
Abstract
Background:
High cathepsin D has been associated with poor prognosis in breast cancer; however, the results of many studies are controversial. Here, we assessed the association between high cathepsin D levels and worse breast cancer prognosis by conducting a meta-analysis.
Methods:
A comprehensive search strategy was used to search relevant literature in PUBMED and EMBASE by September 2018. The meta-analysis was performed in Review Manager 5.3 using hazard ratios (HRs) with 95% confidence intervals (CIs).
Results:
A total of 15,355 breast cancer patients from 26 eligible studies were included in this meta-analysis. Significant associations between elevated high cathepsin D and poor overall survival (OS) (HR = 1.61, 95% CI: 1.35–1.92, p < 0.0001) and disease-free survival (DFS) (HR = 1.52, 95% CI: 1.31–2.18, p < 0.001) were observed. In the subgroup analysis for DFS, high cathepsin D was significantly associated with poor prognosis in node-positive patients (HR = 1.38, 95% CI: 1.25–1.71, p < 0.00001), node-negative patients (HR = 1.78, 95% CI: 1.39–2.27, p < 0.0001), early stage patients (HR = 1.73, 95% CI: 1.34–2.23, p < 0.0001), and treated with chemotherapy patients (HR = 1.60, 95% CI: 1.21–2.12, p < 0.001). Interestingly, patients treated with tamoxifen had a low risk of relapse when their cathepsin D levels were high (HR = 0.71, 95% CI: 0.52–0.98, p = 0.04) and a high risk of relapse when their cathepsin D levels were low (HR = 1.50, 95% CI: 1.22–1.85, p = 0.0001).
Conclusions:
Our meta-analysis suggests that high expression levels of cathepsin D are associated with a poor prognosis in breast cancer. Based on our subgroup analysis, we believe that cathepsin D can act as a marker for poor breast cancer prognosis and also as a therapeutic target for breast cancer.
Keywords
Background
Breast cancer is the most common cancer among women worldwide. In 2018, 2.1 million new cases were diagnosed and approximately 626,000 deaths were reported due to breast cancer. 1 Most breast cancer patients in the United States are diagnosed with early stage disease. 2 Although the five-year survival rate for breast cancer is close to 100% when detected at an early stage, more aggressive breast cancer is likely to return if a proper adjuvant therapy is not given after surgery.3,4 For this reason, adjuvant therapy after primary surgery plays an important role in the survival of breast cancer patients. Various factors affect breast cancer adjuvant therapy decision making. The factors currently taken into account for adjuvant therapy decision making include tumor size, lymph node status, and tumor characteristics (hormone receptor status, HER2 status, and KI-67 status). However, these factors are not instructive for all patients concerning the decision to get adequate adjuvant therapy. Therefore, new protein and molecular markers have been proposed as decision-making aids.5,6
Cathepsin D (CTSD) was first described by Westley and Rochefort in 1979. It is also termed aspartic endoproteinase and is proteolytically active at low pH. 7 CTSD is over-expressed by human epithelial breast cancer cells and results in over-secretion of 52-kDa pro-CTSD into the extracellular environment. 8 CTSD secreted into the extracellular environment is automatically activated under acidic conditions, and activated CTSD affects breast cancer progression by increasing breast cancer cell proliferation, fibroblast growth, tumor angiogenesis, tumor growth and metastasis.9–12 Recent studies have shown that CTSD is involved in estrogen receptor activity and tamoxifen’s drug response,13,14 and has a poor prognosis with extensive induction of angiogenesis in both ovarian and breast cancers.10,15 It has also been reported as a biomarker capable of predicting metastasis and tumor-specific extracellular targets suitable for antibody-based therapies.9,16 As a result, CTSD was expected to act as a potential prognostic factor for breast cancer. Many studies have evaluated the prognostic value of CTSD in breast cancer patients, but contrary to expectations, some studies evaluating the prognostic value of CTSD have shown conflicting results. For this reason, we performed a meta-analysis of relevant literature to better quantify the prognostic impact of CTSD expression.
Methods
Search strategy
In this meta-analysis, we selected studies evaluating the relationship between CTSD protein expression and prognosis in breast cancer. We followed the PRISMA standard guidelines to perform the meta-analysis of observational studies and wrote the manuscript according to the PRISMA checklist 17 (see Supplemental Table 1). PubMed and EMBASE databases were searched through September 2018 for relevant articles that reported the association between CTSD levels and the hazard ratio of breast cancer. To fulfil our selection criteria, the studies had to have been published as a full paper in English; reference lists and review articles were included. Articles were identified by an electronic PUBMED and EMBASE database search using the following keywords: ‘CTSD’, ‘CD’, ‘Cathepsin D’, ’breast cancer’, ‘breast cancer’, ‘breast carcinoma’, ‘breast neoplasm’, ‘breast tumor’, ‘breast tumour’, ‘hazard ratios’, ‘hazard ratio’, ‘HR’, ‘HRs’, ‘survival’, and ‘prognosis’ (see Supplemental Table 2).
Study selection
The inclusion criteria for the analysis were as follows: studies published as full articles and in the English language on adult patients (at least 20) with breast cancer that reported either the prognostic impact of CTSD evaluated by immuno-histochemistry (IHC), enzyme-linked immunosorbent assay (ELISA), immunoradiometric assay (ELSA), and radioimmunoassay (RIA). Studies that included the hazard ratios and 95% confidence intervals (CIs) for overall survival (OS), disease-free survival (DFS), and relapse-free survival (RFS). In this meta-analysis, the results of DFS and RFS were integrated into DFS. Duplicate publications were excluded. Two reviewers independently evaluated all the titles and abstracts identified by the search. The results were then pooled, and all potentially relevant publications were retrieved in full. The two reviewers then evaluated the complete articles for eligibility. To avoid the inclusion of duplicated or overlapping data, we compared author names and the institutions where the patients were recruited. The reasons to consider articles as non-evaluable were: (a) no univariate analysis reported; (b) no possibility to calculate HR using one of the methods mentioned above because the distribution of CTSD was not reported in the article or CTSD was analyzed in combination with other prognostic markers rendering analysis impossible; and (c) duplicated data was published in different journals.
Data extraction and quality assessment
Information was extracted from all publications. The meta-analysis was initially conducted for all the included studies for each of the endpoints of interest. DFS was the primary outcome of interest and OS was the secondary outcome of interest. The following data were collected from each study: author names, publication date, follow-up, detection method, staining location, and the CTSD cut-off value used for analysis. High CTSD was defined according to the cut-off chosen by each author. Subgroup analyses were conducted for node-positive, node-negative, early stage, treated with adjuvant chemotherapy, and treated with tamoxifen subgroups and if there were at least two papers for each subgroup. The quality of each nonrandomized study was evaluated using the validated Newcastle–Ottawa Scale (NOS) in this meta-analysis 18 (see Supplemental Table 3). This scale awards a maximum of nine points to each cohort study (four for quality of selection, two for comparability, and three for quality of outcome and adequacy of follow-up). Studies with an NOS score of 6 were classified as high quality and only such studies were included in our meta-analysis.
Statistical analyses
In this meta-analysis, we included articles that have information including HR and its 95% CI or Kaplan–Meier curve. HRs were calculated based on the high expression of CTSD protein (HR > 1). A HR > 1 implied poor prognosis for patients with breast cancer. The heterogeneity of the studies was evaluated using the I2 value, as described before. 19 We pooled the information with a random or fixed-effect model according to the I2 value. The fixed-effects model method was used when I2 < 50%, indicating a lack of heterogeneity among studies. When heterogeneity was observed, the random-effects model was applied. 20 Publication bias was visually estimated by assessing funnel plots.21,22 The extracted data were aggregated for a meta-analysis using the RevMan5.3 software (Cochrane Collaboration, Copenhagen, Denmark). 23 The prognosis was plotted as a Kaplan–Meier curve and the digitizer Engauge 4.0 software (http://engauge-digitizer.software.informer.com/) was used to digitize and extract the data.
Results
Study characteristics
A flowchart of the studies included in the meta-analysis is presented in Figure 1. A computer-based literature search using the PUBMED and EMBASE databases identified a total of 1003 studies. Among these, 427 studies were eliminated as they were non-human studies, conference abstracts, or articles written in a language other than English. Of the 76 full-text articles evaluated, 50 were eliminated because they contained duplicate data, were review articles, or lacked data necessary for estimating the HR at 95% CI. Finally, 26 studies were included in this meta-analysis. In Tables 1 and 2, the characteristics of included studies are described. The different cut-off values used were those of the authors. Threshold definitions were mean or median values, the best cut-off value, or an established arbitrary value.

Flow chart of the study selection process.
Characteristics of the studies on overall survival outcomes of breast cancer patients according to cathepsin D status.

CTSD, cathepsin D; ELSA, immunoradiometric assay; ELISA, enzyme-linked immunosorbent assay; IHC, immunohistochemistry; KM plot, Kaplan–Meier plot; RIA; radioimmunoassay.
Characteristics of the studies on disease-free survival outcomes of breast cancer patients according to cathepsin D status.

CTSD, cathepsin D; ELSA, immunoradiometric assay; IHC, immunohistochemistry; KM plot, Kaplan–Meier plot.
In total, 19 evaluable studies24–42 for OS (7809 patients) and 15 evaluable studies28,31,33,35,39–41,43–50 for DFS (7546 patients) were included. Subgroup analysis for OS was possible using five studies with 784 node-positive patients,27,28,36,43,51 five studies with 1193 node-negative patients,28,30,34,35,43 and four studies with 575 adjuvant chemotherapy-treated patients.34,36,40,51 Subgroup analysis for DFS was possible for six studies with 2633 node-positive patients,33,36,44,45,48,51 six studies with 2775 node-negative patients,24,25,30,35,36,52 four studies with 657 early stage patients,42,46,48,52 three studies with 459 adjuvant chemotherapy-treated patients,36,44,46 and two studies with 1747 tamoxifen-treated patients.45,47
Analysis of OS or DFS for all patients
The meta-analysis results of the overall population for OS are shown in Figure 2. For the overall population, worse OS (HR = 1.61, 95% CI: 1.35–1.92; p < 0.00001) was observed among patients considered as CTSD positive. Heterogeneity was high (p < 0.00001, I2 = 73%) for these patients; thus, a random-effects model was used. The meta-analysis results of the overall population for DFS is shown in Figure 3. Worse DFS (HR = 1.52, 95% CI: 1.31–1.75; p < 0.00001) was observed among patients considered as CTSD positive. Heterogeneity was high (p = 0.0004, I2 = 64%) for these patients; thus, a random-effects model was used.
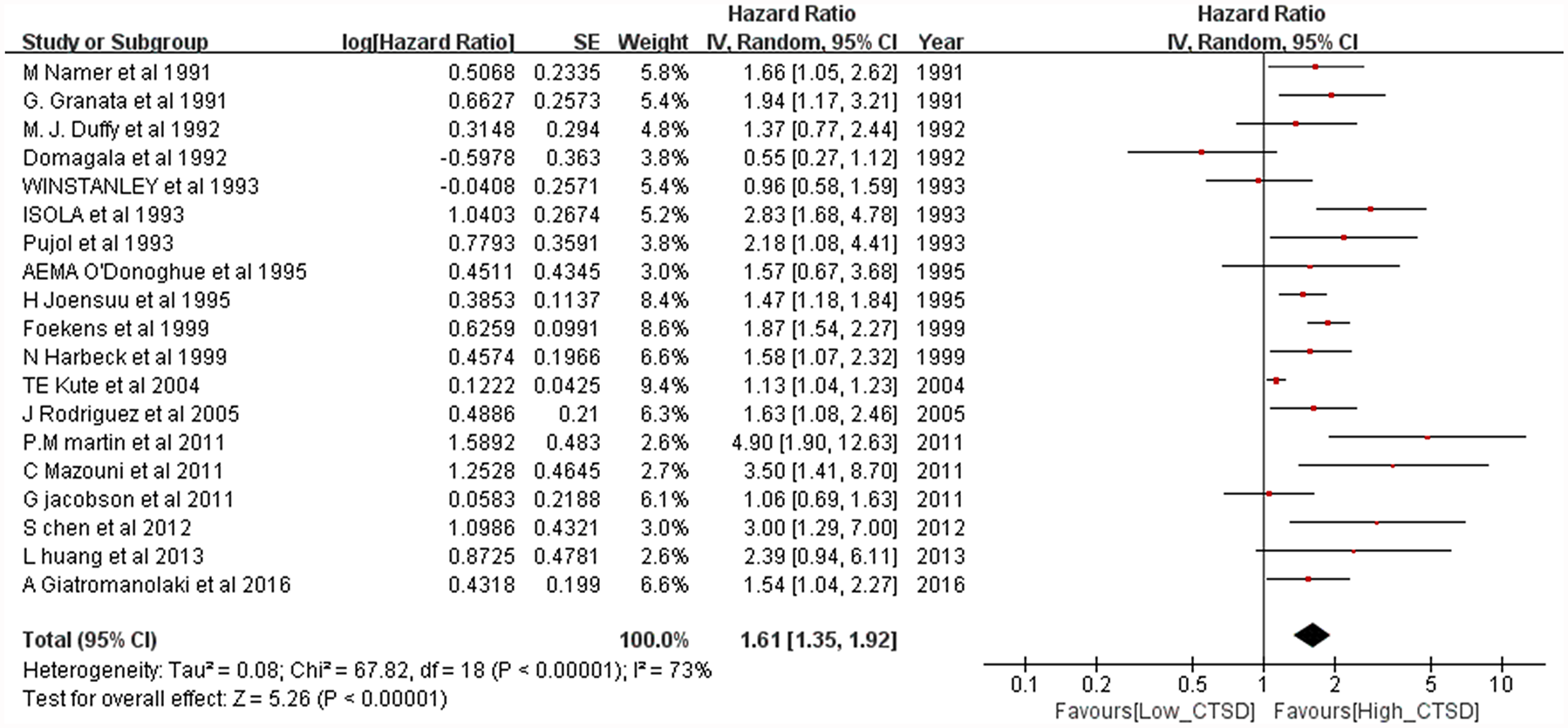
Forest plot for overall survival according to cathepsin D (CTSD) expression.
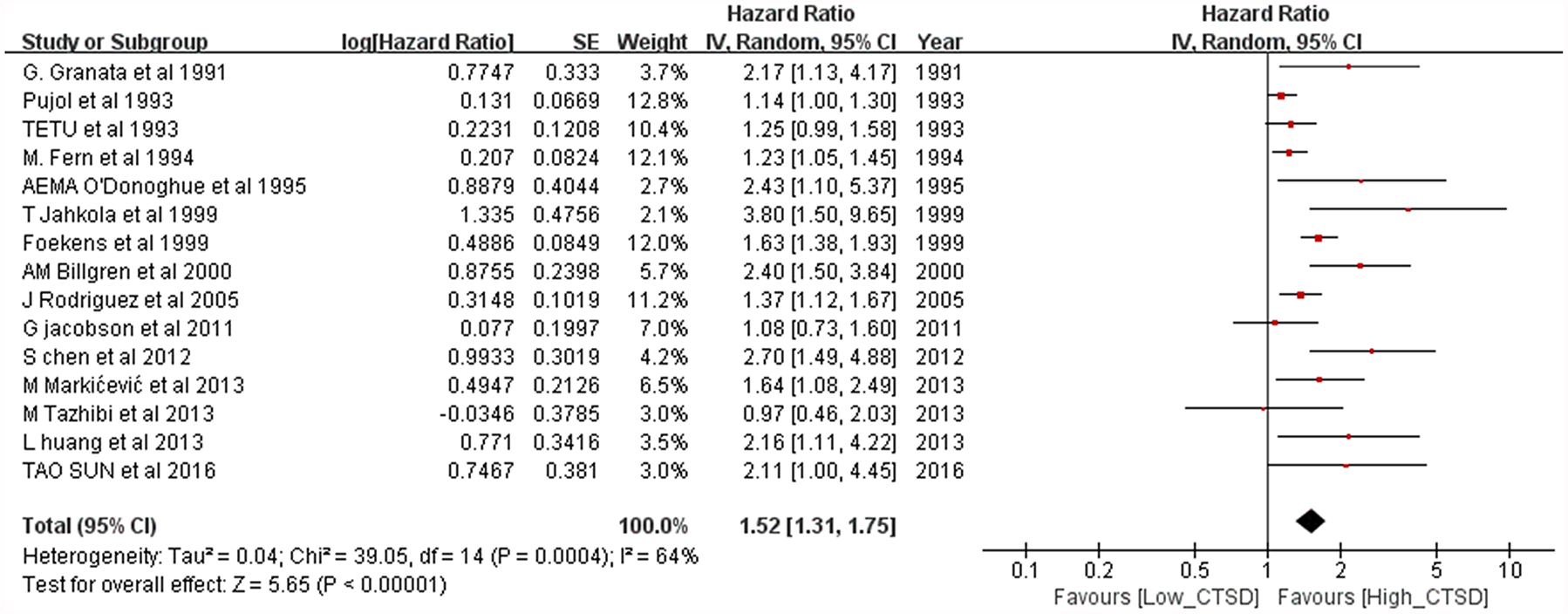
Forest plot for disease-free survival according to cathepsin D (CTSD) expression.
Publication bias
Publication bias was reported via funnel plots; the asymmetry of the funnel plots may have arisen through heterogeneity. The funnel plots of the overall population for OS and DFS are shown in Figure 4. The funnel plots showed an asymmetrical distribution for CTSD among the studies, revealing that publication bias might exist. The funnel plots of subgroup analyses are shown in Supplement Figures 3–5. In the subgroup analyses funnel plots, only the node-negative patients showed an asymmetrical distribution for OS; the remaining groups showed a symmetrical distribution.

Funnel plots of the 27 studies included in the meta-analysis. (a) overall survival and (b) disease-free survival.
Subgroup analyses of OS
In the subgroup analyses for OS, a worse prognosis was observed independently for node-positive patients (HR = 1.65, 95% CI: 1.29–2.11, p < 0.0001; Figure 5a) and node-negative patients (HR = 1.67, 95% CI: 1.18–2.37; p < 0.00001; Figure 5b). Moreover, adjuvant chemotherapy-treated patients showed a worse prognosis (HR = 1.8, 95% CI: 1.39–2.33; p < 0.00001; Figure 5c). Characteristics of the studies included in the subgroup analyses are shown in Table 3.

Forest plots of subgroup analysis for overall survival. (a) node-positive patients, (b) node-negative patients and (c) adjuvant chemotherapy-treated patients.
Summarized hazard ratios of overall and subgroup analyses for overall survival and disease-free survival.

CI, confidence interval; HR, hazard ratio; N–, node-negative; N+, node-positive.
Subgroup analyses of DFS
In the subgroup analyses for DFS, a worse prognosis was observed independently for node-positive patients (HR = 1.38, 95% CI: 1.25–1.71, p < 0.00001; Figure 6a) and node-negative patients (HR = 1.66, 95% CI: 1.44–1.91; p < 0.00001; Figure 6b). Worse prognosis was observed independently for early stage patients (HR = 1.41, 95% CI: 1.16–1.70; p = 0.0004; Figure 6c) and adjuvant chemotherapy-treated patients (HR = 1.6, 95% CI: 1.21–2.12; p = 0.0009; Figure 6d). Patients with high CTSD expression levels showed good prognosis when treated with tamoxifen (HR = 0.71, 95% CI: 0.52–0.98, p = 0.04; Figure 7a). However, patients with low CTSD expression levels showed a worse prognosis when treated with tamoxifen (HR = 1.50, 95% CI: 1.22–1.85, p = 0.0001; Figure 7b).

Forest plot of subgroup analysis for disease-free survival. (a) node-positive patients, (b) node-negative patients, (c) early stage patients and (d) adjuvant chemotherapy-treated patients.
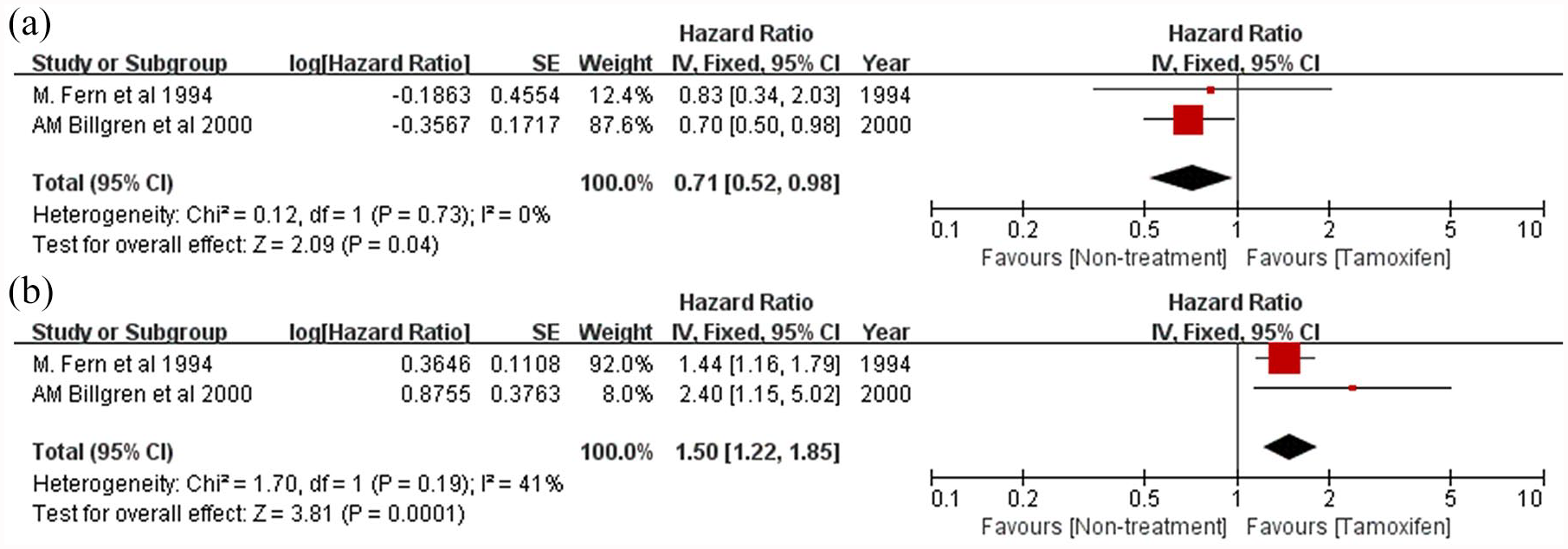
Forest plot of subgroup analyses for patients treated with tamoxifen versus non-treated patients. (a) patients with high cathepsin D expression and (b) patients with low cathepsin D (CTSD) expression.
Discussion
Our meta-analysis confirms that breast cancer patients with high CTSD expression have a worse prognosis in the overall population. The prognostic impact of CTSD was verified through a univariate analysis. Furthermore, our subgroup analysis suggests that CTSD may be helpful to decide the most appropriate adjuvant therapy. To our knowledge, this is the first meta-analysis of published studies to evaluate the association between CTSD expression and prognosis in breast cancer patients.
We found that high CTSD expression in breast cancer was statistically significantly associated with worse prognosis in terms of both OS and DFS. This finding was consistent with most, but not all, of the results of individual studies included this meta-analysis. Prognostic markers are very important for the treatment and prognosis prediction of breast cancer, and we believe that CTSD can be used as a prognostic marker for all breast cancer patients and especially for early stage or node-negative patients. In addition, our subgroup analysis results suggest that CTSD will play an important role in making adjuvant therapy decisions for breast cancer patients.
Adjuvant therapy is currently recommended for all node-positive patients with breast cancer because the 10-year recurrence rate in these patients approaches 70%. In contrast, for node-negative patients with a relatively good prognosis, adjuvant therapy is not recommended. However, even node-negative HER2-positive patients can experience increased recurrence and decreased survival. The prognostic markers considered for adjuvant therapy decision-making for node-negative patients are only HER2 status and tumor size.53,54 More prognostic markers are needed to select the appropriate patients to receive adjuvant therapy. Our study indicates that high CTSD is significantly associated with worse OS and DFS in node-negative patients. These results support previous findings 55 and indicate that CTSD has great potential as a potential prognostic marker for the survival and relapse of node-negative patients. We, thus, believe that CTSD should be considered as a prognostic marker for the survival and relapse of node-negative patients.
In our study, patients with high CTSD seemed to be less affected by adjuvant chemotherapy and had higher rates of relapse at an early stage. Chemotherapy reduces the risk of recurrence in women with early stage breast cancer. However, its absolute benefits may be small and not worth the added risk of toxicity among women with a baseline risk of recurrence.56,57 For this reason, the discovery of accurate prognostic markers that can predict early stage relapse and chemotherapy response is important. Our subgroup analysis indicates that high CTSD can act as a prognostic marker for predicting early stage recurrence and chemotherapy response in breast cancer.
One of the interesting results of our subgroup analysis was the tamoxifen drug response. Hormone-positive breast cancer accounts for about 70% of all breast cancers, and these patients are often treated with anti-hormonal drugs. However, approximately 20–30% of breast cancer patients are resistant to this treatment and have a high risk of relapse.58,59 Although there were only two studies included, these showed that patients with high CTSD who were treated with tamoxifen have a low risk of relapse and patients with low CTSD who were treated with tamoxifen have a high risk of relapse. CTSD is a lysosomal protein that helps maintain homeostasis of cell metabolism and is known to be involved in lysosomal membrane permeabilization. 60 Previous studies have reported that tamoxifen-resistance cells are less susceptible to lysosomal membrane permeabilization, which is associated with low CTSD. These results indicate that CTSD is potentially associated with tamoxifen-resistance and CTSD, and our results support these studies.61–64 These results suggest that CTSD is one of the potentially important proteins for tamoxifen resistance and that CTSD should be considered as a biomarker for predicting tamoxifen resistance.
Study limitations
There are some limitations to our study. First, our meta-analysis only evaluated the univariate prognostic value of CTSD. Because the results from multivariate analyses were excluded, our results may have been biased. Second, heterogeneity existed among the selected studies. Although it was impossible to determine all sources of heterogeneity, we excluded some covariates that might contribute to heterogeneity of data due to unavailable data. These covariates included progesterone receptor status, tumor size, age of patients, and others. Third, in the subgroup analysis, some subgroups contained very small studies, which may bias their findings. Fourth, high CTSD is defined according to the cut-off chosen by each author, so there may be a bias towards high-CTSD definitions. Moreover, language bias might exist due to the references being restricted to English publications only.
Conclusion
Despite some limitations, our meta-analysis supports the prognostic role of CTSD in breast cancer by showing a significant association between its expression and the risk of breast cancer recurrence and death in all populations considered and for both DFS and OS. Furthermore, high CTSD expression may be a potential biomarker for DFS of node-negative, early stage patients and may assist clinicians make decisions regarding tamoxifen treatment.
Supplemental Material
Supplement_Figure_1 – Supplemental material for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis
Supplemental material, Supplement_Figure_1 for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis by Junho Kang, Yeuni Yu, Seongdo Jeong, Hansong Lee, Hye Jin Heo, Jeong Jun Park, Hee Sam Na, Dai Sik Ko and Yun Hak Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
Supplement_Figure_2 – Supplemental material for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis
Supplemental material, Supplement_Figure_2 for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis by Junho Kang, Yeuni Yu, Seongdo Jeong, Hansong Lee, Hye Jin Heo, Jeong Jun Park, Hee Sam Na, Dai Sik Ko and Yun Hak Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
Supplement_Figure_3 – Supplemental material for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis
Supplemental material, Supplement_Figure_3 for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis by Junho Kang, Yeuni Yu, Seongdo Jeong, Hansong Lee, Hye Jin Heo, Jeong Jun Park, Hee Sam Na, Dai Sik Ko and Yun Hak Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
Supplement_Table_1 – Supplemental material for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis
Supplemental material, Supplement_Table_1 for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis by Junho Kang, Yeuni Yu, Seongdo Jeong, Hansong Lee, Hye Jin Heo, Jeong Jun Park, Hee Sam Na, Dai Sik Ko and Yun Hak Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
Supplement_Table_2 – Supplemental material for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis
Supplemental material, Supplement_Table_2 for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis by Junho Kang, Yeuni Yu, Seongdo Jeong, Hansong Lee, Hye Jin Heo, Jeong Jun Park, Hee Sam Na, Dai Sik Ko and Yun Hak Kim in Therapeutic Advances in Medical Oncology
Supplemental Material
Supplement_Table_3 – Supplemental material for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis
Supplemental material, Supplement_Table_3 for Prognostic role of high cathepsin D expression in breast cancer: a systematic review and meta-analysis by Junho Kang, Yeuni Yu, Seongdo Jeong, Hansong Lee, Hye Jin Heo, Jeong Jun Park, Hee Sam Na, Dai Sik Ko and Yun Hak Kim in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Not applicable
Author note
Jeong Jun Park is now affiliated with Department of Anesthesiology and Pain Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Republic of Korea.
Author contribution
JK and YY conceived the study and take responsibility for the integrity of the data and accuracy of the data analysis. HL and SJ did the literature research, performed study selection, data extraction, and synthesis. HJH and JJP participated in the analysis and interpretation of the data. HSN wrote the draft review paper. DSK and YHK revised the manuscript critically for important intellectual content and redrafted some of its sections. All the authors read and approved the final version of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Basic Science Research Program (NRF-2020R1C1C1003741), Collaborative Genome Program for Fostering New Post-Genome Industry (NRF-2017M3C9A6047610), and Medical Research Center (NRF-2018R1A5A2023879) through the National Research Foundation of Korea grant funded by the Korean government.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.