
Abstract
Background:
Cold-atmospheric plasma (CAP) is an ionized gas produced at an atmospheric pressure. The aim of this systematic review is to map the use of CAP in oncology and the implemented methodologies (cell targets, physical parameters, direct or indirect therapies).
Methods:
PubMed, the International Clinical Trials Registry Platform and Google Scholar were explored until 31 December 2017 for studies regarding the use of plasma treatment in oncology (in vitro, in vivo, clinical trials).
Results:
190 original articles were included. Plasma jets are the most-used production systems (72.1%). Helium alone was the most-used gas (35.8%), followed by air (26.3%) and argon (22.1%). Studies were mostly in vitro (94.7%) and concerned direct plasma treatments (84.2%). The most targeted cancer cell lines are human cell lines (87.4%), in particular, in brain cancer (16.3%).
Conclusions:
This study highlights the multiplicity of means of production and clinical applications of the CAP in oncology. While some devices may be used directly at the bedside, others open the way for the development of new pharmaceutical products that could be generated at an industrial scale. However, its clinical use strongly needs the development of standardized reliable protocols, to determine the more efficient type of plasma for each type of cancer, and its combination with conventional treatments.
Introduction
Plasma is described as the fourth fundamental state of the matter. There are various biomedical applications of nonthermal plasma, such as sterilization.1,2 However, its production at an atmospheric pressure (cold atmospheric plasma, CAP) made possible its use for other medical applications (wound healing, blood coagulation, antibacterial treatment, endothelial cell proliferation and more) and while some devices are already used clinically, 3 others are still on the benchside. Two predominant types of plasma discharge devices can be distinguished: direct or indirect discharge sources.2,4–6 Direct plasma discharge sources [e.g. dielectric barrier discharge (DBD)] use the target area as a counter electrode. These direct plasma sources create relatively homogenous plasmas containing high concentrations of plasma-generated species. Although the control of the plasma composition still remains a big challenge, these direct discharge sources are able to control the plasma composition more easily compared with other discharge devices. 4 The major disadvantage of this technique is the application distance (between the electrodes) which must remain within a close range, generally less than 3 mm2, thus limiting its use for small areas of the human body. 4 Indirect discharge sources (e.g. plasma jet) refer to various discharge systems used in plasma science. Hence numerous configurations are found. It generally refers to a system where the carrier gas discharge is operated in a non-sealed electrode arrangement. 7 Plasma jets can be classified according to parameters such as discharge geometry, electrode arrangement, excitation frequency or pattern. More information may be found in the work by Winter and colleagues. 7 The concentration in reactive oxygen and nitrogen species (RONS) is lower than in direct discharge sources and the plasma generated is less controllable. 4 However, the use of some specific carrier gases makes it possible to obtain changes in plasma composition. 4
Two methods of applying plasma are also described: direct treatment and indirect treatment using plasma-activated media or solution (PAM). 5 The first method consists of applying directly the CAP on in vitro cells, in vivo models or human living tissues. The second strategy consists of producing PAM and then applying/injecting it into cell cultures or tumors. More information can be found in the work by Yan and colleagues. 5
In vitro plasma-exposed eukaryotic cells demonstrate several effects such as cell detachment, cell migration alteration, apoptosis or necrosis according to cell type and exposure parameters (power, time of exposure). 2 Similar effects have been observed with cancer cell lines, including apoptosis 8 and decreased cell migration.9,10 Studies even suggest that cancer cells are more sensitive to CAP treatment than normal cells, concluding a selective decrease in cancer cell viability with less cytotoxic effect on nonmalignant cells.11–15 The understanding of the mechanisms responsible for this selectivity is based on several hypotheses that they depend on the basal intracellular level in reactive oxygen species (ROS), the expression of aquaporins, or more recently, on the cholesterol composition of the membrane.16,17
CAP induces both physical effects (production of ultraviolet rays, heat and electromagnetic fields) as well as chemical effects (production of RONS). Whereas the physical effects seem to have a negligible cellular impact,18,19 RONS may induce cell membrane alterations, an increase in intracellular ROS, a decrease of the antioxidant potential and DNA double-strand brakes, and subsequently, apoptosis. 5 For example, singlet oxygen resulting from the application of direct application of CAP or PAM is able to stimulate the production by tumor cells of secondary singlet oxygen. These secondary species induce a decrease in activity of catalase, SOD (superoxide dismutase), nicotinamide adenine dinucleotide phosphate oxidase or the first apoptosis signal receptor and secondarily, a greater sensitivity to RONS. Cytotoxic T cells may also be stimulated. More details may be found in the work by Bauer and colleagues.20,21
To summarize, at present, many basic cellular responses (apoptosis, growth inhibition, selective cancer cell death, cell cycle arrest, DNA and mitochondrial damage, selective increase of ROS, or even immunogenic cell death) have been demonstrated following CAP treatment. 22 Recently, Keidar and colleagues, 22 taking into account these cellular responses, devised a self-adaptive plasma discharge system. Some cellular responses following the treatment could be measured and taken into account to automatically adapt some CAP parameters, such as composition or power, to obtain the most efficient treatment possible.
We are keen to provide an overview of this constantly evolving and promising field of plasma use in oncology. The aim of this systematic review is to map the use of plasma in oncology and the different methodologies implemented so far (cell targets, physical parameters, direct or indirect therapies).
Materials and methods
This systematic review was performed in accordance with the preferred reporting items for systematic reviews and meta-analyses guidelines. 23
Data sources and research strategy
Two major electronic databases were searched: PubMed and Google Scholar. Clinical trials were also identified through the International Clinical Trials Registry Platform search portal (available at http://apps.who.int/trialsearch/).
The research strategy (Table S1) combines both keywords related to plasma (e.g. ‘plasma discharge’ or ‘atmospheric plasma’) and keywords related to medical fields (e.g. tumor, oncology).
This strategy was then slightly adapted to meet requirements of each database. Reference lists of query studies were inspected to identify any additional relevant published or unpublished data. The last research was conducted on 18 January 2018. All citations published after the 31 December 2017 were not considered.
Inclusion criteria
All original reports regarding the use of plasma as a treatment therapy in oncology were included in this systematic review. In vitro, in vivo studies, and clinical trials were considered. Language of publication was restricted to English.
Outcomes
The following outcomes were considered: the countries of authors’ affiliations (each author’s nationality was recorded, a study could be related to several countries), the type of methodology (in vivo, in vitro, clinical trial), the type of plasma discharge device used (DBD or plasma jet), the gas used to produce the plasma (helium, air, argon, azote, with/without adjuvant), the application protocol (direct or indirect treatment) and when applicable, and type of tumor cells (type of cancer or origin of the tumor cell line).
Study selection and data extraction
All results were screened based on titles and abstracts. Full texts of the potentially selected records were obtained for definitive inclusion. Reviews and conference proceedings were not excluded but were considered apart. A standardized extraction form was created to collect data according to the outcomes detailed above (Table S2). Data extraction was performed twice by one author (AD) at a 1-month interval.
Results
A total of 3731 results were identified, corresponding to 3697 unique citations. Based on the inclusion criteria described above, 3468 unique citations were excluded, of which there was one study in Chinese, one in Korean, one in German and one in French6,24–26 A final total of 229 results were included: 190 original articles (82.9%), 30 reviews (13.1%), 7 conference proceedings and 2 ongoing clinical trials. A flow diagram is available (Figure S1). Details for each study are presented in Table S2.
From 2005, the number of original articles has grown exponentially [Figure 1(a)] while the proportion of reviews is variable from year to year [Figure 1(b)]. The world map [Figure 1(c)] reveals that the USA and South Korea, respectively, published 32.3% and 24.0% of the citations.
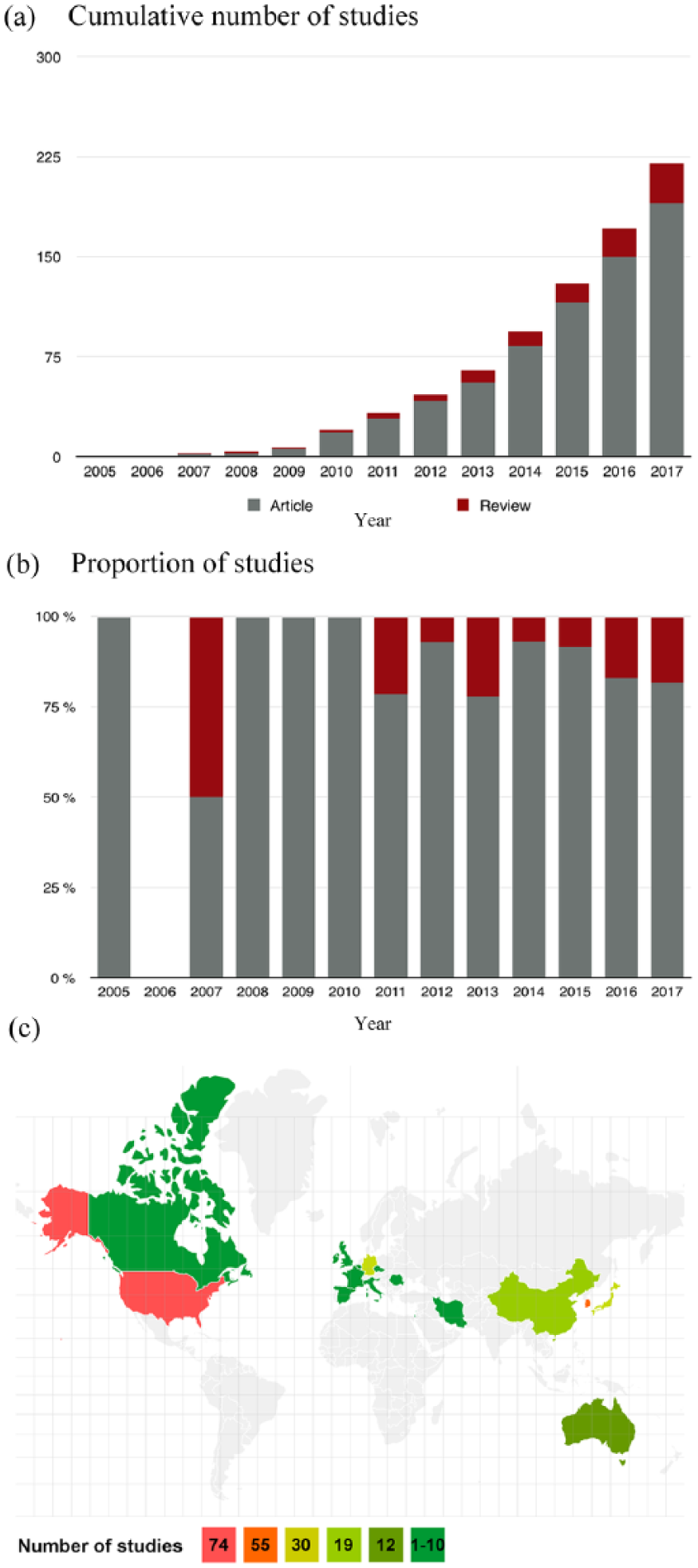
Geographical distribution and type of the included studies.
Plasma production
Two methods of plasma production were found (Figure 2), although the majority of studies used the plasma jet rather than the DBD (72.1% and 27.8%, respectively). One study did not specify the type of plasma production. 27 Helium alone was the most-used carrier gas (35.8%), followed by air (26.3%) and argon (22.1%) (Table 1).
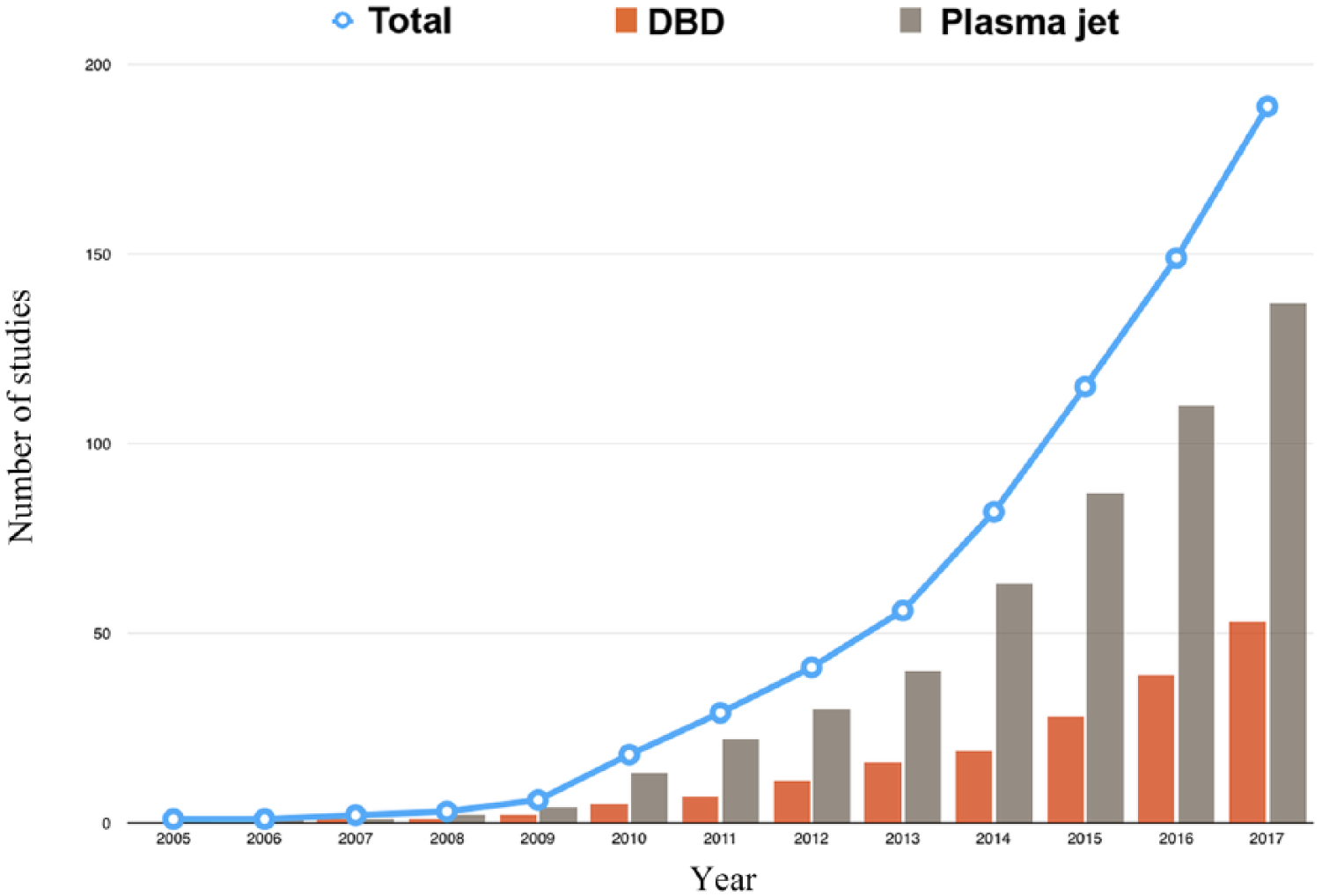
Evolution of the number of studies dealing with dielectric barrier discharge or plasma jet over time.
Gas used in nonreview articles (n = 190).

Studies could be considered in several categories.
Three studies did not specify the gas used to produce the plasma.27–29 The use of argon seems to be on the rise since 2015, while the use of helium remains stable since 2014 (Figure 3).

Yearly distribution of the articles according to the type of carrier gas.
Plasma application
Figure S2 reveals that most of the studies were conducted in vitro (180, 94.7%). The proportion of studies with in vivo results remained low (27, 14.2%). Few clinical trials (3, 1.6%) have been found3,30,31 and two more clinical trials are ongoing.32,33 Figure S3 highlights the predominant use of direct plasma treatments (160, 84.2%) rather than indirect treatments (49, 25.7%). However, in recent years, the number of studies using an indirect plasma treatment has increased, importantly (Figure S3).
Type of neoplasms
The various cancers studied are presented in Table 2. The most commonly reported human cancers (166, 87.4% of total studies) were brain cancer (31, 16.3%), followed by lung cancer (23, 12.1%) and blood cancer (23, 12.1%). Murine cancer cell lines are less studied (29, 15.3% of total studies) and are represented mainly by melanomas (17, 9.0%).
Cancer and tumor cell lines studied in nonreview articles (n = 190).
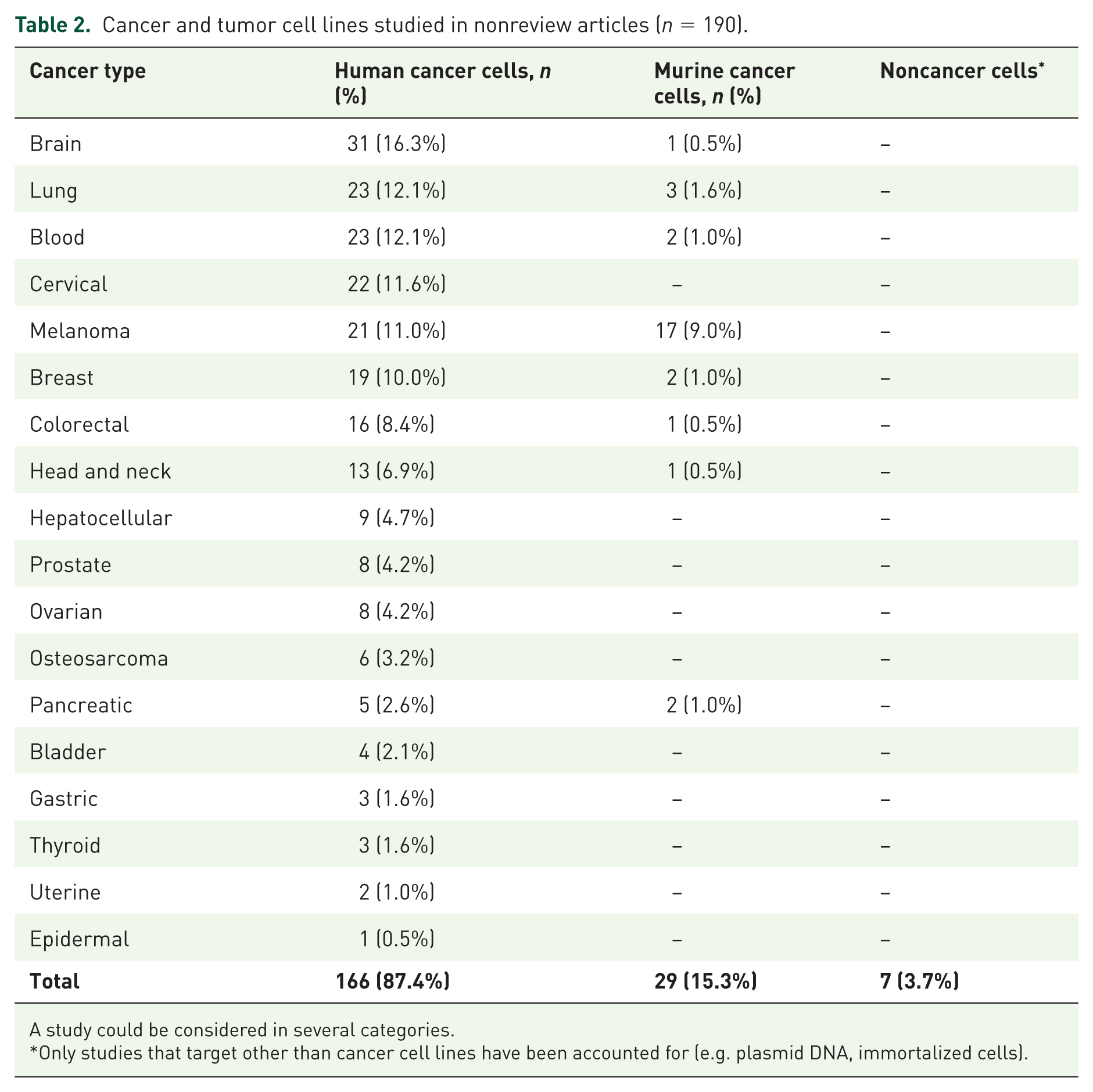
A study could be considered in several categories.
Only studies that target other than cancer cell lines have been accounted for (e.g. plasmid DNA, immortalized cells).
The temporal analysis of the type of cancers derived from either human or murine cell lines are presented in Figure 4(a) and 4(b), respectively. The murine cancer cell line (29, 15.3% of the total studies) is derived mainly from melanoma, and its use significantly increased from 2009. Between 2011 and 2015, six other murine cancer cell lines began to be used. Before 2008, only cells from breast, melanoma and hepatocellular cancers were found in human cell line studies. The year 2009 marked the beginning of the use of a wide range of cancer cell lines.
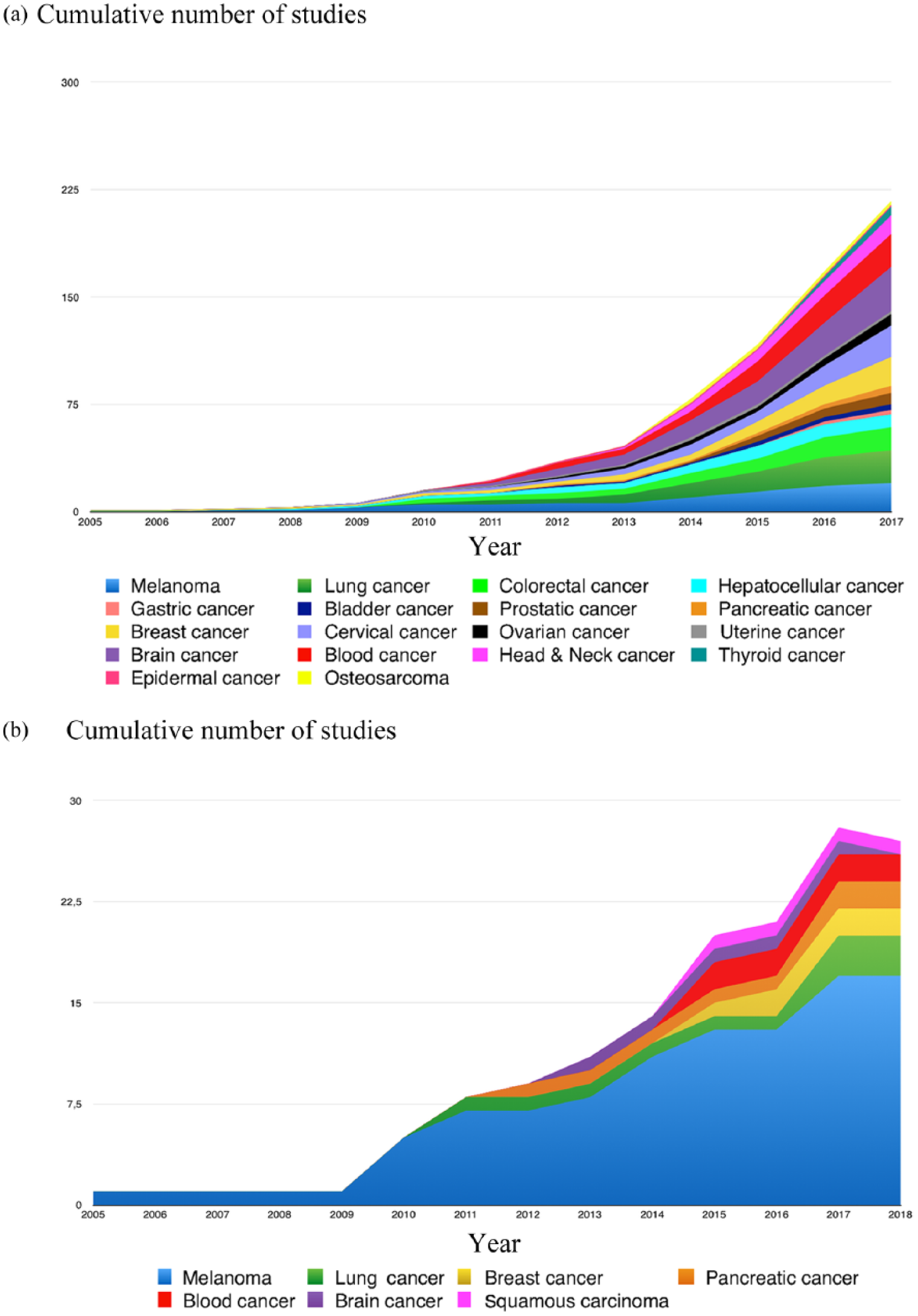
Cumulative histogram of the evolution over the years of the number of articles according to the type of cancer studied.
Discussion
This systematic review highlights the multiplicity of production methods and clinical applications of CAP in the field of oncology. Plasma jet is the predominant discharge device used for plasma production. Direct CAP treatment is the most represented, but indirect treatment appears to be increasing in recent years.
In 2012, the World Health Organization estimated the emergence of more than 14 million new cases of cancer in the world. 34 The search for new, complementary, less-invasive anticancer treatments with fewer side effects is therefore in rapid expansion. CAP induces apoptosis of cancer cells 2 and therefore represents a promising treatment.
One of its main advantages compared with conventional therapies is the potential of selectivity toward cancer cells. 5,16,17,19,35–38 Several hypotheses can be put forward to explain this phenomenon. First, an additional oxidative stress may exceed the cell survival limit more easily in cancer cells.16,38 Second, cancer cells exhibit a higher number of aquaporin on their membranes. 16 These aquaporins are responsible for a more important flow of RONS in cancer cells. Finally, the diffusion of RONS has been associated with the cholesterol composition of the cell membrane. Peroxidation of the membrane lipids results in the formation of pores and increases diffusion of the reactive species. The membrane of cancer cells contains less cholesterol than the membrane of healthy cells. A lower cholesterol fraction results in cells less resistant to peroxidation, with subsequent increased diffusion of reactive species and oxidative stress. 17
This selectivity is an essential parameter in the era of targeted therapies, since it is well known that localized treatments also reduce systemic deleterious side effects. The treatment of tumors and in particular, solid tumors, by anticancer drugs faces three important obstacles: treatment specificity, cancer cell resistance and finally, treatment penetration. Because of its physical and chemical properties, CAP is a multimodal therapeutic tool that could offer an answer to each of these issues. CAP seems to have an effect on cancer cells resistant to current treatments. The mechanisms involved seem to depend, inter alia, on p53, NF-κB, JNK or caspase pathways.39–42 The effects of electrical fields on cancer cells have been studied in vitro, in vivo and on patients. The electrical field causes apoptosis of cancer cells, inhibits tumor growth and improves the survival rate of patients with glioblastoma. 43 Moreover, Janigro and colleagues 44 demonstrated that the treatment of neoplasms by coupling chemotherapy and electric stimulation improved the therapeutic efficiency, allowing dose reduction of chemotherapy drugs by inhibiting multidrug resistance pumps (MDR pumps). Vijayarangan and colleagues 45 concluded that the increased delivery efficiency of the molecule was related to the membrane permeability resulting from the combined action of the RONS and the electric field. The delay between each pulse of the electric field plays a key role in the permeability. Plasma-induced chemical species and electric fields make CAP an interesting tool for optimizing drug delivery. Endocytosis has also been observed in relation to RONS and enhances drug intake. 45
Two discharge sources stand out today with regard the direct application of CAP at the clinical level: plasma jets and floating-electrode DBD (FE-DBD).2,46 The use of a plasma jet allows the propagation of plasma in small capillaries. Moreover, the use of a carrier gas makes it possible to modulate the plasma composition. 4 The prospects of clinical application are in targeting the deep organs. The development of a device called the plasma gun (which is a plasma jet) allows application of the plasma plume up to 1.5 m from the source. 6 Such a system allows the application of CAP under endoscopy and falls within a context of less-invasive surgery. CAP could be considered after tumor resection in order to treat the tumor microenvironment and the wound margins. On the other hand, when using an FE-DBD, the second electrode is not the ground, but human tissue or organ. This discharge device generates plasma in the air and imposes a maximum distance of 3 mm between the two electrodes. FE-DBD has also demonstrated its anticancer properties in vitro and in vivo.46,47 However, no study has examined the potential superiority of one system over the other. Also, the impact of the electric field in the use of FE-DBD should be evaluated.
Direct or indirect application does not result in a significant difference in plasma effects on cancer cells.48,49 A current limit of direct application is the depth of plasma delivery. An in vivo study 50 has shown that CAP could induce apoptosis only through the top cell layers, showing a depth of effective tissue penetration up to 60 μm. However, tissue models have shown that the penetration of RONS from plasma can reach to a single millimeter’s depth. 51 Both types of treatment decrease cell viability. 52 The ultimate objective is to be able to bring the benefits of CAP toward the treatment of patients. Indirect treatments’ cytotoxic effects depend on the medium and the delay between exposure and medium change. 53 An indirect treatment allows the injection of PAM, for instance, to treat more superficial tumors (skin, oral cavity) by direct approach. Moreover, PAM may be stored at −80°C without losing its anticancer effects. 54 The study of the most stable and effective PAM, opens the way for new pharmaceutical products. It is therefore necessary to validate the most reliable therapy for each clinical situation, in terms of efficiency and ergonomics.
We showed that helium alone was the most-used carrier gas for plasma and that gas mixtures were rarely used. The choice of gas is determinant for the plasma composition and the concentration of RONS. According to Kim and colleagues, 55 the rate of apoptosis of human breast cancer cells was greater with helium, and increased if oxygen was added. The amount of ROS increased using helium compared with argon or nitrogen. 56 The addition of oxygen to a flow of helium was responsible for a higher production of ROS. 57 It is not clear which kind of CAP is more efficient in anticancer application, and more studies are needed to determine the more efficient type of plasma for each type of cancer.
Many cancers may benefit from the use of CAP treatments. The most tested cell lines are derived from brain tumors. Brain and central nervous system cancers account for about 1.8% of new cancers and their incidence and mortality rates are higher in developed regions (Europe, North America, Australia/New Zealand). 34 The predominant use of glioblastoma cell lines shown in this study may be related to the aggressive nature of this malignant primary brain tumor, whose prognosis is not superior to 1 year with a very limited long-term survival. This cancer is also highly resistant to chemotherapy, radiotherapy and surgery. 58 Treatment with CAP could become an effective alternative and complementary therapy on these cancers. Another predominant field of study is melanoma, the most aggressive skin cancer. Its prevalence is high, representing 1.6% of the new cancers 34 and its median overall survival rate is less than 2 years. Murine melanoma cancer cell lines and human melanoma cancer cell lines represented 8.6% and 12% of the studies, respectively. Melanoma, like brain cancers, is often resistant to acute treatment modalities. 52 Furthermore, due to the anatomical position of the melanoma, a treatment with CAP can be conceived directly or indirectly. Both approaches have shown their efficiency in reducing the viability of melanoma cells. However, some melanoma cancer lines are less sensitive to PAM than to direct treatments. 52
Twenty-seven in vivo studies have been identified and concluded that there was a significant reduction in tumor size and an increase in survival rate. In vivo interventions were mostly performed on subcutaneous tumor xenografts in mice. Another study based on the use of a tumor chorioallantoic model was conducted. 50 Although the results corroborate the in vitro studies, the development of models closer to clinical situations is necessary. Taking into account the tumor microenvironment is essential and can also be a target of anticancer treatments. 59
Tumors are able to evade surveillance of the immune system through immunosuppressive strategies. The emerging concept of immunotherapy and immunogenic cell death is to restore or rise immunogenicity of tumor cells by exposing new antigens. 60 Following severe stress, cells exhibit damage-associated molecular patterns. ROS produced with CAP could elicit immunogenic cell death. Furthermore, CAP stimulates the recruitment of macrophages and cytotoxic T cells. 61 Mizuno and colleagues 62 suggest that CAP may promote adaptive immunity in vivo against melanoma cells.
The interest of the plasma is thus triple: local induction of an immunogenic cell death, induction of a systemic response against cancerous cells and the induction of an immune memory. 63
Finally, only three clinical trials or follow ups have been identified. Two of them studied the application of CAP on patients with head and neck cancers as a palliative treatment or before tumor resection. Such a therapeutic choice can be explained by the ability of CAP to decontaminate,64,65 treat severely infected wounds or ulcerations66,67 and induce apoptosis in head and neck cancer cell lines.19,68–72 In a recent clinical follow up, Metelmann and colleagues 73 investigated the effect of CAP on the surface of head and neck squamous cell carcinoma tumors. The results have shown an improvement in the quality of life of the patients (reduction in odor and analgesic use), tumor reduction and significant improvement in tumor decontamination.
In addition, an ongoing clinical trial 32 is assessing the effect of CAP on the reduction of lymphocele following pelvic lymph node dissection during robot-assisted radical prostatectomy. Finally, another ongoing clinical trial 33 is in recruitment phase to study the effect of CAP on human cervical intraepithelial neoplasia, once again showing its potential use in oncology.
The increased interest in the use of CAP for cancer treatment by the medical community is closely related to the need for new therapies. One of the future directions in the field of anticancer potential of CAP may be the action on dysplastic cells in particularly extensive lesions in critical areas where surgery would be impossible or too invasive. Interestingly, no resistance to CAPs has been reported to date.
Conclusion
This study highlights the multiplicity of means of production and potential clinical applications of CAP in the field of oncology. Its anticancer action is mainly mediated by the production of reactive species. Among the different promising biological effects, plasma can induce apoptosis of cancer cells resistant to conventional chemotherapy and may be used in combination with current treatments to obtain a synergetic and complementary action. No resistance to CAPs have been reported to date. The clinical use of this innovative therapy requires the development of standardized reliable protocols in order to compare the results between future clinical trials. More studies are also required to determine the more efficient type of plasma for each type of cancer. To obtain comparative results, standardized measures of the effectiveness of the different systems are necessary. While plasma jets and FE-DBDs find their indication in direct approaches, DBD opens the way for the development of new pharmaceutical products that can be generated on an industrial scale.
Supplemental Material
2017_02_19_Table_S1 – Supplemental material for Use of cold-atmospheric plasma in oncology: a concise systematic review
Supplemental material, 2017_02_19_Table_S1 for Use of cold-atmospheric plasma in oncology: a concise systematic review by Antoine Dubuc, Paul Monsarrat, François Virard, Nofel Merbahi, Jean-Philippe Sarrette, Sara Laurencin-Dalicieux and Sarah Cousty in Therapeutic Advances in Medical Oncology
Supplemental Material
2018_02_18_Table_S2 – Supplemental material for Use of cold-atmospheric plasma in oncology: a concise systematic review
Supplemental material, 2018_02_18_Table_S2 for Use of cold-atmospheric plasma in oncology: a concise systematic review by Antoine Dubuc, Paul Monsarrat, François Virard, Nofel Merbahi, Jean-Philippe Sarrette, Sara Laurencin-Dalicieux and Sarah Cousty in Therapeutic Advances in Medical Oncology
Supplemental Material
Supplementary_figures – Supplemental material for Use of cold-atmospheric plasma in oncology: a concise systematic review
Supplemental material, Supplementary_figures for Use of cold-atmospheric plasma in oncology: a concise systematic review by Antoine Dubuc, Paul Monsarrat, François Virard, Nofel Merbahi, Jean-Philippe Sarrette, Sara Laurencin-Dalicieux and Sarah Cousty in Therapeutic Advances in Medical Oncology
Footnotes
Acknowledgements
Study concept and design: AD, PM, SL, FV, JPS, NM, SC.
Acquisition of data: AD, PM, SL, SC.
Analysis and interpretation of data: AD, PM, SC.
Drafting of the manuscript: AD, PM, SC
Administrative, technical and material support: SL, FV, JPS, NM, SC
Study supervision: PM, SL, FV, JPS, NM, SC
All of the named authors were involved in the paper and have read it before being submitted for publication
Funding
This study was supported by the Midi-Pyrenees Region, Paul Sabatier University and the research platform from Toulouse Dental Faculty.
Conflict of interest statement
The authors declare that there is no conflict of interest.
Supplementary material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.