
Abstract
We report a case of interdigitating dendritic cell sarcoma (IDCS) originating from the adrenal gland. A 57-year-old middle-aged woman with no previous history of malignancy came to our hospital after color Doppler ultrasound revealed a right adrenal mass. An abdominal computed tomography scan also showed an adrenal mass. Postoperative pathology confirmed the diagnosis of IDCS. After complete surgical removal of the adrenal tumor, the patient has been disease-free for 1 year. IDCS may have a good prognosis after surgical resection. To our knowledge, this is only the second reported case of IDCS in the adrenal region.
Keywords
Introduction
Interdigitating dendritic cell sarcoma (IDCS) is an extremely rare malignancy that originates from a dendritic cell (DC) tumor and usually presents as lymphadenopathy with local enlargement, rarely accompanied by systemic symptoms such as fever and weight loss. The most common primary site of IDCS is the lymph nodes, which are mainly located in the cervical, mediastinum, and axillary regions. Extralymphatic IDCS lesions mainly occur in the liver, lungs, spleen, digestive system, head and neck, and testes. 1 In 1981, Feltkamp et al. reported the first case of IDCS occurring in the mediastinal region. 2 Subsequently, IDCS cases from the liver, lungs, spleen, digestive system, head and neck, and testicles have been reported. However, IDCS cases originating from the adrenal region are extremely rare, with only one previously reported case. 3 Herein, we report the second case of IDCS originating from the adrenal gland and review relevant knowledge about the pathological features and clinical treatment of IDCS.
Case report
The reporting of this study conforms to the CARE guidelines. 4 The patient gave verbal informed consent for the publication of this case report. A 57-year-old woman was admitted to our hospital with a 1-month history of right adrenal hyperplasia, which was found by color Doppler ultrasound. The patient had no systemic symptoms such as cough or blood-stained sputum, dizziness, chest tightness, fever, night sweats, weight loss, or fatigue. Contrast-enhanced computed tomography showed a 3.4- × 2.1-cm, solitary, heterogeneous density mass with a clear boundary (Figure 1). Other radiological and ultrasound examinations did not reveal significant nodal disease or distant metastasis. The patient underwent a right adrenalectomy, and the pathological findings of the surgical specimen confirmed the diagnosis of IDCS.

Contrast-enhanced computed tomography image: a solitary, heterogeneous-enhanced density mass with a clear boundary.
Histopathology of the surgically removed specimen showed that the tumor cell nuclei were partially round/oval. The chromatin was lightly stained, mostly vacuolated, and the nucleoli were medium-sized. The cytoplasm was abundant, slightly eosinophilic, and the cells were ill-defined. Mitoses were low (<5/10 high-power field). Small lymphocytes were mixed between tumor cells (Figure 2a). Immunohistochemical analysis showed that the tumor cells consistently expressed s100 and weakly expressed CD68, CD163, and SOX10. The Ki67 proliferation index was 15%. Other examined tumor markers including CD1a, Desmin, EMA, CK, CD21, CD23, CD35, HMB, and SMA, were negative (Figure 2b). The patient has been recurrence-free for 1 year since treatment.
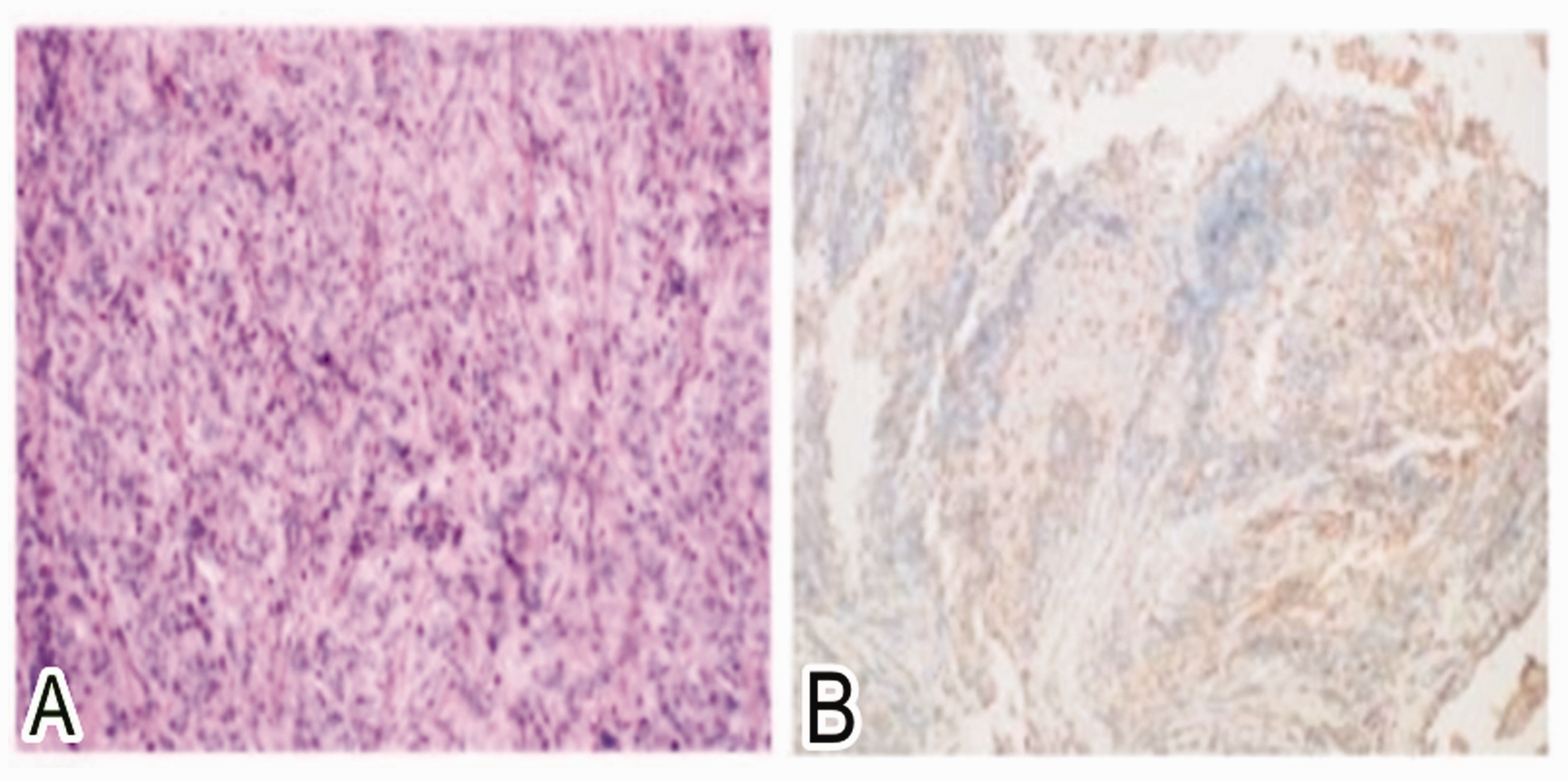
(a) Hematoxylin–eosin staining: tumor cell nuclei were partially round/oval. (b) Immunohistochemical staining: tumor cells consistently expressed s100, and weakly expressed CD68, CD163, and SOX10.
Discussion
DCs are a heterogeneous group of non-lymphoid and non-phagocytic immune helper cells present in lymphoid and non-lymphatic organs. DCs are key antigen presenting cells and initiators of immune responses and include several subtypes such as Langerhans’ cells, interdigitating DCs, follicular DCs, dermal dendrocytes, indeterminate cells, and veiled cells.5–7 DC tumors are very rare, accounting for less than 1% of all lymph node tumors, and IDCs are extremely rare malignancies that originate from DCs. Owing to the overlapping morphology of the various types of DCs, ancillary studies are needed for definitive diagnosis. Other tumor types that need to be excluded are melanoma, spindle cell carcinoma, and various mesenchymal tumors. 8 Approximately 11% of IDCS cases are misdiagnosed as lymphoma, melanoma, peripheral schwannoma, or malignant fibrous histiocytoma. Histomorphology and immunophenotyping can help distinguish IDCS from other spindle cell tumors and metastatic melanomas. 5
IDCS has a distinctive histological pattern, with abundant, slightly eosinophilic cytoplasm, and there is often an indistinct border. The cytoplasm is rich in mitochondria and endoplasmic reticulum, and the nuclei are unevenly shaped and can be serrated, and the nucleolus is obviously larger. Melanin, desmosome junction, and Birbeck granules are not seen. The most commonly described histological pattern of IDCS is the proliferation of spindle-shaped or histiocytic cells, which is similar to other tumor-like conditions including DC tumors, histiocytic lesions, and granulomatous inflammation.1,2,9,10 Currently, there are no specific markers for IDCS, the tumor cells of which often show different immunophenotypes that can be confirmed by multiple immunohistochemical methods. The most commonly expressed molecules are S100, CD68, vimentin, and CD1a, accounting for 95.8%, 58%, 38.7%, and 4.5% of cases, respectively. The diagnosis of IDCS should be established if tumor cells express S100, CD68, and vimentin, but are negative for CK, LCA, CD15, CD30, CD21, and CD35. 1 IDCS can be distinguished from metastatic melanoma by similar immunohistochemical features (S-100+, CD68+/−). However the absence of other melanocyte markers may determine the diagnosis. 8 As a marker associated with cell proliferation, Ki-67 expression ranges from 10% to 40% in IDCS, with a median of 20%.10,11 The Ki-67 results in this case were 15%, which could roughly predict the low disease severity of this patient.
Currently, there is no definitive standard treatment for IDCS. The clinical progression course of IDCS is unpredictable, ranging from indolent to invasive, with a high tendency for distant metastasis (in approximately 33% of patients). Localized IDCS can be surgically treated. The 1-year mortality rate of IDCS patients with resectable diseases is 18%, while that of patients with unresectable diseases is 63%. The results of this study indicated that surgical resection was associated with better disease prognosis and survival. 1 Surgical resection is still the primary treatment for local and resectable IDCS. Adjuvant radiotherapy does not significantly improve the overall survival time or reduce recurrence rates, and systemic chemotherapy is the main treatment for patients with distant metastasis. 12 The chemotherapy regimens for patients with metastatic IDCs include CHOP (cyclophosphamide, adriamycin, vincristine, prednisone), ABVD (adriamycin, bleomycin, vincristine, dacarbazine), and ICE (ifosfamide, carboplatin, etoposide). However, the anticancer efficacy of these regimens is very limited.7,8,13 No significant difference in disease-free survival was reported between patients who underwent surgical resection alone compared with those who received adjuvant therapy. 2 Although the patient we reported refused postoperative adjuvant therapy after surgery, owing to the particularity of the location of this case, the patient has been disease-free for more than 1 year after undergoing surgical treatment.
Conclusions
IDCS is a very rare, aggressive, malignant tumor with similar pathological features to DCs and melanoma, which makes diagnosis difficult. Currently, there is no agreed upon standard therapy to treat IDCS. On the basis of this case, we confirm that IDCS can localize to the adrenal region, and that early and timely detection and diagnosis, as well as complete surgical resection of the lesion, are necessary. To date, surgical resection is the only treatment for IDCS that can ensure long-term disease-free survival. We still need more multicenter cases and long-term follow-up data to guide better clinical decision-making when diagnosing and treating IDCS.