
Abstract
Immunotherapy may result in long-lasting exceptional clinical responses, the molecular background of which is inadequately understood. Here, we present the case of a 63-year-old patient with a past medical history of renal cancer who relapsed many years later. Several treatment lines were administered prior to immunotherapy, which was administered in the ninth line, achieving complete remission which had lasted for more than 3 years. Genomic alterations, tumor mutational burden (TMB), and microsatellite instability as well as PD-L1, MLH1, MSH2, MSH6, PMS2, CD3, CD8, CD20, CD138, CD1a, and FoxP3 expression were assessed in primary and metastatic tumors. Primary and metastatic tumors were microsatellite stable with high TMB, while somatic mutations in MLH1 and TP53 genes were detected, respectively. Although the primary tumor was negative for PD-L1 expression, the lung metastasis was positive. Interestingly, metastasis displayed a dramatically increased infiltration by CD1a-positive dendritic cells in addition to increased CD3+ and CD8+ cytotoxic T cells. Increased infiltration of the metastatic tumor by CD1a+ antigen presenting cells warrants further investigation to assess its potential predictive value.
Introduction
The discovery of immune checkpoint inhibitors (ICIs) has changed the treatment landscape of many solid tumors, improving progression-free survival (PFS) and overall survival (OS) rates. 1 Nivolumab, the first-in-class drug, has been approved for the treatment of many hematological and epithelial malignancies.2,3 It has also been approved for the treatment of advanced renal-cell carcinomas (RCC), based on the results of a randomized phase III trial, which favored nivolumab compared with everolimus. 4
Response to immunotherapy covers a wide spectrum of clinical benefit. On one hand, a small subset of patients treated with immunotherapy presents rapid progression (hyper-progressors) 5 or fatal reactions. 6 On the other hand, there are some exceptional responders with long lasting clinical benefit, the molecular background of whom is poorly understood. 7 Complete responses to monotherapy with ICIs are infrequent events and no validated biomarkers exist to identify patients’ subgroups with a high probability to respond. 8
Here, we report an extraordinary case of a heavily pre-treated patient with metastatic clear-cell RCC (ccRCC) who has experienced a surprising clinical benefit with complete response for more than 3 years after the initial administration of nivolumab. To identify possible predictive biomarkers, we evaluated genomic and tumor immune microenvironment (TIME) alterations.
Case presentation
In 2003, the patient, a 52-year-old Caucasian male, had been diagnosed with RCC and had initially been managed with left nephrectomy. Pathological and clinical staging revealed a grade 2 T1bN0M0 ccRCC and favorable prognostic traits based on Memorial Sloan Kettering Cancer Center (MSKCC) criteria. 9 In April 2014, at the age of 63 years, the patient relapsed with a lung lesion, which was managed surgically with metastasectomy. Histopathological evaluation identified an RCC with particular characteristics similar to those of the primary tumor. Post-surgery staging (May 2014) with positron emission tomography/computed tomography (CT) revealed mediastinal metastatic disease as well as suggestive pleural lesions in the left hemithorax and the patient was started on first-line systemic therapy (time point 0). Subpleural nodules were detected on contrast enhanced CT, despite treatment, 4 months after recurrence (September 2014). Contrast enhanced CT images as well as changes in tumor burden from different follow-up time points are presented in Figures 1 and 2(a) and (b), respectively. At the beginning, the subpleural nodules were discrete and could be measured (measurable disease by RECIST criteria). As the burden of the disease increased, the lesions coalesced, and it was difficult to measure separately. At the time of initiation of immunotherapy there was a homogeneous pleural thickening taking up almost the entire left hemithorax (non-measurable disease by RECIST criteria). During response to treatment, pleural thickening was reduced homogeneously in the left hemithorax and the maximum thickness was measured in order to assess response. Several treatment lines (eight) were administered prior to immunotherapy. The first-line therapy with sunitinib was given for 4 months (from June 2014 to September 2014) and was interrupted due to radiological progression (multiple lesions in the lower lung lobe, increased mediastinal lymph nodes) and skin toxicity. A second-line therapy with everolimus was administered for 3 months (September 2014 to November 2014) and was discontinued due to severe toxicity (stomatitis). We subsequently opted for third-line pazopanib and the patient experienced radiological progression of disease (PD) after a very short period (3 months). Following pazopanib, a re-challenge with everolimus (January 2015) was attempted, but it was discontinued due to re-emergence of grade IV stomatitis. The patient progressed after everolimus and he was treated with axitinib, which was administered from May 2015 to July 2015 with good tolerance but progression of the disease. Subsequently, bevacizumab was administered (May 2015 to July 2015); however, radiological and clinical progression with pleural effusion occurred and the patient was admitted to the University Hospital of Patras with impaired performance status (PS) and dyspnea. Subsequently, pleural effusion drainage was performed. Next, temsirolimus was administered from July 2015 to December 2015, but the patient developed a rapid progression with worsening of his clinical condition (mainly with dyspnea) and a very poor PS. A short period of chest (mediastinum and left hemithorax) radiotherapy (6000 cGy delivered in daily doses of 200 cGy) in order to improve symptomatology was implemented, followed by sorafenib for almost 2 months (April 2016 to May 2016) with the patient experiencing significant PD. In May 2016, the patient was started with the anti-PD-1 agent nivolumab. The treatment was tolerated extremely well and no significant side effects were observed. A rapid clinical benefit was observed early in the course of therapy, with significant improvement of PS. Four months after the initiation of nivolumab, the first follow-up with CT scans confirmed a radiological response. Residual pleural thickening was still present, but it has been stable for several consecutive follow-up examinations and it is therefore considered to represent post-treatment fibrosis (complete response) rather than residual disease. So far, the patient has received 78 cycles of nivolumab and continues in complete radiographic and clinical remission, 48 months after the initiation of immunotherapy (last follow-up April 2020).
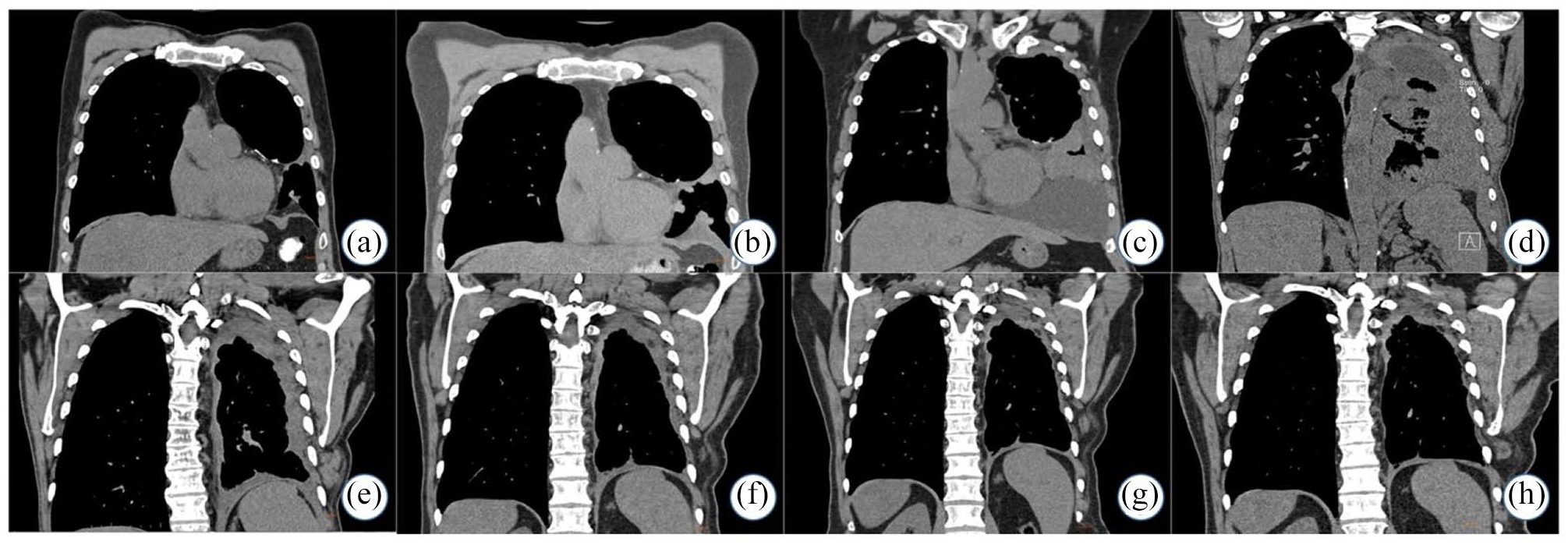
Computed tomography scan assessments of targeted lesions in different time points before immunotherapy. Coronal unenhanced images of the thorax. a–d images at the level of the largest mass, e–f posteriorly at the level where the residual pleural thickening can be best appreciated.(a) Small pleural-based nodules in the left hemithorax, suggestive of recurrent disease after metastasectomy (0 months after recurrence); (b) 3 months after recurrence, increasing size of pleural-based nodules; (c) 7 months after recurrence, the nodules gradually coalesce, causing diffuse pleural thickening, and new loculated pleural effusions; (d) 14 months after recurrence, pleural thickening increases further taking up almost the entire left hemithorax; (e) 4 months after the initiation of nivolumab, pleural thickening has significantly decreased on the first follow-up after immunotherapy; (f) 6 months after the initiation of nivolumab, pleural thickening further decreases on the next two follow-up examinations; (g) 11 months after the initiation of nivolumab, pleural thickening further decreases on the next two follow-up examinations; (h) 31 months after the initiation of nivolumab, stable appearance of mild residual pleural thickening on follow-up examinations, likely representing post-treatment fibrosis.

Changes in tumor burden (a) before and (b) after treatment with nivolumab. The maximum dimension of the largest mass was measured before initiation of nivolumab. At the time of initiation of nivolumab there was homogeneous pleural thickening taking up almost the entire left hemithorax and therefore maximum pleural thickness was measured after initiation of nivolumab. Genomic locations of detected mutations in (c) MLH1 and (d) TP53 genes. Single nucleotide mutation c.1609C>T of MLH1 gene is located in exon 14 leading to stop codon. The missense mutation c.523C>T is located in exon 4 of TP53 gene. MLH1 mutation was detected in the primary renal tumor and TP53 mutation was detected in the metastatic lung lesion.
Materials and methods
Patient consent
A written informed consent was provided from the patient, permitting genomic and TIME profiling of primary and metastatic tumors, as well as publication of relevant clinical and molecular results.
Molecular analysis
Hematoxylin and eosin-stained sections of formalin-fixed and paraffin-embedded (FFPE) tumor biopsies from all samples (primary tumor resected in 2003 and lung metastasis removed in 2014) were reviewed to ensure tumor cell content of >75% and the tumor area was marked by a pathologist. DNA was extracted from the sample under investigation using the Qiagen QIAmp DNA FFPE tissue kit. RNA was extracted using the Qiagen RNeasy FFPE Kit.
Tumor molecular profile analysis was carried out using the Oncomine Comprehensive Assay v3M (Thermo Fisher Scientific) according to the manufacturer’s instructions. This Next Generation Sequencing (NGS) assay analyses 161 unique cancer genes, including 87 oncogenes, 43 copy number amplification genes, 48 tumor suppressor genes, and 51 fusion driver genes. Tumor mutation burden (TMB) analysis was performed using the Oncomine Tumor Mutation Load Assay (Thermo Fisher Scientific), according to the manufacturer’s instructions. The test provides accurate quantitation of somatic mutations to assess tumor mutation load, from limited FFPE samples. The TMB analysis was conducted by annotation of low frequency somatic variants (Single Nucleotide Polymorphisms [SNPs] and Insertions/Deletions [INDELs]) from 409 genes, spanning ~1.2 Mb of exonic sequence. Sequencing was carried out using the Next Generation Sequencing platform Ion Proton (Thermo Fisher Scientific). A TMB score greater or equal to 17 mutations per megabase (Muts/MB) was considered as high, according to the manufacturer’s recommendations.
NGS data analysis was performed with the Ion Reporter™ 5.10 software directly from within Torrent Suite™ 5.0.4 software (Thermo Fisher Scientific). The coverage analysis was performed using the coverage analysis plug-in v5.0.4.0. The statistics generated from this plug-in were used to evaluate the quality of each library in the sequencing run. TMB analysis was conducted with the Ion Reporter™ Software 5.10 analysis workflow that uses a custom variant calling and germline variant filtering algorithm to accurately estimate somatic variants in cancer samples, with no matched normal sample required. TMB measurement is expressed as Muts/MB.
Microsatellite Instability Analysis (MSI) was carried out in parallel on normal and tumor (FFPE) tissue of the patient. MSI analysis was performed using a panel of five microsatellite markers (the Bethesda panel). The markers were amplified using fluorescently labeled primers (Applied Biosystems). The polymerase chain reaction products for each sample were then analyzed by fluorescent fragment analysis on an Applied Biosystems 3130 genetic analyzer.
TIME profiling
Expression of CD3, CD8, FoxP3, CD20, CD138, CD1a, PD-L1, MLH1, MSH2, MSH6, and PMS2 was assessed by immunohistochemistry on FFPE tissue sections in both the primary and metastatic lesions, as previously described. 10 The following primary antibodies were employed: anti-CD3 rabbit polyclonal Ab (DAKO, CA, USA), diluted 1:300; anti-CD8 mouse monoclonal Ab (mAb), clone C8/144B (DAKO, CA, USA), ready to use; anti-Foxp3 mouse mAb, clone 20034 (Abcam, Cambridge, UK), diluted 1:100; anti-CD20 mouse mAb, clone L26 (DAKO, CA, USA), diluted 1:200; anti-CD138 mouse mAb, clone MI15 (DAKO, CA, USA), diluted 1:100; anti-CD1a mouse mAb, clone 010 (DAKO, CA, USA), ready to use; MLH1 mouse mAb, clone ES05 (DAKO, CA, USA), ready to use; MSH2 mouse mAb, clone FE11 (DAKO, CA, USA), ready to use; MSH6 rabbit mAb, clone EP49 (DAKO, CA, USA), ready to use; and PMS2 rabbit mAb, clone EP51 (DAKO, CA, USA), ready to use. DAKO EnVision labeled polymer (DAKO, CA, USA) was used as detection system. PD-L1 expression was assessed by the PD-L1 IHC 22C3 pharmDx (DAKO) on the Autostainer Link 48 platform (DAKO, CA, USA), using the Tumor Proportion Score (TPS), which represents the percentage of viable tumor cells with partial or complete membrane staining at any intensity. Specific conditions for immunohistochemistry can be provided upon request. The immunohistochemically stained slides were evaluated by an experienced pathologist (EK). Representative immunohistochemical images are shown in Figure 3.
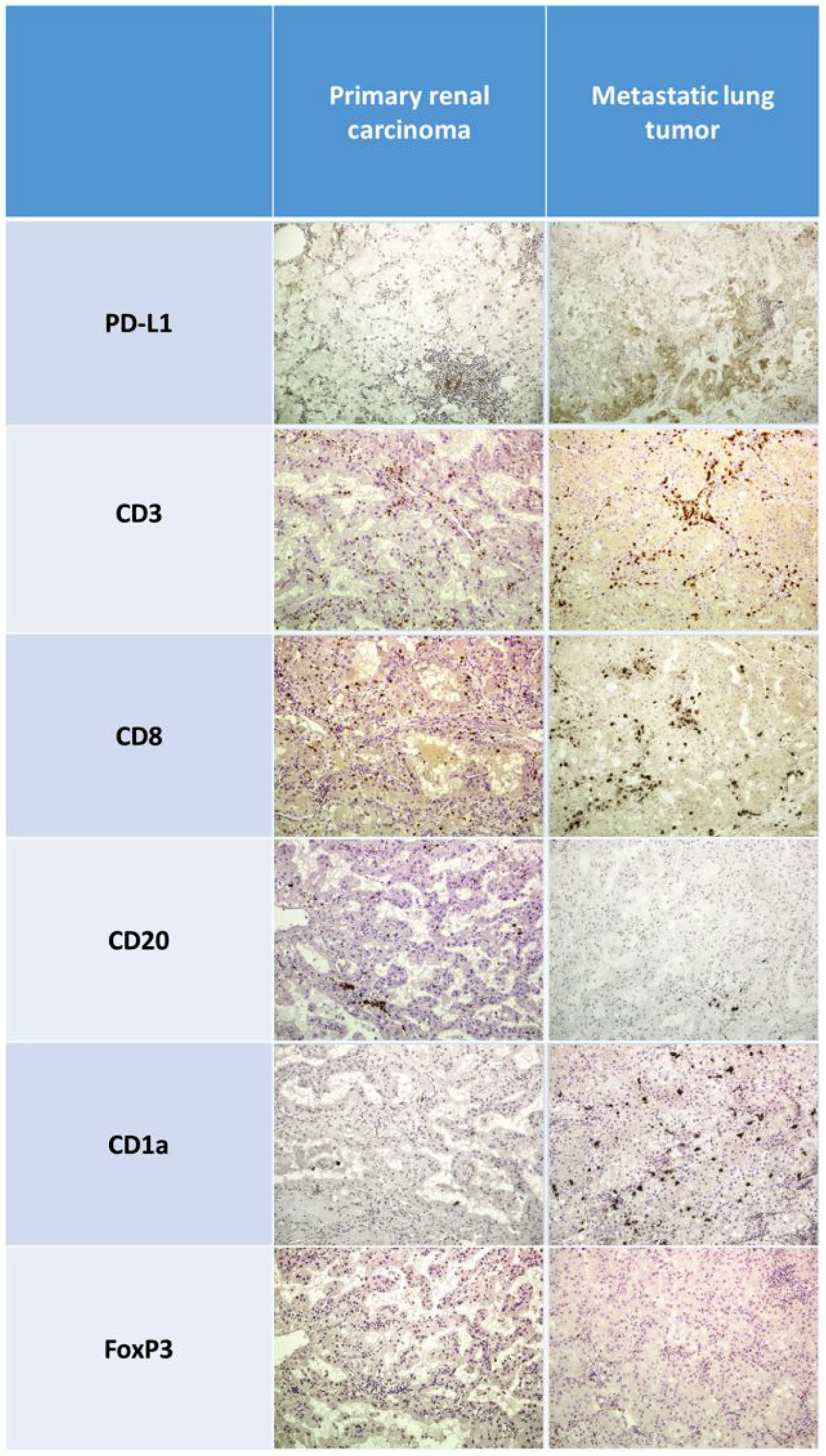
Photomicrographs of FFPE tissue from primary and metastatic lesions stained for PD-L1, CD3, CD8, CD20, CD138, CD1a, and FoxP3 and assessed by immunohistochemistry in primary and metastatic lesions.
Results
Genotyping results
Two somatic mutations were detected in primary renal and lung metastatic tumors by genomic analysis. In the primary tumor, the pathogenic mutation c.1609C>T (p. Gln537Ter) of MLH1 (DNA Mismatch Repair Protein MLH1) gene was identified, while c.523C>T (p.Arg175Cys) in TP53 (Tumor Protein P53) gene was found in the lung metastasis (Figure 2c–d). The first mutation, which has been characterized as pathogenic in the germline setting, has been associated with Lynch Syndrome. 11 It leads to a nonsense genomic change. The c.523C>T (p.Arg175Cys) mutation in TP53 gene provides a missense change. The clinical significance of this mutation is uncertain. Missense substitutions at codon 175 (p.Arg175His, p.Arg175Gly) have been associated with Li-Fraumeni syndrome.12,13 However, the finding by Kato et al. that p.Arg175Cys partially impairs the transcriptional transactivation activity of the TP53 protein in vitro 14 makes unclear whether this mutation is finally pathogenic. 15 Moreover, there are no data regarding its role in response to immunotherapy.
Concurrently, TMB and MSI were assessed in both lesions. Although both the renal primary and lung metastasis were microsatellite stable, TMB was surprisingly high in both tumors. Particularly, the total mutational burden was 267 and 76 mutations/MB in the primary and metastatic lesions, respectively.
Tumor infiltrating immune cells
The neoplastic tissue displayed considerable differences between the primary tumor and the lung metastasis, most notable in the intra-tumoral compartment rather than in the invasive front. The TPS for PD-L1 was <1% for the primary and 1–49% in the metastatic tumor, with peripheral, focal, heterogeneous staining of the tumor border.
The metastatic tumor was infiltrated by higher numbers of CD3+ T cells, CD8+ cytotoxic cells, and FoxP3+ Tregs. The most striking difference was observed in the CD1a+ antigen-presenting cells that were seen mostly infiltrating the epithelial elements and to a lesser extent the intratumoral stroma. The infiltration was accentuated in the most peripheral areas of the metastatic tumor, with a wreath-like distribution of CD1a+ cells. Furthermore, the metastatic tumor showed significantly decreased B-cell infiltration, although plasma cells were not observed in either tumors. With regards to the invasive front, the metastatic tumor displayed a mildly increased infiltration for all cell types, with the most notable difference concerning larger B-cell aggregates, corresponding to tertiary lymphoid structures.
Discussion
This report outlines the molecular background of a patient with metastatic ccRCC who has developed an impressive response following treatment with nivolumab. The new era of immunotherapy in cancer has raised new therapeutic options in previously untreated patients as well as in cases with resistant disease, such as the current patient. There is a more than urgent need for predictive biomarkers in order to achieve better patient selection, elimination of side effects, avoidance of catastrophic rapid progression, and reduction of financial toxicity. To this aim, investigation of exceptional responders could shed light on potential predictive parameters that might merit further investigation in subsequent studies.
The genomic landscape of ccRCC includes genomic alterations in VHL (von Hippel–Lindau tumor suppressor), PBRM1 (Polybromo 1), SETD2 (SET Domain Containing 2), BAP1 (BRCA1 Associated Protein 1), and TCEB1 (Transcription elongation factor B polypeptide 1)16,17 genes. VHL inactivation by either mutation or methylation is the most frequent driver change in ccRCC, being present in about 80% of ccRCC. 17 In the present case, no mutation was identified in the previously mentioned genes. However, the primary renal tumor harbored the pathogenic mutation c.1609C>T of MLH1 gene, which results in a base change leading to a premature stop codon and shortened protein. 11 Despite the presence of c.1609C>T, MLH1 expression was detected by IHC in both primary and metastatic tumors. On the contrary, MLH1 gene was not mutated in the lung recurrence. Although, this alteration has been associated with Lynch syndrome, 11 the fact that this mutation was not detected in the metastatic recurrence as well as in the peripheral blood, augments the hypothesis of somatic mutation in the tumor, which was not included in the clone that gave rise to lung metastasis. Regarding its predictive value, no data exist regarding the predictive value of this mutation in immunotherapy.
Another interesting finding of the analysis was the detection of c.523C>T mutation in TP53, which is of uncertain significance. It has been documented that although TP53 mutations are present in 20% of RCC cases, 18 their frequency is 2.2–2.8% in ccRCC. 17 Moreover, it has been shown that p53 expression is correlated with poor prognosis in RCC patients. 19 On the contrary, limited data exist regarding their predictive significance in immunotherapy. In non-small cell lung cancer (NSCLC), TP53 mutations have been correlated with poor efficacy of immunotherapy. 20 On the other hand, Assoun et al. have reported that patients with advanced TP53-mutated NSCLC treated with immunotherapy, faced longer median OS, PFS, and better objective response rate. 21 In addition, TP53 mutations inhibit tumor immunity in gastric cancer, 22 while a prolonged PFS has been observed in anti-PD-1-treated patients harboring TP53-mut/STK11-EGFR-WT tumors. 23
With respect to TMB, it was extremely high in the primary tumor as well as in the metastatic lesion. Based on the MSI status, this finding cannot be attributed to Mismatch Repair (MMR) deficiency. Partially, the mutation of MLH1 could theoretically contribute to the mutational load of the primary tumor. However, this alteration cannot explain the hypermutated phenotype of the metastatic lesion. High TMB could also be attributed to the mutations of other genes, such as DNA Polymerase Epsilon Catalytic Subunit (POLE), but no mutations were found in this gene in the current NGS analysis. The possibility other genes, not analyzed here, to bear genetic alterations leading to high TMB burden cannot be excluded. In addition, although TMB has been proposed as a predictive factor for immunotherapy, no evidence exists regarding its value in RCC. For instance, elevated TMB further improved the likelihood of benefit from ICIs in advanced NSCLC. 24 On the contrary, Maia et al. failed to show any relationship of TMB to immunotherapy response in metastatic RCC, 25 while Wang et al. have reported no association between TMB and PD-L1 expression in RCC patients. 26
Another intriguing finding was the positive conversion of PD-L1 expression. The primary renal tumor was negative for PD-L1 expression, while the lung metastasis was positive (1–49%). Jilaveanu et al. have reported that expression of PD-L1 is significantly higher in metastases than in primary RCCs. 27 Furthermore, recent studies have shown that PD-1 blockade improved OS and PFS for metastatic melanoma, NSCLC, and RCC. 4 Although, PD-L1 positivity has been used as a predictive biomarker in immunotherapy with PD-1/PD-L1 checkpoint inhibitors, 3 the predictive significance of tumor PD-L1 expression in RCC patients treated with nivolumab was not proved in CheckMate 025. 4
Also of interest were the alterations in the tumor infiltrating immune cells between primary and metastatic tumors. Carcinoma specimens were significantly infiltrated by CD3 and CD8 positive T cells, as well as CD1a-positive dendritic cells, with enrichment from the primary to the metastatic lung tumor. So far, no evidence exists regarding the predictive value of CD3 and CD8 positive T cells in RCC patients treated with nivolumab. From KEYNOTE-001 trial (NSCLC), a significantly higher density of preexisting CD8-positive cells has been associated with immunotherapy response. 28 On the contrary, no predictive value of CD1a-positive infiltrating cells has been proven until now. Nonetheless, the co-existence of increased infiltration of the metastatic tumor by CD3 and CD8 T lymphocytes and increased PD-L1 expression in concert with increased CD1a positive antigen presenting cell infiltration supports the hypothesis of immune activation, laying the groundwork for the greatest benefit by immunotherapy. Notably, the importance of CD1a-positive antigen presenting cells in immune surveillance, and thus possibly in immunotherapy, is shown in a study on cutaneous squamous carcinogenesis. This process involves progression from the premalignant actinic keratosis (AK) to the preinvasive in situ squamous cell carcinoma (isSCC) and finally to the invasive squamous cell carcinoma (inSCC) (Stravodimou A et al. submitted in Archives of Dermatological Research, AODR-D-20-00107). In this study, cancer progression was associated with a decrease of antigen presenting cells in isSCC and inSCC compared with AK, despite the increase of CD3 and CD8 positive lymphocytes in the malignant lesions. Although in the present case the increase of antigen presenting cells in the metastasis concerns a single patient, this observation merits further investigation and evaluation in retrospective and prospective cohorts.
Despite our interesting observations from the analysis of this case, we have to acknowledge some limitations in this study. Although we assessed the molecular and immunological profile of the pulmonary metastasis, we did not include any information regarding the pleural mass due to tissue availability. Analysis of the pleural malignancy may provide a better understanding of tumor heterogeneity and tumor evolution. In addition, it would be ideal if tissue from pleural metastasis, sampled after systematic treatments and prior the initiation of immunotherapy, could have been evaluated, as better correlations would have emerged.
Despite the aforementioned weaknesses, the major advantage of our study is the combined analysis of molecular profile with immunological microenvironment not only in the primary, but also in a metastatic lesion providing possible insights in the ccRCC evolution. In addition, molecular correlates from this case also suggests further evaluation of specific immune cell subpopulations since they have not been studied in this context until now.
Conclusion
This study presents hypothesis-rising observations. Additional data are required to confirm the possible value of infiltrating antigen presenting cells or their combination with CD3 and CD8 lymphocytes, high TMB and PD-L1. Furthermore, the role of somatic pathogenic mutation c.1609C>T of MLH1 gene needs to be clarified.