
Abstract
Glioblastoma is not only the most common primary brain tumor, but also the most aggressive. Currently, the most effective treatment of surgery, chemotherapy and radiation therapy allows for a modest median survival of 15 months. Here, we report a case of a 57-year-old male with histologically confirmed glioblastoma with unfavorable prognostic characteristics (poor performance status and persistent neurological symptoms after surgery), whose expected 5-year survival is 0%. Further genetic analysis offered a mixed prognostic picture with positive methylation of 0-6-methylguinine-DNA (deoxyribonucleic acid) methyltransferase (MGMT; favorable prognosis) and wild-type isocitrate dehydrogenase 1 (IDH-1; unfavorable prognosis). Remarkably, the patient showed a progression-free survival of 5.5 years and a total survival of 6.5 years. In the context of recently published literature, the authors hypothesize that the patient’s use of the antipsychotic medication risperidone may have had a potential antitumor effect. Risperidone antagonizes the dopamine-2 receptor and the serotonin-7 receptor, both of which have been individually implicated in the growth and progression of glioblastoma. To the authors’ knowledge, this is the first clinical case in the literature to explore this association.
Introduction
Glioblastoma (GBM) remains the most common and most aggressive primary brain tumor, with a median survival of merely 3–4 months without treatment [Omuro and DeAngelis, 2013]. This increases to 12 months with surgery and adjuvant radiation therapy [Stupp et al. 2005]. Currently, however, the first-line treatment includes surgery, radiation therapy and chemotherapy, which offers a median survival of almost 15 months [Stupp et al. 2005]. In addition, the 5-year survival rates of GBM patients have historically been under 5%, although recursion-partitioning analysis (RPA) indicates that this value reaches 0% statistically with an older age of diagnosis (>50-years old) and a lower Karnofsky Performance Status score (KPS; <70) [Shaw et al. 2003]. The survival after recurrence of disease has been reported to be between 3 and 4 months [Omuro and DeAngelis, 2013]. In this case report, we present a patient with a number of unfavorable characteristics: KPS score < 70 (50) at diagnosis, and the presence of preoperative symptoms that persisted after surgery. Despite these prognostically unfavorable features, and contrary to all abovementioned statistics, our patient showed a remarkable survival of 6.5 years with a progression-free survival of about 5.5 years. Furthermore, the patient survived an additional year after first evidence of recurrence of GBM. One of the patient’s medications was risperidone, a dopamine receptor D2 (DRD2) antagonist, used to treat schizophrenia. One very recent study showed that DRD2 activity was required for GBM growth [Li et al. 2014]. It reported that DRD2 antagonists suppressed the growth of patient-derived GBM both in vitro and in vivo [Li et al. 2014]. Risperidone is also an inhibitor of the serotonin receptor 7 (5-HT7), which is overexpressed in GBM and known to stimulate its growth [Kast, 2010]. The efficacy of this class of medications in GBM, however, has not been demonstrated in humans in a clinical setting. Given the context, this report addresses that gap by highlighting a potentially novel mechanism of treatment in GBM.
Case report
Patient history and examination
This 57-year-old man checked himself into an outside hospital for depression, aphasia and gait imbalances, which prompted a workup. A magnetic resonance imaging (MRI) scan on 8 July 2006 demonstrated a 6.5 cm heterogeneous left posterior temporal tumor and led to the diagnosis of GBM. At the time of presentation, the patient had an extensive history of psychiatric diseases: paranoid schizophrenia, anxiety, severe depression, as well as a controlled seizure disorder.
Operation
Based on the preoperative MRI (Figure 1A, B), the patient underwent a left temporoparietal craniotomy on 18 July 2006. A gross total resection of the tumor was achieved and confirmed with a postoperative MRI, performed within 48 hours of surgical resection (Figure 1C, D).

Contrast-enhanced magnetic resonance imaging (MRI) images: (A) preoperative (axial) (B) preoperative (coronal) (C) postoperative (axial) (D) postoperative (coronal) (E) recurrence (axial) (F) recurrence (coronal) (G) postrecurrence treatment plan (axial and coronal). [A] refers to the anterior side, [P] refers to the posterior side, [R] refers to the right side, [L] refers to the left side, [H] refers to the head and [F] refers to the feet. The white arrows are pointing to the tumor. The color scheme associated with Figure 1G shows the dose of the radiation delivered around the tumor.
Postoperative, prerecurrence management
After the surgery, the patient remained symptomatic, as he was having difficulties with his walking and memory. He received adjuvant radiation therapy (60 Gy at 2.0 Gy per fraction) concurrently with temozolomide (75 kg/m2), completing therapy on 5 October 2006. Subsequently, he was placed on maintenance temozolomide (150 kg/m2) with treatment for days 1–5 for every 28-day cycle, which was the regimen he continued until December 2011 when the disease recurred.
Magnetic resonance imaging, postrecurrence treatment and outcome
MRIs were performed every 2 months, starting after the left temporoparietal craniotomy in July 2006 until disease recurrence in late December 2011 (nearly 5.5 years of progression-free survival). MRI results from 22 December 2011 showed a previously unseen area of nodular enhancement measuring up to 4 mm in the left posterior cingulum. Apart from the radiological signs of recurrence, the patient also presented with clinical deterioration of increased memory loss, worsening vision, decreased motor ability and a shuffling gait. After recurrence, the patient was switched to metronomic doses of temozolomide (75 mg/m2), which meant a low-dose intake every day for 6 weeks with 2-week gaps in between the 6-week cycles. The patient was also treated with fractionated stereotactic radiosurgery (SRS 30 Gy in five fractions) in February 2012 and with Avastin (Genentech, Inc., San Francisco, CA, USA) [Gutin et al. 2009].
After initial evidence of recurrence, a follow-up MRI in early January 2012 showed that the nodular enhanced area increased in size to 7 mm (Figure 1E, F). Another MRI in April 2012 showed that the nodule had decreased in size to 2–3 mm, suggesting an initially favorable response to the stereotactic radiosurgery (SRS) and chemotherapy regimen (Figure 1G). Another MRI in July 2012, however, showed an enlargement of a left-sided heterogeneous-enhancing mass within the left cingulum and contiguous genu of the corpus callosum. On 12 September 2012, MRI results showed a continued increase in tumor size in the left medial parietal lobe with extension across the midline within the splenium of the corpus callosum.
After multiple falls, the patient was found to have bilateral subdural hematomas on 28 October 2012, for which he underwent a craniotomy 3 days later. The patient never recovered consciousness after the surgery. On 17 December 2012, he developed acute respiratory failure and progressed to respiratory and cardiac arrest on the same day.
Management of the paranoid schizophrenia
The patient was prescribed risperidone in the year 2000, about 6.5 years before he was diagnosed with GBM. When he was diagnosed with GBM in 2006, he was taking a total daily dose of 6 mg and up to 6.5 mg as needed. Dosage information up until his diagnosis of GBM is unknown. By late 2006, his dose had been reduced to 4.5 mg/day. He was taking this dose until it was again lowered to 4 mg in early 2008. In early 2009 and early 2011, respectively, his dose was reduced to 3 mg/day and then to 2.5 mg/day. Just 3 months before his recurrence, his dose was again reduced to 2 mg/day. He was taking this dose until his death. Throughout this course, the patient complained that he felt overmedicated and was experiencing shuffling gait and cognitive decline with dementia-like symptoms. It was felt that these symptoms might have been due to the side effects of the antipsychotic therapy. As such, the risperidone dose was decreased several times between 2006 and 2012.
Genetic and histological analysis
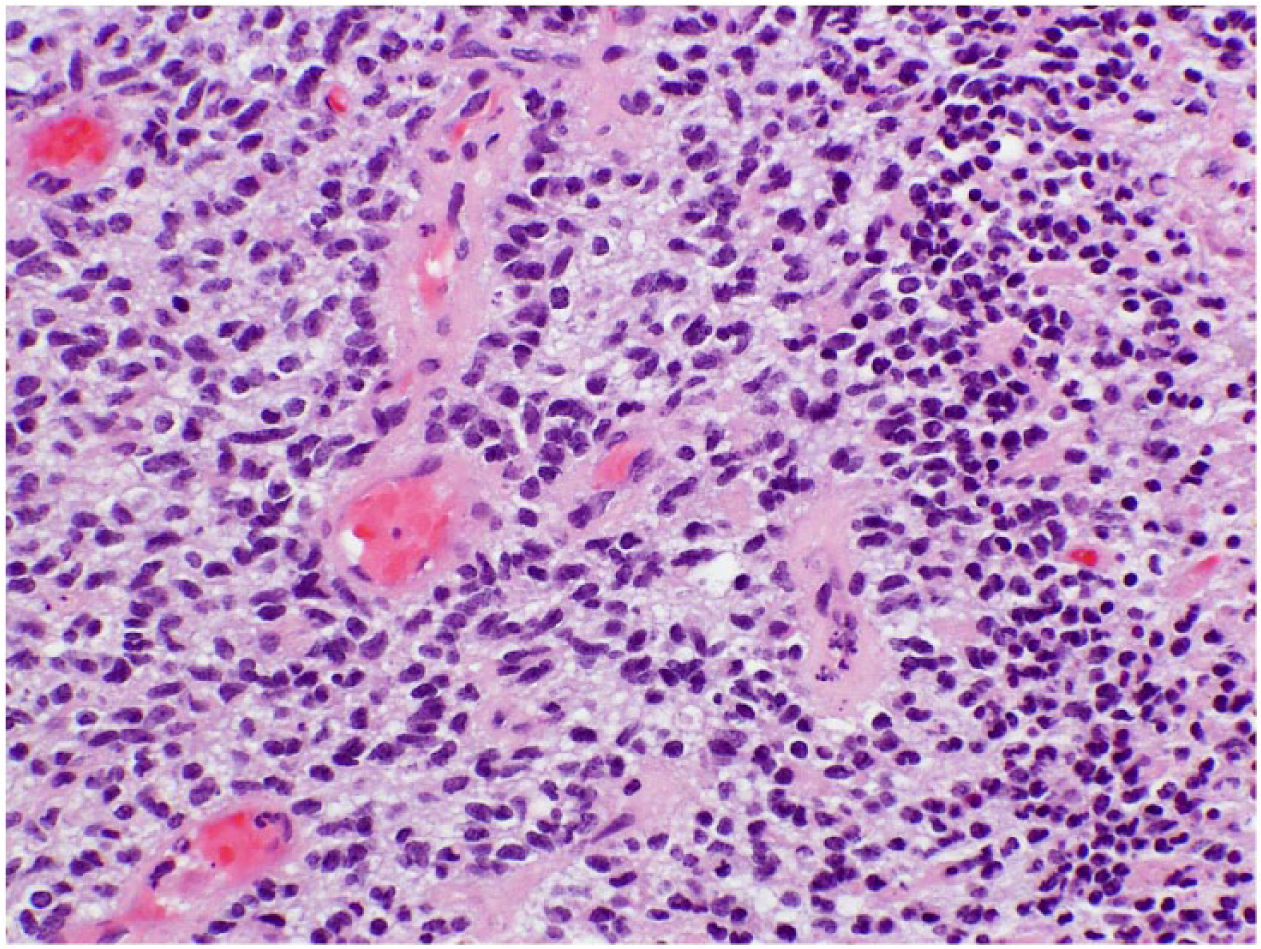
Histological analysis of the tumor showed dense cellularity and pseudopalisading necrosis, confirming the diagnosis of GBM (Figure 2). Further analysis confirmed small-cell cytology (Figure 3). Genetic analysis of the patient’s tissue revealed wild-type IDH-1 expression (Figure 4), positive methylation at the MGMT promoter and a KI-67 labeling index of 15% (Figure 5).

Hematoxylin and eosin-stained section at 20×, which demonstrates dense cellularity, necrosis and perinecrotic pseudopalisading cells that are characteristic of glioblastoma.
Hematoxylin and eosin stained at 40×, which demonstrates small cell cytology of the lesion.

Hematoxylin counterstain at 40×, which demonstrates absence of mutant IDH-1 (R132H). (a), Hematoxylin counterstain at 40×, which demonstrates labeling of tumor cells in the positive immuno-histochemical control sample, an astrocytoma shown to be IDH 1(R132H)-mutant on PCR amplification and direct sequencing (b).

Hematoxylin counterstain at 40×, which demonstrates a MIB-1/Ki-67 labeling index of 15%.
Discussion
In order to evaluate the role of risperidone in the long survival of our patient, it is crucial to assess relevant genetic and nongenetic prognostic factors. The patient’s KPS of 50 and postoperative neurological symptoms suggest a poor prognosis. In fact, RPA analysis indicates a 5-year survival rate of 0% in such a patient, irrespective of any other prognostic variables [Shaw et al. 2003]. Genetic studies were performed with respect to MGMT methylation status, IDH-1 mutation status and KI-67 labeling index in order to achieve a fuller understanding of the patient’s prognosis. The MGMT gene encodes for a deoxyribonucleic acid (DNA)-repair protein that can remove methyl groups from guanine bases, thereby interfering with the mechanism of action of the alkylating agent temozolomide [Kim et al. 2012]. As such, MGMT promoter methylation may be associated with reduced expression of the protein and, therefore, an increased susceptibility to temozolomide [Kim et al. 2012]. In one study, the median progression-free survival was 18 months and 9 months, and overall survival was 29 months and 20 months in the methylation and nonmethylation groups, respectively [Kim et al. 2012]. Another study showed a median progression-free survival of 7.5 and 6.3 months, and overall survival of 18.9 and 11.1 months in the methylation and nonmethylation groups, respectively [Weller et al. 2009]. While these and other studies show a prognostic benefit with MGMT methylation, the added progression-free survival and overall survival is typically in the order of months rather than years. As such, we do not believe that our patient’s MGMT methylation status can wholly explain the progression-free survival of over 65 months and overall survival of over 75 months, especially given the patient’s other unfavorable prognostic factors.
The IDH-1 gene encodes for isocitrate dehydrogenase, which is known to be prognostically important in brain tumors [Cohen et al. 2013]. It is known that lower-grade gliomas and secondary GBM (GBM that progresses from lower-grade gliomas) often carry an IDH mutation at the amino-acid residue 132, typically resulting in the conversion from arginine to histidine (R132H) [Cohen et al. 2013]. Conversely, primary GBM rarely show the IDH-1 mutation [Cohen et al. 2013]. Therefore, the IDH wild-type genotype, as is the case with our patient, signifies a worse prognosis. A third prognostic factor involves the KI-67 protein, which is an antigen found in many dividing cancer cells. The fraction of KI-67-positive cancer cells, termed the KI-67 labeling index, may have prognostic significance in GBM. A study with 24 patients found a median labeling index of 20.5% (range of 2.3–62%). The individuals with a labeling index of between 10% and 30% had an average survival of 15.8 months [Mastronardi et al. 1999]. Another study found a median KI-67 labeling index of 13.0% (range 7.2–31.8%) in 19 patients [Schröder et al. 2002]. In this study, a 15% KI-67 labeling index correlated with a time to recurrence of symptoms of just over 6 months [Schröder et al. 2002]. Given the current literature, the patient’s IDH-1 wild type status and KI-67 labeling index would indicate a relatively poor prognostic outcome, suggesting that the patient’s long survival is despite these characteristics.
Given that the patient mostly has unfavorable prognostic characteristics, the expected survival time is likely less than that represented in the current literature. As such, a total survival of 6.5 years and a progression-free survival of 5.5 years are remarkably unusual. In addition, the survival time of 1 year after recurrence is quite unusual as well. We propose a possible explanation by examining the patient’s long-term risperidone use for his paranoid schizophrenia. Specifically, we are interested in risperidone’s effect as a DRD2 and 5-HT7 antagonist. A handful of laboratory studies exploring the effects of risperidone and similar medications on GBM have recently been published. There is, however, no clinical data on this topic in the current literature. From the few laboratory studies that have been conducted, we know that activation of the DRD2 by dopamine leads to a cascade of events that favors the proliferation and survival of cells [Bartek and Hodny, 2014; Li et al. 2014]. Activation of the receptor first leads to activation of the trimeric G-protein complex, which then recruits a GTPase [Bartek and Hodny, 2014; Li et al. 2014]. This GTPase hydrolyzes the RAP1-GTP into its inactive GDP form [Bartek and Hodny, 2014; Li et al. 2014]. The RAP1-GTP is known to bind to Raf-1 and sequester it, preventing it from activating the MAK/ERK pathway [Bartek and Hodny, 2014; Li et al. 2014]. This MEK/ERK pathway is a canonical mitogenic pathway, meaning that it promotes cellular proliferation and survival [Bartek and Hodny, 2014; Li et al. 2014]. A DRD2 antagonist would prevent the downstream hydrolysis and inactivation of the RAP-GTP1 into its GDP form. RAP-GTP1 would then be free to sequester Raf-1 and inhibit its ability to activate MEK/ERK.
It was thought that, due to the aforementioned pathway, DRD2 antagonists might offer some interesting anticancerous benefits. Researchers from the University of California, San Diego and Harvard University confirmed this to be likely. They made several findings that are potentially pertinent to our patient. They used small-hairpin ribonucleic acid (shRNA) to silence the expression of certain genes in GBM cells [Li et al. 2014]. This allowed them to uncover which genes and pathways were the most important in the growth of the cancer cells. One such pathway was the DRD2 receptor pathway [Li et al. 2014]. In addition, the DRD2 messenger ribonucleic acid (mRNA) and protein expression were elevated in GBM relative to control specimens [Li et al. 2014]. They were also able to suppress the growth and proliferation of the GBM cells by using either a silencing shRNA or a DRD2 antagonist [Li et al. 2014]. They were able to successfully achieve anticancerous effects with four DRD2 antagonists, one of which was risperidone [Li et al. 2014].
Another potential effect of risperidone is the inhibition of the 5-HT7 receptor in serotonin signaling [Mahé et al. 2004]. One study showed that all human GBM cell lines tested expressed the functional 5-HT7 receptor [Mahé et al. 2004]. Another study reported that 5-HT7 agonists stimulated the ERK pathway and interleukin-6 (IL-6) synthesis in a GBM cell line [Lieb et al. 2005]. The important role of the ERK pathway in stimulating GBM has been discussed above and seems to be relevant to both dopamine and serotonin signaling. Back in 1997, researchers first reported that IL-6 was able to mediate the growth of GBM in an autocrine fashion [Candi et al. 1997]. Since then, the role of IL-6 in GBM growth has been corroborated. Since the activation of the ERK pathway and IL-6, in part, depends on serotonin signaling, clinical inhibition of the 5-HT7 receptor may provide a potential antitumor benefit in GBM [Mahé et al. 2004]. Despite these data, we are not aware of any clinical evidence in humans suggesting a benefit of DRD2 and 5-HT7 antagonists in GBM. As such, we believe that this report may offer valuable insight into a potentially novel mechanism for the treatment of GBM.
As previously mentioned, the patient’s risperidone dose was decreased from up to 6.5 mg/day to 2 mg/day from 2006 until disease recurrence. It is plausible that such a significant reduction may have inadvertently removed the potential protective effects of risperidone. It is possible that a subthreshold level was eventually reached, beyond which the DRD2 antagonism was no longer sufficient to prevent disease progression. A study looking at the risperidone’s DRD2 receptor occupancy at different doses showed that 79% of the receptors were occupied at a dose of 6 mg/day [Kapur et al. 1997]. The receptor occupancy, however, fell to 73% at 4 mg/day and to 66% at 2 mg/day [Kapur et al. 1997]. As such, the lowering of the doses from 6 mg to 2 mg may have had a clinically significant effect with respect to the drug’s ability to suppress the growth of GBM cells. It must also be noted that about 9 months before the recurrence of the GBM, records showed that the patient sometimes forgot to take his medications. Given the patient’s complicated 12–15 medications regimen, and given his increasing forgetfulness in taking his medications, it is likely that the patient was receiving a lower daily dose of risperidone than prescribed, just before the recurrence.
Conclusion
The therapeutic potential of using DRD2 and 5-HT7 antagonists in GBM is an important avenue that deserves further scrutiny and attention. These drugs are already FDA approved and may be repurposed relatively quickly if benefit is shown through more research. It still remains, however, that research on this topic is lacking in the existing literature. While the basic sciences will further elucidate the potential role of dopamine and serotonin signaling in the pathophysiology of GBM and the potential benefits of these antagonists, it is incumbent upon clinicians to observe relevant effects and associations between these drugs and certain diseases like GBM, and perhaps even other cancers.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Conflict of interest statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary Materials
Additional information can be accessed upon request from the authors of the paper.