
Abstract
Background and aims:
Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR TKIs) are effective against classical EGFR mutations in lung cancer. However, their effectiveness and the prognosis of lung cancer patients with complex EGFR mutations are not well delineated. Therefore, we aimed to investigate the treatment effectiveness of different EGFR TKIs in patients with complex EGFR mutations.
Patients and methods:
From 2005 to 2020, we collected lung adenocarcinoma tissue samples for EGFR mutation analysis using direct Sanger sequencing. Patients with EGFR mutations treated with EGFR TKIs as first-line treatment were enrolled. Clinical characteristics, EGFR mutation status, treatment response, progression-free survival (PFS), and overall survival (OS) were analyzed.
Results:
Among 2675 patients with EGFR mutations, 239 (8.9%) had complex EGFR mutations, of whom 125 received EGFR TKI treatment as first-line treatment. Multivariate analysis revealed that afatinib was a more favorable factor for PFS than gefitinib [hazard ratio (HR), 2.01; 95% confidence interval (CI), 1.11–3.62] and erlotinib (HR, 2.61; 95% CI, 1.31–5.22), especially in patients with uncommon mutation patterns. Afatinib treatment as first-line treatment was also associated with longer OS compared with erlotinib (HR, 2.48; 95% CI, 1.20–5.12). Classical mutation pattern was associated with longer PFS (p = 0.001) and OS (p = 0.020). Secondary T790M was detected in 22 of 52 (42.3%) patients who had re-biopsied tissue samples after acquiring resistance to EGFR TKIs. There was no significant difference in secondary T790M formation after acquired resistance to the three EGFR TKIs (p = 0.261). Furthermore, three (5.8%) patients had small-cell lung cancer transformation.
Conclusion:
Afatinib is an effective first-line treatment for patients with lung adenocarcinoma harboring complex EGFR mutations, especially those with uncommon mutation patterns.
Introduction
Lung cancer is the leading cause of cancer-related death worldwide. 1 Most patients have an advanced-stage disease or distant metastases at the initial diagnosis of lung cancer. The prognosis of lung cancer is poor, and the effectiveness of standard platinum-based chemotherapy is limited. 1 The advancement of targeted therapy provides a favorable survival benefit for patients with non-small cell lung cancer (NSCLC) harboring oncogenic driver mutations, such as EGFR and B-Raf mutations or ALK and ROS-1 fusion genes.2–6
EGFR mutations are the most important predictive biomarkers of the effectiveness of tyrosine kinase inhibitors (TKIs) targeting the epidermal growth factor receptor (EGFR). 7 Deletion in exon 19 (del-19) and L858R point mutation in exon 21 are the most common types of EGFR mutation and are classified as classical mutations. 8 Patients harboring tumors with these mutations have shown favorable treatment responses to EGFR TKIs. 7
Besides classical mutations, approximately 10% of NSCLC patients with EGFR mutations have rare or uncommon mutations, including L861Q, G719X, and S768I. Such uncommon EGFR mutations are associated with a poorer prognosis and a less effective EGFR TKI treatment than classical mutations. 9 After a pooled analysis of three studies from the LUX-Lung clinical trial program (phase II LUX-Lung 2, phase III LUX-Lung 3, and phase III LUX-Lung 6), afatinib (a second-generation EGFR TKI) showed effectiveness for uncommon EGFR mutations based on the objective response rate, duration of response, disease control, progression-free survival (PFS), and overall survival (OS). 10 In 2018, afatinib was approved by the US Food and Drug Administration (FDA) for lung cancer with EGFR L861Q, G719X, and S768I mutations. 11
Most EGFR mutations in NSCLC are single mutations, but sometimes a single tumor sample can have two or more different concomitant EGFR mutations, termed as “complex EGFR mutations”. 12 The frequency of complex EGFR mutations is 3.2–6.0%.13,14 The introduction of another mutation leads to a conformational change in the EGFR tyrosine kinase domain, affecting the affinity of the receptors and the treatment response to TKIs.14,15 In our previous study, patients with complex classical EGFR mutations had the same response rate, PFS, and OS as those with single classical mutations. 16 Moreover, patients with complex EGFR mutations with the classical mutation pattern had a better response to gefitinib and longer PFS and OS than those without the classical mutation pattern. 16 However, it is unclear whether the different EGFR TKIs have the same effectiveness in patients with complex EGFR mutations.
Although there have been a few studies on complex EGFR mutations and EGFR TKIs, the sample sizes of these published studies are very small and the conclusions were inconsistent.13,16 Especially, the mechanism of acquired resistance to EGFR TKIs remains unclear in patients with complex EGFR mutations. In this study, we aim to clarify the effectiveness of different EGFR-TKIs as the first-line therapy in lung adenocarcinoma patients with complex EGFR mutations.
Materials and methods
Patients and tissue procurement
This study was conducted in the National Taiwan University Hospital (NTUH) from June 2005 to March 2020. We enrolled patients if they had (1) a stage IV disease status or stage I–III lung adenocarcinoma with a subsequent systemic relapse, (2) tumors with complex EGFR mutations, and (3) first-line systemic treatment with first-generation (gefitinib or erlotinib) or second-generation (afatinib) EGFR TKIs. To evaluate the effectiveness of EGFR TKIs, patients who received concurrent radiotherapy or combined chemotherapy and EGFR TKI treatment were excluded from the subsequent analysis. The study was approved by the Institutional Review Board of the NTUH Research Ethics Committee (REC No. 201103013RC and 201111039RIC). All patients provided written informed consent for the collection of demographic and clinical outcome data and for molecular analysis before the collection of tissue specimens, including surgically resected lung tumors, bronchoscopy biopsy/brushing specimens, and malignant pleural effusions (MPEs) from thoracentesis. Some patients had been reported in our prior studies.16–20
The International Multidisciplinary Classification of Lung Adenocarcinoma, established by the International Association for the Study of Lung Cancer (IASLC), American Thoracic Society, and European Respiratory Society, was adopted to confirm the histological classification of lung adenocarcinoma. 21 MPEs or ascites was confirmed by cytologists.
All patients underwent a complete lung cancer staging—including bronchoscopy; computed tomography (CT) of the head, chest, and abdomen; and a whole-body bone scintigraphy. The disease status was determined according to the seventh edition of the IASLC TNM staging system. 22 The patients’ clinical data, including demographic information, smoking status, performance status, treatment regimens, and imaging studies, were reviewed. Patients who had smoked fewer than 100 cigarettes in their lifetime were categorized as never-smokers, 23 whereas those who had quit smoking for more than a year were regarded as former smokers. The Eastern Cooperative Oncology Group performance status was also recorded. 24
Evaluation of treatment response to EGFR TKIs in lung adenocarcinoma patients
The enrolled patients received single-agent EGFR TKIs daily as first-line systemic treatment, with no concurrent chemotherapy or radiotherapy for the primary lung tumor during the EGFR TKI treatment course. They underwent chest radiography every 2–4 weeks and CT of the chest (including the liver and adrenal glands) every 2–3 months as routine clinical practice and as needed for the evaluation of treatment response. The treatment response was evaluated using the Response Evaluation Criteria in Solid Tumors guidelines (version 1.1). 25 The objective responses were defined as complete response, partial response (PR), stable disease (SD), and progressive disease. 25 Acquired resistance was defined as objective treatment response, including a PR to EGFR TKI treatment or durable SD (PFS, ⩾6 months), followed by disease progression. OS was calculated as the duration from the start of the first-line systemic treatment for a metastatic or disease relapse status until death from any cause. PFS was defined as the duration from the initiation of EGFR TKI treatment to disease progression or death, whichever occurred first.
EGFR mutation analysis
RNA was extracted from tissue specimens, including lung tumors, metastatic sites, and MPEs. The quantity and quality of the extracted RNA were measured by spectrophotometry. Tissue specimens were processed for EGFR mutation analysis as described previously.26,27 Exons 18–21 of the EGFR gene were amplified by reverse transcription-polymerase chain reaction (RT-PCR) using the QIAGEN OneStep RT-PCR Kit (QIAGEN, Hilden, Germany), as described previously.26,28
Complex EGFR mutations with classical and uncommon mutation patterns
The mutations were defined as complex EGFR mutations when two or more different concomitant EGFR mutations were detected, as in our previous study. 16 Complex EGFR mutations that contained either a del-19 or L858R mutation were defined as having the “classical mutation pattern”, whereas those without a del-19 or L858R mutation were defined as having the “uncommon mutation pattern”.
Statistical analysis
All categorical variables were analyzed using the chi-squared test, whereas Fisher’s exact test was used for small study sizes (<5). The median ages between groups were compared using the non-parametric Mann–Whitney U test. PFS and OS curves were plotted using the Kaplan–Meier method and compared using the log-rank test. Two-sided p-values of <0.05 were considered significant. Multivariate analysis was performed using the Cox regression model to evaluate the predictive factors of PFS and the potential prognostic factors of OS. All analyses were performed using SPSS software (version 17.0 for Windows; SPSS Inc., Chicago, Illinois, USA).
Results
Clinical characteristics of lung adenocarcinoma patients with complex EGFR mutations
From June 2005 to March 2020, we consecutively collected lung adenocarcinoma specimens. There were 4714 patients who had adequate tissue samples for EGFR mutation analysis, and 2675 patients (mutation rate, 56.7%) had tumors harboring EGFR mutations. Among the 2675 patients, there were 239 (8.9%) patients who had complex EGFR mutations, including 48 patients with de novo T790M of EGFR mutations (Figure 1). The detail of these complex EGFR mutations other than de novo T790M is shown in Supplemental Material Table 1 and Supplemental Figure 1 online. L858R was the major component of the complex EGFR mutations. We did not detect patients with complex EGFR mutations that contained exon 20 insertion in this cohort whether the patients took EGFR TKIs or not.
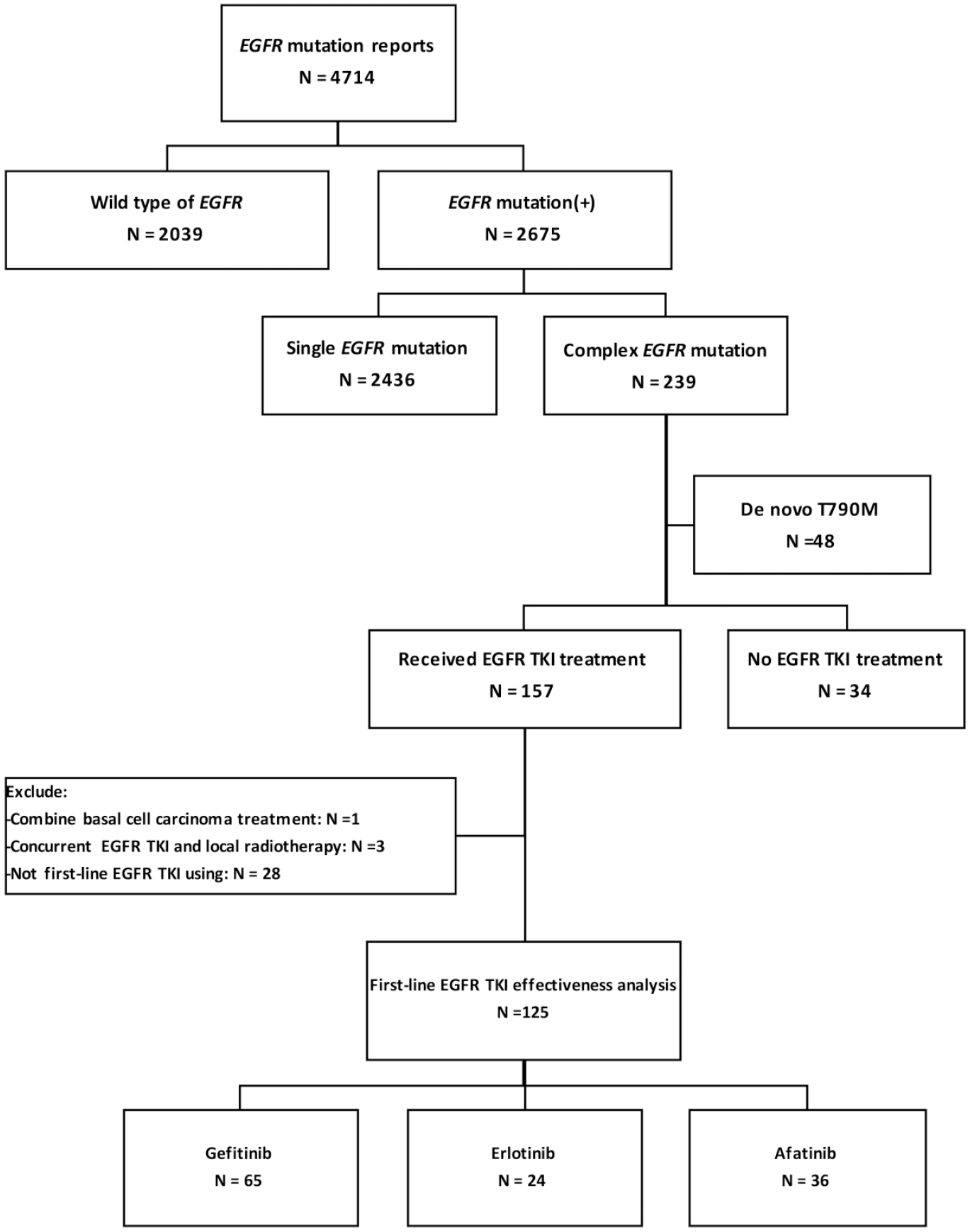
Flowchart for patient collection.
To evaluate the effectiveness of EGFR TKIs, we excluded patients with tumors harboring de novo T790M mutations due to intrinsic resistance to first- and second-generation EGFR TKIs.29,30 Only patients who received EGFR TKIs as first-line treatment were enrolled to reduce the treatment heterogenicity and potential chemotherapy impacts. We also excluded three patients who received local curative radiotherapy as a combination therapy with EGFR TKI treatment and one patient with basal cell carcinoma who received systemic treatment. Finally, we enrolled 125 lung adenocarcinoma patients with complex EGFR mutations who took EGFR TKIs as first-line treatment, to evaluate the effectiveness of the drugs.
Table 1 summarizes the clinical characteristics of the 125 patients who received EGFR TKIs as first-line treatment, including 65 (52.0%) gefitinib, 24 (19.2%) erlotinib, and 36 (28.8%) afatinib. The median age at diagnosis was 65.5 (range: 27.5–88.1) years old. Among them, 83 (66.4%) were female, 102 (81.6%) were never-smokers, and 83 (66.4%) had the classical mutation pattern. The proportions of the complex EGFR mutations are shown by Figure 2 and Supplemental Table 2. Of them, there were 68 patients (54.4%) with complex EGFR mutations that contained L858R. There were no significant differences in age, smoking history, Eastern Cooperative Oncology Group performance status, disease stage [relapse, stage IV (M1a) and stage IV (M1b)] between patients treated with the different EGFR TKIs as first-line treatment. The erlotinib-treated patients had more male, and afatinib-treated patients had more patients with uncommon mutation pattern.
Clinical characteristics of lung adenocarcinoma patients with complex EGFR mutations treated with EGFR TKIs as first-line systemic treatment.

By Kruskal–Wallis test.
Patients with stages I–III with systemic relapse after definitive surgery.
ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor gene; EGRF TKI, epidermal growth factor receptor tyrosine kinase inhibitor
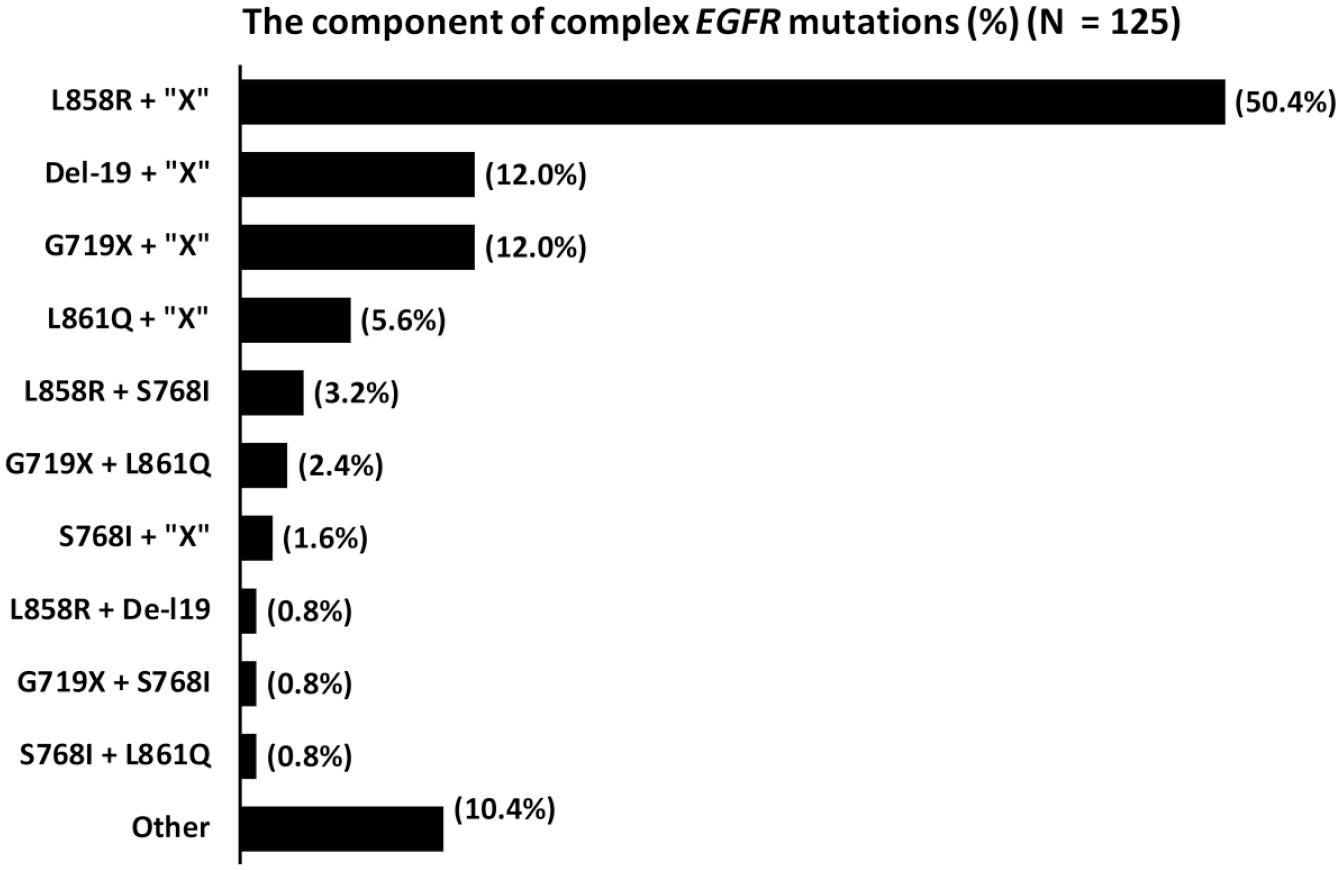
The proportion of different mutation components of complex EGFR mutations in patients who received EGFR TKIs as first-line treatment (n = 125). [del-19, deletion in exon 19; “X”, EGFR mutation other than common (L858R and del-19) and uncommon mutations (G719X, S768I, and L861Q)].
Treatment response to EGFR TKIs in lung adenocarcinoma patients with complex EGFR mutations
Among the 125 patients, there was no significant difference in the maximum treatment response rate between the three EGFR TKIs [gefitinib versus erlotinib versus afatinib: 70.8% (46 of 65) versus 62.5% (15 of 24) versus 83.3% (30 of 36); p = 0.179] (Supplemental Table 3). In addition, patients with the classical mutation pattern had a higher treatment response rate than those with the uncommon mutation pattern [81.9% (68 of 83) versus 54.8% (23 of 42); p = 0.001].
Effectiveness and survival analysis of different EGFR TKIs in patients with complex EGFR mutations
To evaluate the effectiveness of the three EGFR TKIs, the PFS and OS of the patients who received the different EGFR TKIs as first-line treatment were compared. There was no significant difference in PFS between the three drugs (gefitinib versus erlotinib versus afatinib: 7.4 months versus 8.1 months versus 9.7 months; p = 0.264) [Figure 3(A)]. There was also no significant difference in OS between the three drugs (gefitinib versus erlotinib versus afatinib: 18.4 months versus 13.3 months versus 26.4 months; p = 0.101) [Figure 3(B)].

Kaplan–Meier survival curve of progression-free survival (PFS) and overall survival (OS) in lung adenocarcinoma patients with complex epidermal growth factor receptor (EGFR) mutations who took EGFR TKIs treatment as first-line treatment. (A) There were no significant differences in PFS between the three EGFR TKIs (gefitinib versus erlotinib versus afatinib: 7.4 months versus 8.1 months versus 9.7 months; p = 0.264, by the log-rank test). (B) There were no significant differences in OS between the three EGFR TKIs (gefitinib versus erlotinib versus afatinib: 18.4 months versus 13.3 months versus 26.4 months; p = 0.101, by the log-rank test).
To clarify the interaction between complex EGFR mutation patterns and treatment responses to EGFR TKIs, patients were stratified according to the classical and the uncommon mutation patterns. For patients with the classical mutation pattern, there were no significant differences in treatment response to the three EGFR TKIs [gefitinib versus erlotinib versus afatinib: 83.0% (39 of 47) versus 73.7% (14 of 19) versus 88.2% (15 of 17); p = 0.506] and in PFS (gefitinib versus erlotinib versus afatinib: 10.9 months versus 8.5 months versus 9.6 months; p = 0.385) [Figure 4(A)].

Kaplan–Meier survival curve of progression-free survival (PFS) in the three EGFR TKI-treated adenocarcinoma patients with complex epidermal growth factor receptor (EGFR) mutations. (A) For patients with the classical mutation pattern, there were no significant differences in PFS between the three EGFR TKIs (p = 0.385). (B) For patients with the uncommon mutation pattern, there was a significant difference that the PFS of afatinib was longer than gefitinib and erlotinib (gefitinib versus erlotinib versus afatinib: 3.0 months versus 0.9 months versus 10.5 months; p = 0.013).
For patients with the uncommon mutation pattern, the second-generation EGFR TKI (afatinib) had a higher response rate [78.9% (15 of 19)] than the two first-generation EGFR TKIs [gefitinib: 38.9% (7 of 18); erlotinib: 20.0% (1 of 5)] (p = 0.013). There were significant differences in PFS between the three EGFR TKIs (gefitinib versus erlotinib versus afatinib: 3.0 months versus 0.9 months versus 10.5 months; p = 0.013). Furthermore, afatinib was associated with longer PFS than gefitinib (p = 0.011) and erlotinib (p = 0.004) [Figure 4(B)].
The patients with the classical mutation pattern had longer PFS (9.6 months versus 5.2 months; p = 0.023) and OS (27.6 months versus 15.2 months; p = 0.039) than those with the uncommon mutation pattern [Supplemental Figure 2(A) and (B)]. These results were the same in our prior reports, which showed gefitinib had good treatment efficacy in patients with classical mutation pattern. 16
Prognostic factors in patients with complex EGFR mutations treated with EGFR TKIs as first-line treatment
Multivariate analysis was performed using the Cox regression model to determine potential predictive factors of PFS, including age (<65 years versus ⩾65 years), sex, smoking, performance status, presence of the classical mutation pattern, and EGFR TKI use (Table 2). Compared with patients treated with afatinib, patients treated with gefitinib [hazard ratio (HR), 2.01; 95% confidence interval (CI), 1.11–3.62; p = 0.020] or erlotinib (HR, 2.61; 95% CI, 1.31–5.22; p = 0.007) had shorter PFS. Patients with the classical mutation pattern had significantly longer PFS than those with the uncommon mutation pattern (HR, 0.41; 95% CI, 0.24–0.69; p = 0.001). Being male (HR, 2.08; 95% CI, 1.16–3.73; p = 0.014) was significantly associated with shorter PFS. Compared with stage IV M1b, disease relapse (HR, 0.39; 95% CI, 0.21–0.72; p = 0.003) and stage IV M1a (HR, 0.55; 95% CI, 0.34–0.90; p = 0.018) at the initial diagnosis of lung cancer were favorable predictive factors of PFS.
Multivariate analysis of predictive factors for progression-free survival in complex EGFR mutant patients who have taken EGFR TKIs.

Patients with stages I to III with systemic relapse after definitive surgery.
CI, confidence interval; ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR, epidermal growth factor receptor gene; EGFR TKI, epidermal growth factor receptor tyrosine kinase inhibitor; HR, hazard ratio; y/o, years old.
For OS, multivariate analysis was also performed using the Cox regression model to determine the potential prognostic factors (Table 2). Compared with patients who received afatinib, patients treated with erlotinib had a significantly shorter OS (HR, 2.48; 95% CI, 1.20–5.12; p = 0.014), but there was no significant difference in OS from patients treated with gefitinib (OR, 1.44; 95% CI, 0.80–2.60; p = 0.226). The classical mutation pattern (HR, 0.55; 95% CI, 0.33–0.91; p = 0.020) was associated with longer OS than the uncommon mutation pattern. Being male (HR, 2.64; 95% CI, 1.41–4.94; p = 0.002) and having stage IV MIb [compared with disease relapse (HR, 0.47; 95% CI, 0.25–0.89; p = 0.020) or stage IV M1a (HR, 0.38; 95% CI, 0.21–0.67; p = 0.001)] were poor prognostic factors of OS. Pemetrexed using (HR, 0.54; 95% CI, 0.31–0.94; p = 0.029) was also a good prognostic factor.
Secondary T790M mutations and small cell lung cancer transformation after acquired resistance to EGFR TKIs
A total of 80 EGFR TKI-treated patients met the criteria of acquired resistance to EGFR TKIs, and we obtained tissue samples in 52 of them after they developed acquired resistance. The clinical characteristics of these patients are listed in Table 3. Secondary T790M mutations were detected in 22 patients (42.3%) (Table 4), and there was no significant difference in T790M mutation between patients treated with the three EGFR TKIs, gefitinib [38.5% (10 of 26)], erlotinib [66.7% (6 of 9)] and afatinib [35.3% (6 of 17)] (p = 0261).
Clinical characteristics of the patients with or without secondary T790M development after acquired resistance to EGFR TKIs.

By Mann–Whitney U test.
By Fisher’s exact test.
Patients with stages I–III with systemic relapse after definitive surgery.
ECOG PS, Eastern Cooperative Oncology Group performance status; EGFR TKI, epidermal growth factor receptor tyrosine kinase inhibitor.
Patients who have secondary T790M after acquired resistance to EGFR TKIs.

3rd-G, third generation; EGFR, epidermal growth factor receptor gene; EGFR TKI, epidermal growth factor receptor tyrosine kinase inhibitor; F, female; M, male; Max., maximum; OS, overall survival; Osi, osimertinib; PD, progressive disease; PFS, progression-free survival; PR, partial response; SD, stable disease.
There was no significant difference in the detection of secondary T790M mutations between patients with the classical [46.5% (20 of 43)] and the uncommon mutation patterns [22.2% (2 of 9); p = 0.272], using Fisher’s exact test, because of the small sample size. There were also no significant differences in PFS [T790M(+) versus T790M(−): 9.4 months versus 11.5 months; p = 0.143] and OS [T790M(+) versus T790M(−): 38.4 months versus 26.8 months; p = 0.340] between patients with and without secondary T790M mutations.
Small cell lung cancer (SCLC) transformation was detected in three (5.8%) tissue samples of with acquired resistance to EGFR TKIs (two patients for gefitinib and one for erlotinib). The three pairs of pre- and post-treatment specimens showed the same complex EGFR mutations: L858R + K757N, L858R + V834L and L858R + L833V. One post-treatment sample particularly had concomitant L858R + K757N + T790M mutations in addition to SCLC transformation. Two of the patients had a partial response after receiving etoposide/cisplatin treatment for SCLC transformation. One patient received supportive care only because of poor performance status.
Discussion
Complex EGFR mutations are a rare subtype of EGFR-mutant lung cancers. The effectiveness of different EGFR TKIs in patients with complex EGFR mutations has not been fully elucidated. The incidence of complex EGFR mutations in lung adenocarcinoma has been reported to be 0.12–16.00% in all patients with EGFR mutations,13,31 and the incidence in the current study was 5.1% (239 of 4714). Our cohort study comprised a comprehensive comparison of treatment effectiveness between different EGFR TKIs as first-line treatment in patients with complex EGFR mutations. Afatinib was a more favorable factor for PFS than the first-generation EGFR TKI, gefitinib, and erlotinib, especially in patients with uncommon mutation patterns. Compared with erlotinib, the PFS benefit of afatinib as first-line treatment also translated to overall survival benefit. Classical mutation pattern was a favorable predictive and prognostic factor of PFS and OS. The incidence of secondary T790M mutations was 42.3%. In addition to secondary T790M mutation, SCLC transformation was also one of the mechanisms of acquired resistance to EGFR TKIs among patients with complex EGFR mutations.
For patients with complex EGFR mutations with the classical mutation pattern, administration of first- and second-generation EGFR TKIs resulted in similar treatment response and PFS rates by univariate analysis. However, in patients with the uncommon mutation pattern, the second-generation EGFR TKI, afatinib, showed better effectiveness and longer PFS than the first-generation EGFR TKIs, gefitinib and erlotinib. This finding is similar to that of the LUX-Lung clinical trials, in which afatinib demonstrated clinical activity in patients with uncommon mutations L861Q, G719X, and S768I. 10 Because of the result of the previously mentioned study in 2015, clinicians of the present study might prefer to prescribed more afatinib for patients with uncommon mutation patterns. In contrast, the first-generation EGFR TKIs gefitinib and erlotinib have shown inconsistent responses in patients with uncommon EGFR mutations.32–35 In in vitro studies, afatinib had a lower half-maximal inhibitory concentration (IC50) in Ba/F3 cell lines transfected with S768I or G719X mutations than first-generation EGFR TKIs.36,37 Afatinib also had a lower IC50 in Ba/F3 cells transfected with the complex EGFR mutations L858R + L747P, L858R + D761Y, and L858R + T854A than gefitinib and erlotinib. 38 In our study, afatinib also showed clinical activity in lung adenocarcinoma of complex EGFR mutations, especially with mutations of a uncommon pattern.
Although afatinib showed better effectiveness in patients with the uncommon mutation pattern, the benefit did not reflect prolonged OS when compared with gefitinib. Such findings are similar to those of the LUX-Lung 7 clinical trial, which demonstrated no significant difference in OS between afatinib and gefitinib, although the PFS and treatment response rates were significantly improved with afatinib. 39 However, patients treated with afatinib had longer OS than those treated with erlotinib. Therefore, there may be still different effectiveness of the different first-generation EGFR TKIs. In addition, it is unknown whether specific EGFR TKIs can prolong the OS of patients with specific complex EGFR mutation types. Therefore, further studies involving a larger number of patients with complex EGFR mutations are necessary to explore the effects of different EGFR TKIs, especially the novel third-generation agent osimertinib, on survival.
In our previous study, the effectiveness of gefitinib and the OS rate in patients with complex EGFR mutations with the classical mutation pattern were similar to those of patients with single classical EGFR mutations. 40 However, an in vitro study showed that some rare types of EGFR substitution mutations suggest relative gefitinib resistance when combined with the common EGFR mutations. 41 Complex EGFR mutations with different patterns may cause various conformational changes in the EGFR protein, resulting in different sensitivities to EGFR TKIs.
The present study showed that L858R was the predominant subtype contained in the complex EGFR mutation. For single EGFR mutation, the PIONEER study demonstrated that the incidences of individual mutation types were 40.6% (303 of 746) for L858R and 43.0% (321 of 746) for del-19 in Asian patients with EGFR mutations. 42 In Taiwan, the incidences of L858R and del-19 were 43–44% and 37–51% in patients with EGFR mutations, respectively.43,44 There was no obvious difference in mutation incidences between L858R and del-19. For complex EGFR mutations, Reiss et al. and Yang et al. both reported that there were more patients with complex EGFR mutation that contained L858R than those that contained del-19.45,46 Therefore, the incidence of complex EGFR mutation that contained L858R is higher than those that contained del-19.
Recently, real-time PCR methods, such as the amplification refractory mutation system real-time PCR and Cobas systems, have been used to detect EGFR mutations in NSCLC. The real-time PCR has demonstrated higher sensitivity than that of Sanger sequencing, but is prone to missing mutations due to the use of a special primer design for prespecified known mutations. 47 To detect unknown or rare concomitant EGFR mutations, our study used Sanger sequencing, which is the gold standard for gene mutation detection. Recently, next-generation sequencing (NGS) is used to detect genetic alteration for lung cancer patients. Compared with traditional methods, NGS can comprehensively sequence complete genomes, exomes, and transcriptomes. So, rare mutation could be detected more frequently by NGS. Therefore, categorizing complex EGFR mutations according to their sensitivity to different EGFR TKIs is important to enable precision medicine.
Although patients with EGFR mutations have a favorable treatment response to EGFR TKIs initially, acquired resistance to EGFR TKI treatment can eventually develop. Various mechanisms of acquired resistance have been discovered. 48 However, T790M mutation is the most common mechanism of acquired resistance (~50%) to first- and second-generation EGFR TKIs.30,49 In the current study, the incidence of acquired T790M mutations was 42.3% among patients with complex EGFR mutations. A complex conformational change due to two or more concomitant mutations may be an obstacle to developing T790M mutations. More clinical trials are still necessary to confirm the incidence of acquired T790M mutations.
Platinum-based doublet chemotherapy has been approved as the standard treatment for patients with NSCLC. In addition, pemetrexed in combination with cisplatin or carboplatin has also been approved as first-line treatment in non-squamous patients with NSCLC and a performance status of 0–1 and EGFR-, ALK-, or ROS1-negative disease. 50 Recently, pemetrexed combined with carboplatin and gefitinib has been shown to prolong survival, although it could not prolong a second PFS. 51 Therefore, this combination therapy is also considered as first-line treatment in patients with EGFR mutations. We also showed the survival benefit of pemetrexed treatment (Table 3). However, it remains unclear whether the combination therapy of EGFR TKIs and pemetrexed/platinum can benefit patients with complex EGFR mutations.
EGFR exon 20 insertion mutations account for 1.6–5% of all EGFR mutations in Asia,52–55 and about 2–10% in Europe and USA.56–60 Our group had also reported EGFR exon 20 insertions comprised 4.0% of EGFR mutated NSCLC patients. 61 The present study showed that no exon 20 insertion was detected in the complex EGFR mutations. We explored the COSMIC database, which collected 211 lung cancers with EGFR insertion mutations, and no complex EGFR mutation with exon 20 insertion was reported. In addition, Yang et al. pooled analysis assessed the activity of afatinib in 693 patients with tumors harboring uncommon EGFR mutations, and there were also no patients harboring complex EGFR mutation with exon 20 insertion. 46 However, there were still a few patients with complex EGFR mutation that contained exon 20 insertions reported from large cohorts of patients with EGFR mutations and using high-sensitive detection methods for EGFR mutations, for example, NGS.45,52,62 For mutation analysis, low tumor contents in small lung biopsy tissue samples may cause detection limitation and pitfall. In addition, Tsai et al. demonstrated that RNA is a more favorable source for EGFR testing than genomic DNA in the highly heterogeneous specimens of MPE related to lung cancer. 27
Osimertinib is approved for first-line treatment of lung cancers with classical EGFR mutations. The efficacy of osimertinib for lung cancers with complex EGFR mutation is rarely reported. Recently, Cho et al. reported that the efficacy of osimertinib for patients with NSCLC harboring uncommon EGFR mutations, including two G719X + S768I and two G719X + L861Q, and the maximum response were three PR and one SD. 63 In addition, Yang et al. reported a case with complex mutations of EGFR H773L + V774M, who was irresponsive to gefitinib, but had sustained disease control to osimertinib in combination with bevacizumab for 12 months. 64 Astaras et al. presented a patient with complex EGFR mutations in exon 21 (L833V + H835F), showing a response to osimertinib with a PFS of 9 months. 65 Because of the limited number of patients with complex EGFR mutations, the efficacy of osimertinib in this group of patients warrants future study.
The present study showed 100% of response rates to osimertinib in patients with complex EGFR mutations that contained del-19 (2 of 2). Especially, both of the two patients with del-19 received osimertinib after acquired resistance to afatinib. Recently, the GioTag study showed that sequential afatinib and osimertinib conferred OS of about 3.5 years, and time to treatment failure of over 2 years, in NSCLC patients with EGFR mutation. 66 However, because of the limited patient numbers, it is uncertain whether osimertinib has favorable effectiveness for patients with complex EGFR mutations after acquired resistance to afatinib. Future study with more patients is warranted for this issue.
Although this study has the largest number of patients with complex EGFR mutations so far, it has some limitations. First, all included patients received first- and second-generation EGFR TKIs only. We have not evaluated the effectiveness of the third-generation EGFR TKI osimertinib, although the FDA has approved it as first-line treatment for metastatic NSCLC with classical EGFR mutations and T790M mutations. Second, the re-biopsy samples of patients after they acquired resistance to EGFR TKIs were limited. Obtaining tissue specimens for molecular analysis is a key point in current precision medicine. However, the patients’ conditions may be too poor to be suitable for re-biopsy, especially when they experience disease progression after EGFR TKI treatment. Liquid biopsy to detect T790M mutations from circulating cancer cells or cell-free DNA from the blood may be another choice. 67
In conclusion, this study enrolled the largest number of patients with complex EGFR mutations. Afatinib as the first-line therapy provided a better treatment efficacy and survival benefit in lung adenocarcinoma with complex EGFR mutations, especially with uncommon mutation pattern. Patients with classical mutation pattern had longer PFS and OS than those with uncommon patterns. Moreover, SCLC transformation remained one of the mechanisms for acquired resistance to EGFR TKIs, in addition to T790M mutations. Because of the treatment efficacy and survival benefit, afatinib is an effective first-line treatment for patients with complex EGFR mutations, especially those with uncommon mutation patterns.
Supplemental Material
supl_table_and_figure_20200426TAMOdocx – Supplemental material for The effectiveness of afatinib in patients with lung adenocarcinoma harboring complex epidermal growth factor receptor mutation
Supplemental material, supl_table_and_figure_20200426TAMOdocx for The effectiveness of afatinib in patients with lung adenocarcinoma harboring complex epidermal growth factor receptor mutation by Shang-Gin Wu, Chong-Jen Yu, James Chih-Hsin Yang and Jin-Yuan Shih in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
The authors would like to thank the second and the third Core Lab, Department of Medical Research, National Taiwan University Hospital for providing laboratory facilities. In addition, the authors also would like to thank Joel W. Neal for his comments on the oral presentation in the 2019 World Conference of Lung Cancer (WCLC), Barcelona, Spain.
Author contribution
SG Wu and JY Shih had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study design and patient specimen collection: SG Wu, JY Shih, CJ Yu and James CH Yang. Data collection, literature search, and drafting of the manuscript: SG Wu and JY Shih. Study supervision: CJ Yu, James CH Yang and JY Shih. All authors approved the final draft of the submitted manuscript.
Conflict of interest statement
SG Wu has received speaking honoraria from Roche, AstraZeneca and Pfizer. JY Shih has received personal fees for advisory boards from AstraZeneca, Roche, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Ono Pharmaceutical, Chugai Pharmaceutical, and Bristol-Myers Squibb; speaking honoraria from AstraZeneca, Roche, Boehringer Ingelheim, Eli Lilly, Pfizer, Novartis, Merck Sharp & Dohme, Ono Pharmaceutical, Chugai Pharmaceutical, and Bristol-Myers Squibb; and travel expenses from Roche, Pfizer, Merck Sharp & Dohme, Chugai Pharmaceutical, and Bristol-Myers Squibb. CJ Yu declares no conflict of interest. JCH Yang has received advisory board and speaker honoraria from Boehringer Ingelheim, AstraZeneca, Roche/Genentech, Pfizer, Novartis, MSD, Merck Serono, Clovis Oncology, and Bayer.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board of the National Taiwan University Hospital Research Ethics Committee (REC No. 201103013RC and 201111039RIC). All patients provided written informed consent for the collection of demographic and clinical outcome data and for molecular analysis before the collection of tissue specimens.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Ministry of Science and Technology, R.O.C. (MOST 106-2314-B-002-099-MY3), National Health Research Institutes (NHRI-EX105-10421BI), National Taiwan University Hospital, Taipei, Taiwan (106-003689 and 107-N4002, 107-CGN-16, 108-CGN-10) and New Century Health Care Promotion Foundation, Taiwan (2018).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.