37 for second-line therapy. Interestingly, in our study patients treated with a non-taxane-based second-line therapy experienced a numerically longer OS compared with patients treated with taxanes. This stands in contrast to a recent report from Abraham et al. that showed a superior outcome for taxane-containing regimens. Notably, in that study the majority of patients was treated with a combination chemotherapy of carboplatin plus paclitaxel, whereas in our study taxanes were administered as a single-agent regimen. 37
We finally aimed to identify predictive markers for second line therapy benefit. In an exploratory propensity score adjusted subgroup analysis we found that the favorable association between longer OS and second-line therapy was consistent across several relevant clinical subgroups. Importantly, also patients with an ECOG performance status ⩾1, as well as patients aged 65 years or older seemed to gain a survival advantage from second-line therapy. Although these findings support the use of palliative second-line therapy, treatment decision should be made individually after comprehensive consideration of the patient’s specific situation, health status and wishes. The following limitations of this study have to be considered: first, despite rigorous adjustment for differences of patients’ baseline characteristics between the two study groups by the IPTW, a residual risk of confounding especially of unmeasured covariates, cannot be fully excluded. 22 Second, due to the retrospective study design no valid data regarding quality of life were available. Third, imaging data for radiographic response assessment were not re-assessed by central radiology review. Fourth, information on dose density of the respective second-line treatment regimens were missing. Fifth, adverse events were assessed in retrospect from chart reviews leading to a potential risk of underreporting.
Despite these limitations, this study provides valuable data to aid in treatment decision-making in the management of patients with first-line refractory aESCC.
Conclusion
In this real-world comparative efficacy study, we implemented a propensity score model to investigate the potential benefit of second-line therapy over active symptom control in a western population of patients with aESCC. Overall, we found that aESCC is associated with detrimental outcomes. Although response rates are low, second-line therapy improves OS compared with symptomatic treatment. Importantly, also patients with reduced ECOG performance status seem to gain a survival advantage from systemic second-line therapy. Further prospective studies are needed to validate our findings.
Supplemental Material
sj-docx-1-tam-10.1177_17588359211039930 – Supplemental material for Benefit of second-line therapy for advanced esophageal squamous cell carcinoma: a tri-center propensity score analysis
Supplemental material, sj-docx-1-tam-10.1177_17588359211039930 for Benefit of second-line therapy for advanced esophageal squamous cell carcinoma: a tri-center propensity score analysis by Moritz Müller, Florian Posch, Dominik Kiem, Dominik Barth, Lena Horvath, Michael Stotz, Renate Schaberl-Moser, Martin Pichler, Richard Greil, Philipp J. Jost, Andreas Seeber, Arno Amann, Konstantin Schlick, Armin Gerger and Jakob M. Riedl in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
None.
Author contributions
Conceived and designed the study: MM, FP, JMR. Collected data and contributed patients: All authors. Performed all statistical analyses: FP. Interpreted the results: All authors. Wrote the first draft of the manuscript: MM, FP, JMR. Contributed to the writing of the manuscript: All authors. Agree with the manuscript’s results and conclusions: All authors. ICMJE criteria for authorship read and met: All authors.
Availability of data and materials
All data generated or analyzed during this study are included in this published article (and its supplemental information files). Statistical analysis code is available on request from FP. The dataset analyzed during the current study cannot be shared under the current protocol and ethics committee approval.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Ethics approval and consent to participate
The study was approved by the institutional review board of the Medical University of Graz, Austria; document number 32-660 ex 19/20. Written informed consent was not obtained from individual patients because this is not mandated in Austria for retrospective database studies given approval by an ethics committee.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from Servier Austria GmbH. The hypothesis of this study was not suggested by the sponsor, and the funding body had no role in the design, analysis, and publication of the current analysis.
Patient involvement
Patients were neither involved in the design or conduct of this study, nor in the writing of this manuscript.
Transparency declaration
The lead author (JMR) affirms that the manuscript is an honest, accurate, and transparent account of the study being reported and that no important aspects of the study have been omitted.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.