
Abstract
Objective
To evaluate survival following afatinib (AF) and erlotinib (ER) treatment in advanced del19 lung adenocarcinoma (AD19LA) with asymptomatic brain metastasis (ABM) after pemetrexed–cisplatin chemotherapy (PCC).
Methods
Data were retrospectively analysed from individuals with AD19LA and ABM after PCC who received AF or ER for 2 years or until intolerable adverse events (AEs), withdrawal, or death. The primary outcome was survival; secondary outcomes were AEs.
Results
The final analysis included 174 AD19LA individuals (AF: n = 86; ER: n = 88) with a median follow-up of 24.2 months (IQR 2.1–28.3). Significant differences in overall survival (16.2 months [95%CI 15.4–17.1] for AF vs 7.2 months [95%CI 6.3–8.1] for ER) (HR 0.50, 95%CI 0.36–0.71, p<0.0001) and median progression-free survival (9.4 months [95%CI 8.5–9.7] for AF vs 5.6 months [4.7–6.2] for ER) (HR 0.66, 95%CI 0.47–0.94, p=0.02) were observed between the groups. Rates of all-grade AEs were 82.5% for AF and 72.7% for ER, and rates of grade ≥3 AEs were 37.2% for AF and 34.0% for ER.
Conclusion
Compared with ER, AF treatment may be more beneficial in terms of survival in the management of AD19LA after PCC with a tolerable safety profile.
Keywords
Introduction
Afatinib (AF) and erlotinib (ER) are frequently used in the treatment of advanced del19 lung adenocarcinoma (AD19LA) following pemetrexed-cisplatin chemotherapy (PCC). 1 Previous reports have demonstrated that AF and ER are associated with improved survival in individuals with asymptomatic brain metastasis (ABM) instigated by AD19LA.1,2 Despite the reported efficacy of both AF and ER, about it remains unclear which drug is more effective in AD19LA patients.3,4 Previous studies have been limited by factors including the number of subjects, length of follow-up, and duration of treatment, meaning that discussions on which treatment modality is superior have focused on survival advantages.5–7 Furthermore, inconsistent inclusion and exclusion criteria and variations in mutant subtypes and endpoint definitions have not been sufficiently clarified in some previous studies,2,8 leading to ambiguity in study conclusions. Comparisons between AF and ER have been of significant interest.8–9 Although prospective comparative studies of these agents have been reported, sample size limitations and heterogeneity among study participants mean that further research is needed to draw definitive conclusions with respect to survival benefit.5,10,11
To the best of our knowledge, this study is the first to compare survival associated with AF and ER treatment in Chinese patients with AD19LA following PCC.
Methods
Study population and endpoints
The collection of patient data was approved by the Institutional Review Board of the Affiliated Hospital of Hebei University, and an exemption for informed consent was obtained from the board given the retrospective study design. Data were collected from AD19LA individuals with ABM following PCC from January 2015 to December 2018. Inclusion criteria were laboratory and clinically diagnosed AD19LA; ABM triggered by AD19LA in patients receiving 6-cycle intravenous pemetrexed (500 mg/m2) plus cisplatin (75 mg/m2) once every 3 weeks, followed by oral AF 40 to 50 mg/d or ER 150 mg/d ER until intolerable adverse events (AEs), withdrawal, or death; and Eastern Cooperative Oncology Group (ECOG) status of 0 to 2. 10 Major exclusion criteria were a definite history of lung or brain surgery or radiotherapy; discontinuation or interrupted use of AF or ER for reasons other than an AE; uncontrolled conditions such as diabetes mellitus or hypertension; tumour invasion of major blood vessels; tumour-induced perforation; and New York Heart Association classification of 3. The primary outcome was survival, and secondary outcomes were AEs.
Definitions of descriptive variables
Overall survival (OS) was calculated from initiation of AF or ER treatment to death and progression-free survival (PFS) was calculated from initiation of AF or ER treatment to the occurrence of disease progression. ABM was confirmed after PCC. The assessment of drug response or disease progression was according to the Response Evaluation Criteria in Solid Tumours (RECIST v1.1). 5 The Common Toxicity Criteria scale v4.0 12 was used to evaluate AEs.
Statistical analysis
Categorical and continuous data were compared using a Chi-square test, Fisher’s exact test, Mann–Whitney U test, or Student’s t-test as appropriate. Survival analysis was performed using the Kaplan–Meier method. Survival differences were analysed using a Cox proportional hazard regression model. All statistical analyses were performed using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). A two-sided p value < 0.05 was regarded as significant.
Results
In total, 213 AD19LA individuals with ABM following previous PCC between January 2018 and January 2020 were evaluated. Of these, 39 (33.9%) cases were excluded based on the exclusion criteria, leaving 174 cases for final evaluation (AF: n=86; ER: n = 88). The mean age of patients was 64.5 (±12.78) years in the AF group and 64.4 (±13.81) years in the ER group, and there was a female predominance in both groups. No notable differences in patient characteristics were observed between the groups, as shown in Table 1. The median follow-up for all patients was 24.2 months (IQR 2.1–28.3).
Baseline characteristics between groups.

AF: afatinib; ER: erlotinib; LA: lung adenocarcinoma; BM: brain metastases; ECOG: Eastern Cooperative Oncology Group.
Survival analysis
A significant difference in median OS was observed between the groups (16.2 months [95%CI 15.4–17.1] for AF vs 7.2 months [95%CI 6.3–8.1] for ER) (hazard ratio [HR] 0.50, 95%CI 0.36–0.71, p < 0.0001), as shown in Figure 1. A significant difference was also observed in median PFS (9.4 months [95%CI 8.5–9.7] for AF vs 5.6 months [4.7–6.2] for ER) (HR 0.66, 95%CI 0.47–0.94, p = 0.02), as shown in Figure 2. HRs were calculated using the Cox proportional hazards model, with adjustment for age, gender, smoking status, and number of brain metastases as covariates and AF/ER therapy as a time-dependent factor.

Median OS (16.2 months [95%CI 15.4–17.1] for AF vs 7.2 months [95%CI 6.3–8.1] for ER) (HR 0.50, 95%CI 0.36–0.71, p < 0.0001). *HR was calculated using the Cox proportional hazards model, with adjustment of age, gender, smoking, and BM number as covariates and AF/ER therapy as a time-dependent factor. AF: afatinib; ER: erlotinib; BM: brain metastases; OS: overall survival; HR: hazard ratio.
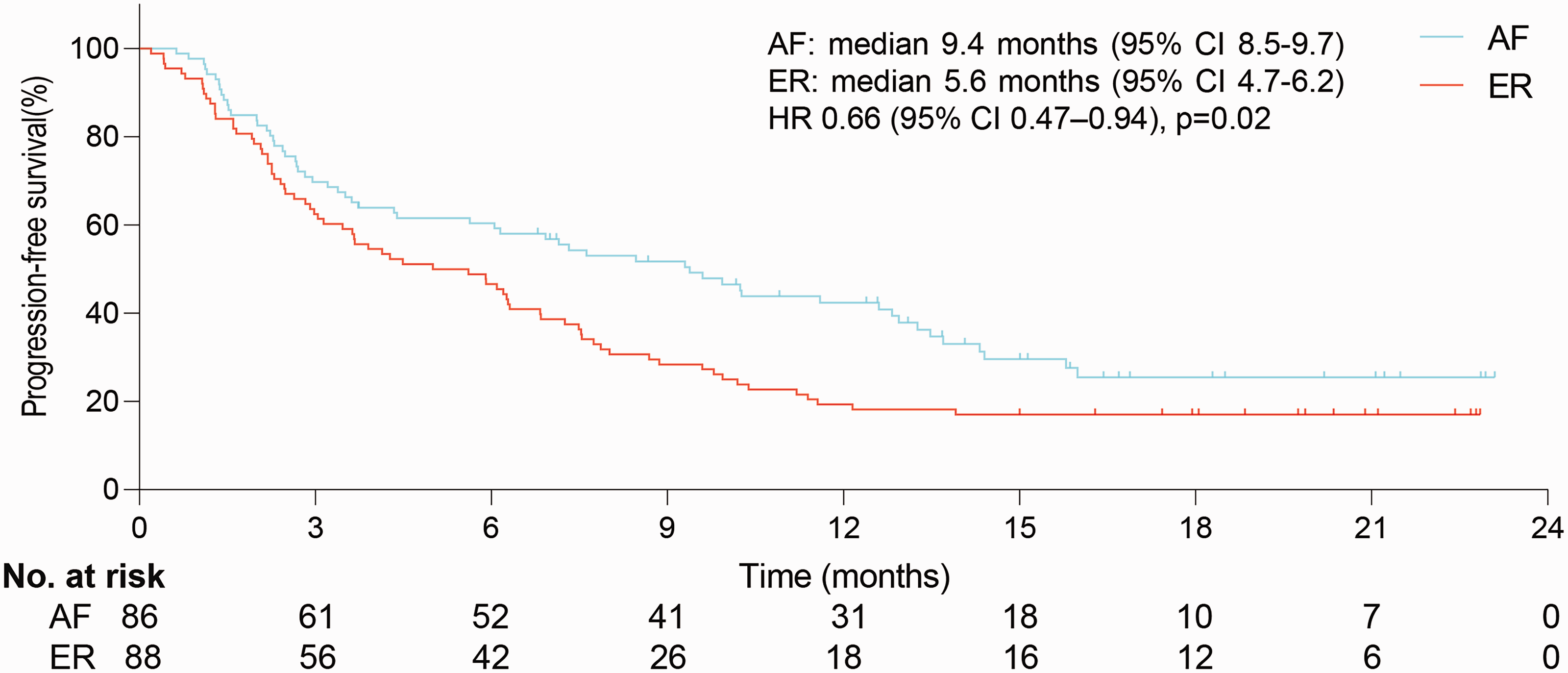
Median PFS (9.4 months [95%CI 8.5–9.7] for AF vs 5.6 months [95%CI 4.7–6.2] for ER) (HR 0.66, 95%CI 0.47–0.94, p=0.02). *HR was calculated using the Cox proportional hazards model, with adjustment of age, gender, smoking, and BM number as covariates and AF/ER therapy as a time-dependent factor. AF: afatinib; ER: erlotinib; BM: brain metastases; PFS: progression-free survival; HR: hazard ratio.
Adverse events
A safety evaluation was performed in the data from all individuals as shown in Table 2. The rate of all-grade AEs was 82.5% for AF and 72.7% for ER, while the rate of grade ≥3 AEs was 37.2% for AF and 34.0% for ER. All-grade AEs were diarrhoea (54.6% for AF vs 41.0% for ER, p = 0.07) and rash (18.6% for AF vs 20.4% for ER, p = 0.96). Grade ≥3 AEs were diarrhoea (26.7% for AF vs 23.8% for ER, p = 0.66) and rash (9.3% for AF vs 9.0% for ER, p = 0.97). The majority of reported AEs were classified as mild to moderate in severity and were reversible.
Main drug-related adverse events.
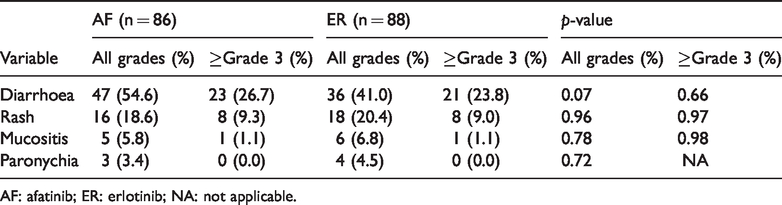
AF: afatinib; ER: erlotinib; NA: not applicable.
Discussion
Findings from the present study show that AF conferred a survival benefit compared with ER in the management of AD19LA with ABM in individuals following prior PCC. Consistent with some previous studies,2,10 our findings indicate an analogous survival advantage for AF.
Our results indicate that AF is clearly associated with longer PFS compared with ER, even after adjusting for potential variables. However, despite the prolongation of PFS in the AF subgroup, the prolongation of PFS by AF in the overall population was unattainable because there were more cases with worse prognosis in the AF group. A combined analysis of the LUX-Lung 3 and LUX-Lung 6 trials13,14 demonstrated that AF was effective in the treatment of ABM with a common EGFR mutation. Consistent with the present findings, AF confers a survival advantage in treating AD19LA with ABM in individuals following PCC. Greater effectiveness and wider irreversible ErbB blockade are typically attributed to improved survival outcomes associated with AF compared with ER treatment.9,15 In a retrospective study 2 of 1632 patients with stage IIIb to IV lung adenocarcinoma indicated that AF may be a preferred EGFR-TKI for advanced-stage disease harbouring non-classical mutations. The results of a previous phase II trial (LUX-Lung 4) 16 indicated that AF had modest but remarkable efficacy in non-small cell lung cancer (NSCLC) following third- or fourth-line management with median PFS of 4.4 months (95%CI, 2.8–4.6) and median OS of 19.0 months (95%CI, 14.9–N/A) in individuals who progressed while receiving ER and/or gefitinib.
AF, a novel aniline-quinazoline derivative with high selectivity, belongs to the second generation of EGFR-TKIs, which can irreversibly block the ErbB family, inhibit the formation of dimers on the receptor, strengthen the blocking of downstream signals, deter the proliferation and metastasis of tumours, and weakened drug resistance.13,15 In the first-line treatment of AD19LA (LUX-Lung 3 and LUX-Lung 6), AF significantly prolonged PFS and time to treatment failure (TTF) compared with ER, but OS was not significantly extended. Of note, however, AF was associated with significantly longer OS compared with chemotherapy in these studies. 14 Additionally, in the second-line treatment of AD19LA, AF significantly prolonged PFS and OS.13,17
ER, a reversible EGFR-TKI, is used as second-line treatment for AD19LA and triggers the blockage of signal transduction to impede tumour growth.8,18 Pre-clinical and clinical studies have shown that ER has an inhibitory effect on epidermal growth factor tyrosine kinase and anti-tumour activity against a variety of tumour types2,13 and does not increase toxicity when used in combination with or on the basis of chemotherapy drugs.7,8,17 ER was approved by the FDA in 2004 for the treatment of locally advanced or metastatic NSCLC in patients refractive to first-line chemotherapy.6,16 At present, there is no direct evidence that the expression of EGFR is related to the efficacy of ER.13,15 Given the lack of consensus on the role of EGFR mutation screening in patient management and limitations of study design and other factors, 12 we did not generate sufficient evidence in the present study to draw reliable conclusions on the relationship between EGFR and ER. In addition, Tommaso et al. 19 has proposed that the chemotherapy regimen administered after diagnosis may change the expression level of EGFR, meaning that the pathological specimens used for diagnosis in the present analysis might not accurately reflect the expression level of EGFR in patients treated with targeted agents.
This study had several limitations. First, the level of evidence may have been influenced by the study design. Our inclusion and exclusion criteria may have introduced bias (survivor bias, bias in the data records, or information bias). Some patients showed disease progression after drug treatment, but diagnostic criteria for such progression are lacking, which may have affected the results and subsequent conclusions to a magnitude which cannot be determined. Despite these shortcomings, the well-defined disease pathway and fixed treatment schedule, coupled with the relatively robust study design, mean that these factors might not have played a decisive role in the study outcome. However, future prospective randomized controlled studies are needed to clarify the efficacy of AF versus ER. Second, our follow-up analysis may have been influenced by the frequency and length of follow-up and the quality of recorded data. Finally, there exist unified standards 14 for when to initiate treatment with AF and ER, but these standards might not have been adhered to in all cases.
In conclusion, our results showed that patients with AD19LA and ABM after PCC had significant survival advantages after treatment with AF compared with ER. Although our aim was to compare survival between these two drugs, it may be necessary to further evaluate the duration of treatment in future studies. Whether long-term targeted therapy instigates or amplifies AEs is currently inconclusive6,15 and could not be sufficiently clarified in the present review. A prospective trial to examine the peak duration of AEs is therefore required. Our further analyses after long-term follow-up may determine whether our findings are consistent with the results of previous prospective studies.