
Abstract
Background:
Chemotherapy is an established treatment for stage III colon cancer cases. Older age is known to be associated with less chemotherapy use in these patients, but there might be other relevant factors besides age that influence treatment administration. We summarized evidence on associations between comorbidity and adjuvant chemotherapy administration in stage III colon cancer patients in a systematic review and meta-analysis.
Methods:
We searched the PubMed and Web of Science databases up to 2 June 2020 for studies on comorbidities and chemotherapy use in patients with stage III colon cancer. Summary odds ratios (OR) and 95% confidence intervals (95% CI) were estimated using random-effects models. Subgroup analyses according to year of colon cancer diagnosis, timing of comorbidity assessment, and geographical region were also conducted.
Results:
Thirty-three studies were included in this review, including 219,406 stage III colon cancer patients overall. Chemotherapy administration was 60.9% (95% CI: 56.9% to 64.9%), increasing from 57.1% before 2001 to 66.3% after 2010. There were inverse associations between comorbidities and chemotherapy administration. Compared with patients with Charlson comorbidity score 0, those with scores 1 (OR = 0.79, 95% CI = 0.72–0.87) and 2+ (OR = 0.49, 95% CI = 0.42–0.56) received chemotherapy less often. Among comorbidities, the strongest predictors of chemotherapy non-use were dementia (OR = 0.37, 95% CI = 0.33–0.54), followed by heart failure (OR = 0.44, 95% CI = 0.28–0.70) and stroke (OR = 0.56, 95% CI = 0.38–0.81).
Conclusions:
Merely 60% of stage III colon cancer patients receive chemotherapy. Comorbidities are strong predictors of chemotherapy non-use, but the association differs by comorbid condition and is strongest with dementia. Given the survival disadvantage of colon cancer patients with comorbidities, further evidence on the risk–benefit ratio of chemotherapy according to the type and severity of comorbidity and on the extent to which the survival disadvantage of comorbidity is explained by less use or lower tolerability of chemotherapy is needed to foster personalized medical care in these patients.
Background
Colorectal cancer is the third most commonly diagnosed malignancy and the second major cause of cancer death worldwide. 1 Approximately two-thirds of colorectal cancers occur in the colon. 1 In recent decades, surgical resection of colon cancer tumors has been complemented by postoperative chemotherapy mainly for stage III patients. 2 Although stage II patients with high-risk features (e.g. presence of lymphovascular and perineural invasion) appear to benefit from chemotherapy, 3 application of chemotherapy in this patient group is controversial. In stage III patients, clinical trials have suggested that chemotherapy use is associated with about 25% reduction in all-cause mortality.4,5
Despite the benefits of chemotherapy for stage III colon cancer, between one-third and nearly half of the patients still do not receive this effective treatment.6,7 Older age is the main determinant of chemotherapy non-use,6,8,9 but about one-fifth of patients younger than 75 years do not receive chemotherapy,9,10 suggesting that there might be other relevant factors that affect treatment administration aside from age. Colon cancer is mainly diagnosed at older age, when comorbidities (e.g. diabetes) are common11,12 and they might impact treatment decisions. It is well documented that comorbidities are strongly associated with poorer colon cancer prognosis, 13 and mediation by less chemotherapy utilization by patients with comorbidities has been suggested as one of the possible mechanisms underlying this association. 14
In recent years, several studies have evaluated associations between comorbidities and chemotherapy use in patients with stage III colon cancer. However, no study has summarized results from such studies in a systematic review or a meta-analysis. Quantification of this association is important, as it may have clinical relevance and may confound the association between chemotherapy and patient survival in observational studies. Herein, we conducted a systematic review and meta-analysis to summarize evidence on associations between comorbidity and administration of adjuvant chemotherapy in stage III colon cancer patients, paying particular attention to whether the associations also differ by specific comorbidities, age, year of diagnosis, timing of comorbidity assessment, or geographical region.
Methods
Search strategy
We systematically searched PubMed and Web of Science (Core Collection) from inception (1978 and 1995, respectively) to 2 June 2020 for relevant studies. For the PubMed search, the following search strategy was used, incorporating Medical Subject Headings (MeSH) terms: (comorbidity OR comorbidities OR multimorbidity OR “chronic diseases”[Title/Abstract] OR “chronic conditions”[Title/Abstract] OR “chronic illnesses”[Title/Abstract] OR comorbidity[MeSH]) AND ((chemotherapy OR “adjuvant treatment” OR treatment[Title/Abstract] OR “adjuvant therapy” OR chemotherapy[MeSH]) AND (use OR uptake OR receipt OR nonuse OR underuse OR initiation OR administration OR utilization OR adherence OR patterns)) AND (“colon cancer” OR “bowel cancer” OR “colonic cancer” OR “colonic neoplasms”[MeSH]). Further details of the search strategy have been summarized in Supplemental Table S1. We also hand-searched the reference lists of articles for additional relevant studies. This review was conducted in accordance with the PRISMA 15 and MOOSE guidelines, 16 and its protocol was registered with PROSPERO (registration number CRD42020187250).
Eligibility criteria
Studies were eligible for inclusion in this review if they: (i) were published observational studies that assessed comorbidity [summary measures or specific diseases such as diabetes, myocardial infarction, heart failure, renal disease, stroke, chronic obstructive pulmonary disease (COPD), or dementia] and their associations with adjuvant chemotherapy use in stage III colon cancer patients; and (ii) reported risk estimates of these associations [e.g. odds ratios (ORs) or relative risks (RRs) and 95% confidence intervals (95% CIs)] or provided sufficient information to calculate them. We defined chemotherapy use as receipt of any chemotherapy regimen after colon cancer surgery.
We did not consider clinical trials because participants of such studies are often younger 17 and have lower comorbidity compared with cancer patients in the real-life setting.18,19 Studies on colorectal or colon cancer patients in general that did not provide results specific for stage III colon cancer patients were excluded, except for those that analyzed stage III together with high-risk stage II patients because high-risk stage II patients represented a small fraction of the study populations (<15%). In case multiple studies used the same study population, the less informative articles were excluded (Figure 1). Studies published as abstracts or posters only were excluded because their information was not sufficient for quality assessment.
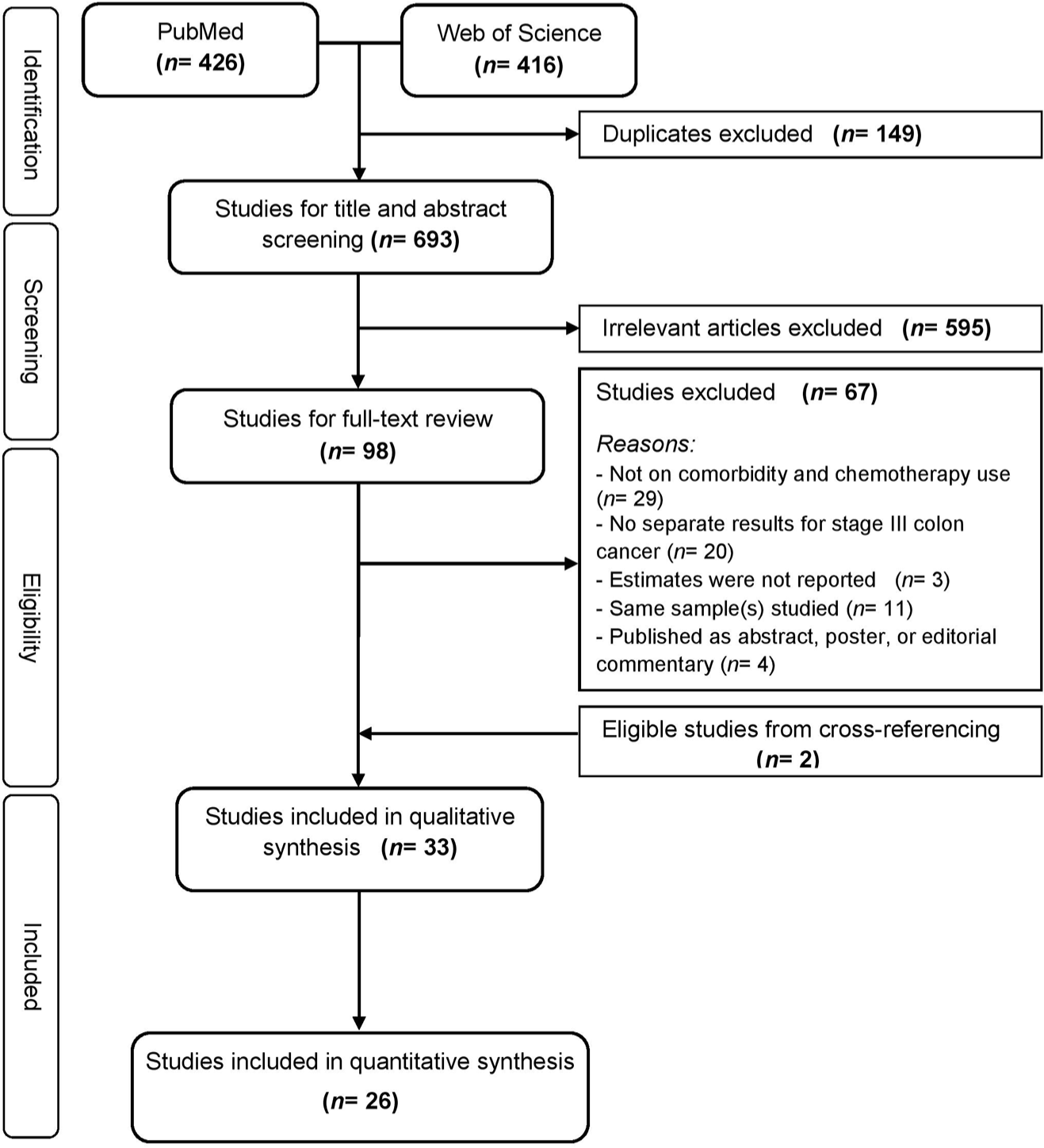
PRISMA flow diagram showing selection of eligible studies.
Data extraction and quality assessment
Two authors (DB and KG) used pre-designed data extraction forms to abstract data from the eligible studies independently. One of the forms summarized basic characteristics of the studies (e.g. first author, country, period of colon cancer diagnosis, sample size), as reported in Table 1. The second form summarized the results of each of the studies as well as the covariates that were adjusted for, as shown in Supplemental Tables S2–S3. We used the Newcastle–Ottawa Scale 20 to assess the quality and risk of bias of the included studies. In brief, the included studies were assessed against the following criteria: (i) representativeness of the study sample, (ii) valid assessment of comorbidities, (iii) appropriate ascertainment of chemotherapy use, and (iv) adjustment for at least age and year of colon cancer diagnosis in the multivariable analysis. Further details of the assessment criteria and corresponding scores are shown in Supplemental Table S4. The highest achievable score was nine: higher scores indicate high quality and low risk of bias. In case of initial disparity in the data extraction or quality assessment between the two authors, consensus was achieved through additional review and comprehensive discussion.
Characteristics of the included studies on comorbidities and chemotherapy administration.

Included high-risk stage II colon cancer patients.
Mean age.
Eight European cancer registries (Belgium, Estonia, Germany, Italy, Poland, Portugal, Slovenia, and Spain).
1990–1991, 1995, 2000–2005, and 2010.
Up to the time of administration of chemotherapy.
For estimate of prevalence only (assessed the association between dementia and chemotherapy use).
Quality assessment was conducted using the Newcastle–Ottawa scale [RE, Representativeness of sample; EX, Exposure assessment; O, Outcome (chemotherapy) assessment; AD, Adjustment for at least age and year of diagnosis]—higher scores indicate high quality and low risk of bias.
ACE-27, Adult comorbidity evaluation-27; CCI, Charlson comorbidity index; Chemo, Adjuvant chemotherapy; NR, Not reported; NZ, New Zealand; Prop, Proportion of patients with comorbidity; Pros, Prospective; RCS, Royal College of Surgeons; Retro, Retrospective; UK, United Kingdom; USA, United States of America.
Statistical analysis
Studies that used the same summary measure [e.g. Charlson comorbidity index (CCI) 50 and Adult comorbidity evaluation (ACE-27) 51 ] or assessed similar comorbid conditions were selected for meta-analysis, if their reference groups allowed for combination of risk estimates. We treated RRs and ORs as equivalent estimates because they were all derived from cohort studies. In brief, we log-transformed the extracted estimates and calculated their standard errors indirectly. 52 We then used both the fixed-effect and random-effects models to estimate summary ORs. Results from the random-effects models are reported as the main results because they take into consideration both within- and between-study heterogeneity. 53 When studies reported risk estimates for CCI scores >2 separately, the estimates were first pooled using a fixed-effect model before including them in the main analysis (e.g. ORs for CCI 2 and 3+ were combined to get an estimate for category CCI 2+).23,40,41,48 Some studies also reported results stratified by sources of comorbidity information (in-patient and outpatient records) 21 and age at diagnosis only (<75 and 75+ years),10,27 which we combined in a similar way to derive estimates for all comorbidity sources and for all ages, respectively.
We assessed heterogeneity between studies using the I 2 statistic, where I 2 >50% indicated substantial heterogeneity. 54 We also used the Egger’s test to assess potential publication bias aside from visualization with the funnel plot. 55 The Trim-and-Fill funnel plot method was moreover used to investigate and correct for potential publication bias. 56 We also conducted subgroup analyses by combining studies according to specific comorbidities, timing of comorbidity assessments, year of colon cancer diagnosis, geographical region, and quality score. Variations (heterogeneity) in the associations between comorbidity and chemotherapy use according to these factors were evaluated using a random-effects meta-regression.
Two-sided statistical testing was employed, with a significance level of 5%. All analyses were performed with the SAS software, version 9.4 (SAS Institute, Cary, NC) and the “meta” package (version 4.12-0) 57 in R, version 3.6.3 (R Development Core Team).
Results
Literature search and characteristics of the included studies
The literature search yielded 842 records: 426 from PubMed and 416 from Web of Science (Figure 1). After removal of duplicates and full-text review, 33 studies were included in this review. Of the 33 studies, 26 using similar comorbidity scores and groupings or analyzing similar specific comorbid conditions were included in the quantitative synthesis. Of studies included in this review, the majority (91%) were from North America (18/33) and Europe (12/33, Table 1). Nearly all the studies from North America originated in the USA (16/18), and half the studies from Europe were from the Netherlands (6/12). Almost all the included studies were cohort studies (32/33), the vast majority using data from population-based cancer registries linked to hospital data (28/33). A majority of the studies referred to patients diagnosed before 2010 (26/33). Over half of the studies included patients of all ages (21/33), whereas nearly half of the studies from the USA (7/16) included only patients aged 65+ years. The sample sizes ranged from 126 to 124,008 patients, with a total of over 219,406 colon cancer patients. Two smaller studies additionally included high-risk stage II colon cancer patients.37,48 The majority of the studies adjusted for at least age in the analyses, with the exception of six studies reporting crude results only.10,14,27,36,37,47 The median quality assessment score of the studies was 7/9 (interquartile range, 6–7).
Assessment of comorbidity
About one-third of the studies (13/33) determined comorbidities before or up to colon cancer diagnosis (Table 1), whereas approximately one-fifth (7/33) determined comorbidities before colon cancer surgery or during hospitalization for colon cancer surgery. The majority of the studies evaluated comorbidities from administrative data (25/33), whereas one-fourth assessed them from medical records (8/33). A majority of the studies used summary measures of comorbidity (27/33), mostly the CCI or its adaptation (22/27), with few using the ACE-27 (n = 3) or numeric count (n = 3).
Our meta-analysis of 23 studies providing data on the prevalence of comorbidity showed that over half of the patients had at least one comorbid condition (51.3%, 95% CI: 42.8% to 59.6%; Table 2), but they differed by summary score. For example, while the prevalence of comorbidities in patients assessed with ACE-27 was 78.8%, it was 45.0% in patients assessed with CCI (p < 0.001). The prevalence of comorbidities also differed by geographical region even among studies that used the CCI. For example, CCI score >0 was higher in Europe than in North America (56.2% versus 40.3%), even though almost all the studies from Europe included patients of all ages, whereas nearly half of the North American studies included only patients aged 65+ years. The prevalence of comorbidities increased from 38.8% in the studies including patients diagnosed before 2001 to 53.1% in those including patients diagnosed after 2010.
Prevalence of comorbidity and administration of adjuvant chemotherapy, overall and by year of cancer diagnosis and geographical region.
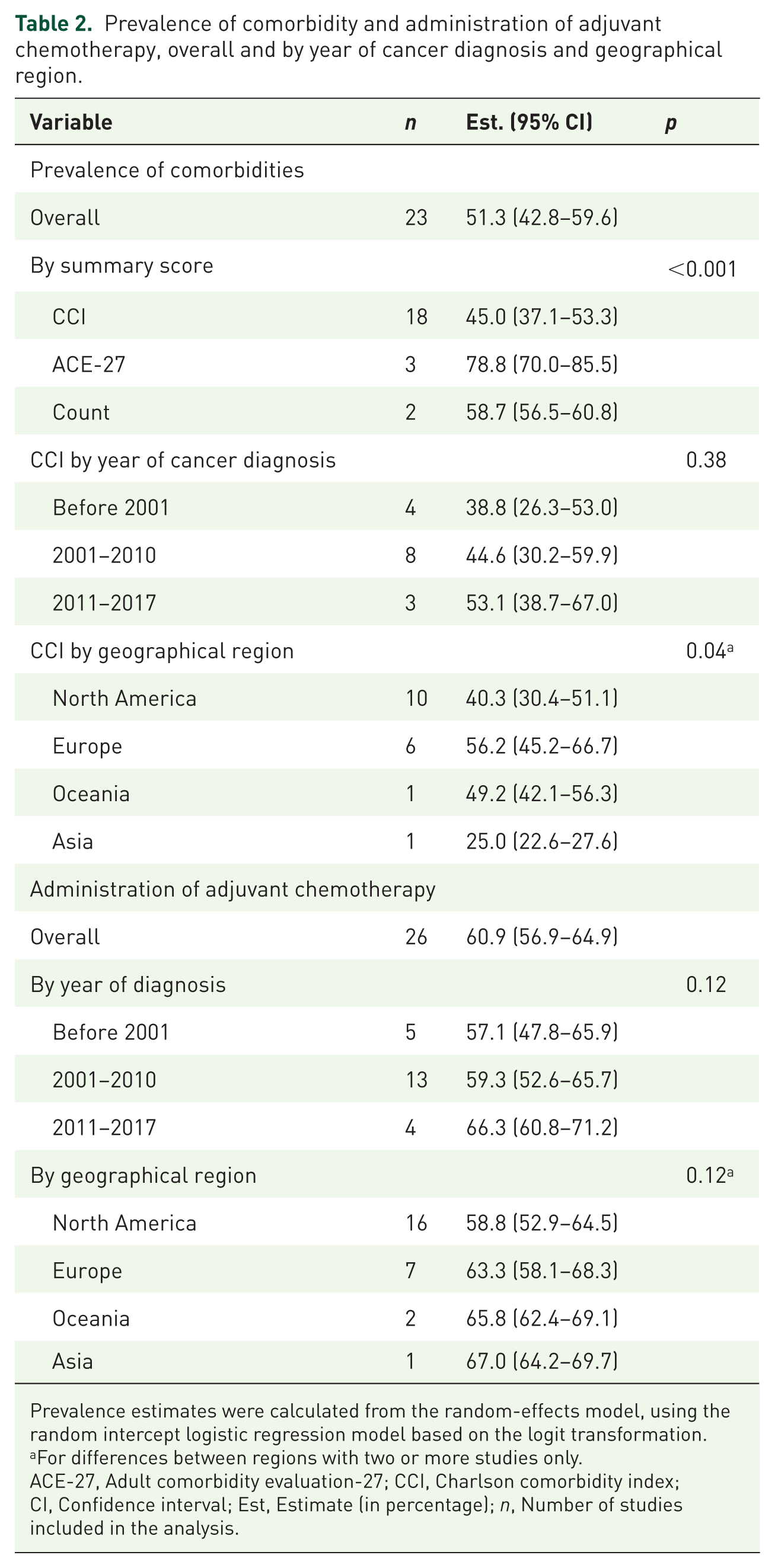
Prevalence estimates were calculated from the random-effects model, using the random intercept logistic regression model based on the logit transformation.
For differences between regions with two or more studies only.
ACE-27, Adult comorbidity evaluation-27; CCI, Charlson comorbidity index; CI, Confidence interval; Est, Estimate (in percentage); n, Number of studies included in the analysis.
Chemotherapy administration
Of 26 studies providing data on chemotherapy use (Table 2), the proportion of patients receiving chemotherapy was 60.9% (95% CI, 56.9% to 64.9%). Chemotherapy use increased steadily over time; it increased from 57.1% in the studies whose patients were diagnosed before 2001 to 66.3% in those whose patients were diagnosed after 2010 (p = 0.04). Chemotherapy administration was 63.3% in Europe and 58.8% in North America (p = 0.25).
Associations of overall comorbidity with chemotherapy administration
Twenty-seven studies evaluated the associations of summary measures [quantified by CCI (n = 22),7,9,10,21,23,25,26,29,31–33,35,40–49 by ACE-27 (n = 3),27,36,39 or by numeric count (n = 3)22,28,47—one study reported results for both CCI and numeric count 47 ] with chemotherapy use (Supplemental Table S2). Regardless of how overall comorbidity was quantified, comorbidity was inversely associated with chemotherapy administration, but the associations were not statistically significant in some of the smaller studies.31,39,46,49 In one study, associations of comorbidities with chemotherapy non-use were only seen for comorbidities obtained from in-patient records, but not for those obtained from outpatient records. 21
Results from 15 out of the 22 studies using the CCI and with similar comorbidity groupings were combined in a meta-analysis (Figure 2).9,10,21,23,25,32,35,40–44,47–49 Compared with patients with CCI score 0, those with scores 1 (OR = 0.79, 95% CI = 0.72–0.87) and 2+ (OR = 0.49, 95% CI = 0.42–0.56) received chemotherapy less often. There was a high degree of heterogeneity in the results (I2 = 88%, pheterogeneity < 0.01 and I2 = 85%, pheterogeneity < 0.01 for CCI scores 1 and 2+, respectively). The funnel plot suggested mild publication bias in the results for CCI 1 (Egger’s test p = 0.06) but not for CCI 2+ (Egger’s test p = 0.33, Supplemental Figure S1). Correction with the Trim-and-Fill method led to an attenuation of the OR of chemotherapy use to 0.89 (95% CI = 0.81–0.97, for CCI 1 versus 0).

Meta-analysis of overall comorbidity quantified by CCI and chemotherapy administration.
Our meta-analysis of studies on the associations of overall comorbidity quantified by ACE-27 score27,36,39 and numeric count22,28,47 with chemotherapy administration is illustrated in Figure 3. The associations of ACE-27 with chemotherapy administration were modest, with only the severe versus no comorbidity difference reaching statistical significance (OR = 0.52, 95% CI = 0.31–0.86). There was no evidence of heterogeneity in the results, and the funnel plot did not suggest any publication bias (data not shown). For the numeric count, we observed an inverse association between number of comorbidities and chemotherapy use. Compared with patients with no comorbidity, those with one and 2+ comorbidities had 44% (OR = 0.56, 95% CI = 0.33–0.94) and 75% (OR = 0.25, 95% CI = 0.09–0.69) lower odds of receiving chemotherapy, respectively. There was a high degree of heterogeneity (I2 = 84%, pheterogeneity < 0.01 and I2 = 93%, pheterogeneity < 0.01 for one and 2+ comorbidities, respectively) due to one small study that reported crude results only. 47 Removal of that study yielded an I2 of 0% (pheterogeneity = 0.15) and the associations were attenuated (data not shown). However, patients with one and 2+ comorbidities still had significantly lower odds of chemotherapy use, 25% and 57%, respectively.

Meta-analysis of overall comorbidity quantified by ACE-27 score and numeric count and chemotherapy administration.
Associations of individual comorbidities with chemotherapy administration
Our meta-analysis of studies on the associations of diabetes (n = 5),24,34,37,38,48 myocardial infarction (n = 2),39,48 heart failure (n = 4),24,37,39,48 stroke (n = 2),38,48 renal disease (n = 2),34,48 COPD (n = 6),22,24,37–39,48 and dementia (n = 5)14,21,30,34,39 with chemotherapy administration is shown in Figure 4. Patients having any of these diseases received chemotherapy less often, but the associations with myocardial infarction and renal disease were not statistically significant. Associations varied by comorbid condition and were strongest for dementia (OR = 0.37, 95% CI = 0.33–0.54), followed by heart failure (OR = 0.44, 95% CI = 0.28–0.70) and stroke (OR = 0.56, 95% CI = 0.38–0.81). We observed no indication of publication bias (Egger’s test p > 0.13), but the associations for renal disease, COPD, and dementia were heterogeneous. Meta-regression analysis suggested that interactions of COPD with age and year of colon cancer diagnosis accounted for all the between-study heterogeneity (~100%) in the associations for COPD (pmoderation = 0.018; data not shown). For the associations with dementia, interaction with year of colon cancer diagnosis explained about 80% of the between-study heterogeneity (pmoderation = 0.035).

Meta-analysis of specific comorbidities and chemotherapy administration.
Subgroup analyses of overall comorbidity and chemotherapy administration
Age at colon cancer diagnosis
Three studies conducted subgroup analyses by age (<75 and 75+ years, Supplemental Table S2).10,27,33 While comorbidity was inversely associated with chemotherapy use in younger patients (<75 years), no associations were seen in older patients (75+ years). In one of the studies, there was a significant interaction between comorbidity and age (pinteraction = 0.004). 33
Comorbidity assessment time, year of diagnosis, geographical region, and quality score
Inverse associations between CCI score and chemotherapy use were observed irrespective of timing of comorbidity assessment, year of colon cancer diagnosis, geographical region, or quality score (Table 3). The results from the studies determining comorbidities before/at colon cancer surgery, referring to patients diagnosed in 2001–2010, and from North America were heterogeneous. Meta-regression analysis showed that interactions of CCI score with timing of comorbidity assessment and year of colon cancer diagnosis explained all the between-study heterogeneity (~100%) in the associations for CCI 2+ (versus 0, pmoderation < 0.001), with year of diagnosis alone explaining about 70% of the between-study heterogeneity (pmoderation = 0.003). The between-study heterogeneity in the associations for CCI 1 (versus 0) was not explained by these factors (data not shown).
Subgroup analysis of studiesa on associations between overall comorbidity quantified by the Charlson comorbidity index and chemotherapy administration.

Reference group is patients with CCI score 0 (OR <1.00 indicates lower likelihood of receiving chemotherapy).
Two studies reporting crude results only were excluded (van den Broek et al. 47 and Yamano et al. 10 ).
Based on the Newcastle–Ottawa scale.
p-values assess between-study heterogeneity of associations in the subgroups and were calculated from the random-effects meta-regression using the restricted maximum likelihood method for estimation of between-study variance.
CCI, Charlson comorbidity index; CI, Confidence interval, n, Number of studies; OR, Odds ratio.
Discussion
We summarized evidence on the associations between comorbidities and chemotherapy administration in stage III colon cancer patients in a systematic review and meta-analysis, with a particular focus on potential variations in the associations by specific comorbidities. We observed a strong inverse association between comorbidity and chemotherapy use, but the association differed by comorbid condition. Comorbidities showing the strongest associations with chemotherapy non-use were dementia, followed by heart failure and stroke.
Our meta-analysis demonstrated that the prevalence of comorbidity differed by geographical region, even among studies using the CCI. For example, comorbidities were higher in Europe than in North America. A possible explanation is that the majority of the studies from North America evaluated comorbidities from administrative data, which have been suggested to mostly underestimate the prevalence of comorbidities. 58 Our meta-analysis also showed improvement in comorbidity assessment or documentation over time, as comorbidities were higher in the studies that included patients with more recent years of colon cancer diagnosis. This may also explain the observed higher comorbidities in Europe than in North America because the studies from Europe included patients with more recent years of diagnosis.
Our study showed that chemotherapy administration has increased over time—from 57% in patients diagnosed before 2001 to 66% in patients diagnosed after 2010. However, we found that merely 60% of the patients received chemotherapy, despite the established benefits of chemotherapy for stage III colon cancer cases.4,5,44,59 Our meta-analysis of 15 cohort studies including 177,018 patients showed that patients with mild (CCI 1) and moderate–severe comorbidity (CCI 2+) had 21% and 51% lower odds of receiving chemotherapy, respectively. Similar patterns of inverse associations between comorbidity and chemotherapy use were observed across subgroups defined by timing of comorbidity assessments, calendar year of diagnosis, and geographical region. Concerns about efficacy and less tolerability of chemotherapy might explain the observed disproportionately lower chemotherapy use in comorbid patients. However, evidence on the risk–benefit ratio of chemotherapy in stage III colon cancer patients is still sparse. Data from three cohort studies24,25,60 suggest that some patients with comorbidities may derive similar survival benefits from chemotherapy as those not having comorbidities. A pooled analysis of four trials also suggested that patients with comorbidities experience comparable adverse treatment effects as non-comorbid patients. 61 In the clinical trials, the incidence of grade 3/4 adverse effects in patients with CCI scores 0–1 and 2+ who received oxaliplatin-based treatments were 54% versus 56%, respectively. However, the trials sampled relatively healthy patients. Also, the CCI is only a summary measure of a broad and heterogeneous group of comorbidities. It is thus not clear which specific comorbidities (type, severity) have an impact on the risk of severe adverse effects. The observational studies also did not consider severity of comorbid conditions, frailty, or functional status.24,25,60 Thus, confounding by indication and residual confounding due to insufficient adjustment for comorbidities may have led to biased results in these studies. Further studies overcoming these important limitations are required to clarify in which comorbid patients and to what extent application of chemotherapy may improve health outcomes. Also, the majority of the studies assessing the effect of chemotherapy have focused on survival as an endpoint,4–6,44,59 but evaluation of quality of life is also important.
Among the included studies reporting age-stratified analysis,10,27,33 comorbidities were associated with chemotherapy non-use in patients aged <75 years, whereas no associations were seen in older patients (75+ years). Although there is no upper age limit for administration of chemotherapy,2,62 several studies have demonstrated substantially less frequent chemotherapy administration in older patients,6,8,9 due to concerns about the risk–benefit relation of chemotherapy in this patient group. Our results indicate that comorbidities might play more important roles in treatment decisions in younger than in older patients. However, the lack of significant associations among older adults might be due to small number of patients without comorbidities or receiving chemotherapy in this age group. Further research providing age-stratified analysis is thus needed to clarify whether and to what extent the association between comorbidity and chemotherapy use differs by age.
Although comorbidity was inversely associated with chemotherapy use irrespective of how overall comorbidity was quantified, the associations were generally modest for the ACE-27 score. This indicates that the effects of comorbidity on treatment administration may differ by summary scores and appear to be more pronounced for the CCI score. Reasons for this disparity are unclear, but a possible explanation may be the inclusion of a large number of comorbidities in the ACE-27, 51 some of which may be less correlated with chemotherapy use, unlike the CCI which considers only 19 comorbidities. 50 Also, in one of the included studies, comorbidities obtained from outpatient records only were not associated with chemotherapy use, whereas strong associations were reported for those obtained from in-patient records. 21 This suggests that studies using information from outpatient records only for risk adjustment may less accurately estimate the effect of comorbidities, leading to residual confounding. Further research comparing the predictive capacities of various comorbidity scores and information sources regarding treatment use will be useful, as lower comorbidity of chemotherapy recipients has been suggested to be associated with better survival. 48
Because summary scores provide little information on the specific diseases that mainly affect treatment administration, we additionally conducted a meta-analysis on individual comorbidities. We found that the associations between comorbidities and chemotherapy use differed by comorbid condition. Dementia was the strongest predictor of chemotherapy non-use, followed by heart failure and stroke. Reasons for the stronger association with dementia are unclear, but mediation by patient refusal may play a key role. Patient refusal is one of the common reasons for chemotherapy non-use, 8 and cognitive impairment due to dementia could result in patient refusal, by interfering with patient communication, consent for treatment, or adherence to therapeutic advice. 30 Another important finding that warrants further investigation is the appropriateness of using summary scores for confounder adjustment in studies whose outcomes are not related to mortality. For instance, in the CCI, heart failure, COPD, diabetes, and dementia have a weight of one, whereas renal disease has a weight of two. 50 We, however, observed that the associations of dementia and heart failure with chemotherapy non-use were stronger than that of renal disease. Because the CCI weights were derived from mortality risk estimates, it is possible that the risk estimates for treatment use vastly differ from those for mortality, as observed in our study. This suggests that using information on type and severity of comorbidities, rather than summary scores, may provide better adjustment for confounding in observational studies.
There are several other possible mechanisms through which comorbidities may affect chemotherapy administration. First, evidence suggests that patients with comorbidities are less likely to be referred for oncological assessment and chemotherapy treatment,63,64 both of which are associated with chemotherapy use. 65 Second, patients with comorbidities have increased risk of postoperative complications after colon cancer surgery, 35 which have also been suggested to be strongly associated with chemotherapy non-use.35,41 Third, in many countries, contraindications of chemotherapy include poor functional status, 62 which strongly correlates with comorbidity. 66
Our findings highlight differences in important characteristics such as comorbidities between recipients and non-recipients of chemotherapy. Yet, many observational studies evaluating the effects of chemotherapy in colon cancer patients lack information on comorbidities.6,67 Also, most studies adjusting for comorbidities have only considered those relevant for calculating specific summary scores.44,48,59 For example, although psychotic disorders such as schizophrenia are associated with increased mortality in colon cancer patients,30,68 they are not part of the CCI. 50 This may explain in part why estimates of chemotherapy benefits are usually larger in observational studies6,44,59 than in clinical trials.4,5 Treatment effect estimates from observational studies should thus be interpreted with caution, as they may be affected by residual confounding due to suboptimal ascertainment of comorbidities and rarely measured factors such as frailty.
Our study was the first to quantify to what extent comorbidities influence chemotherapy administration in colon cancer patients in a meta-analysis. The quality of the included studies was high, and the majority adjusted for at least age, the main predictor of chemotherapy use.6,8,9 There was, however, heterogeneity in some of the results, mainly due to differences in year of colon cancer diagnosis possibly because of changing treatment recommendations. 69 Because treatment regimens vary by age or year of diagnosis, 69 we defined the outcome of this review as receipt of any chemotherapy regimen. For instance, the efficacy and safety of oxaliplatin-based therapies in older patients are still controversial and hence rarely applied in this patient group. 70 Older patients are thus often given less aggressive treatments (e.g. capecitabine monotherapy, a 5-fluorouracil pro-drug), but survival benefits of different regimens in older patients are comparable. 71 Also, the inverse associations between comorbidity and treatment administration might be stronger for aggressive (e.g. oxaliplatin-based therapies) than for less aggressive treatments, which might explain in part the observed stronger associations in younger patients. Future studies should assess this knowledge gap.
Our study has some limitations. First, even though we did not restrict our electronic literature search to specific languages, it is possible that some relevant studies (e.g. those published in languages other than English or German) were missed. Also, like all reviews, our results might be affected by selective reporting arising from unpublished studies with non-significant results. However, the funnel plot suggested only mild publication bias in the results for CCI score. Second, the use of various comorbidity scores and groupings precluded us from combining results from all the included studies. However, similar patterns of inverse association between comorbidity and chemotherapy administration were also reported by those studies that could not be included in this meta-analysis.7,26,29,31,33,45,46 Third, about one-third of the studies did not report when comorbidities were determined,10,25,34–37,39,40,42,46,49 and one study determined comorbidities up to the time of chemotherapy administration. 45 These might result in reverse causality (e.g. comorbidities due to chemotherapy treatment), but the meta-regression analysis showed no indication of significant effect modification by timing of comorbidity assessments. Lastly, other factors such as microsatellite instability 72 and functional status 62 also affect treatment decisions, but only three studies adjusted for functional status.9,48,49
Conclusion
Results from this first systematic review and meta-analysis suggest that comorbidities are strong predictors of chemotherapy non-use in stage III colon cancer patients besides older age. The association differs by comorbid condition and is strongest with dementia. Given the survival disadvantage of colon cancer patients with comorbidities, further evidence is needed on the risk–benefit ratio of chemotherapy according to the type and severity of comorbidity. Also, quantifications of the proportions of chemotherapy non-use that are attributable to comorbidities and the extent to which the survival disadvantage of comorbidity is explained by less use or lower tolerability of chemotherapy are research gaps. Dedicated studies answering these important questions could provide further evidence to foster personalized medical care in patients with comorbidities.
Supplemental Material
sj-pdf-1-tam-10.1177_1758835920986520 – Supplemental material for The association of comorbidities with administration of adjuvant chemotherapy in stage III colon cancer patients: a systematic review and meta-analysis
Supplemental material, sj-pdf-1-tam-10.1177_1758835920986520 for The association of comorbidities with administration of adjuvant chemotherapy in stage III colon cancer patients: a systematic review and meta-analysis by Daniel Boakye, Rajini Nagrini, Wolfgang Ahrens, Ulrike Haug and Kathrin Günther in Therapeutic Advances in Medical Oncology
Footnotes
Author contributions
Study concept and design: DB and KG. Search strategy development and literature search: DB. Extraction, analysis, and interpretation of data: DB, RN, WA, UH, and KG. Drafting of the manuscript: DB. Critical revision of the manuscript for important intellectual content: DB, RN, WA, UH, and KG. All authors read and approved the final manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support forthe research, authorship, and/or publication of this article: The publication of this article was funded by the Open Access Fund of the Leibniz Association.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.