
Abstract
The introduction of anti-HER2 therapies to the treatment of patients with HER2-positive breast cancer has led to dramatic improvements in survival in both early and advanced settings. Despite this breakthrough, nearly all patients with metastatic HER2-positive breast cancer eventually progress on anti-HER2 therapy due to de novo or acquired resistance. A better understanding not only of the underlying mechanisms of HER2 therapy resistance but of tumor heterogeneity as well as the host and tumor microenvironment is essential for the development of new strategies to further improve patient outcomes. One strategy has focused on inhibiting the HER2 signaling pathway more effectively with dual-blockade approaches and developing improved anti-HER2 therapies like antibody–drug conjugates, new anti-HER2 antibodies, bispecific antibodies, or novel tyrosine kinase inhibitors that might replace or be used in addition to some of the current anti-HER2 treatments. Combinations of anti-HER2 therapy with other agents like immune checkpoint inhibitors, CDK4/6 inhibitors, and PI3K/AKT/mTOR inhibitors are also being extensively evaluated in clinical trials. These add-on strategies of combining optimized targeted therapies could potentially improve outcomes for patients with HER2-positive breast cancer but may also allow de-escalation of treatment in some patients, potentially sparing some from unnecessary treatments, and their related toxicities and costs.
Keywords
Introduction
A better understanding of tumor biology and HER2 signaling has led to the development and approval of new HER2-targeted agents that, together with the use of continued anti-HER2 therapy beyond progression, have resulted in unpreceded survival outcomes in patients with advanced HER2-positive breast cancer. 1
The addition of trastuzumab to standard therapy dramatically improved prognosis for patients with HER2-positive breast cancer, and became a landmark in the treatment of these patients.2,3 The second anti-HER2 agent that was incorporated into routine practice of advanced HER2-positive disease was lapatinib, an oral tyrosine kinase inhibitor (TKI) that reversibly inhibits HER1 or epidermal growth factor receptor (EGFR) and HER2 kinases. The approval of lapatinib was based on the improvement in progression-free survival (PFS) found in a phase III trial when combined with capecitabine versus capecitabine alone though no improvement in overall survival (OS) was observed. 4 Pertuzumab is a humanized monoclonal antibody that binds to HER2 on extracellular domain II, a different domain than trastuzumab, preventing homo- and heterodimer formations and blocking one of the most powerful heterodimers, HER2/HER3, that activates several intracellular signaling cascades including cell proliferation and survival. The addition of pertuzumab to a taxane and trastuzumab combination compared with taxane and trastuzumab therapy alone as a first-line treatment in advanced HER2-positive breast cancer resulted in an improvement not only in PFS but also in OS by almost 16 months, reaching a median survival of nearly 5 years and establishing this regimen as the preferred regimen in the first-line setting. 1 Finally, trastuzumab emtansine (T-DM1) is an antibody–drug conjugate (ADC) comprised of trastuzumab covalently linked to a maytansine derivate (DM1), a potent antimitotic agent that binds microtubules. 5 After selectively binding to HER2, the conjugate is internalized within endocytic vesicles and degraded in the lysosomes, releasing the active payload within the cell. This results in cell death by mitotic catastrophe. 6 T-DM1 significantly improved both PFS and OS compared with lapatinib plus capecitabine as a second-line treatment 7 and as a later line in patients with advanced HER2-positive breast cancer previously treated with trastuzumab. 8 Based on those results, T-DM1 is currently the only ADC approved to treat breast cancer and the standard second-line therapy for advanced HER2-positive disease. To date, there is no standard of care treatment for patients with advanced HER2-positive tumors following treatment with trastuzumab, pertuzumab and T-DM1. Treatment options at this point include lapatinib plus capecitabine, combinations of trastuzumab with other chemotherapies (such as vinorelbine or gemcitabine), or dual-blockade combinations without chemotherapy, such as trastuzumab with lapatinib or endocrine therapy with either trastuzumab or lapatinib in patients with hormone receptor (HR)-positive disease.
Despite the outstanding improvement in survival with the introduction of anti-HER2 therapies alone or as dual HER2-blockade in the standard treatment of advanced disease, most patients ultimately develop progressive disease and die. Furthermore, up to 40–50% of patients with advanced HER2-positive breast cancer will develop brain metastases during their disease course. Better options for the prevention and treatment of brain metastases are clearly needed. 9 A growing understanding of the underlying mechanisms of primary and acquired resistance to anti-HER2 therapies and compensatory pathways as well as tumor heterogeneity and the tumor microenvironment is essential for the development of novel therapeutic strategies. A substantial number of novel anti-HER2 treatments are being investigated extensively in the preclinical and clinical settings to further improve patient outcomes. Here, we review the rationale and latest evidence of those novel treatments and approaches to overcome resistance in advanced HER2-positive breast cancer.
Mechanisms of resistance and response heterogeneity to anti-HER2 therapy
Many potential resistance mechanisms to anti-HER2 therapy have been described that ultimately lead to reactivation of the HER2 pathway or its downstream signaling, through pathway redundancy or stimulation of alternative survival pathways. 10 Some of these mechanisms include incomplete blockade of the HER2 receptor that activates compensatory mechanisms within the HER family (such as HER3), activation of alternative receptor tyrosine kinases (RTKs) or other membrane receptors outside of the HER family [such as insulin-like growth factor 1 receptor (IGF-1R) 11 and MET 12 ], and alterations in downstream signaling pathways, such as hyperactivation of the PI3K/AKT/mTOR pathway13,14 by reduced levels of tumor suppressor genes (like PTEN and INPP4-B), or by activating mutations in PIK3CA (phosphatidylinositol-4,5 bisphosphate 3-kinase catalytic subunit). 15 Several other biologic features have been associated with response heterogeneity to anti-HER2 therapy, including HER2 mRNA or protein levels, 16 tumor intrinsic subtype, 17 alterations in the HER2-receptor (such as p95HER2), 18 and host and tumor microenvironment components, such as tumor infiltrating lymphocytes (TILs) 19 and FCγR polymorphisms. 20 In the CLEOPATRA trial for instance, high HER2 protein and high HER2 and HER3 mRNA levels were associated with a significantly better outcome (p < 0.05). In contrast, PIK3CA mutation was identified as a strong negative prognostic biomarker, despite deriving benefit from pertuzumab and trastuzumab treatment. 21 In the EMILIA trial, a greater benefit in OS was also observed in patients treated with T-DM1 and high HER2 mRNA expression. 22 Notably, PIK3CA mutations were associated with significantly shorter PFS and OS in patients treated with capecitabine plus lapatinib, but not in T-DM1 treated patients (median PFS 10.9 vs. 9.8 months; OS, not reached in mutant or wild type). 22 Regarding TILs, an increased quantity of stromal TILs was significantly associated with improved OS in patients with advanced HER2-positive breast cancer treated with docetaxel, trastuzumab, and pertuzumab or placebo in the CLEOPATRA trial. 19
It has also been demonstrated that the cyclin D1-CDK4 pathway can mediate resistance to HER2-targeting therapies in vitro and in vivo and that targeting resistant tumor cells with CDK 4/6 inhibitors re-sensitizes them to anti-HER2 therapy and delays tumor recurrence in HER2-driven breast cancers in vivo in patient-derived xenograft tumors. 23 As discussed below, trials are currently underway to evaluate the efficacy of combined HER2 and CDK4/6 inhibition in HER2-positive breast cancer.
Substantial preclinical and clinical studies support the bidirectional cross-talk between HER2 and estrogen receptor (ER) signaling when both receptors are expressed in breast cancer cells. 24 Tumors that express both ER and HER2 are less sensitive to endocrine therapy than ER-positive and HER2-negative tumors, and ER can act as an escape pathway to HER2 inhibition.25,26 Concurrent inhibition of ER together with dual anti-HER2 therapy can improve outcomes, as demonstrated in several trials in early and advanced HER2-positive breast cancer.27–29
The HER2Δ16 splice variant is a major oncogenic driver that promotes trastuzumab resistance. Preclinical data suggest trastuzumab-resistant HER2Δ16 cells are sensitive to the SRC kinase inhibitor dasatinib and data from a phase I/II (GEICAM/2010-04) study suggest there may be a signal for activity when dasatinib is combined with trastuzumab and paclitaxel in the first-line treatment for patients with advanced HER2-positive breast cancer.30,31 In addition, SRC activation by itself has been associated with trastuzumab resistance. 32
The mechanisms that contribute to T-DM1 resistance are not fully understood. There are multiple components to consider when identifying mechanisms of resistance for ADCs, such as the ones related to the antibody, the linker or the payload. Preclinical studies have shown that CDK1/cyclin B1 activity is needed for T-DM1 action. Silencing cyclin B1 induces resistance to T-DM1 while increasing the levels of cyclin B1 in resistant cells partially restores sensitivity. 33 Other potential mechanisms of T-DM1 resistance have been proposed including the reduction of the intracellular DM1 payload due to upregulation of multidrug resistance proteins (e.g. MDR1), 34 impaired lysosomal proteolytic activity 35 or lysosomal transporter loss (e.g. SLC46A3). 34
Interestingly, molecular imaging seems promising not only to further our understanding of tumor heterogeneity in advanced HER2-positive breast cancer but also to identify patients who will unlikely benefit from T-DM1. 36 In the prospective ZEPHIR trial, striking levels of inter- and intrapatient heterogeneity in HER2 expression were observed, with one-third of patients having little or no trastuzumab-zirconium uptake (HER2-Positron emission tomography (PET)/computed tomography (CT) scan [PET/CT scan]) across their metastatic sites. Moreover, the combined use of HER2-PET/CT scan and early fluorodeoxyglucose-PET/CT scan discriminated patients treated with T-DM1 with a median time to treatment failure (TTF) of 2.8 months from those with 15 months of TTF. 36 Despite the extensive translational research being conducted, most of the mechanisms of HER2 resistance and potential biomarkers of response or resistance either have not been clinically validated, or the results are contradictory. 37 To date, no biomarker beyond HER2 exists for patient selection for anti-HER2 therapy in HER2-positive breast cancer. Of note, the interpretation of mechanisms of resistance based solely in preclinical models can be challenging due to tumor heterogeneity, the complex nature of drug resistance and compensatory pathways, and the use of different tumor cell lines. Moreover, multiple mechanisms of resistance may coexist in the same cell.
Novel strategies to overcome resistance to HER2-targeted therapy
Replacement of current anti-HER2 therapies for improved anti-HER2 drugs
ADCs
ADCs are a therapeutic class that provide wider therapeutic window by more efficient and specific drug delivery. ADCs exploit target selectivity of monoclonal antibodies (MAbs) to deliver cytotoxic drugs to antigen-expressing cells to improve tumor selectivity and reduce damage to normal cells. 38 The success observed with the first-in-class T-DM1 has led to a rapid and extensive development of new ADCs. Table 1 lists several anti-HER2 ADCs in clinical development.7,39–41
HER2-directed ADCs in clinical development.
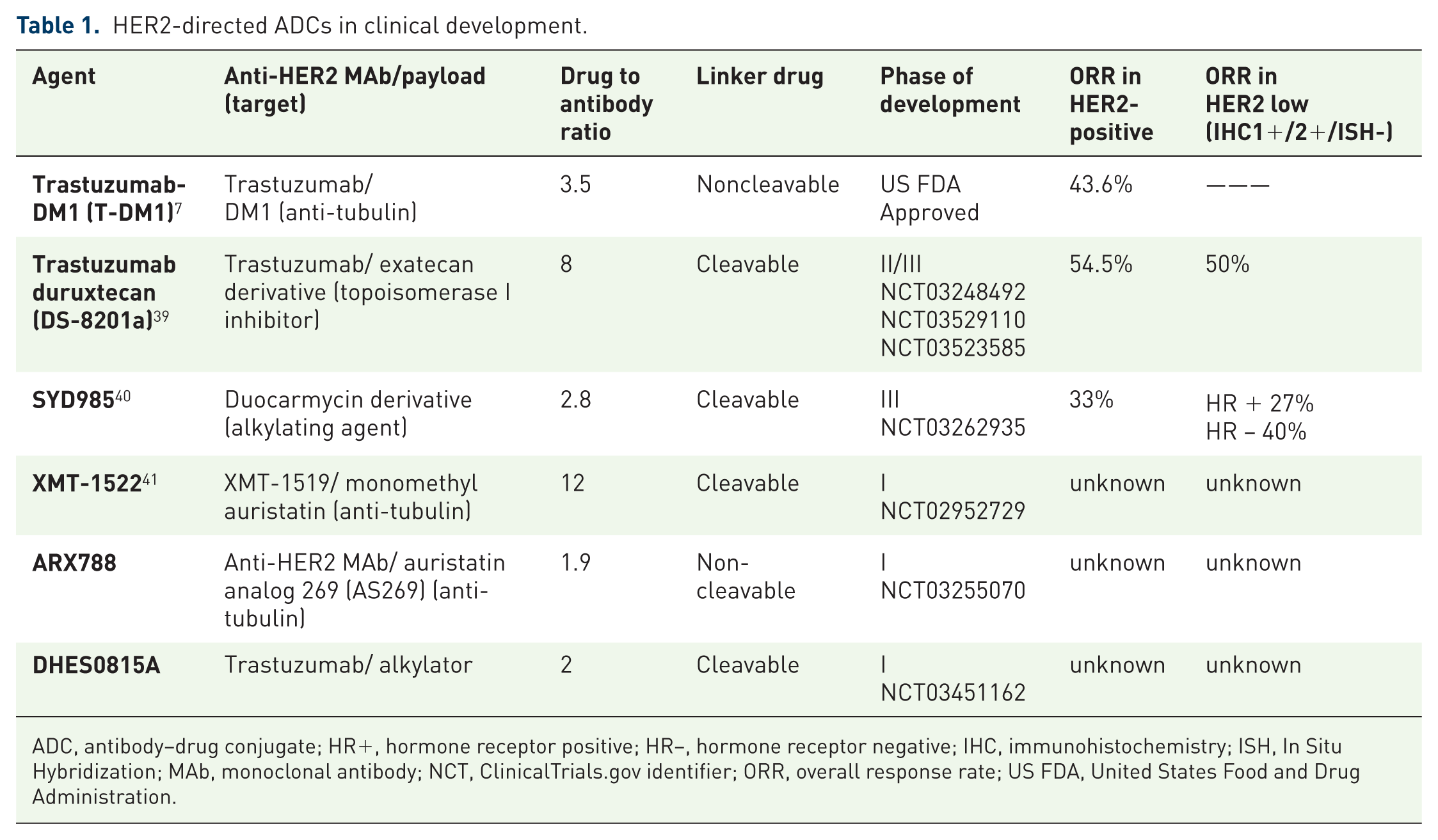
ADC, antibody–drug conjugate; HR+, hormone receptor positive; HR−, hormone receptor negative; IHC, immunohistochemistry; ISH, In Situ Hybridization; MAb, monoclonal antibody; NCT, ClinicalTrials.gov identifier; ORR, overall response rate; US FDA, United States Food and Drug Administration.
ADCT-502 (ADC Therapeutics) is also a novel pyrrolobenzodiazepine (PBD)-based ADC that targets HER2-expressing solid tumors, including breast cancers. 46 However, based on data from the phase I study (ClinicalTrials.gov identifier: NCT03125200) that showed that ADCT-502 did not meet the necessary efficacy and safety profile required for patient benefit, clinical testing of this drug was recently halted.
In preclinical models, another bivalent biparatopic HER2-targeting ADC that targets two nonoverlapping epitopes on HER2 and is conjugated with microtubule inhibitor demonstrated superior activity than T-DM1 in breast cancer models and was able to overcome T-DM1 resistance. This biparatopic ADC also demonstrated bystander killing activity. 47
In contrast with T-DM1, most of these new ADCs have a cleavable drug linker (see Table 1) that mediates the bystander killing effect. This is the passive diffusion of the free cytotoxin from target-positive cancer cells into the tumor microenvironment, killing neighboring cancer cells that are insensitive to the ADC because of the lack or limited target expression. This desired feature of those novel HER2-targeting ADCs, given that heterogeneity is frequent in HER2-positive breast cancer, may be however, a double-edged sword with an increased toxicity.
Novel anti-HER2 antibodies
Margetuximab (MGAH22, MacroGenics) is an Fc-optimized chimeric monoclonal antibody that binds to the same epitope as trastuzumab. Margetuximab has enhanced Fcγ receptor-binding properties with an increased affinity for CD16A polymorphisms and a decreased affinity for FcγRIIB (CD16B), an inhibitory receptor, which allows it to bind more tightly to effector cells and increase antibody-dependent cell-mediated cytotoxicity (ADCC); it also preserves the antiproliferative properties of trastuzumab. 48 A first-in-human phase I study demonstrated promising single-agent activity of margetuximab in heavily pretreated patients with HER2-positive solid tumors. Among 24 patients with metastatic breast cancer, the ORR was 17% and 3 out of the 4 responders remained on treatment for 39–54 months. 49 The most common AEs were grade 1–2 constitutional symptoms and no cardiotoxicity was observed. Margetuximab is currently being evaluated in the randomized phase III SOPHIA trial (ClinicalTrials.gov identifier: NCT02492711) that compares margetuximab plus chemotherapy with trastuzumab plus chemotherapy as a third-line therapy in patients with HER2-positive breast cancer after prior treatment with trastuzumab, pertuzumab, and T-DM1. The US FDA has granted Fast Track designation for the investigation of margetuximab for the treatment of patients with metastatic or locally advanced HER-positive breast cancer previously treated with anti-HER2-targeted therapy.
Bispecific antibodies
Bispecific antibodies (BsAbs) combine the functionality of two MAbs that target two different targets or epitopes, either in the same or in different receptors. BsAbs can interfere with two or more RTK signaling pathways, by inactivating either the RTKs or their ligand. Several are currently being studied in patients with advanced HER2-positive disease.
T-cell bispecific antibodies (TCBs) are engineered molecules that include, within a single entity, binding sites to the invariant CD3 chain of the T-cell receptor (TCR) and to tumor-associated or tumor-specific antigens. Binding to the tumor antigen results in crosslinking of the TCR and subsequent lymphocyte activation and tumor cell killing. However, on-target off-tumor effects caused by redirected lymphocytes can result in severe toxicities. Several are currently in clinical development:
Expression of the tumor-specific antigen p95HER2, a truncated form of HER2, occurs in about 40% of HER2-positive tumors. Rius Ruiz and colleagues have developed a TCB against p95HER2 (p95HER2-TCB) that has a potent anti-tumor effect on breast tumors expressing p95HER2, both in vitro and in vivo. 54 In contrast with HER2, p95HER2 is not expressed in normal tissues, therefore, it has no effect on nontumor cells that do not overexpress HER2. Those findings support further investigation with this compound.
Novel TKIs
TKIs are orally bioavailable small molecules developed to further block the HER receptor family, acting on the intracellular domain. Those HER-directed TKIs have a lower molecular weight compared with MAbs, allowing them a more efficacious penetration through the blood–brain barrier and therefore, theoretically may be more effective for the treatment of HER2 brain metastases. Lapatinib was the first TKI approved in HER2-positive advanced breast cancer (and to date, remains the only one) based on the results described above. Dual blockade with lapatinib plus trastuzumab without chemotherapy also demonstrated benefit in OS in heavily pretreated patients with advanced disease, when compared with lapatinib alone. 55 Initial results with these molecules, however, have not been the ones initially expected, even in the treatment of brain metastases.56,57As a first-line therapy, lapatinib was found to be inferior to trastuzumab when combined with paclitaxel. 58 In the same way, afatinib was found to be not as effective as trastuzumab and less tolerated when each was combined with vinorelbine in a phase III trial (LUX-Breast1 study). 59 No difference was detected between lapatinib-capecitabine and trastuzumab-capecitabine for the incidence of brain metastases in the phase III CEREBEL (EGF111438) study. 56 In the phase II LUX-Breast3 trial, patients with HER2-positive breast cancer and progressive brain metastasis previously treatment with trastuzumab, lapatinib or both, were randomized to afatinib alone, afatinib plus vinorelbine or the investigator’s choice of treatment. Similarly, afatinib-containing regimens not only did not show better activity than investigator-selected treatments but also seemed to be less tolerated. No further development of afatinib for HER2-positive breast cancer is currently planned. There are, however, several novel TKIs in clinical development (Table 2).60–66
HER2-directed TKIs in clinical development.

CBR, clinical benefit rate; CNS, central nervous system; DCR, disease control rate; EGFR, epidermal growth factor receptor; m, months; NA, not applicable; NCT, ClinicalTrials.gov identifier; ORR, overall response rate; PFS, progression-free survival; TKI, tyrosine kinase inhibitor; US FDA, United States Food and Drug Administration; w, weeks.
Combinations of anti-HER2 agents with other drugs
Immunotherapy
Preclinical and clinical data suggest that HER2-positive breast cancer is immunogenic. 71 In contrast with luminal tumors, HER2-positive tumors have a higher mutational burden, and harbor higher numbers of TILs and programmed cell death protein 1 ligand (PD-L1) positivity. 72 In addition, mechanisms of action of anti-HER2 MAbs include not only ADCC but also the generation of adaptive immunity. 73 Together, these data support the rationale of combining anti-HER2 therapies with immune checkpoint blockade (anti-PD-1 or anti-PD-L1 agents). Results from the JAVELIN phase I study, 74 however, were disappointing and no responses were seen with single-agent avelumab in the subgroup of patients with advanced pretreated HER2-positive breast cancer. The first study to evaluate the addition of pembrolizumab to trastuzumab in patients with trastuzumab-resistant HER2-positive breast cancer was the PANACEA (IBCSG 45-13/BIG 4-13/KEYNOTE-014) study. This phase Ib/II study demonstrated that the combination was associated with an ORR of 15.2% and a median of PFS and OS of 2.7 months and 16 months, respectively, in PD-L1 positive patients. 75 However, these data also highlight the limitations of this combination, as no responses were seen in the PD-L1 negative cohort and most of the PD-L1 positive patients who initially responded eventually developed resistant disease. Several randomized studies are ongoing to further evaluate the role of immune checkpoints inhibitors in HER2-positive metastatic breast cancer. Results from the phase II KATE2 trial (ClinicalTrials.gov identifier: NCT02924883) assessing the efficacy and safety of T-DM1 in combination with atezolizumab or placebo in pretreated patients with HER2-positive advanced breast cancer were recently presented. 76 In this trial, the addition of atezolizumab to T-DM1 did not demonstrate a significant PFS benefit in the ITT population (8.2 versus 6.8 months; hazard ratio 0.82; 95% CI 0.55–1.23). However, an exploratory endpoint demonstrated promising PFS in the PD-L1 positive (PD-L1 IHC expression >1%) and stromal TIL subgroups. 76 The phase III NRG-BR004 trial (ClinicalTrials.gov identifier: NCT03199885) is investigating the combination of paclitaxel, trastuzumab, pertuzumab with or without atezolizumab as a first-line treatment. In addition, trastuzumab deruxtecan (DS-8201a) is also being evaluated in combination with nivolumab in a phase Ib study (ClinicalTrials.gov identifier: NCT03523572) in patients with advanced breast (with high and low HER2 expression) and urothelial cancers.
Immunotherapy with HER2-targeting vaccines are also being currently investigated in clinical trials. The HER2 vaccine NeuVaxTM (Nelipepimut-S or E75 peptide combined with granulocyte macrophage-colony stimulating factor) 77 is being evaluated in two phase II clinical trials in combination with trastuzumab in breast cancer patients with HER2–3+ (ClinicalTrials.gov identifier: NCT02297698) and in HER2–1+/2+ (ClinicalTrials.gov identifier: NCT02297698), respectively. ETBX-021 is another HER2-targeting vaccine comprising an Ad5 vector and a modified HER2 gene insert that is being evaluated in a phase I clinical trial with locally advanced or metastatic HER2-low-expressing (IHC 1+/2+) breast cancer.
CDK4/6 inhibitors
There is a strong rationale to evaluate CDK4/6 inhibitors in HER2-positive breast cancer. Activity of CDK4/6 is regulated by several mechanisms that include mitogenic signaling pathways (such as HER2) by increasing CCND1 expression or increasing cyclin D1 protein stability.23,78 In addition, mouse models have shown that cyclin D1/CDK4 plays an important role in the formation and growth of breast tumors driven by ERBB2.23,79,80 Preclinical studies demonstrate a clear synergy between anti-HER2 therapy and CDK4/6 inhibitors,81,82 and that CDK4/6 inhibition can specifically overcome acquired resistance to anti-HER2 therapy. 23 Moreover, CDK4/6 inhibition delayed recurrence of HER2-driven breast cancers in mouse models. 23 Early clinical data also support the use of CDK4/6 inhibitors in HER2-driven breast cancers, especially in the subset of patients with ER-positive, HER2-positive disease.83,84 Currently, there are many clinical trials evaluating the role of CDK4/6 inhibitors in advanced HER2-positive breast cancer, including two global, randomized trials: the MonarcHER study (ClinicalTrials.gov identifier: NCT02675231), which evaluates the role of abemaciclib with trastuzumab in pretreated metastatic disease, and the PATINA study (ClinicalTrials.gov identifier: NCT02947685), which explores the benefits of adding palbociclib to trastuzumab, pertuzumab and an aromatase inhibitor after an induction of standard first-line therapy. Initial reports from the phase II SOLTI-1303 PATRICIA trial (ClinicalTrials.gov identifier: NCT02448420), which evaluates the combination of palbociclib, trastuzumab ± letrozole in heavily pretreated (up to 2–4 prior lines in the metastatic setting) patients with HER2-positive breast cancer, suggest that the combination is active particularly in the luminal subtype by PAM50, with a better PFS compared with nonluminal (12.4 versus 4.1 months, hazard ratio 0.30, 95% CI;0.11–0.86 p = 0.025).85,86 Thus, identification of the nonluminal subtypes by PAM50 might help to identify those patients who might not derive a great benefit from this treatment strategy, regardless of HR status. Other nonrandomized phase Ib/II studies in advanced HER2-positive breast cancer are ongoing, including those combining palbociclib and T-DM1 (ClinicalTrials.gov identifier: NCT01976169); palbociclib, trastuzumab, pertuzumab and anastrozole (ClinicalTrials.gov identifier: NCT03304080); ribociclib with trastuzumab or T-DM1 (ClinicalTrials.gov identifier: NCT02657343); and palbociclib with tucatinib and letrozole (ClinicalTrials.gov identifier: NCT03054363). The JPBO trial (ClinicalTrials.gov identifier: NCT02308020) is testing abemaciclib as a single agent in patients with brain metastasis secondary to HR-positive breast cancer, non-small cell lung cancer, or melanoma, including a cohort of patients with HR+, HER2-positive breast cancer. However, within the cohort of HR-positive, HER2-positive patients, there were no objective responses seen at the time of the interim analysis, and the cohort was not able to move to the second stage. 87
PI3K/Akt/mTOR inhibitors
As mentioned previously, dysregulations in the PI3K/AKT/mTOR pathway seem to play an important role in trastuzumab resistance. PI3K inhibition results in an enhanced HER2 signaling in HER2-overexpressing breast cancer, especially in an increased expression of HER2 and HER3. 88 Targeting both pathways could prevent the development of resistance. However, results of two phase III trials evaluating the role of everolimus, an mTOR inhibitor, in combination with either trastuzumab plus paclitaxel as first-line treatment (BOLERO-1) 89 or in combination with trastuzumab plus vinorelbine in trastuzumab-resistant (BOLERO-3) 90 advanced HER2-positive breast cancer were quite disappointing with a significant increase in toxicity. Although in the PFS subgroup analysis of both studies, the benefit of adding everolimus to the standard therapy seemed greater in patients who had HR-negative disease.89,90 Moreover, the combined biomarker analyses of the BOLERO-1 and BOLERO-3 trials demonstrate an improved PFS in patients harboring PIK3CA mutations or PTEN loss when treated with everolimus. 91 Current efforts have focused on evaluating α-specific PI3K inhibitors, the isoform encoded by the PIK3CA gene, such as alpelisib (BYL719) in combination with anti-HER2 therapies. Alpelisib was combined with LJM716 (a HER3 inhibitor) and trastuzumab in patients with HER2-positive advanced breast cancer with a PIK3CA mutation and prior pertuzumab and T-DM1 (ClinicalTrials.gov identifier: NCT02167854). Preliminary results of this combination showed a high toxicity profile including diarrhea, hyperglycemia, hypokalemia, mucositis and transaminitis, and limited activity (best response was stable disease (SD) in five of six evaluable patients). 92 A phase I study of alpelisib and T-DM1 in heavily pretreated HER2-positive patients showed significant activity, with an ORR of 43% and median PFS of 8.1 months (95% CI 3.9–10.8). Furthermore, activity was observed in T-DM1-resistant patients with an ORR and clinical benefit rate of 30% and 60%, respectively, and median PFS of 6.3 months (95% CI 1.6–10.5). The dose-limiting toxicity (DLT) was a maculopapular rash. Most frequently reported toxicities included fatigue, rash, gastrointestinal side effects, thrombocytopenia, anemia, elevated liver enzymes, and hyperglycemia. 93 Taselisib (GDC-0032), a β-sparing PI3K inhibitor, is being evaluated in an ongoing phase Ib dose-escalation trial in combination with different anti-HER2 therapies in patients with advanced HER2-positive breast cancer (ClinicalTrials.gov identifier: NCT02390427). Copanlisib is a pan-class I PI3K inhibitor with particular activity against PI3Kα that is being evaluated in combination with trastuzumab. Results from a phase Ib (ClinicalTrials.gov identifier: NCT02705859; PantHER trial) in pretreated metastatic HER2-positive breast cancer (with a median of four prior lines) showed no DLTs but grade 3 hypertension was reported in 33% (n = 4) of patients. The best response was stable disease in 9/12 patients and 6 patients continued treatment ⩾16 weeks. The PIK3CA mutation was present in 6/12 (50%) of tumors. 94 MEN1611 is a potent, selective, orally available class I PI3k inhibitor showing high activity against p110α mutant isoforms, and minimal inhibition of the δ isoform that is going to be evaluated in a phase Ib study in combination with trastuzumab with or without fulvestrant (B-PRECISE-01 study). The study will enroll patients with PIK3CA-mutated, HER2-positive, advanced breast cancer pretreated with anti-HER2 based therapy.
Conclusion
Although the use of anti-HER2-targeted therapy has dramatically changed the outlook for patients with advanced HER2-positive breast cancer, almost all patients ultimately experience disease progression. Most of them advance to the point where no approved HER2-targeting treatment controls their disease. This might change in the near future as many promising anti-HER2 therapies are being developed in this setting. The newer HER2 ADCs such as DS-8201a and SYD985 may replace T-DM1 in the second-line treatment space or may be utilized in the third-line and beyond setting after progression on T-DM1. Moreover, these newer ADCs, as opposed to T-DM1, are active not only in patients with HER2-positive breast cancer but also in patients with HER2 low-expressing tumors (IHC1+ or 2+/FISH) in whom to date, there are no current anti-HER2 therapies specifically indicated. This desired feature of its bystander effect may be particularly useful in heterogeneous cancer cell populations among HER2-positive disease. On the other hand, the new TKIs, such as neratinib or tucatinib, are being explored with capecitabine and may demonstrate activity in the third-line setting, though may be associated with increased toxicity relative to trastuzumab. And finally, margetuximab plus chemotherapy is being compared with trastuzumab plus chemotherapy also in the third-line setting in a registrational study.
These strategies of combining optimized HER2-targeted therapies could potentially improve outcomes for HER2-positive breast cancer patients but may also allow de-escalation of treatment in selected patients, potentially sparing some from unnecessary treatments and their related toxicities. Hence, potential biomarkers of response or resistance such as intrinsic subtypes, might be helpful to better select patients for these strategies. Moreover, specific strategies for HR-positive, HER2-positive breast cancer are needed, such as the current studies exploring the use of CDK 4/6 inhibitors in the first and later line setting with anti-HER2 therapy and specific trials allowing patients with progressive brain metastases (who are generally excluded from clinical trials) should be enhanced. The underlying mechanisms of resistance to anti-HER2 therapies and compensatory pathways are indeed complex and a wide range of mechanisms of resistance may coexist in the same cell. Therefore, combining clinical strategies and strengthening international collaborations in the translational setting might be needed to validate predictive biomarkers beyond HER2, which will help us to better select patients and improve their outcomes.
Footnotes
Acknowledgements
We thank Kaitlyn T. Bifolck, BA, for her editorial support. Fundación AECC (Asociación Española Contra el Cáncer) and the Spanish Society of Medical Oncology (SEOM) grants (to S. Pernas)
Funding
This manuscript did not receive specific funding.
Conflict of interest statement
S. Pernas has received honoraria for talks and travel grants from Roche, outside of the submitted work and has served on advisory boards for Polyphor. S. Tolaney receives institutional research funding from Eli Lilly, Pfizer, Novartis, Exelixis, Eisai, Merck, Bristol Meyers Squibb, AstraZeneca, Nektar, Nanostring, Cyclacel, and Immunomedics. S. Tolaney has served on advisory boards or as a consultant for Eli Lilly, Pfizer, Novartis, Eisai, Merck, AstraZeneca, Nektar, Nanostring, Immunomedics, and Puma.