
Abstract
Background:
Immune checkpoint inhibitors (ICIs) have shown encouraging treatment efficacy for metastatic breast cancer in several clinical trials. However, response only occurred in a small population. Evidence predicting response and survival of patients with metastatic breast cancer following ICI treatment with existing biomarkers has not been well summarized. This review aimed to summarize the efficacy and predictive factors of immune checkpoint therapy in metastatic breast cancer, which is critical for clinical practice.
Methods:
PubMed, Embase, Cochrane Library, Web of Science, www.clinicaltrials.gov, and meeting abstracts were comprehensively searched to identify clinical trials. The outcomes were objective response rate (ORR), treatment-related adverse events (trAEs), immune-related adverse events (irAEs), progression-free survival (PFS), and overall survival (OS).
Results:
In this review, 27 studies with 1746 patients were included for quantitative synthesis. The pooled ORR was 19% [95% confidence interval (CI) = 12–27%]. Programmed death-ligand 1 (PD-L1)-positive patients had a higher response rate [odds ratio (OR) = 1.44, p = 0.01]. First-line immunotherapy had a better ORR than second-line immunotherapy (OR = 2.00, p = 0.02). Tumor-infiltrating lymphocytes (TILs) ⩾5% (OR = 2.53, p = 0.002) and high infiltrated CD8+ T-cell level (OR = 4.33, p = 0.006) were ideal predictors of immune checkpoint therapy response. Liver metastasis indicated poor response (OR = 0.19, p = 0.009). However, the difference was non-significant in ORR based on age, performance status score, lymph node metastasis, and lactate dehydrogenase (LDH) level. In addition, the PD-L1-positive subgroup had a better 1-year PFS (OR = 1.55, p = 0.04) and 2-year OS (OR = 2.28, p = 0.02) following ICI treatment. The pooled incidence during ICI therapy of grade 3–4 trAEs was 25% (95% CI = 16–34%), whereas for grade 3–4 irAEs it was 15% (95% CI = 11–19%).
Conclusions:
Metastatic breast cancer had modest response to ICI therapy. PD-L1-positive, first-line immunotherapy, non-liver metastasis, and high TIL and CD8+ T-cell infiltrating levels could predict better response to ICI treatment. Patients with PD-L1-positive tumor could gain more survival benefits from immune checkpoint therapy.
Introduction
According to the estimates of global cancer statistics, breast cancer is known as the most common cancer and the second leading cause of cancer-related death among women. 1 In the United States, approximately 268,600 new cases and 42,260 deaths due to female breast cancer are expected to occur in the year 2019. 2 Despite the progress and advancements in the systematic treatment of breast cancer, approximately 20% of the patients will experience distant metastatic disease in the first 5 years. 3 Patients with recurrence or metastatic breast cancer have a poor prognosis with a 5-year relative survival rate of 27%. 2
In recent years, immune checkpoint therapy has been proved as an effective strategy in various advanced solid tumors and has rapidly become a hotspot in the research of antitumor drugs. Following the great success of immune checkpoint inhibitors (ICIs) in melanoma in 2010, multiple new monoclonal antibodies against cytotoxic T-lymphocyte-associated antigen-4 (CTLA-4), programmed cell death protein-1 (PD-1), and programmed cell death-ligand-1 (PD-L1) have been trialed and approved by the US Food and Drug Administration (FDA) in a diversity of solid tumors. 4 Although breast cancer was once regarded as an immune-quiescent tumor, recent research has reported that some subtypes may respond favorably to immune checkpoint therapy. 5 Patients with metastatic breast cancer have shown an objective response rate (ORR) of 3~45% following treatment with ICIs in different reported phase II clinical trials.6–10 In the newly reported phase III trial (IMpassion130), the PD-L1 inhibitor atezolizumab combined with nab-paclitaxel conferred a significant improvement of progression-free survival (PFS) compared with the nab-paclitaxel group in triple-negative breast cancer (7.2 months versus 5.5 months). 11 In addition, patients with PD-L1-positive tumors had a better PFS compared with patients with PD-L1-negative tumors. In another study by Voorwerk et al., patients with a high level of tumor-infiltrating CD8+ T cells were also associated with a better ORR during the treatment with ICIs. 12 Although immunotherapy demonstrated a promising efficiency in metastatic breast cancer, only a small proportion of patients would benefit from it in addition to a high rate of severe adverse events. To date, evidence predicting the response and survival of patients with metastatic breast cancer following ICI treatment with existing biomarkers has not been adequately summarized.
In this study, we performed a systematic review and meta-analysis of the reported clinical trials to evaluate the response and safety of immune checkpoint therapy in patients with metastatic breast cancer. In addition, the predictive role of several existing biomarkers for immunotherapy response was also investigated for the first time to identify the population who would potentially benefit.
Methods
Search strategy
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. 13 Cochrane information (https://methods.cochrane.org/prognosis/tools) and prognostic meta-analysis guidelines were used as a guidance for biomarker analysis. 14
The PICOTS system was used to describe the key items for framing this review and its objective and methodology:
Population – patients with metastatic breast cancer.
Index prognostic factors – particular biomarker (PD-L1 expression, line of ICI therapy, tumor-infiltrating lymphocyte [TIL] level, CD8+ T-cell infiltration level, liver metastasis, age, Eastern Cooperative Oncology Group [ECOG] performance status score, lymph node metastasis and lactate dehydrogenase [LDH] level).
Comparator prognostic factors – not applicable for this review.
Outcomes – objective response rate (ORR), treatment-related adverse events (trAEs), immune-related adverse events (irAEs), progression-free survival (PFS) and overall survival (OS).
Timing – biomarker measurements were performed before ICI treatment and all follow-up information on the outcomes were extracted from the studies.
Setting – hospital/treatment center.
A comprehensive search of PubMed, Embase, the Cochrane Library, Web of Science online databases and www.clinicaltrials.gov was performed on 5 August 2019. The retrieval strategy contained the following keywords: Nivolumab, Pembrolizumab, Atezolizumab, Durvalumab, Avelumab, Ipilimumab, Tremelimumab, immune checkpoint inhibitor, PD-1 inhibitor, PD-L1 inhibitor, CTLA-4 inhibitor, and breast cancer. The detailed protocol and search strategy are presented in Supplemental Appendices 1 and 2. We also reviewed abstracts from American Society of Clinical Oncology conferences using the same criteria reported in the following. The reference lists from these studies were hand searched for eligible articles. All search strategies were conducted following the guidelines.
Inclusion and exclusion criteria
Only prospective clinical trials of patients with metastatic breast cancer treated with an ICI (including anti-PD-1, anti-PD-L1, and anti-CTLA-4 inhibitor) that reported ORR, trAEs, irAEs, PFS or OS outcomes were included. Articles published online ‘ahead of print’ were included. Meeting abstracts without published full-text original articles were eligible for this study. Exclusion criteria were insufficient data, not advanced or metastatic breast cancer, preclinical studies, case reports, letters, commentaries, and reviews. In addition, retrospective studies were excluded in this review. When duplicate studies from the same trial were identified, only those with the most complete and updated data were included.
Study selection
All search results were independently inspected by two authors (YZ and XZ) and discrepancies were consulted with a third reviewer (SZ). Reviewers applied selection criteria after screening the potentially included studies. Duplicates were removed using Endnote X9 software or manually.
Data extraction
Baseline characteristics of each study (authors, year of publication, or conference presentation, line of ICI treatment, type of ICI agents, breast cancer subtype, number of patients enrolled, combination therapy, and median OS) were recorded by two reviewers independently. The primary outcome was the ORR, while the secondary outcomes were trAEs, irAEs, PFS, and OS. Data were extracted from different subgroups in the same trial to analyze biomarkers that predict ORR, PFS and OS of ICI treatment. These results were described by odds ratios (ORs) and 95% confidence intervals (CIs).
Methodology quality assessment
The quality of each randomized controlled trial (RCT) and non-randomized trial was assessed using the Cochrane risk-of-bias tool and the methodological index for non-randomized studies (MINORS), respectively. The risk of bias using the Cochrane risk-of-bias tool was expressed as low, high, or unclear risk including the aspects of selection, performance, detection, attrition, reporting, and other biases. MINORS is recognized as the most appropriate guideline to evaluate the methodological quality of non-randomized trials and contains eight specific items. 15 The Quality In Prognosis Studies (QUIPS) tool was used to assess the risk of bias in the studies of prognostic factors.14,16 Six important domains were considered for evaluation, including study participation, study attrition, prognostic factor measurement, confounding measurement and account, outcome measurement, and analysis and reporting. Two reviewers made the assessments, with disagreements consulted with a third reviewer. All RCTs and non-randomized trials were scored and recorded.
Quality of evidence assessment
The Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach was used to assess the quality of evidence of the major outcomes. The following elements were included for evaluation: study design, risk of bias, inconsistencies, imprecision of the results, indirectness, and publication bias. The quality of evidence for the major outcomes was graded as high, moderate, low, or very low.
Data synthesis and analysis
The rates of ORR, trAEs, and irAEs were extracted and pooled using the Meta package in R software (version 3.5.0). ORs and 95% CIs describing the predictive outcomes (ORR, PFS, and OS) of biomarkers were synthesized using Review Manager software (version 5.3, Cochrane Collaboration). The difference was considered significant when 95% CI does not include 1.0. We used Cochrane’s Q test (reported with a χ2 value and p value) and the I2 test to estimate study heterogeneity. Heterogeneity was indicated if p < 0.1 and I2 > 50%. ORs and 95% CIs for each of the comparisons in the subgroup were pooled using the fixed-effects model (if heterogeneity Cochrane’s Q test p > 0.1) and the random-effects model (if heterogeneity Cochrane’s Q test p < 0.1) in the Review Manager software. 17 Subgroup analysis was performed to address the possible sources of heterogeneity and identify the potential subsets of patients. Meta-regression was also performed to explain heterogeneity using the Meta package in R software. In addition, Egger’s test was performed with STATA software 15.1 (Stata Corp, College Station, TX, USA) to assess potential publication bias. 18
Results
Baseline characteristics of included studies
The details of our literature search are summarized in the PRISMA flow diagram (Figure 1). Overall, our electronic search strategy identified 1492 potential articles, of which 27 studies were included in the systematic review. Of the 27 studies, 16 were full-text articles, whereas 11 studies were abstracts. Sixteen studies used PD-1 antibody,7,8,12,19–31 eight studies used PD-L1 antibody,6,9–11,32–35 two studies used CTLA-4 antibody36,37 and one study used both PD-1 and CTLA-4 antibody. 38 Patients with triple-negative breast cancer (TNBC), human epidermal growth factor receptor 2 (HER2) overexpression, and breast cancer with any subtypes were enrolled in 16, two, and nine studies, respectively. The main baseline characteristics of the included studies are reported in Table 1. Overall, 27 studies that enrolled 1746 patients were included in the final quantitative synthesis. The methodology quality of included studies was evaluated in both RCTs and non-randomized trials (Supplemental Tables 1 and 2). The risk of bias of included prognostic factors studies was assessed using the QUIPS tool (Supplemental Table 3).
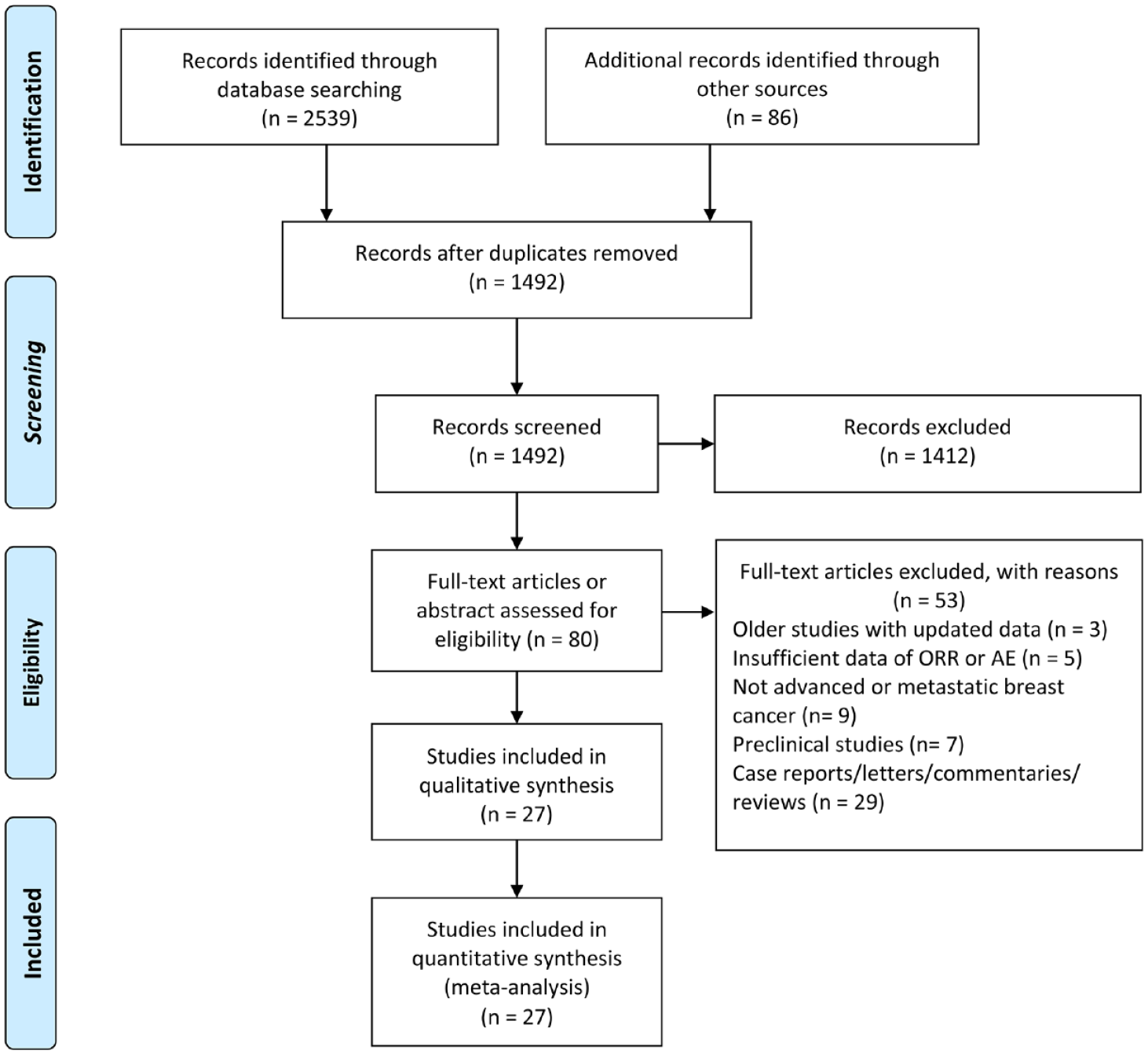
PRISMA flow diagram of study retrieval and selection.
Main baseline characteristics and outcomes of the included studies.

BRCA1/2, BRCA1/2 DNA repair associated; C, group of control; CTLA-4, cytotoxic T lymphocyte-associated antigen 4; E, group of experiment; ER+, estrogen receptor positive; HER2+, human epidermal growth factor receptor 2 overexpression; NA, not available; NCT, national clinical trial; ORR, overall response rate; OS, overall survival; PD-1, programmed death 1; PD-L1, programmed death ligand 1; RCT, randomized controlled trial; TNBC, triple negative breast cancer.
Objective response rates of ICI treatment
The data for ORR were available from 27 studies, including 1746 patients treated with immune checkpoint therapy. The pooled percentage for ORR was 19% (95% CI = 12–27%) (Supplemental Figure 1). In subgroup analysis, anti-PD-L1 immunotherapy had a higher rate of ORR compared with anti-PD-1 immunotherapy (28% versus 16%) (Figure 2). No response in patients was observed after receiving anti-CTLA-4 immunotherapy in both trials. An objective response was observed in 35% (95% CI = 19–50%) of patients who received the first-line immunotherapy and 22% (95% CI = 12–35%) of patients treated with second-line immunotherapy. With an ORR of 23% and 28%, TNBC and HER2 overexpression breast cancer had a relatively higher ORR than other breast cancer subtypes. The combination of immunotherapy with systematic therapy demonstrated a better ORR than monotherapy with ICI (26% versus 9%). In addition, 49% of patients achieved objective response after receiving a combination of ICI and nab-paclitaxel/paclitaxel chemotherapy, which had the highest ORR in all combined treatments. Other subgroup comparisons are shown in Figure 2. Subgroup analysis of ORR revealed that heterogeneity considerably decreased after division into specific subgroups in varying degrees (Figure 2). Given the heterogeneity, its contribution of median OS, proportion of PD-L1-positive patients, median age, sample size, year of publication, and quality score were analyzed by meta-regression analysis (Supplemental Figure 3A). ORR was significantly correlated with median OS, which was a contribution to overall heterogeneity (p = 0.004). Egger’s test (p = 0.196) indicated no publication bias existed in this meta-analysis for ORR.

Forest plot of subgroup analysis of ORR in different immune checkpoint targets, line of ICI therapy, PD-L1 expression, ICI drug, subtype of breast cancer, metastatic site, CD8+ T-cell infiltration level, tumor-infiltrating lymphocytes, and combination therapy.
Biomarkers for ORR, PFS, and OS following ICI treatment
To determine the prognostic factors of ORR, PFS, and OS in patients with metastatic breast cancer receiving ICI treatment, 13 studies with subgroup data were included for further analysis. PD-L1-positive patients had a higher ORR than those with PD-L1-negative tumors (OR = 1.44, 95% CI = 1.09–1.91, p = 0.01, I2 = 0%) (Figure 3A). As PD-L1 expression on immune cells is more prevalent than that on tumor cells in breast cancer, 39 we also evaluated the predicted value based on PD-L1 expression on immune cells. However, PD-L1 expression on infiltrating immune cells (OR = 1.33, 95% CI = 0.93–1.90, p = 0.12, I2 = 0%) was not able to predict ORR of immunotherapy (Supplemental Figure 2A). First-line immunotherapy showed a better ORR than second-line immunotherapy (OR = 2.00, 95% CI = 1.13–3.52, p = 0.02, I2 = 0%) (Figure 3B). There was an association between TIL and tumor-infiltrated CD8+ T-cell level and ORR in favor of TIL ⩾5% (OR = 2.53, 95% CI = 1.39–4.61, p = 0.002, I2 = 38%) and patients with high CD8+ T cells (OR = 4.33, 95% CI = 1.53–12.22, p = 0.006, I2 = 7%) (Figure 3C–D). Patients with liver metastasis had a poorer ORR compared with those with metastasis in other sites (OR = 0.19, 95% CI = 0.06–0.66, P = 0.009, I2 = 0%) (Figure 3E). In addition, the difference was non-significant in ORR based on age, performance status score, lymph node metastasis, and LDH level (Supplemental Figure 2B–E). Tumor mutation burden (TMB) was only reported in one study, which revealed a non-significant difference between the response and non-response group. 12 Microsatellite instability (MSI) was also reported in one study to predict response and survival. One patient with MSI breast metastatic tumor had an ongoing remission for 102 weeks after receiving ICI for 1 year. 12 Data of 1-year PFS, 1-year OS, and 2-year OS were collected from subgroups of the previously mentioned studies. Pooled analysis demonstrated that patients with PD-L1-positive tumor had a better 1-year PFS than those with PD-L1-negative tumor following ICI therapy (OR = 1.55, 95% CI = 1.02–2.36, P = 0.04, I2 = 0%) (Figure 4A). PD-L1-positive expression was not a predictive biomarker for 1-year OS following immunotherapy, possibly due to the short follow-up time (OR = 1.19, 95% CI = 0.91–1.56, p = 0.20, I2 = 15%) (Supplemental Figure 4). However, patients with PD-L1-positive tumor had better 2-year OS after receiving ICI therapy (OR = 2.28, 95% CI = 1.16–4.48, p = 0.02, I2 = 0%) (Figure 4B). With atezolizumab, patients with PD-L1-positive tumor in a phase III trial (IMpassion130) had an improved OS, which indicated that immune checkpoint therapy has better effect in certain populations (hazard ratio = 0.62; 95% CI = 0.45–0.86). Egger’s test was conducted to assess publication bias in the biomarker meta-analysis. No potential publication bias was observed except in the case of performance status score (Supplemental Figure 5). GRADE quality of evidence assessment and its clinical importance is summarized in Supplemental Table 4.

Forest plots of ORR comparisons based on (A) PD-L1 expression, (B) line of ICI therapy, (C) TIL level, (D) CD8+ T-cell infiltration level, and (E) liver metastasis

Forest plots of comparison of (A) PFS rate at the first year and (B) OS rate at the second year based on PD-L1 expression level after receiving ICI treatment.
Incidence of adverse events
The pooled analysis of safety outcomes was conducted in 21 studies, including trAEs and irAEs. The ICI treatment had a relative high frequency of trAEs of any grade (70%, 95% CI = 58–82%) (Supplemental Figure 6A) and trAEs of grade 3 or more severity (25%, 95% CI = 16–34%) (Supplemental Figure 7A). Combination of ICI treatment with systematic therapy (91%, 95% CI = 85–97%) had a higher incidence of trAEs of any grade compared with monotherapy (64%, 95% CI = 64% to 68%) (Supplemental Figure 8A). Combination of ICI with nab-paclitaxel/paclitaxel chemotherapy had the highest rate of trAEs of any grade (98%, 95% CI = 94–100%) in all combinations. The incidence of irAEs of any grade and 3–4 grade was 34% (95% CI = 18–51%) and 15% (95% CI = 11–19%), respectively (Supplemental Figures 6B and 7B). All grade irAEs occurred in 28% (95% CI = 12–44%) of patients treated with PD-1 inhibitors and were found in 53% (95% CI = 11–94%) of patients treated with PD-L1 inhibitors (Supplemental Figure 8B). Pembrolizumab (18%, 95% CI = 12–25%) and avelumab (10%, 95% CI = 6–16%) had a significantly lower rate of irAEs compared with atezolizumab (74%, 95% CI = 41–100%) and nivolumab (81%, 95% CI = 70–89%) (Supplemental Figure 8B).
Ongoing randomized controlled phase III trials
We identified five ongoing randomized controlled phase III trials evaluating immune checkpoint therapy in combination with chemotherapy in metastatic breast cancer (Table 2). ICI was used as the first-line and second-line therapies in four and one study, respectively, for metastatic breast cancer. Pembrolizumab (PD-1 inhibitor) and atezolizumab (PD-L1 inhibitor) were investigated in three and two trials, respectively. Only one trial had enrolled patients with HER2+ breast cancer and evaluated the impact of atezolizumab on PFS in combination with pertuzumab, trastuzumab, and paclitaxel. The estimated completion dates of these trials range from 11 April 2019 to 1 January 2023.
Ongoing randomized controlled phase III trials with immune checkpoint therapy in advanced or metastatic breast cancer.

NCT, national clinical trial; OS, overall survival; PFS, progression-free survival; TNBC, triple negative breast cancer; HER2+, human epidermal growth factor receptor 2 overexpression.
Discussion
To date, this study is the first meta-analysis investigating the efficacy and safety of ICI treatment in patients with metastatic breast cancer. In particular, this review is the first to summarize the several potential biomarkers for response and survival prediction which is essential to identify the patients who benefited from treatment with ICIs. The results showed that immune checkpoint therapy had an ORR of 19% (95% CI = 12–27%). Subgroup analysis demonstrated that PD-L1-positive tumor, first-line immunotherapy, high TIL level, non-liver metastasis, and high CD8+ T-cell infiltrating level predict high ORR in ICI treatment. PD-L1 expression on infiltrating immune cells was not an ideal biomarker for response prediction. With respect to survival prediction, PD-L1 expression was a potential prognostic factor for 1-year PFS and 2-year OS following immune checkpoint therapy. TNBC and HER2 overexpression breast cancer had a relatively higher ORR than other breast cancer subtypes. The combination of immunotherapy with systematic therapy showed a better ORR than ICI (26% versus 9%) monotherapy. Approximately half of the patients achieved objective response following combination of ICI with nab-paclitaxel/paclitaxel chemotherapy, which had the highest ORR in all combination treatment. The incidence of grade 3–4 trAEs was 25% (95% CI = 16–34%) while grade 3–4 irAEs was 15% (95% CI = 11–19%) during immunotherapy. All grade trAEs occurred in almost all patients treated with the combination of ICI and nab-paclitaxel/paclitaxel chemotherapy. PD-1 inhibitors showed fewer all grade irAEs than PD-L1 inhibitors.
Given the remarkable innovation and progress made in immunotherapeutic strategies to treat cancer, novel active agents have emerged as the saviors of patients with multiple advanced or metastatic cancers. 40 Over the past decade, strategies such as monoclonal antibodies, immune enhancing adjuvants, vaccines against oncogenic viruses, and adoptive cell therapies have been well established. 41 Targeting regulatory pathways in T cells, immune checkpoint therapy has demonstrated its efficacy and benefit in improving the survival in metastatic melanoma, non-small cell lung cancer, and renal cell carcinoma.42–44 The efficacy of immune checkpoint therapy in breast cancer has been examined in initial clinical trials, which revealed modest but interesting responses. 45 In the phase III randomized clinical trial (IMpassion130), the PD-L1 inhibitor atezolizumab combined with nab-paclitaxel conferred a significant improvement of PFS compared with the nab-paclitaxel group in TNBC (hazard ratio = 0.80; 95% CI = 0.69–0.92; p = 0.002). As a result, atezolizumab became the first FDA-approved immune checkpoint agent for use in combination with nab-paclitaxel for patients with metastatic TNBC in March 2019. Although significant benefit for PFS was found in the atezolizumab treatment group, OS was non-significant between the two groups in all patients (hazard ratio = 0.84; 95% CI = 0.69–1.02; p = 0.08). However, atezolizumab revealed an improved OS in patients with PD-L1-positive tumors, indicating that immune checkpoint therapy has a better effect in certain populations (hazard ratio = 0.62; 95% CI = 0.45–0.86). In this study, positive PD-L1 expression was found to be associated with an improved 1-year PFS and 2-year OS in patients receiving immune checkpoint therapy. These results are critical for clinical practice in selecting patients who would potentially benefit.
Historically, breast cancer was considered immunologically quiescent compared with other solid tumors such as non-small cell lung cancer and melanoma. With a lower TMB, breast cancer may have fewer neoantigen generations to stimulate antitumor immune response. 46 TNBC and HER2 overexpression breast cancers are known to have higher TMB and TIL rates compared with luminal breast cancer.47–49 The immune microenvironment can exert great influence on the progression of breast cancer, which results in the different clinical prognosis of patients.50–52 We found that patients with TNBC and HER2 overexpression breast cancer had a better response to immune checkpoint therapy, which could be attributed to their high TMB and TIL rate. In addition, a high TIL level was associated with a high response rate. The PD-L1 expression level is an acknowledged prognostic factor in different cancers.53–55 PD-L1 expression in tumor cells is a confirmative biomarker for predicting response to PD-1/PD-L1 checkpoint inhibition according to the analyses of more than 10 different solid tumors, which was the same as that for breast cancer in our results.56–58 PD-L1 mainly expresses on tumor-infiltrating immune cells rather than on tumor cells in patients with TNBC, thus it might be a prognostic factor for response. 59 We performed a pooled analysis of the response rate based on the PD-L1 status on tumor-infiltrating immune cells and found a non-significant positive trend. Liver metastasis of breast cancer indicates a poor response to immune checkpoint therapy compared with other metastatic sites. The liver is an immune tolerogenic organ because of its exposure to various antigens (toxins, gut-derived microbial products, etc.) and chronic inflammatory state.60,61 Several mechanisms have been proved to explain liver-induced immune tolerance, including trapping and inactivation of CD8+ T cells,62,63 activation of Treg cells by Kupffer cells 64 and poor activation of CD4+ T cells. 65 In addition, chronic hepatitis B virus (HBV) infection can remarkably induce natural killer cell receptor imbalance and dysfunction which results in immune tolerance. 66 Therefore, liver metastatic cancers have a lower response to ICI treatment by means of these mechanisms to evade the immune system and facilitate tumor progression.
Detection of PD-L1 is always an important research direction of cancer immunotherapy. Immunohistochemistry (IHC) is the most common method to determine PD-L1 expression and multiple monoclonal PD-L1 antibodies have been well developed, such as clone 22C3, 67 clone 28-8, 68 and clone SP142. 69 However, the accuracy of these PD-L1 IHC detection methods has remained controversial. PD-L1 assessment by IHC can sometimes show as false negative, which means some patients with PD-L1 positive are misdiagnosed as PD-L1 negative. For instance, glycosylation of cell surface PD-L1 can render its polypeptide antigens inaccessible to PD-L1 antibodies, which can lead to false negative IHC judgement and inconsistent therapeutic outcomes of ICI treatment. 70 As a result, a small proportion of patients with PD-L1-negative tumor can still gain benefit from ICI therapy according to the outcomes of clinical trials. Therefore, developing advanced methods or using multiple biomarkers to make joint prediction is the focus of future investigation. For example, removing the glycosylation and exposing the antigens before PD-L1 IHC staining to reduce the false-negative rate of detection. 70
This analysis had several limitations. First, given the lack of randomized clinical trials in the initial stages of immunotherapy research in breast cancer, bias was inevitable to some extent. Second, several important prognostic values for response and survival were not included in the subgroup meta-analysis (TMB, MSI, etc.). Third, the small number of patients enrolled in each clinical trial contributed to the high heterogeneity in the analysis of response and adverse events. Fourth, as the clinical exploration of ICI treatment in breast cancer is still in the early stages, results of biomarker prediction from multivariate analysis have not been reported. Outcomes from multivariate analysis, by which the prognostic effect of this biomarker can be evaluated together with other prognostic factors after proper adjustment, are far more informative than those from univariate analysis. A new biomarker might not add to existing predictors if adjusted results are unavailable. Therefore, more multicenter RCTs with high quality, large sample size, multivariate analysis, and adequate follow-up are required for further validation.
In conclusion, although immune checkpoint therapy has demonstrated its promising efficacy in metastatic breast cancer, the majority of patients are not likely to benefit from it. Different populations appeared to have varying responses to ICI treatment. Our analysis found that PD-L1-positive tumor, first-line immunotherapy, non-liver metastasis, high TIL, and CD8+ T-cell infiltrating level could predict a better response to ICI therapy. The PD-L1-positive subgroup could gain more survival benefits from immune checkpoint therapy.
Supplemental Material
Supplementary_Materials_3 – Supplemental material for Efficacy and predictive factors of immune checkpoint inhibitors in metastatic breast cancer: a systematic review and meta-analysis
Supplemental material, Supplementary_Materials_3 for Efficacy and predictive factors of immune checkpoint inhibitors in metastatic breast cancer: a systematic review and meta-analysis by Yutian Zou, Xuxiazi Zou, Shaoquan Zheng, Hailin Tang, Lijuan Zhang, Peng Liu and Xiaoming Xie in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Authors Yutian Zou, Xuxiazi Zou and Shaoquan Zheng contributed equally to this work.
Author contributions
Conception and design, XX and PL; development of methodology, YZ and XZ; acquisition of data, YZ, XZ, SZ and HT; formal analysis, YZ and LZ; writing, YZ, XZ and SZ; reviewing and editing, XX and PL. All authors read and approved the final manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the National Natural Science Foundation of China (81872152, Xiaoming Xie).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.