
Abstract
Hepatocellular carcinoma (HCC) remains a major cause of cancer-related mortality worldwide. Delayed diagnosis is a major factor responsible for the poor prognosis of HCC. Several advances have been made in the field of liver imaging with the use of novel imaging contrasts, improving current imaging techniques with contrast-enhanced computed tomography (CT) and magnetic resonance imaging (MRI), introduction of new technologies such as contrast liver ultrasound, and development of novel biomarkers with the goal of early detection of HCC and improving outcomes of patients with HCC. This review focuses on current surveillance strategies and development of biomarkers with the goal of early detection of HCC.
Introduction
Hepatocellular carcinoma (HCC) is the fifth most common cancer worldwide and the second most common cause of cancer-related mortality according to the World Health Organization. 1 The annual incidence rates vary depending on the geographic location with Eastern Asia and Sub-Saharan Africa having the highest incidence of HCC. 1 Hepatitis B vaccination remains the best intervention to reduce the incidence of HCC in places where hepatitis B virus (HBV) is highly prevalent as demonstrated in Taiwan. 2 In the United States, the incidence of HCC has been rising and is expected to peak in 2030 with the highest increase in Hispanics, followed by Blacks and then Whites, and a decrease in Asian Americans according to a recent analysis of the Surveillance Epidemiology End Results (SEER). 3 Surgical intervention by resection or liver transplantation are the only curative options; however, only 10–23% of patients are surgical candidates at the time of presentation.4–7 Unfortunately, most patients present with advanced HCC and face a 1-year survival of 15–39% with limited treatment options.8,9
In this review we highlight novel biomarkers and imaging tests that are being investigated to improve surveillance and early diagnosis of HCC. Ultimately, early diagnosis will provide more treatment options and lead to improved survival for patients with HCC.
Surveillance for HCC
The poor prognosis of HCC is largely related to late diagnosis. Historically, serum alpha-fetoprotein (AFP) and diagnostic imaging with computed tomography (CT) or magnetic resonance imaging (MRI) have been primary diagnostic modalities. However, the poor prognosis due to late diagnosis of HCC has proven unacceptable and, recently, significant efforts have been devoted to identifying patients with early stage HCC.
Presence of cirrhosis, chronic hepatitis B, and prior history of HCC are some of the factors involved in the decision to enter a patient into a surveillance program for HCC (Table 1). 10 All major societies including the American Association for the Study of Liver Diseases (AASLD), the European Association for the Study of the Liver (EASL), and the Asian-Pacific Association for the Study of the Liver (APASL) agree on the importance of liver cancer surveillance with abdominal imaging every 6 months. For example, The AASLD recommends HCC surveillance with a liver ultrasound with or without serum AFP every 6 months. 10 However, patients with Child’s class C cirrhosis are not recommended to enter a surveillance program unless they are listed for liver transplantation given their low expected survival without transplantation.
Populations with HCC screening benefit. Modified from Marrero et al. 10

HCC, hepatocellular carcinoma; PBC, primary biliary cholangitis.
A large meta-analysis showed HCC surveillance can lead to detection of HCC at an earlier stage resulting in improved survival [pooled odds ratio (OR) 1.9, 95% confidence interval (CI) 1.67–2.17]. 11 The study also showed that patients who underwent HCC surveillance were more likely to have HCC detected at an earlier stage using Milan or Barcelona Clinic Liver Cancer (BCLC) criteria (OR 2.08, 95% CI 1.88–2.33). 11 Furthermore, patients diagnosed with HCC by surveillance were more likely to undergo curative treatment than those who presented symptomatically or were diagnosed incidentally (OR 2.24, 95% CI 1.99–2.52). 11 The pooled rate of receiving curative treatment among patients undergoing surveillance was 51.6% (95% CI 50.2–53%) and 23.7% (CI 22.8–24.7%) in patients who presented symptomatically or were diagnosed incidentally.
Despite the benefits of HCC surveillance, it is not often implemented. Entering into HCC surveillance program requires awareness of disease stage or cirrhosis and the screening guidelines, ordering appropriate screening imaging studies as well as patient adherence of screening studies and frequencies. Goldberg et al. highlighted the number of specialist visits by gastroenterology or infectious diseases in the first year after cirrhosis diagnosis being the strongest predictors for HCC surveillance. 12 In addition, ultrasounds ordered more than 3 months in advance were less likely to be done. In fact, ultrasounds ordered more than 180 days from the due date were associated with 23% decreased odds of being performed. 12 Primary care provider knowledge level about the liver cancer and awareness of effective HCC therapies are also predictors for pursuing HCC surveillance according to McGowen et al. 12 Patient’s understanding also plays an important role in screening for HCC. Farvadin et al. constructed a survey questionnaire for patients at high risk for HCC. 13 The survey revealed that 48.6% of patients did not believe they need to undergo HCC surveillance if they eat a healthy diet and 34% of the patients surveyed believed they did not need to undergo HCC screening if they had a normal physical examination or absence of symptoms. 13
Imaging
Ultrasound
Ultrasound has many advantages. It is widely available, inexpensive, almost risk free, and accepted by most patients compared with contrast imaging. It has a wide historical sensitivity of 40–80% with a specificity of 82–100%.14–17 A recent meta-analysis revealed a poor ultrasound sensitivity of 47% (95% CI 33–61%) at detecting early HCC. 17 However, the results of a traditional grayscale abdominal ultrasound are highly dependent on the expertise of its operator. In addition, obese patients pose a challenge to the ultrasound as the resolution of the images are highly affected by the presence of liver steatosis and subcutaneous fat. It is also important to note that a coarse liver echotexture can also make underlying liver lesions difficult to visualize. The size of the liver lesion also affects the sensitivity of the ultrasound (Table 2).
Abdominal ultrasound sensitivity according to nodule size. 18

A recent study by Samylova et al. 18 reported that the sensitivity of an abdominal ultrasound in the setting cirrhosis is worse in patients with body mass index (BMI) ⩾ 30 kg/m2 compared with BMI <30 kg/m2 (0.76 versus 0.86, p < 0.01) or in patients with nonalcoholic steatohepatitis (NASH) compared with other etiologies (0.59 versus 0.84, p < 0.02). The authors also investigated whether addition of AFP to ultrasound in this cohort of patients improves the sensitivity of the ultrasound. They concluded that addition of AFP (using a cutoff ⩾ 20 ng/ml) significantly improved the sensitivity from 0.82 to 0.89 in patients with BMI >30 kg/m2. The sensitivity of the combination of the ultrasound with AFP ⩾ 20 ng/ml in patients with NASH remained lower than in patients without NASH (0.72 versus 0.91, p < 0.008). The addition of AFP to ultrasound had no significant effect on the sensitivity in patients with BMI ⩾ 30 kg/m2 compared with patients with BMI <30 kg/m2 (0.89 versus 0.90, p = 0.98). Furthermore, ultrasound missed up to 41% of HCC lesions in patients with NASH and up to 10% in patients with BMI ⩾ 30 kg/m2. 18 Based on these findings, the authors suggested the use of cross-sectional imaging for obese patients or those with NASH. However, cross-sectional imaging is not without risks. While providing clearer images, deeper tissue penetration, and improved diagnostic accuracy for HCC, it carries the risk of radiation exposure and nephrotoxicity. The conclusion of the authors is in line with the recommendations of the ultrasound liver imaging reporting and data system (US LI-RADS) for screening and surveillance of HCC. 19
The US LI-RADS emphasizes the importance of reporting on the quality of the ultrasound in every ultrasound report. In brief, the US LI-RADS advocates the presence of a detection score and a visualization score on every ultrasound report. The detection score consists of three categories: US-1 negative, US-2 subthreshold, and US-3 positive. The visualization score refers to the expected sensitivity of the performed ultrasound and consists of three categories: visualization A (no or minimal limitations), visualization B (moderate limitations), and visualization C (severe limitations). Visualization A refers to studies where the limitations are not expected to affect the sensitivity in the detection of underlying masses. Visualization B refers to situations where limitations may mildly decrease the sensitivity for detection of small masses as in the presence of intermediate heterogeneity of the liver or in situations where a small portion of the liver is not well seen. Visualization C is defined as a study with limitations that result in significant lowering of the sensitivity of the ultrasound. Such situations include the presence of marked heterogeneity of the liver parenchyma and absence of visualization of the majority of the diaphragm (50%) or greater than 50% of the liver. 19 Such reporting can improve communication with patients, referring physicians and radiologists as well as improving patient care.
Contrast-enhanced CT and MRI
Unlike other malignancies, HCC can be diagnosed based on imaging characteristics on multiphasic CT and MRI. HCC is characterized by arterial enhancing phase followed by a washout phase on portal venous/delayed phase. Introduction of hepatobiliary contrast agents [gadobenate dimeglumine (Gd-BOPTA, Multihance, Bracco, Milan, Italy) and gadoxetate dimeglumine (Gd-EOB-DTPA, Primovist in Europe and Eovist in the United States, Bayer Healthcare] has improved detection of HCC. While only 5% of the injected Gd-BOPTA is excreted into the biliary system, approximately 50% of the Gd-EOB-DPTA undergoes biliary excretion improving the sensitivity of HCC detection by 5–15% with Gd-EOB-DPTA. 20 MRI has a higher sensitivity than CT in diagnosing HCC, but the sensitivity varies according to the size of the liver nodule (Table 3). Overall, MRI has a sensitivity of 77–100% for detecting nodular HCC while CT has a sensitivity of 68–91%. 21 However, the sensitivity is only 45–80% with MRI and 40–75% with CT for lesions measuring 1–2 cm and it is close to 100% for lesions larger than 2 cm. 21 CT and MRI are not indicated as surveillance tests for HCC owing to their higher cost when compared with ultrasound. They also carry the risk of developing toxicity such as hypersensitivity reaction, nephrogenic systemic fibrosis in patients with advanced renal disease receiving gadolinium-based contrast agents, concern about accumulation of gadolinium in the brain, and iodine-induced nephrotoxicity from the intravenous contrast agents. 20 In addition, CT is also associated with radiation exposure. Newly abbreviated protocols have been proposed to maximize the benefits of the cross-sectional MRI with limiting contrast exposure.22,23 Such shortened protocols involve T1-weighted imaging from the hepatobiliary phase after gadoxetate disodium infusion and T2-weighted imaging and diffusion-weighted imaging. These abbreviated contrast MRI protocols have the potential to shorten MRI imaging times which could reduce costs and increase patient comfort.
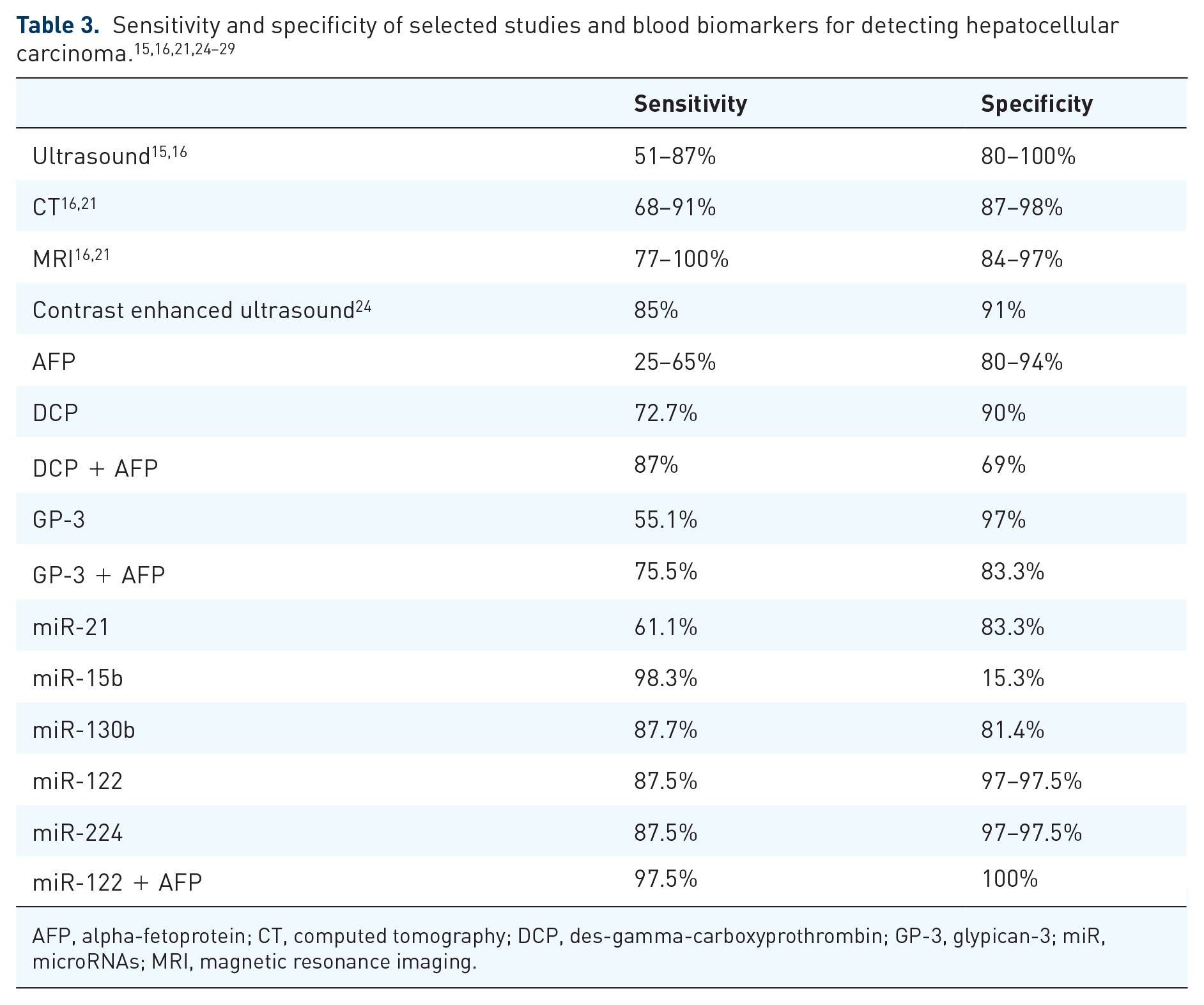
AFP, alpha-fetoprotein; CT, computed tomography; DCP, des-gamma-carboxyprothrombin; GP-3, glypican-3; miR, microRNAs; MRI, magnetic resonance imaging.
Contrast-enhanced ultrasound
Contrast-enhanced ultrasound (CEUS) is an imaging modality that is superior to the grayscale ultrasound in terms of offering real-time visualization of contrast-enhanced images in the arterial, portal-venous, and late phase. CEUS can be used to better characterize liver lesions identified on ultrasound, CT, or MRI but is not an appropriate imaging modality for HCC surveillance. The advantage of CEUS includes the ability to visualize the arterial and venous phases in real time through the use of micro bubbles. Micro bubble injections can be performed as many times as needed to obtain adequate imaging of a target lesion since the agent is nontoxic and is excreted through the lungs. The sensitivity and specificity of CEUS for HCC larger than 2 cm in diameter is also comparable with MRI and CT. 20 A recent meta-analysis showed the pooled sensitivity and specificity of CEUS for the diagnosis of HCC as 0.85 (95% CI 0.84–0.86) and 0.91 (95% CI 0.90–0.92), respectively. 24 CEUS has advantages over CT and MRI in being portable, radiation free, and does not rely on a potentially nephrotoxic contrast agent.30–32 However, it has limited penetration of the liver parenchyma that can lead to missing deep liver lesions. It can overlook lesions in the subdiaphragmatic areas and mistake the falciform ligament and surrounding fat for lesions. CEUS can also give false positive results with scars, fibrosis, sarcoidosis, inflammatory pseudotumors, and necrosis. 33
(18F)fluoro-2-deoxy-D-galactose positron emission tomography/computed tomography
Positron emission tomography (PET) with the glucose analogue 2-(8F)fluoro-2-deoxy-D-glucose (FDG) is not widely used in either diagnosis or surveillance for HCC. Its use was first demonstrated in a small study of 39 patients with known or suspected HCC and demonstrated high specificity (100%). 34 In the interim, several small studies have shown the utility FDGal PET in detecting HCC and HCC metastasis.35–37 However, PET has limited value in the diagnosis of HCC since most HCCs are not highly metabolically active. For this reason, PET can miss 30–50% of HCC lesions. 20
Blood based biomarkers
Small molecules, such as proteins and nucleic acids, or tumor cells themselves that can be detected in the blood of patients could be excellent diagnostic biomarkers for HCC. The development of biomarkers is guided by the National Cancer Institute Early Detection Research Network (NCI-EDRN). 38 This program involves five phases of investigation that range from Phase I, identification of potential biomarkers, to Phase V, randomized trials to determine whether biomarkers can lead to early identification and reduction in mortality. This program carries potential biomarkers from bench to bedside and clinical application. However, only AFP have made it through all phases (Table 3). 39
AFP
AFP was first discovered in the serum of patients with HCC in 1964 and has since been the primary diagnostic biomarker for HCC. 40 AFP is primarily a protein of development and is highest during gestation, falling to trace levels after birth.41,42 High serum AFP has been shown to correlate with the presence and progression of HCC and it is used as both a diagnostic and prognostic factor. Despite this, there are multiple problems using AFP as a diagnostic marker, such as elevation in non-HCC diseases, cirrhosis, hepatitis, cholangiocarcinoma, testicular germ cell tumor, and metastatic colon cancer. 43 Furthermore, the sensitivity and specificity of AFP ranges from 25–65% and 80–94%, respectively.44,45 In fact, only about 60–80% of HCC have elevated AFP levels, leaving a large margin for false negatives and missed diagnosis. It is for this reason that AFP alone is not recommended as the main screening test for HCC. Lectin-binding alpha-fetoprotein (AFP-L3) is a subfraction of AFP. It has a high specificity of 99.4% for HCC and a low sensitivity of 18.8%. 46 It has been shown that the levels of AFP and AFP-L3 can be detected in the blood 6 months prior to the diagnosis of HCC. 47 Adding AFP-L3 (cutoff 4%) increased the sensitivity of the ultrasound to 94.3% compared with a sensitivity of 88.6% of ultrasound plus AFP (cutoff >5 ng/ml). While sensitivity increased with the addition of AFP and AFP-L3 to the ultrasound, the specificity decreased from 96.4 to 82.7%. 47 Therefore, investigation of other new biomarkers is desperately needed.
Des-gamma-carboxyprothrombin
The development of proteomics research and high-throughput analyses has led to the identification of multiple proteins that are upregulated in HCC and may provide potential biomarkers. Des-gamma-carboxyprothrombin (DCP), also known as prothrombin induced by vitamin K absence II (PIVKA II), is an abnormal prothrombin molecule which is upregulated in HCC. Malignant transformation of hepatocytes and HCC are associated with alterations in post-translational modifications (PTMs) of proteins. DCP is the result of altered vitamin-K-dependent carboxylation. 48 DCP has been evaluated as a screening biomarker for HCC with mixed results. One benefit of DCP is that it is less likely to be elevated in non-HCC liver diseases than AFP. In a single study comparing patients with HCC with those with cirrhosis and chronic hepatitis, DCP had a sensitivity and specificity of 72.7% and 90.0% for HCC, respectively. 49
DCP and AFP
The combination of DCP and AFP was evaluated for the early diagnosis of HCC in a multicenter case-control study by Lok et al. 50 Results from this study showed the combination yielded an increase in sensitivity to 87% from 65% with AFP alone, but a decrease in specificity from 84% to 69%. For screening purposes, this increase is sensitivity is clearly beneficial and may prompt additional diagnostic studies. A separate case-control study from France compared cirrhotic controls against patients with HCC, of which 32 of 85 patients (38%) had early stage HCC (classified as BCLC stage A). 51 DCP alone showed an area under receiver operating characteristic curve (AUROC) of 0.81, 95% CI 0.70–0.92, and positive predictive value (PPV) of 77% for the diagnosis of HCC. The combination of DCP and AFP was found to have an AUROC of 0.83, 95% CI 0.72–0.93, indicating they may be useful for diagnosis in patients with cirrhosis. In a Chinese study of 120 patients with HCC, DCP alone was inferior to the combination of DCP+AFP by having lower sensitivity (53.3% versus 78.3%) and specificity (85.6% versus 53.3%). 52
Glypican-3
Glypican-3 (GPC3) is another protein which represents a potential biomarker for the diagnosis of HCC. GPC3 is involved in cell proliferation, survival, and tumor suppression. 53 Normally absent in healthy hepatocytes, GPC3 is upregulated in HCC and is thought to participate in canonical Wnt signaling growth pathway.54,55 Similar to AFP, GPC3 is not present in all HCCs but is found in 33% of patients who were seronegative for both DCP and AFP. 56 One study suggested that an acute rise in GPC3 suggests transition from premalignant liver lesion to HCC. 57 Another benefit of GPC3 is its nonexpression in healthy hepatocytes and expression being independent of tumor size. 58 A meta-analysis comparing GPC3 to AFP expression in early tumors (defined as BCLC 0 or A, TNM stage 1) found GPC3 had sensitivity and specificity of 55.1% and 97.0% compared with 34.7% and 87.6% for AFP. 25 In addition, combination of GPC3 and AFP increased sensitivity to 76% for diagnosis of HCC when tumors were <3 cm.
The GALAD model
The GALAD model incorporates AFP, AFP-L3, and DCP into a formula taking account age, sex, and gender of the patient. It is calculated as −10.08 + 1.67 × [gender (1 for male, 0 for female)] + 0.09 × [age] + 0.04 × [AFP-L3] + 2.34 × log[AFP] + 1.33 × log[DCP]. 59 It has been developed to predict the probability of having HCC in patients with chronic liver disease. 59 The GALAD score has been validated in Germany, Japan, UK, and Hong Kong. It has recently been validated in the USA through a retrospective study by Yang et al. 60 When compared with ultrasound as a surveillance test, the GALAD score had a higher area under the curve (AUC) than ultrasound (0.95 versus 0.82; p < 0.01). A GALAD score of −1.18 had a sensitivity of 92%, specificity of 79% and AUC of 0.92 versus 0.82 for an abdominal ultrasound (95% CI 0.88–0.96) for detecting early stage HCC defined as BCLC 0-A). 60 Even for AFP negative tumor, a cutoff of -1.18 was associated with a sensitivity of 89% and specificity of 81%. 60
Biomarkers in development
Multiple proteins are upregulated in HCC and many have been previously identified and reported in the literature as potential biomarkers for diagnosis or early detection of HCC. Overall, the heterogeneity of HCC tumors and multiple different etiologies makes surveillance and diagnosis difficult based on serum protein levels alone. Therefore, identification of other small molecules has been of importance in HCC research.
Similar to the advancements in proteomics, transcriptome analysis has promoted genomics research to identify nucleic acids in serum and tumor tissue which are upregulated in HCC and may serve as both novel biomarkers and therapeutic targets. Perhaps the most notable of these nucleic acids are microRNAs (miRNA). miRNAs are small (17–25 nucleotides), noncoding RNAs that bind complementary sequences in target mRNA to induce degradation. In cancer, miRNAs may function as either tumor suppressor genes or oncogenes. Over 500 miRNA genes have been identified and found to affect multiple transcriptional programs, including proliferation, differentiation, and apoptosis. Xia et al. recently examined three large publicly available datasets, gene expression omnibus (GEO), Oncomine, and The Cancer Genome Atlas (TCGA), to identify 23 differentially expressed genes targeted by 9 miRNAs and 10 long noncoding RNAs (lncRNA) in HCC. 61 These databases contain gene expression data from tissue samples, not serum, making the results difficult to apply as biomarkers. However, these results are an example of the first step of biomarker investigation: identification of possible targets.
Circulating miRNAs in the serum and plasma have been described as targets for biomarker analysis. Circulating miRNAs are a promising biomarkers for HCC as they are relatively stable and are protected from RNase activity in the pathogenesis of HCC.62,63 Patient-level studies have been conducted for the diagnostic potential of serum miRNAs with encouraging findings (Table 3). A study of patients with hepatitis B or C was conducted to examine miR-21 serum expression and found it had 61.1% sensitivity and 83.3% specificity (AUROC = 0.773) in differentiating between patients with HCC and chronic hepatitis. 26 The AUROC was 0.953 for differentiating those with HCC from healthy controls. A separate study evaluated patients from China with HCC, chronic hepatitis B, and healthy controls for the potential use of miR-15b and miR-130b as biomarkers for HCC detection. 64 Analysis of these patients found miR-15b had the highest sensitivity reported (98.3%), however very low specificity (15.3%) while miR-130b had sensitivity and specificity of 87.7% and 81.4%, respectively. Notably, the AUROC for miR-130b was very high (0.913) for detecting HCC amongst those with chronic hepatitis B and healthy controls. Lin et al. proposed and validated a serum miRNA classifier (seven differentially expressed miRNAs: miR-29a, miR-29c, miR-133a, miR-143, miR-145, miR-192, and miR-505) to detect HCC in the training cohort, and two independent validation cohorts. miRNA classifier had higher sensitivity (range 70.4–85.7%) than did AFP of 20 (40.7–69.4%) to detect HCC, whereas its specificity (80.0–91.1%) was similar to that of AFP of 20 (84.9–100%). miRNA classifier had a larger AUC than did AFP to identify small-size (AUC 0·833 [0.782–0.883] versus 0·727 [0.664–0.792], p = 0.0018) and early stage (AUC 0.824 [0.781–0.868] versus 0·754 [0.702–0.806], p = 0.015) HCC and could also detect AFP-negative (AUC 0.825 [0.779–0.871]) HCC. 27
More recently, Amr et al. evaluated the diagnostic potential of miR-122 and miR-224 in HCC and found that both had sensitivity of 87.5% and specificities of 97.0–97.5% for diagnosing early stage HCC (BCLC stage A4) compared with patients with chronic hepatitis. 28 The diagnostic accuracy was 0.98 for miR-122 and 0.93 for miR-224. Compared with controls, accuracy for detecting HCC was 0.96 for miR-122 and 0.94 for miR-224. Most notably, combining either miR-122 with AFP yielded a sensitivity of 97.5%, specificity of 100% and diagnostic accuracy of 1.0, better than any measure alone in this study.
MicroRNA are not the only nucleic acids studied as biomarkers for HCC. LncRNA have also been studied as potential biomarkers. Li et al. examined multiple databases to identify lncRNAs which were upregulated in HCC and then used serum samples from an independent cohort of HCC and control patients to evaluate their utility as biomarkers. 29 Through this study, two lncRNAs were identified as potential biomarkers: HULC and Linc00152, both of which were upregulated in the plasma of patients with HCC. AUROC for diagnosis of HCC were 0.78 and 0.85 for HULC and Linc00152, respectively. Combination of HULC and Linc00152 yielded an AUROC of 0.87 and the addition of AFP increased the AUROC to 0.89.
Despite the increased sensitivity, specificity, and AUROC associated with each of the miRNAs and lncRNAs above, there are multiple limitations to be overcome. Ideal biomarkers must have sufficient sensitivity and specificity, but perhaps more importantly, must be widely available and cost-effective for surveillance. While these small molecules perform well in studies, validation in large cohorts still needs to be performed and standard cutoffs for screening and diagnostic purposes need to be established. Furthermore, detection of these molecules requires real-time or quantitative polymerase chain reaction (PCR) for detection and quantification. The cost for isolation of miRNA, primers for processing and amplification, and testing for quantification is sufficiently high that it may be difficult to apply on a large scale. Standardization of testing through the development of an assay that is widely available and easily processed with little opportunity for human error is paramount for establishing effective screening and diagnostic tests.
Liquid biopsy detects circulating tumor cells (CTCs), methylation status, mutation of specific tumor-related nucleic acids including DNA, RNA, and miRNAs originating from CTCs or being shed into the blood stream directly from living or dying tumor cells. 65 It consists of obtaining samples from different time points over the course of a disease in a minimally invasive manner. Ideally, such liquid biopsy offers the advantages of early detection of cancer, prediction of treatment response, real-time monitoring for disease recurrence, and prediction of resistance to therapy. 66 Circulating tumor DNA (ctDNA) represents tumor-derived fragmented DNA in the bloodstream of cancer patients. Alteration of the ctDNA associated genes such as p15, p16, APC, SPINT2, SFRP1, p16INK4a, TFPI2, GSTP1, and RASSF1A is linked to the development and progression of HCC.66,67 Reverse transcription (RT)-PCR was the first method used to detect CTCs in 1994. Since then, other enrichment techniques such as ISET technology, CanPatrol CATC analysis platform (SurExam, China), CellSearchTM, CTC-Chip, flow cytometry, and CanPatrolTM have been developed for CTC isolation, characterization, prognosis assessment for metastasis, and efficacy of a drug. 66 Many targets have been studied as potential valuable biomarkers for HCC assessment using these techniques. Such tumor-specific molecules include MAGE-1, MAGE-3, hTERT, GPC-3, CD133, CD90, K19, CD44, and PLAC1. However, the biomarkers lack specificity as they were also seen in other forms of malignancies in addition to HCC. 50 In order for liquid biopsy to make it to clinical practice, it needs to overcome major hurdles. It needs to have standardized assay protocols and multicenter validation studies.
Conclusion
Despite the advances in the field of HCC and the availability of surgical resection and liver transplantation as curative measures for early HCC, screening and adherence to surveillance rates for HCC remain poor. Educating the gate keepers, that is, primary care physicians, health care associates, and the population at risk, about HCC is an important factor in increasing the rate of early detection of HCC. Imaging studies, especially abdominal ultrasound, are currently the backbone for screening for HCC. Once a liver lesion is detected by an abdominal ultrasound in a patient at risk for development of HCC, it is followed by contrast imaging for confirmation, adding to the cost of HCC detection. Multiple studies have proven the cost effectiveness of screening for liver cancer with abdominal ultrasound. Combining biomarkers with abdominal ultrasound seems to be the next step in increasing the sensitivity and specificity of the screening test for HCC. However, such biomarkers need to be widely available, affordable, and easily accessible.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Women’s Guild of Cedars-Sinai Medical Center. The funder had no role in decision to publish, or preparation of the manuscript.
Conflict of interest statement
The authors declare that there is no conflict of interest.