
Abstract
Objective
To determine if there is a relationship between the levels of serum uric acid and the different Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages (1–4) classified by the severity of the airflow limitation in patients with stable chronic obstructive pulmonary disease (COPD).
Methods
Electronic databases, including PubMed®, Embase®, Web of Science™ and China National Knowledge Infrastructure (CNKI), were searched from inception to December 2018. Observational studies that reported serum uric acid levels in stable COPD patients were included. Two investigators independently extracted data and RevMan version 5.3 was used to carry out the statistical analyses.
Results
Seven studies with 932 stable COPD patients and 401 healthy control subjects were included in this meta-analysis. Serum uric acid levels were significantly higher in stable COPD patients compared with healthy control subjects (mean difference [MD] 1.91, 95% confidence interval [CI] 1.55, 2.28). Serum uric acid levels were significantly lower in the GOLD 1+2 subgroup compared with the GOLD 3+4 subgroup (MD −1.39, 95% CI −1.63, −1.15).
Conclusion
Serum uric acid might be a useful biomarker for identifying disease severity in stable COPD patients, but further studies are needed to confirm this finding.
Introduction
Chronic obstructive pulmonary disease (COPD) is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases. 1 COPD has become the third highest global cause of death affecting around 63 million individuals during 1990–2010. 2
As a routine laboratory index, serum uric acid is frequently used to evaluate the renal function of patients and it has also been shown to be the main contributor to the antioxidant capacity. 3 Previous studies demonstrated that uric acid could be an independent biomarker of impaired prognosis for some extrapulmonary diseases (such as congestive heart failure and metabolic syndrome), which may be associated with impaired oxidative metabolism.4–6 Furthermore, the association between the levels of serum uric acid and the severity of pulmonary disease has also drawn more and more attention.7–9 Although there have been some studies reporting serum uric acid levels in COPD, the sample sizes of these studies were limited so that the specific association between the levels of serum uric acid and COPD remains confusing.10,11
This current meta-analysis comprehensively collected data on serum uric acid levels in stable COPD patients compared with healthy control subjects in order to: (i) determine if there is a relationship between the levels of serum uric acid and the different Global Initiative for Chronic Obstructive Lung Disease (GOLD) stages (1–4) classified by the severity of the airflow limitation; 12 (ii) determine if serum uric acid could be used as a biomarker to predict the severity of COPD and even the risk of future exacerbations.
Materials and methods
Database and literature search strategy
Electronic databases, including PubMed®, Embase®, Web of Science™ and China National Knowledge Infrastructure (CNKI), were searched from inception to December 2018, to identify relevant studies using both key words and free text words: (‘pulmonary disease, chronic obstructive’ [MeSH Terms]) and (‘Uric acid’ [MeSH Terms]). The language was restricted to English in the PubMed®, Embase® and Web of Science™ databases.
Eligibility criteria
The inclusion criteria were as follows: (i) observational studies of COPD patients with full texts; (ii) COPD patients were diagnosed using the GOLD criteria; (iii) COPD patients were in a stable condition; (iv) the serum uric acid levels were reported. The exclusion criteria were as follows: (i) conference abstracts, editorials or comments, reviews, letters, notes, theses; (ii) animal models; (iii) uric acid levels were not measured in the blood; (iv) data were incomplete.
Data extraction
First, the two investigators (H.L. & Y.C.) independently screened the titles and abstracts of the studies according to the eligibility criteria. If the studies met with the eligibility criteria, the full texts were reviewed for further selection. The findings of the two investigators (H.L. & Y.C.) were compared and any disagreements were resolved. The main characteristics that were extracted were as follows: first author, the year of publication, country/territory, study group, sample size, age range, body mass index (BMI) range and the serum uric acid levels in the COPD and control groups. The study outcomes were serum uric acid levels in stable COPD patients compared with healthy control subjects and serum uric acid levels in different GOLD stages (1–4) classified by the severity of the airflow limitation.
Statistical analyses
Statistical analyses were undertaken using RevMan software version 5.3 (Cochrane Collaboration, Oxford, UK). Continuous variables are presented as mean ± SD with 95% confidence interval (CI) and categorical variables are presented as n and percentage (%). Cochrane's Q statistic and the I2 statistic value were adapted to assess the heterogeneity. P < 0.10 or I2 statistic value ≥50% was defined as high heterogeneity and a random-effects model was applied, otherwise a fixed-effects model was used. 13 Subgroup analysis according to different territories (Asia, Africa and Europe) and sensitivity analyses that removed a study significantly deviating from the other studies were performed to explore sources of heterogeneity. Because of the limitation of the number of included studies, analysis of publication bias was not performed. This study used methodology based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines.
Results
The flow chart showing the selection process is presented in Figure 1. The initial search of the electronic databases identified 411 studies. Of these, 145 studies were removed because of duplication. The titles and abstracts of 266 articles were then screened and 229 of them were excluded (conference abstracts, editorials or comments, reviews, letters, notes, theses, animal models, irrelevant topics). After a full-text review of 37 articles, 30 that did not meet the eligibility criteria were excluded (no stable COPD patients, smokers, data incomplete, uric acid not measured in the blood). Finally, seven studies were included in this meta-analysis.10,11,14–18

Flow diagram of eligible studies showing the number of citations identified, retrieved and included in the final meta-analysis.
The characteristics of the seven included studies are presented in Table 1.10,11,14–18 The studies were published between 2007 and 2018 and originated from India, Turkey, Egypt, Spain and China. Five studies included both a stable COPD group and a healthy control group.10,11,14,15,18 Two studies only included a stable COPD group.16,17 The GOLD stages of the included patients were recorded in five studies.10,11,14,16,18 In total, 932 stable COPD patients and 401 healthy control subjects were included in this meta-analysis.

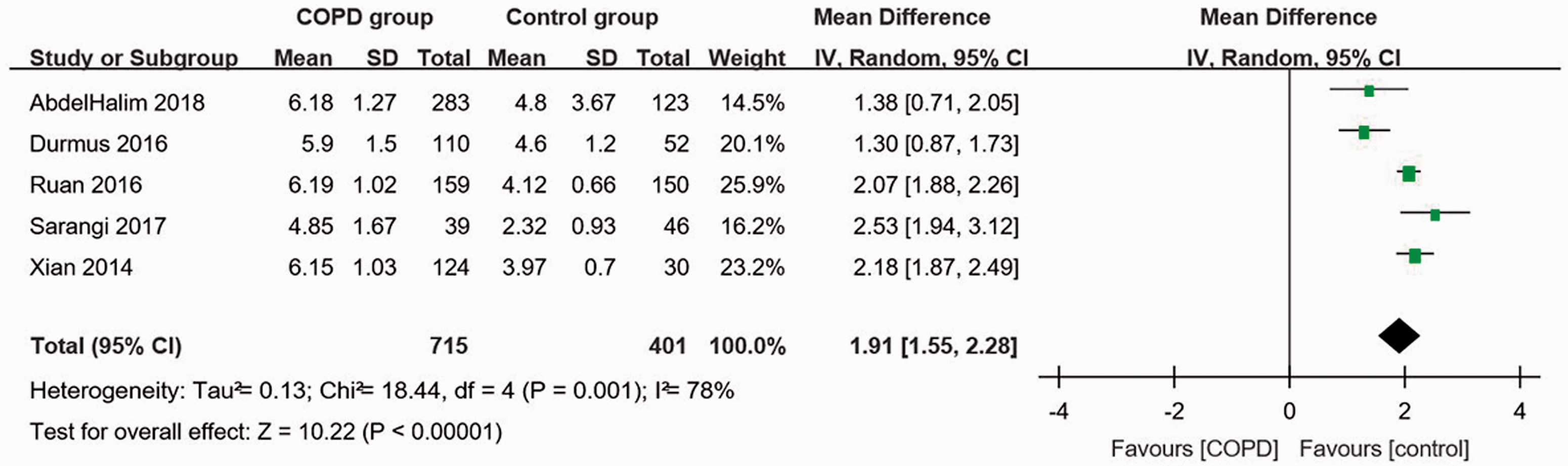
Figure 2 shows the forest plot for serum uric acid levels in the stable COPD group compared with the healthy control group. A random-effects model was used because high levels of heterogeneity were observed among the five studies.10,11,14,15,18 Serum uric acid levels were significantly higher in stable COPD patients than healthy controls (mean difference [MD] 1.91, 95% CI 1.55, 2.28, P < 0.001; I2 = 78%, P = 0.001). The forest plot for serum uric acid levels in different GOLD stages classified by the severity of the airflow limitation is shown in Figure 3.10,11,14,16,18 The GOLD 1 and GOLD 2 stages were combined into one subgroup that had less severe airflow limitations and a forced expiratory volume in 1 sec (FEV1) > 50% predicted. The combined GOLD 3 and GOLD 4 subgroup had more severe airflow limitations, with a FEV1 < 50% predicted. Serum uric acid levels were significantly lower in the GOLD 1+2 subgroup compared with the GOLD 3+4 subgroup (MD −1.39, 95% CI −1.63, −1.15, P < 0.001; I2 = 88%, P < 0.001).

When comparing serum uric acid levels in the stable COPD group with the healthy control group, three studies were from Asia, one from Africa and one from Europe.10,11,14,15,18 The forest plot for serum uric acid levels in the different territories is shown in Figure 4. The results showed that serum uric acid levels were significantly higher in the stable COPD patients than the healthy controls in all three territories (Asia: MD 2.14, 95% CI 1.96, 2.32, P < 0.001; I2 = 11%, P = 0.32; Africa: MD 1.38, 95% CI 0.71, 2.05, P < 0.001; Europe: MD 1.30, 95% CI 0.87, 1.73, P < 0.001).

There were three studies from Asia and two from Europe when comparing serum uric acid levels in different GOLD stages classified by the severity of the airflow limitation.10,11,14,16,18 The forest plot for serum uric acid levels in different GOLD stages classified by the severity of the airflow limitation in different territories is shown in Figure 5. Serum uric acid levels were significantly lower in the GOLD 1+2 subgroup in Asia (MD −1.62, 95%CI −2.17, −1.06, P < 0.001; I2 = 68%, P = 0.04). There was no significant difference between the GOLD stages 3 + 4 and 1 + 2 subgroups in Europe.

A ‘leave-one-out’ sensitivity analysis was performed in order to evaluate the impact of the heterogeneity between the studies. None of the results were altered after any one study was excluded.
Discussion
This current meta-analysis of seven studies with 932 stable COPD patients and 401 healthy control subjects that investigated the association between serum uric acid levels and COPD showed that serum uric acid levels were significantly higher in stable COPD patients than in healthy control subjects.10,11,14–18 Serum uric acid levels were significantly higher in the GOLD 3 + 4 subgroup compared with the GOLD 1 + 2 subgroup.
The results of the current meta-analysis were in agreement with several other studies. For example, two previous studies also found that both serum uric acid levels were significantly increased in COPD patients compared with healthy controls.19,20 Furthermore, two studies demonstrated that serum uric acid levels were significantly higher in patients with more airflow obstruction (GOLD stages 3 + 4) than in the milder subgroups (GOLD stages 1 + 2).20,21 A recent study showed that patients with airflow limitation had significantly higher serum uric acid levels compared with never-smoking patients without airflow limitation. 22 These findings highlight the possible role of uric acid as a biomarker for COPD and appear to support a positive correlation between serum uric acid levels and the disease severity of COPD.
However, there was also a study that reported findings that were inconsistent with those of the current meta-analysis, finding no correlation between serum uric acid levels and the disease severity of COPD. 23 The inconsistence might result from the relatively small sample size in that study, which only involved 38 patients and the levels of serum uric acid were not reported. 23
This current meta-analysis had several limitations. First, it involved seven observational studies rather than randomized controlled trials. As a result of the limited number of studies included in the meta-analysis, the degree of heterogeneity among the seven studies was high so an analysis of the extent of publication bias was not possible. Secondly, the analysis did not evaluate other potential confounding factors such as sex, age, BMI and smoking because these factors might also influence the levels of serum uric acid. Thirdly, the current meta-analysis was not registered with The International Prospective Register of Systematic Reviews, also known as PROSPERO, but this will be done for all future analyses. In addition, the study populations in some of the included studies were small, which might have had a negative impact on the statistical power. More relevant studies with larger study populations should be undertaken to further explore the role of serum uric acid levels in COPD. Future studies should also consider the potential confounding factors and control for them between the COPD and healthy control groups.
To the best of our knowledge, this is the first meta-analysis to explore the association between serum uric acid levels and COPD. This current meta-analysis demonstrated that serum uric acid levels were significantly higher in stable COPD patients than healthy control subjects, and there was a relationship between the levels of serum uric acid and the severity of the airflow limitation in stable COPD patients.
In conclusion, serum uric acid may be a useful biomarker for identifying disease severity of stable COPD patients. Further studies are warranted to confirm this finding.
Footnotes
Authors' contributions
Both authors contributed to the data analysis, drafting and revision of the article, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This study was supported by the National Natural Science Foundation of China (No. 81873410).