
Abstract
Objective
This study aimed to identify a predictive marker of response to epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) in patients with EGFR-mutant advanced lung adenocarcinoma.
Methods
A cohort of 190 patients with EGFR-mutant advanced lung adenocarcinoma was analyzed. Receiver operating characteristic curve analysis was used to evaluate the optimal cutoffs for fibrinogen levels, the neutrophil-to-lymphocyte ratio (NLR), and the platelet-to-lymphocyte ratio (PLR) for predicting progression-free survival (PFS). Univariate and multivariate survival analyses were performed to identify factors correlated with PFS and overall survival (OS).
Results
High NLR was associated with worse performance status. In univariate analysis, fibrinogen levels, NLR, and PLR were correlated with OS and PFS. In multivariate analysis, all three variables remained predictive of OS, whereas only fibrinogen levels and PLR were independent prognostic factors for PFS. Furthermore, the combination of fibrinogen levels and PLR (F-PLR score) could stratify patients into three groups with significantly different prognoses, and the score was independently predictive of survival.
Conclusion
The F-PLR score predicted the prognosis of patients with EGFR-mutant advanced lung adenocarcinoma who received EGFR-TKIs, and this score may serve as a convenient blood-based marker for identifying high-risk patients.
Keywords
Introduction
Lung cancer is the leading cause of death globally, and non-small cell lung cancer (NSCLC) is the most common form of lung cancer. 1 Approximately 70% of patients are diagnosed with advanced or locally advanced disease, and their prognosis is poor. For patients harboring epidermal growth factor receptor (EGFR) mutations, EGFR tyrosine kinase inhibitors (TKIs) have proven superior to chemotherapy in patients with relapsed or advanced lung cancer in clinical trials.2–6 For first-generation EGFR-TKIs (including gefitinib, erlotinib, and icotinib), the median progression-free survival (PFS) was approximately 8 to 10 months, and nearly all patients inevitably experience drug resistance and treatment failure. However, the response to treatment varies significantly among individuals, and a useful marker for predicting prognosis is lacking.
Local and systemic inflammation is a hallmark of cancer. 7 Recently accumulated evidence indicates that inflammation is an important factor affecting patients’ responses to treatment and prognosis. A series of blood-based markers, including the neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR), have been reported to be effective for predicting patients’ survival in various cancers,8–10 including NSCLC. 11 Blood coagulation disorder is a common complication of malignant tumors, and recent studies demonstrated that coagulation system activation is associated with progression and metastasis in various cancers.12,13 Therefore, fibrinogen, an importation protein mediating coagulation pathways, is considered a prognostic factor for patients with cancer. Several studies evaluated the prognostic role of fibrinogen in various cancers.14–16 In NSCLC, Zhong et al. 17 reported in a meta-analysis that the plasma fibrinogen level is an independent predictor for overall survival (OS). Recently, an increasing number of studies have evaluated the prognostic role of the combination of fibrinogen levels and other blood-based markers, such as NLR and PLR, in patients with NSCLC 18 and breast cancer. 19 However, the prognostic significance of combinations of these variables in patients with advanced NSCLC has yet to be evaluated.
In the present study, we retrospectively analyzed a cohort of 194 patients with advanced EGFR-mutant lung adenocarcinoma to evaluate the prognostic role of NLR, PLR, fibrinogen, and their combination following EGFR-TKI treatment.
Patients and methods
Patient selection
Patients who were pathologically diagnosed with lung adenocarcinoma at Second Xiangya Hospital (Changsha, China) between January 2016 and December 2018 were consecutively and retrospectively recruited. All patients underwent genetic testing via next-generation sequencing or the amplification-refractory mutation system, and the presence of mutant EGFR was confirmed. All patients in the present cohort consented to treatment with a first-generation EGFR-TKI (gefitinib, erlotinib, or icotinib) as the first-line treatment, and a blood test was performed within 1 week prior to treatment. Patients with histories of other malignant tumors, chronic inflammatory diseases, recent steroid therapy, acute infection, or inflammation were excluded. All patient personal information was de-identified. Approval was obtained from the Ethical Committee and institutional review board of Second Xiangya Hospital, Central South University (Changsha, Hunan, China) on May 5, 2020. The requirement for informed consent was waived by the consent was waivered by the Ethical Committee of the institution because of the retrospective nature of the research.
Data collection and follow-up
The patients’ clinicopathological characteristics (including age, sex, smoking history, brain metastasis status, Eastern Cooperative Oncology Group performance status [ECOG PS], EGFR mutation status, blood routine test data, and coagulation function test results) were obtained from the electronic medical record system of Second Xiangya Hospital. NLR was calculated as follows: NLR = neutrophil count/lymphocyte count. PLR was calculated as follows: PLR = platelet count/lymphocyte count. ECOG PS was used to evaluate the patients’ physical status (on a scale of 0–5, with higher scores indicating a worse general condition). PFS was calculated from the date of diagnosis to that of disease progression (based on Response Evaluation Criteria in Solid Tumors 1.1) or death. OS was calculated from the date of diagnosis to that of death of any cause or the last follow-up date (April 1, 2020). The reporting of this study conforms to the STROBE statement. 20
F‑PLR score
The F-PLR score was created by combining fibrinogen levels and PLR. For both fibrinogen levels and PLR, patients were given a score of 1 if the value exceeded the cutoff, whereas a score of 0 was given for lower values. Thus, the total F-PLR ranged 0 to 2.
Statistical analysis
All statistical analyses were performed using SPSS 22.0 (IBM, Armonk, NY, USA). Receiver operating characteristic (ROC) curves were used to calculate the optimal cutoffs for fibrinogen levels, NLR, and PLR. Survival analysis was performed using the Kaplan–Meier method. The chi-squared and log-rank tests were used to compare the baseline clinical characteristics and survival curves, respectively. The predictive factors for survival were evaluated via univariate and multivariate analyses using the Cox hazards regression method. All tests were two-sided, and P < 0.05 indicated statistical significance.
Results
Patient characteristics
In total, 190 patients with advanced EGFR-mutant lung adenocarcinoma were enrolled in the present study. The clinicopathological characteristics of the cohort are presented in Table 1. The mean age of all patients was 60 years (range, 28–79 years), and 104 (54.7%) patients were female. Most patients (133, 70.0%) were non-smokers. In total, 155 (80.4%) patients had an ECOG PS of 0 or 1. Twenty-four patients had brain metastasis, and five patients received whole-brain radiation therapy concurrent with TKI therapy. Among all patients, 80 (42.1%) patients carried the L858R mutation in exon 21, 103 (54.2%) displayed exon 19 deletion, and 7 (3.7%) had other rare mutations. According to the ROC curve, the area under the ROC curves for fibrinogen levels, NLR and PLR were 0.644, 0.517, and 0.522, respectively. The optimal cutoffs for fibrinogen levels, NLR, and PLR were 3.75 g/L, 3.28, and 273.84, respectively. Hence, 73 (38.4%) patients were assigned to the high fibrinogen group, 92 (48.4%) patients were assigned to the high NLR group, and 33 (17.4%) patients were assigned to the high PLR group.
Baseline characteristics of the patients.

ECOG PS, Eastern Cooperative Oncology group performance status; EGFR, epidermal growth factor receptor; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Relationships of fibrinogen levels, NLR, and PLR with clinicopathological characteristics
The relationships of fibrinogen levels, NLR, and PLR with patients’ clinical characteristics are presented in Table 2. Patients with high NLR had worse ECOG PS (P = 0.003). Fibrinogen levels, NLR, and PLR did not display significant correlations with age, smoking status, brain metastasis, and the EGFR mutation status based on the aforementioned cutoffs.
Clinicopathological characteristics of the patients according to fibrinogen levels, NLR, and PLR.

ECOG PS, Eastern Cooperative Oncology group performance status; EGFR, epidermal growth factor receptor; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio.
Univariate and multivariate Cox regression analyses of PFS and OS
In univariate analysis, ECOG PS, fibrinogen levels, NLR, and PLR were significantly associated with PFS (P = 0.013, P < 0.001, P = 0.013, and P < 0.001, respectively, Figure 1a–c) and OS (P < 0.001, P = 0.025, P = 0.005, and P = 0.001, respectively, Figure 1d–f), whereas other clinical characteristics, including age, gender, smoking status, brain metastasis, and mutation type, were not significantly associated with patient survival in the present analysis (Table 3).
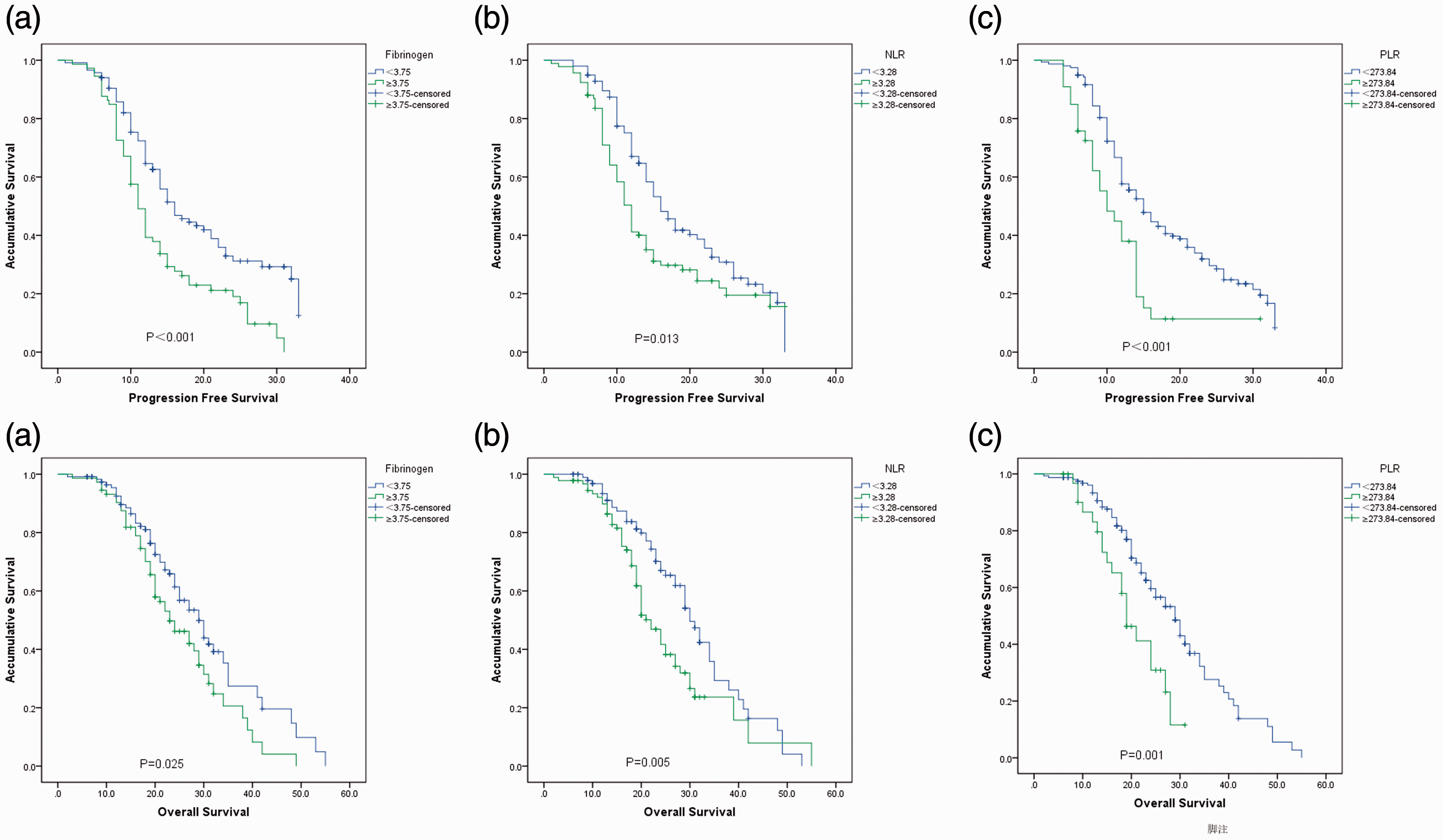
Kaplan–Meier survival curves for progression-free survival according to fibrinogen levels (a), NLR (b), and PLR (c) and for overall survival according to fibrinogen levels (d), NLR (e), and PLR (f) in patients with epidermal growth factor receptor-mutant lung adenocarcinoma treated with first-generation epidermal growth factor receptor tyrosine kinase inhibitors. NLR, neutrophil-to-lymphocyte ratio, PLR, platelet-to-lymphocyte ratio.
Univariate analysis of potential factors associated with PFS and OS.

PFS, progression-free survival; OS, overall survival, ECOG PS, Eastern Cooperative Oncology group performance status; EGFR, epidermal growth factor receptor; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; MST, median survival time.
In the multivariate Cox regression analysis, PLR (hazard ratio [HR] = 1.843; 95% confidence interval [CI] = 1.149–2.957; P = 0.011) and fibrinogen levels (HR = 1.890; 95% CI = 1.323–2.699; P < 0.001) were independent prognostic factors for PFS. Meanwhile, PLR (HR = 1.729; 95% CI = 1.018–2.936; P = 0.0043), NLR (HR = 1.552; 95% CI = 1.012–2.381; P = 0.0044), and fibrinogen levels (HR = 1.565; 95% CI = 1.047–2.340; P = 0.029) were identified as independent predictors of OS (Table 4).
Multivariable Cox regression analyses of PFS and OS

PFS, progression-free survival; OS, overall survival, NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; HR, hazard ratio; CI, confidence interval.
Prognostic value of the F‑PLR score
In total, 100 (52.6%) patients had an F‑PLR score of 0, 75 (39.5%) patients had an F‑PLR score of 1, and 15 (7.9%) patients had an F‑PLR score of 2. The median PFS times for patients with F‑PLR scores of 0, 1, and 2 were 18.3, 12.2, and 7.8 months, respectively (P < 0.001; Figure 2a), and the median OS times for these patients were 30.1, 23.4, and 18.8 months, respectively (P = 0.021; Figure 2b).

Kaplan–Meier curves of progression-free survival (a) and overall survival (b) according to the F-PLR score (0 = low fibrinogen and low PLR, 1 = low fibrinogen and high PLR or high fibrinogen and low PLR, 2 = high fibrinogen and high PLR). PLR, platelet-to-lymphocyte ratio.
Discussion
In the present study, we retrospectively analyzed a cohort of patients with EGFR-mutant lung adenocarcinoma who received EGFR-TKIs to evaluate the prognostic value of the blood-based biomarkers fibrinogen, NLR, and PLR. We found that PLR, NLR, and plasma fibrinogen levels were correlated with PFS and OS. Multivariate analysis demonstrated that high PLR and high plasma fibrinogen levels were independent prognostic factors for worse PFS, and high NLR, PLR, and fibrinogen levels were independent prognostic factors for worse OS. Moreover, the combination of fibrinogen levels and PLR could better predict the survival of patients, thus revealing a novel marker for patient stratification.
Lung adenocarcinoma can be divided into two groups according to the gene mutation status. For patients without known driver gene mutations (e.g., EGFR, ALK, ROS-1), chemotherapy and/or radiation therapy is the major treatment modality. For patients with driver gene mutations, targeted therapy is the major treatment modality. Although several trials demonstrated that EGFR-TKIs improve PFS in patients with advanced NSCLC harboring EGFR mutations, drug resistance is nearly inevitable, representing a major challenge for clinicians. Thus, biomarkers to predict drug effectiveness and facilitate patient stratification and treatment adjustment are urgently needed. Biomarkers predictive of EGFR-TKI effectiveness are lacking. It has been reported that PD-L1 expression and the immune microenvironment are associated with EGFR-TKI effectiveness, 21 indicating that the inflammatory status is associated with drug response. Inflammatory responses represent a common complication of malignant tumors because cytokines released by tumor cells can induce systemic inflammation. 22 Systemic inflammation affects the counts of inflammation-related cells, including neutrophils, lymphocytes, and platelets. Thus, blood-based biomarkers that can be used to characterize the inflammatory status have proven effective for predicting patient prognosis for various cancers. NLR and PLR are the most widely studied biomarkers, and they have proven prognostic significance in various cancers.8,23,24 Regarding NSCLC, studies reported that NLR and PLR could predict patient survival in both early and advanced stages.25–28 In the present study, we identified PLR and NLR as independent prognostic factors for PFS, in line with previous reports. These results further indicated that systemic inflammation is involved in the development of EGFR-TKI resistance; however, the underlying mechanism requires further investigation. Targeting systemic inflammation might represent a promising strategy to delay drug resistance. Concerning OS, NLR and PLR were also predictive factors. This may attributable to the impact of follow-up treatment. Generally, the follow-up treatment after EGFR-TKI resistance includes targeted therapy and chemotherapy, which have different mechanisms of resistance, thereby limiting the ability of a single biomarker to predict OS.
Fibrinogen is a protein synthesized by the liver that mediates blood coagulation, and it is an acute reactive protein involved in the inflammatory process. Recent evidence indicated the involvement of fibrinogen in a series of cancer-related processes, including cell proliferation, angiogenesis, and epithelial–mesenchymal transformation, which are correlated with cancer progression and drug resistance. 29 Clinical studies have evaluated the prognostic role of fibrinogen in various cancers.9,14,30 Regarding lung cancer, Zhong et al. 17 conducted a meta-analysis of 16 studies involving 6881 patients, finding that a plasma fibrinogen concentration of ≥4 g/L portended worse OS. In the present study, we also found that a higher fibrinogen level is an independent prognostic factor for PFS and OS, as reported previously.
Because multiple blood-based prognostic biomarkers have been discovered in various cancers, the combination of biomarkers to increase prognostic significance and improve patient stratification is increasingly emphasized. Several studies evaluated the combination of fibrinogen levels with other inflammatory markers, including NLR, PLR, and the lymphocyte-to-monocyte ratio, in gastric cancer, 31 colorectal adenocarcinoma, 32 and esophageal carcinoma. 33 The findings highlighted the promise of such combinations for predicting patient survival. Liang et al. 18 retrospectively analyzed a cohort of patients with NSCLC and found that the combination of fibrinogen levels and NLR (F‑NLR) has potential as a novel and useful blood marker for predicting postoperative survival. In the present study, we found that fibrinogen levels and PLR were independent prognostic factors for PFS and OS, and the F-PLR score could stratify patients with NSCLC into three distinctive risk groups, thereby improving the prognostic significance over either biomarker alone.
The present study had obvious limitations. First, because of the retrospective nature of the study, patient selection bias and follow-up bias were inevitable. Second, because of the limited sample size, only 15 patients had an F-PLR score of 2. Although significant differences were noted among the groups, the results should be interpreted with caution. Further prospective studies are required to validate the role of fibrinogen and other blood-based biomarkers in predicting prognosis in patients with EGFR-mutant NSCLC receiving first-line EGFR-TKI treatment.
In summary, our research demonstrated that plasma fibrinogen levels, NLR, and PLR are promising and easily measured biomarkers that could be used to predict the prognosis of patients with advanced lung adenocarcinoma who received EGFR-TKIs. In addition, the combination of fibrinogen levels and PLR may represent a promising biomarker with higher predictive potential that is worthy of further investigation.